

Volume 14, Issue 2 (Mar & Apr 2024)
J Research Health 2024, 14(2): 139-146 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Changizi M, Mohamadian H, Cheraghian B, Salmanzadeh S, Maqsoodi F, Ghorbani Kalkhajeh S. Prevalence of COVID-19 Protective Behavior (The Use of Face Mask) Among Pedestrians in the Southwestern Regions of Iran: An Observational Study. J Research Health 2024; 14 (2) :139-146
URL: http://jrh.gmu.ac.ir/article-1-2185-en.html
URL: http://jrh.gmu.ac.ir/article-1-2185-en.html
Maryam Changizi1 

 , Hooshang Mohamadian2 , Bahman Cheraghian3 , Shokrollah Salmanzadeh4 , Fatemeh Maqsoodi2 , Sasan Ghorbani Kalkhajeh5
, Hooshang Mohamadian2 , Bahman Cheraghian3 , Shokrollah Salmanzadeh4 , Fatemeh Maqsoodi2 , Sasan Ghorbani Kalkhajeh5
, Hooshang Mohamadian2 , Bahman Cheraghian3 , Shokrollah Salmanzadeh4 , Fatemeh Maqsoodi2 , Sasan Ghorbani Kalkhajeh5
1- Department of Community Medicine, School of Medicine, Abadan University of Medical Sciences, Abadan, Iran. , mrs.changizi@yahoo.com
2- Department of Public Health, School of Health, Abadan University of Medical Sciences, Abadan, Iran.
3- Department of Biostatistics and Epidemiology, School of Public Health, Hearing Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
4- Department of Infectious Diseases, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
5- Department of Community Medicine, School of Medicine, Abadan University of Medical Sciences, Abadan, Iran.
2- Department of Public Health, School of Health, Abadan University of Medical Sciences, Abadan, Iran.
3- Department of Biostatistics and Epidemiology, School of Public Health, Hearing Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
4- Department of Infectious Diseases, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
5- Department of Community Medicine, School of Medicine, Abadan University of Medical Sciences, Abadan, Iran.
Full-Text [PDF 662 kb]
(647 Downloads)
| Abstract (HTML) (3335 Views)
Full-Text: (1221 Views)
Introduction
Severe acute respiratory syndrome coronavirus (SARS CoV 2) has affected many people and caused countless deaths. The impact of this disease on welfare, economy, employment, and other aspects of daily life has been observed throughout societies and individuals [1]. Early stages of COVID-19 pandemic, public health messages about wearing face masks use were contradictory and accompanied by various opinions that caused public dissatisfaction and confusion. Finally, the recommendations evolved with scientific understanding [2]. Current strategies, such as physical distance of at least one meter and more, face mask use, and hand washing have been suggested [3]. Data show that wearing a mask protects all people, including healthcare workers and the public, from infection with the virus and can have more benefits [1]. The main advantage of these measures is the reduction of further transmission of the virus and consequently the reduction of adverse outcomes, number of hospitalizations, and deaths [4]. Research has shown that face mask usage reduces the daily growth rate of infection between 47%-70% [5, 6]. A face mask can also reduce the initial risk of respiratory infection by 6%-15% [4]. However, resistance still exists among people to use this tool for personal protection and the use of masks has been reported to be moderate or low among some people [7, 8]. Face masks can vary in terms of filtration efficiency and breathability [9]. In addition, some people found that long-term use of the mask in hot environments is uncomfortable, and covering the nose and mouth may prevent verbal and non-verbal communication [10]. Others also believe that using a face mask is associated with oxygen decrease and prefer not to use it. However, the available data do not support these cases [11]. Iran is also one of the countries with the highest infection and death rates due to COVID-19 [6]. One way to control the coronavirus in Iran is to encourage face mask usage [1]. Therefore, it is necessary to know the prevalence of mask use in some areas. This study was conducted to estimate the prevalence of face mask use among pedestrians in Abadan, Khorramshahr, and Shadegan cities with different characteristics.
Methods
This population-based cross-sectional study was conducted in Abadan, Khorramshahr and Shadgan in southwestern cities of Iran from June to August 2021.
Inclusion criteria
The inclusion criteria included all the pedestrians of determinate neighborhoods in Abadan, Khorramshahr and Shadgan in the southwest cities of Iran.
Exclusion criteria
The exclusion criteria included covering the face with something other than a mask so that the observer cannot recognize the pedestrian’s face mask.
Sample size
The minimum sample size was determined based on the formula to estimate a population proportion in a cross-sectional study with the characteristics of P>0.456, d=0.05, α=0.05 and z=1-α/2 was determined 381 subjects. According to the sampling method and applying the planned effect of 1.5, the minimum sample size was 571 for each region. Due to the unequal size of an area and using a proportional, the final sample size was 6 852. According to the municipal areas the statistical population and measuring the two issues, surely, this number of samples can be representative of measuring southern urban areas.
Accordingly, 34 262 284 and 1 142 people were considered for the urban population of Abadan, Khorramshahr and Shadgan in the southwest cities of Iran. Finally, 7 425 pedestrians were observed in this study, which were 135 clusters of 55 people from 85 urban neighborhoods
Sampling
We employed nine observers with bachelor’s degrees. During two educational sessions, the main researcher trained the observer on how to select subjects and complete the observation checklist. Also, daily monitoring on observer was done by the supervisors. The location of the stations was selected by a purposeful method among the busy passages in Abadan, Khorramshahr and Shadegan neighborhoods. In the last stage, sampling was performed by the non-probability sampling method. In each station, observer, including three men and six women filled out the data. The form contains the studied variables for individual. The observers recorded the variables of gender, age, face mask usage, gloves, shield and type of face mask and correct use of a face mask. Incorrect use of face mask was stated in the checklist with insufficient coverage of the mouth and nose and wearing mask upside down. Observation during busy hours of each area was done from 8:00 AM to 13:00 PM and 17:00.00 PM to 00:00 AM.
Data collection
Data were collected by observation. In this research, a multi-stage sampling method was used. First, cities were divided into several categories based on the division of urban areas. Then in each area according to its population, several observation stations were randomly selected from the list of neighborhoods.
Participants
Pedestrian areas of urban stations determined in the study.
Data analysis
Data were analyzed with WINPEPI (accurate determination of confidence interval) and software, version 26. We used descriptive tests (reporting gender, age and sex, use of masks, etc.). The prevalence rate was estimated with a 95% confidence interval (95% CI), chi-square (the relationship between gender and the use of face masks), and Fisher’s exact tests. The Statistical significance was acceptable if P<0.05. The normality of the data was checked by the Kolmogorov-Smirnov test.
Results
A total number of 7425 pedestrians were assessed in this study. Most pedestrians observed were in the age group of 21-30 years (23.7%). Most subjects were men 4115(55.4%). Among the pedestrians, 3997(53.8%) people used facemasks. Table 1 presents demographic characteristic of pedestrians and preventive behaviors.
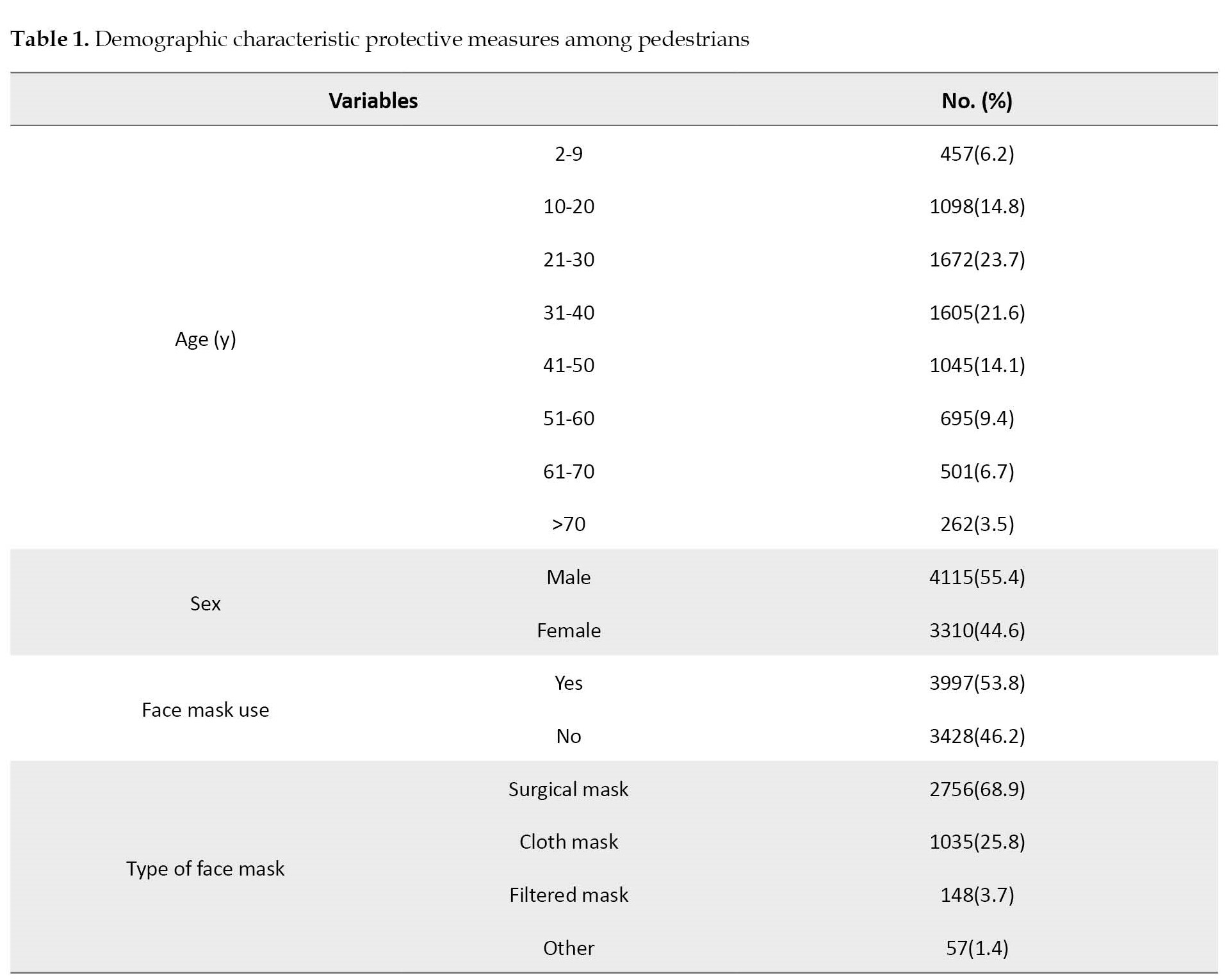
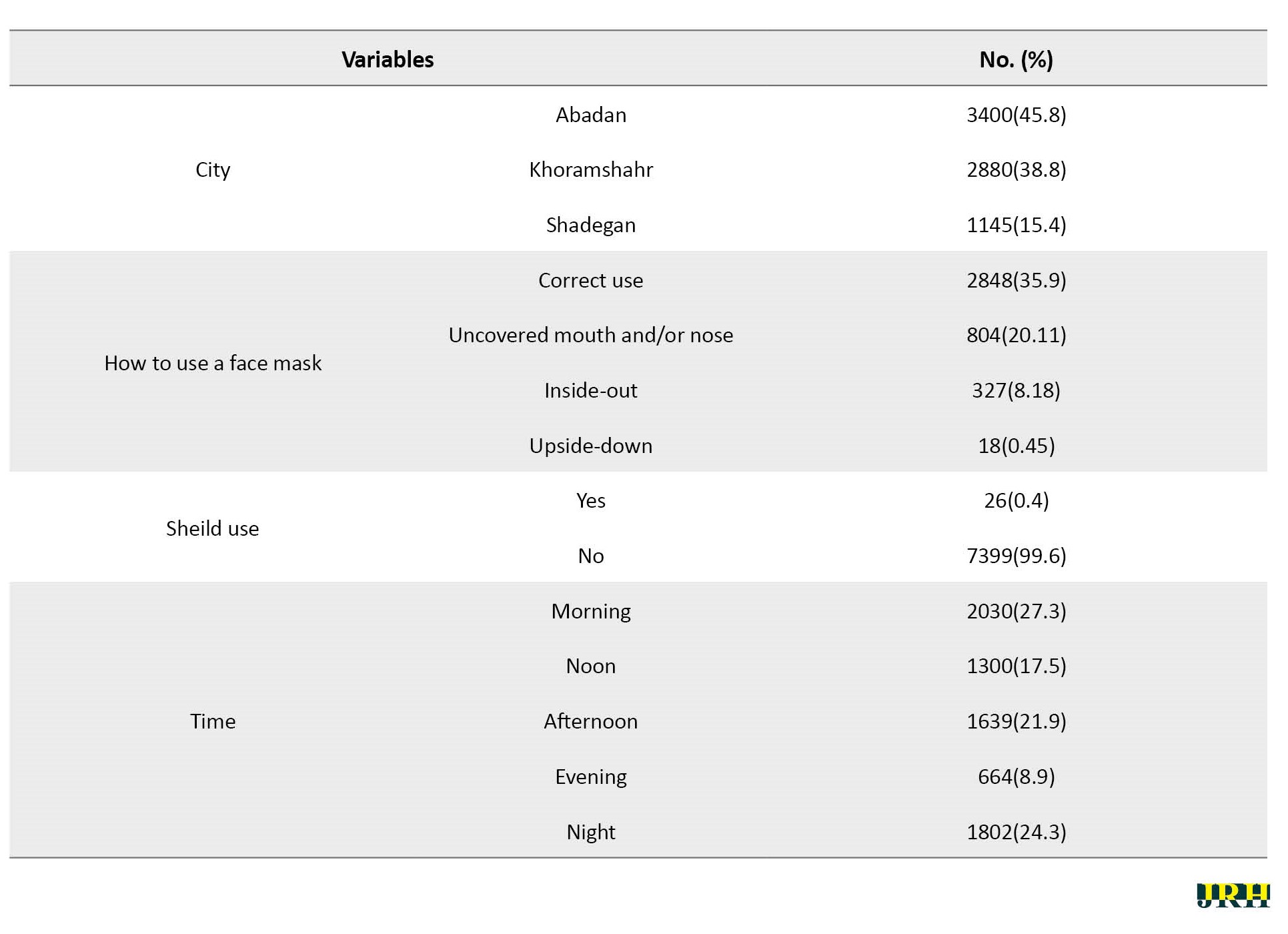
The prevalence of facemask usage was 53.7% (95% confidence interval [95% CI, 52.7%, 55.0%). The highest prevalence of mask use was observed in the age group of 31-40 years (59.8%) and the lowest in the age group of 70 years and older (44.7%). In the present study, usage masks among men more than women (54.3% vs 53.0%). The prevalence of mask use was the highest in Abadan City and it was the lowest in Khorramshahr City. The most commonly used mask among pedestrians was the surgical mask (37.1%) and the lowest were filtered mask (2%). The usage of filter masks was higher among the age group of 10-20 years (2.6%). The most common use of surgical masks was in the age group of 21-30 years (40.9%). Older people aged 61-70 used more cloth masks than others (15.4%). The use of masks was more in the morning and at night (25.4% vs 24.5%, P<0.001). The usage face mask and type of it was related to the age of pedestrians (P<0.001). No relationship was found between gender and mask use and mask type (P=0.05). Pedestrians observation were at 9-10 AM (23.7%), 11 AM (13.4%) and 8 PM (11.6%). Pedestrians usage of face mask was related to observation times (P<0.001). Pedestrians in the age group of 21-30 years, 26.67% more used face masks correctly (Table 2).
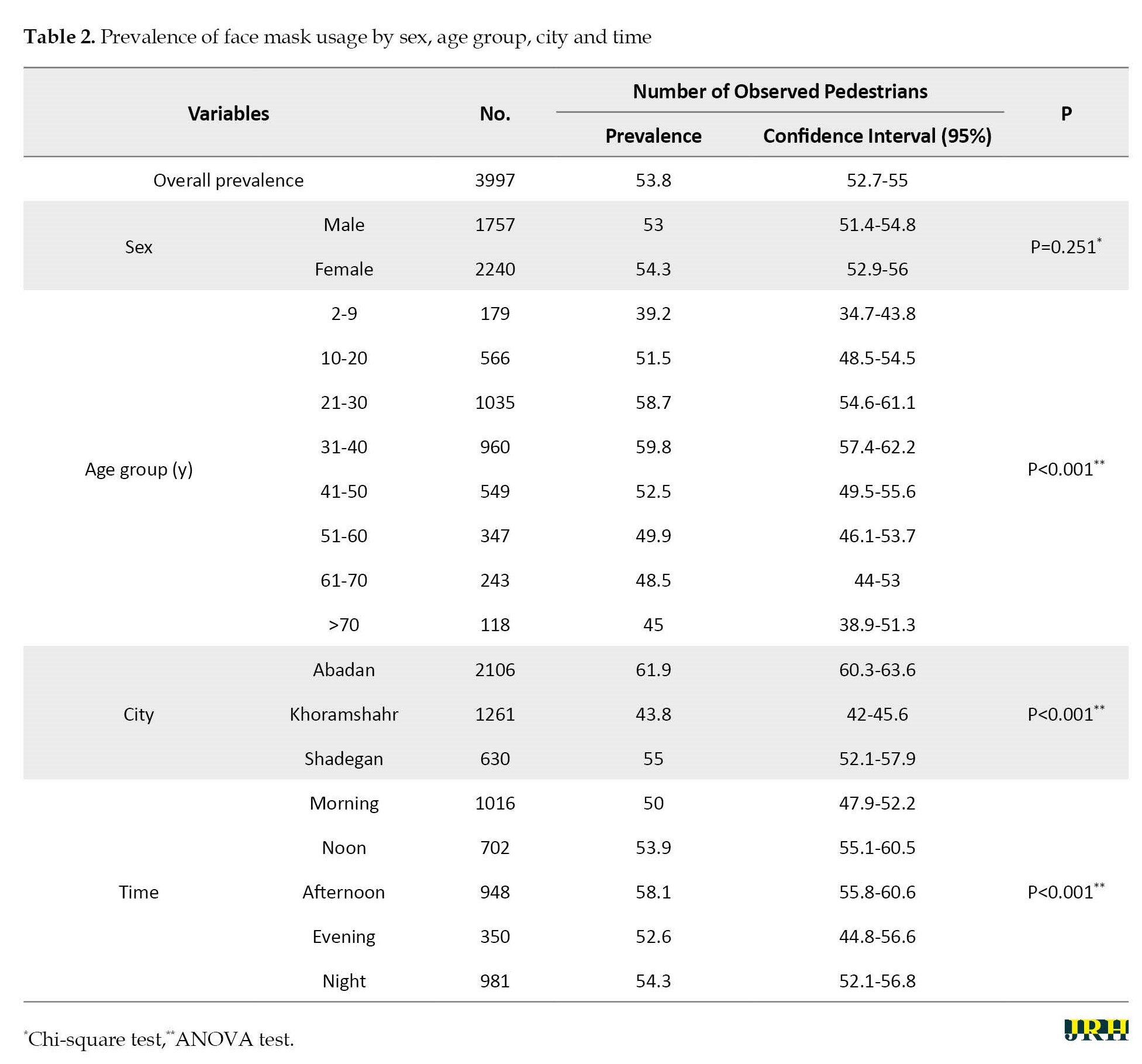
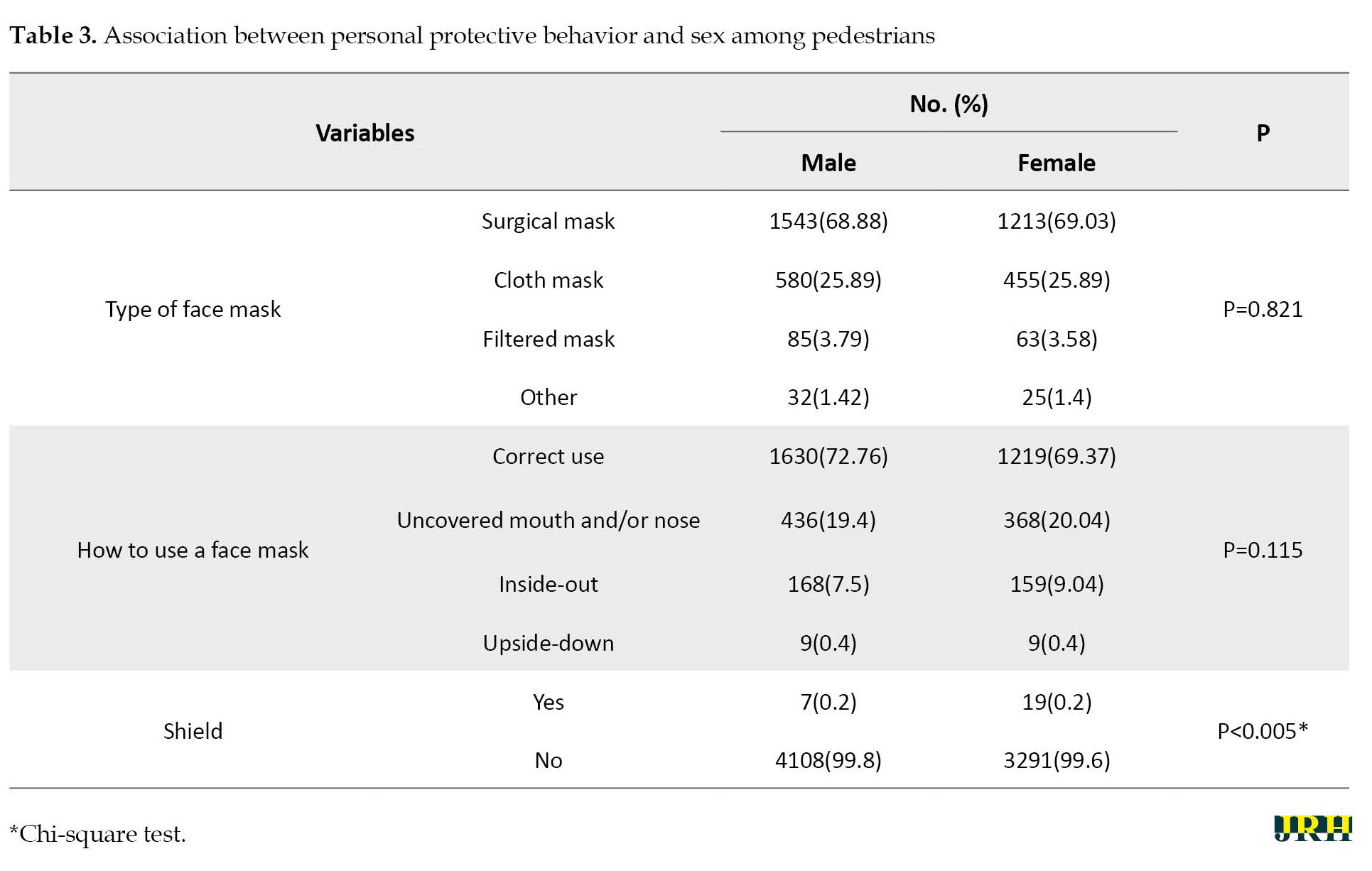
In the present study, only 35.9% used the mask correctly. Also, the correct use of the mask was slightly higher in men than women, but no significant relationship was observed (P=0.115).
A significant relationship was observed between correct use of the mask and age (P=0.05). The use of shield was more in women. The use of shield was related to sex (P<0.001) (Table 3).
Discussion
This study was conducted to investigate the prevalence of mask use and its types in age groups. The prevalence of face mask use among pedestrians in this study is still lower than Southeastern Iranian population and pedestrians in Hong Kong, Poland, Vermont, India, and the United Arab Emirates. In this study, the prevalence of mask use was higher than pedestrians in Bangkok, Paris and Lima [3, 12-16]. This difference may be due to individuals’ cultural characteristics, beliefs and attitudes. In other words, cultural context plays an essential role in face mask use. Therefore, Sadeqi Arani and Kemmelmeier indicated that the mask use in society is a kind of cultural behavior [17, 18]. Out of the age groups, the elderly used the face mask less than other age groups. The results of this study are inconsistent with the Raihmi research and may be due to differences in sample size and less leaving home by elderly [7]. However, the elderly are vulnerable to infection, hospitalization, and even death from COVID-19. It is essential to pay attention to them until the end of the epidemic. Kwan aimed to explore health beliefs and face mask wearing behaviors among older people and indicated that promoting health beliefs can be a strategy to encourage face mask among the elderly [19]. In this study, the percentage of correct use of the face mask was lower than the results of Rahimi (75.6%) and the studies of Gunasekaran (Malaysia) and CW Tam 2020 (Hong Kong) [7, 13, 15]. Face mask use and its correct use were higher in men than women but statistically no difference was observed between them. Men seem to be more present in public places than women are, while our results are inconsistent with the results of other studies[3, 6, 16]. In this study, the most commonly used face mask were surgical masks which is consistent with the study of Rahimi and Tom [7, 13]. In addition pedestrians aged 30-40 years preferred the surgical mask, and people aged 50-61 years preferred the cloth mask; perhaps the reason is its cost-effectiveness and health reliability [20]. Filtered face mask were also significant among people aged 70 years and older [7]. We found that the pedestrians wore face mask more at 5 PM and 1 PM. Crowds during these hours seem to have affected the behavior of using a respirator. In the present study, shields were very low and were more common among females. Gender differences seem to be effective in preventive behaviors [16]. In our study, the use of face mask was related to age and other demographic variables, which is similar to other studies [2, 7, 16, 21]. Due to the use of the observation method in data collection, we cannot estimate the education and income level variables. The strengths of this study were estimating the prevalence of face mask use over a long period after the COVID-19 pandemic, sampling with a large sample size in 3 cities and use of the observation method that is more accurate than self-reporting.
Conclusion
The prevalence of mask use and its correct use was low among pedestrians. Individual resistances and misconceptions still were observed about using this protection tool. However, health care providers should not be discouraged but should make more efforts to health education, and comprehensive support, setting rules, and supervision can help correct beliefs and encourage the use of face masks until the end of the epidemic and vaccination of a high percentage of the population.
Ethical Considerations
Compliance with ethical guidelines
This research is approved by the Research Ethics Committee of Abadan University of Medical Sciences (Code: IR.ABADANUMS.REC.1400.001). The data collection method was observational and no participants were observed, informed consent was not obtained following the regulations. Material and intellectual rights and information of individuals remain confidential.
Funding
This research was supported by the Deputy for Research, Abadan University of Medical Sciences (Grant No.: 790). As the financial sponsor of this research, the Deputy for Research of Abadan University of Medical Sciences had no role in designing the study, collecting, analyzing, interpreting the data, and writing the article.
Authors' contributions
Conceptualization: Maryam Changizi; Methodology: Maryam Changizi, Bahman Cheraghian and Shokrollah Salmanzadeh; Investigation: Maryam Changizi , Hooshang Mohamadian and Bahman Cheraghian; Data collection: Hooshang Mohamadian and Maryam Changizi; Data analysis: Fatemeh Maqsoodi, Maryam Changizi and Bahman Cheraghian; Writing the original draft: Maryam Changizi; Review and editing: Maryam Changizi and Bahman Cheraghian; Supervision: Maryam Changizi, Hooshang Mohamadian and Sasan Ghorbani Kalkhajeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to all the pedestrians participating in the study and observers of this research.
References
Severe acute respiratory syndrome coronavirus (SARS CoV 2) has affected many people and caused countless deaths. The impact of this disease on welfare, economy, employment, and other aspects of daily life has been observed throughout societies and individuals [1]. Early stages of COVID-19 pandemic, public health messages about wearing face masks use were contradictory and accompanied by various opinions that caused public dissatisfaction and confusion. Finally, the recommendations evolved with scientific understanding [2]. Current strategies, such as physical distance of at least one meter and more, face mask use, and hand washing have been suggested [3]. Data show that wearing a mask protects all people, including healthcare workers and the public, from infection with the virus and can have more benefits [1]. The main advantage of these measures is the reduction of further transmission of the virus and consequently the reduction of adverse outcomes, number of hospitalizations, and deaths [4]. Research has shown that face mask usage reduces the daily growth rate of infection between 47%-70% [5, 6]. A face mask can also reduce the initial risk of respiratory infection by 6%-15% [4]. However, resistance still exists among people to use this tool for personal protection and the use of masks has been reported to be moderate or low among some people [7, 8]. Face masks can vary in terms of filtration efficiency and breathability [9]. In addition, some people found that long-term use of the mask in hot environments is uncomfortable, and covering the nose and mouth may prevent verbal and non-verbal communication [10]. Others also believe that using a face mask is associated with oxygen decrease and prefer not to use it. However, the available data do not support these cases [11]. Iran is also one of the countries with the highest infection and death rates due to COVID-19 [6]. One way to control the coronavirus in Iran is to encourage face mask usage [1]. Therefore, it is necessary to know the prevalence of mask use in some areas. This study was conducted to estimate the prevalence of face mask use among pedestrians in Abadan, Khorramshahr, and Shadegan cities with different characteristics.
Methods
This population-based cross-sectional study was conducted in Abadan, Khorramshahr and Shadgan in southwestern cities of Iran from June to August 2021.
Inclusion criteria
The inclusion criteria included all the pedestrians of determinate neighborhoods in Abadan, Khorramshahr and Shadgan in the southwest cities of Iran.
Exclusion criteria
The exclusion criteria included covering the face with something other than a mask so that the observer cannot recognize the pedestrian’s face mask.
Sample size
The minimum sample size was determined based on the formula to estimate a population proportion in a cross-sectional study with the characteristics of P>0.456, d=0.05, α=0.05 and z=1-α/2 was determined 381 subjects. According to the sampling method and applying the planned effect of 1.5, the minimum sample size was 571 for each region. Due to the unequal size of an area and using a proportional, the final sample size was 6 852. According to the municipal areas the statistical population and measuring the two issues, surely, this number of samples can be representative of measuring southern urban areas.
Accordingly, 34 262 284 and 1 142 people were considered for the urban population of Abadan, Khorramshahr and Shadgan in the southwest cities of Iran. Finally, 7 425 pedestrians were observed in this study, which were 135 clusters of 55 people from 85 urban neighborhoods
Sampling
We employed nine observers with bachelor’s degrees. During two educational sessions, the main researcher trained the observer on how to select subjects and complete the observation checklist. Also, daily monitoring on observer was done by the supervisors. The location of the stations was selected by a purposeful method among the busy passages in Abadan, Khorramshahr and Shadegan neighborhoods. In the last stage, sampling was performed by the non-probability sampling method. In each station, observer, including three men and six women filled out the data. The form contains the studied variables for individual. The observers recorded the variables of gender, age, face mask usage, gloves, shield and type of face mask and correct use of a face mask. Incorrect use of face mask was stated in the checklist with insufficient coverage of the mouth and nose and wearing mask upside down. Observation during busy hours of each area was done from 8:00 AM to 13:00 PM and 17:00.00 PM to 00:00 AM.
Data collection
Data were collected by observation. In this research, a multi-stage sampling method was used. First, cities were divided into several categories based on the division of urban areas. Then in each area according to its population, several observation stations were randomly selected from the list of neighborhoods.
Participants
Pedestrian areas of urban stations determined in the study.
Data analysis
Data were analyzed with WINPEPI (accurate determination of confidence interval) and software, version 26. We used descriptive tests (reporting gender, age and sex, use of masks, etc.). The prevalence rate was estimated with a 95% confidence interval (95% CI), chi-square (the relationship between gender and the use of face masks), and Fisher’s exact tests. The Statistical significance was acceptable if P<0.05. The normality of the data was checked by the Kolmogorov-Smirnov test.
Results
A total number of 7425 pedestrians were assessed in this study. Most pedestrians observed were in the age group of 21-30 years (23.7%). Most subjects were men 4115(55.4%). Among the pedestrians, 3997(53.8%) people used facemasks. Table 1 presents demographic characteristic of pedestrians and preventive behaviors.
The prevalence of facemask usage was 53.7% (95% confidence interval [95% CI, 52.7%, 55.0%). The highest prevalence of mask use was observed in the age group of 31-40 years (59.8%) and the lowest in the age group of 70 years and older (44.7%). In the present study, usage masks among men more than women (54.3% vs 53.0%). The prevalence of mask use was the highest in Abadan City and it was the lowest in Khorramshahr City. The most commonly used mask among pedestrians was the surgical mask (37.1%) and the lowest were filtered mask (2%). The usage of filter masks was higher among the age group of 10-20 years (2.6%). The most common use of surgical masks was in the age group of 21-30 years (40.9%). Older people aged 61-70 used more cloth masks than others (15.4%). The use of masks was more in the morning and at night (25.4% vs 24.5%, P<0.001). The usage face mask and type of it was related to the age of pedestrians (P<0.001). No relationship was found between gender and mask use and mask type (P=0.05). Pedestrians observation were at 9-10 AM (23.7%), 11 AM (13.4%) and 8 PM (11.6%). Pedestrians usage of face mask was related to observation times (P<0.001). Pedestrians in the age group of 21-30 years, 26.67% more used face masks correctly (Table 2).
In the present study, only 35.9% used the mask correctly. Also, the correct use of the mask was slightly higher in men than women, but no significant relationship was observed (P=0.115).
A significant relationship was observed between correct use of the mask and age (P=0.05). The use of shield was more in women. The use of shield was related to sex (P<0.001) (Table 3).
Discussion
This study was conducted to investigate the prevalence of mask use and its types in age groups. The prevalence of face mask use among pedestrians in this study is still lower than Southeastern Iranian population and pedestrians in Hong Kong, Poland, Vermont, India, and the United Arab Emirates. In this study, the prevalence of mask use was higher than pedestrians in Bangkok, Paris and Lima [3, 12-16]. This difference may be due to individuals’ cultural characteristics, beliefs and attitudes. In other words, cultural context plays an essential role in face mask use. Therefore, Sadeqi Arani and Kemmelmeier indicated that the mask use in society is a kind of cultural behavior [17, 18]. Out of the age groups, the elderly used the face mask less than other age groups. The results of this study are inconsistent with the Raihmi research and may be due to differences in sample size and less leaving home by elderly [7]. However, the elderly are vulnerable to infection, hospitalization, and even death from COVID-19. It is essential to pay attention to them until the end of the epidemic. Kwan aimed to explore health beliefs and face mask wearing behaviors among older people and indicated that promoting health beliefs can be a strategy to encourage face mask among the elderly [19]. In this study, the percentage of correct use of the face mask was lower than the results of Rahimi (75.6%) and the studies of Gunasekaran (Malaysia) and CW Tam 2020 (Hong Kong) [7, 13, 15]. Face mask use and its correct use were higher in men than women but statistically no difference was observed between them. Men seem to be more present in public places than women are, while our results are inconsistent with the results of other studies[3, 6, 16]. In this study, the most commonly used face mask were surgical masks which is consistent with the study of Rahimi and Tom [7, 13]. In addition pedestrians aged 30-40 years preferred the surgical mask, and people aged 50-61 years preferred the cloth mask; perhaps the reason is its cost-effectiveness and health reliability [20]. Filtered face mask were also significant among people aged 70 years and older [7]. We found that the pedestrians wore face mask more at 5 PM and 1 PM. Crowds during these hours seem to have affected the behavior of using a respirator. In the present study, shields were very low and were more common among females. Gender differences seem to be effective in preventive behaviors [16]. In our study, the use of face mask was related to age and other demographic variables, which is similar to other studies [2, 7, 16, 21]. Due to the use of the observation method in data collection, we cannot estimate the education and income level variables. The strengths of this study were estimating the prevalence of face mask use over a long period after the COVID-19 pandemic, sampling with a large sample size in 3 cities and use of the observation method that is more accurate than self-reporting.
Conclusion
The prevalence of mask use and its correct use was low among pedestrians. Individual resistances and misconceptions still were observed about using this protection tool. However, health care providers should not be discouraged but should make more efforts to health education, and comprehensive support, setting rules, and supervision can help correct beliefs and encourage the use of face masks until the end of the epidemic and vaccination of a high percentage of the population.
Ethical Considerations
Compliance with ethical guidelines
This research is approved by the Research Ethics Committee of Abadan University of Medical Sciences (Code: IR.ABADANUMS.REC.1400.001). The data collection method was observational and no participants were observed, informed consent was not obtained following the regulations. Material and intellectual rights and information of individuals remain confidential.
Funding
This research was supported by the Deputy for Research, Abadan University of Medical Sciences (Grant No.: 790). As the financial sponsor of this research, the Deputy for Research of Abadan University of Medical Sciences had no role in designing the study, collecting, analyzing, interpreting the data, and writing the article.
Authors' contributions
Conceptualization: Maryam Changizi; Methodology: Maryam Changizi, Bahman Cheraghian and Shokrollah Salmanzadeh; Investigation: Maryam Changizi , Hooshang Mohamadian and Bahman Cheraghian; Data collection: Hooshang Mohamadian and Maryam Changizi; Data analysis: Fatemeh Maqsoodi, Maryam Changizi and Bahman Cheraghian; Writing the original draft: Maryam Changizi; Review and editing: Maryam Changizi and Bahman Cheraghian; Supervision: Maryam Changizi, Hooshang Mohamadian and Sasan Ghorbani Kalkhajeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to all the pedestrians participating in the study and observers of this research.
References
- Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person -person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet. 2020; 395(10242):1973-87. [DOI:10.1016/S0140-6736(20)31142-9] [PMID]
- Picard J, Cornec G, Baron R, Saliou P. Wearing of face masks by healthcare workers during COVID-19 lockdown: What did the public observe through the French media? The Journal of Hospital Infection. 2020; 106(3):617-20. [DOI:10.1016/j.jhin.2020.08.009] [PMID]
- Beckage B, Buckley TE, Beckage ME. Prevalence of face mask wearing in Northern Vermont in response to the covid-19 pandemic. Public Health Reports (Washington, DC: 1974). 2021; 136(4):451-6. [DOI:10.1177/00333549211009496] [PMID]
- Brainard J, Jones NR, Lake IR, Hooper L, Hunter PR. Community use of face masks and similar barriers to prevent respiratory illness such as COVID-19: A rapid scoping review. Euro surveillance: Bulletin Europeen sur les Maladies Transmissibles, European Communicable Disease Bulletin. 2020; 25(49):2000725. [DOI:10.2807/1560-7917.ES.2020.25.49.2000725] [PMID]
- Mitze T, Kosfeld R, Rode J, Wälde K. Face masks considerably reduce COVID-19 cases in Germany. Proceedings of the National Academy of Sciences of the United States of America. 2020; 117(51):32293-301. [DOI:10.1073/pnas.2015954117] [PMID]
- Li Y, Liang M, Gao L, Ayaz Ahmed M, Uy JP, Cheng C, et al. Face masks to prevent transmission of COVID-19: A systematic review and meta-analysis. American Journal of Infection Control. 2021; 49(7):9006. [DOI:10.1016/j.ajic.2020.12.007] [PMID]
- Rahimi Z, Shirali GA, Araban M, Mohammadi MJ, Cheraghian B. Mask use among pedestrians during the COVID-19 pandemic in Southwest Iran: An observational study on 10,440 people. BMC Public Health. 2021; 21(1):133. [DOI:10.1186/s12889-020-10152-2] [PMID]
- Liang M, Gao L, Cheng C, Zhou Q, Uy JP, Heiner K, et al. Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. Travel Medicine and Infectious Disease. 2020; 36:101751. [DOI:10.1016/j.tmaid.2020.101751] [PMID]
- Rassouli M, Ashrafizadeh H, Shirinabadi Farahani A, Akbari ME. COVID-19 Management in Iran as one of the most affected countries in the world: Advantages and weaknesses. Frontiers in Public Health. 2020; 8:510. [DOI:10.3389/fpubh.2020.00510] [PMID]
- Yaqoob S, Saleem A, Jarullah FA, Asif A, Essar MY, Emad S. Association of acne with face mask in healthcare workers amidst the covid-19 outbreak in Karachi, Pakistan. Clinical, Cosmetic and Investigational Dermatology. 2021; 14:1427-33. [DOI:10.2147/CCID.S333221] [PMID]
- Samannan R, Holt G, Calderon-Candelario R, Mirsaeidi M, Campos M. Effect of face masks on gas exchange in healthy persons and patients with chronic obstructive pulmonary disease. Annals of the American Thoracic Society. 2021; 18(3):541-4. [DOI:10.1513/AnnalsATS.202007-812RL] [PMID]
- Khosravi M, Amali M, Jalili F, Ghiasi Z. Prevalence and associated factors of personal protective measures among the Southeastern Iranian Population During the COVID-19 Pandemic. Electronic Journal of General Medicine. 2022; 19(3):em367. [DOI:10.29333/ejgm/11833]
- Tam VC, Tam SY, Poon WK, Law HKW, Lee SW. A reality check on the use of face masks during the COVID-19 outbreak in Hong Kong. EClinicalMedicine. 2020; 22:100356. [DOI:10.1016/j.eclinm.2020.100356] [PMID]
- Ganczak M, Pasek O, Duda-Duma Ł, Świstara D, Korzeń M. Use of masks in public places in Poland during SARS-Cov-2 epidemic: A covert observational study. BMC Public Health. 2021; 21(1):393. [DOI:10.1186/s12889-021-10418-3] [PMID]
- Gunasekaran GH, Gunasekaran SS, Gunasekaran SS, Zaimi NS, Abdul Halim NAB. Prevalence of facemask use among general public when visiting wet market during COVID-19 pandemic: An observational study. medRxiv. 2020. [DOI:10.1101/2020.05.17.20105023]
- Elachola H, Ebrahim SH, Gozzer E. COVID-19: Facemask use prevalence in international airports in Asia, Europe and the Americas, March 2020. Travel Medicine and Infectious Disease. 2020; 35:101637. [DOI:10.1016/j.tmaid.2020.101637] [PMID]
- Sadeqi Arani Z. [Predicting the use of masks in the covid-19 based on the systems thinking, personal - social responsibility, moral obligations and individualism: An approach of consumer behavior theory (Persian)]. Iranian Journal of Medical Ethics and History of Medicine. 2021; 14:174-87. [Link]
- Kemmelmeier M, Jami WA. Mask wearing as cultural behavior: An investigation across 45 U.S. States during the covid-19 pandemic. Frontiers in Psychology. 2021; 12:648692. [DOI:10.3389/fpsyg.2021.648692] [PMID]
- Kwan RYC, Lee PH, Cheung DSK, Lam SC. Face mask wearing behaviors, depressive symptoms, and health beliefs among older people during the covid-19 pandemic. Frontiers in Medicine. 2021; 8:590936. [DOI:10.3389/fmed.2021.590936] [PMID]
- Leffler CT, Ing E, Lykins JD, Hogan MC, McKeown CA, Grzybowski A. Association of country-wide coronavirus mortality with demographics, testing, lockdowns, and public wearing of masks. The American Journal of Tropical Medicine and Hygiene. 2020; 103(6):2400-11. [DOI:10.4269/ajtmh.20-1015] [PMID]
- Nemat A, Asady A, Raufi N, Zaki N, Ehsan E, Noor NAS, et al. A survey of the healthcare workers in Afghanistan during the COVID-19 Pandemic. The American Journal of tropical Medicine and Hygiene. 2020; 104(2):537-9. [DOI:10.4269/ajtmh.20-1367] [PMID]
Type of Study: Orginal Article |
Subject:
● Disease Control
Received: 2022/12/2 | Accepted: 2023/07/4 | Published: 2024/03/1
Received: 2022/12/2 | Accepted: 2023/07/4 | Published: 2024/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
