

Volume 13, Issue 4 (Jul & Aug 2023)
J Research Health 2023, 13(4): 291-302 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khorasani-Zavareh D, Dehghani Tafti A, Nasiriani K, Hajimaghsoudi M, Fallahzadeh H, Eftekhari A. Development and Psychometric Evaluation of Traffic-related Pre-hospital Mortality Prevention Questionnaire. J Research Health 2023; 13 (4) :291-302
URL: http://jrh.gmu.ac.ir/article-1-2207-en.html
URL: http://jrh.gmu.ac.ir/article-1-2207-en.html
Davoud Khorasani-Zavareh1 

 , Abbasali Dehghani Tafti2 , Khadijeh Nasiriani3 , Majid Hajimaghsoudi4 , Hossien Fallahzadeh5 , Adel Eftekhari6
, Abbasali Dehghani Tafti2 , Khadijeh Nasiriani3 , Majid Hajimaghsoudi4 , Hossien Fallahzadeh5 , Adel Eftekhari6
, Abbasali Dehghani Tafti2 , Khadijeh Nasiriani3 , Majid Hajimaghsoudi4 , Hossien Fallahzadeh5 , Adel Eftekhari6
1- Safety Promotion and Injury Prevention Research Center, Department of Health in Emergencies and Disasters, School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Department of Neurobiology, Care Sciences and Society (NVS), H1, Division of Family Medicine and Primary Care, Huddinge, Sweden.
2- Department of Health Education and Promotion, School of Public Health, Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran
3- Department of Nursing, Research center for Nursing and Midwifery care, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
4- Clinical Research Development Center, Shahid Rahnemoon Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5- Department of Biostatistics and Epidemiology, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
6- Department of Nursing, Meybod School of Nursing, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,adel.eftekhari.66@gmail.com
2- Department of Health Education and Promotion, School of Public Health, Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran
3- Department of Nursing, Research center for Nursing and Midwifery care, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
4- Clinical Research Development Center, Shahid Rahnemoon Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5- Department of Biostatistics and Epidemiology, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
6- Department of Nursing, Meybod School of Nursing, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,
Full-Text [PDF 664 kb]
(995 Downloads)
| Abstract (HTML) (4093 Views)
Full-Text: (951 Views)
1. Introduction
Mortality related to traffic accidents is one of the current challenges worldwide imposing a lot of costs on the economy of countries [1, 2]. Comparatively, more than 90% of deaths due to traffic accidents occur in low- and middle-income countries [3]. According to estimates based on the death time of the casualties, 80% of these deaths occur in the pre-hospital phase [4].
According to the studies and predictions, pre-hospital care is vital in the effective management of these deaths to provide higher quality care and reduce injuries and death of casualties [5]; therefore in the case of traffic accident management and provision of comprehensive and timely services in the pre-hospital stage, at least 39% of these deaths are potentially preventable [6].
The system of providing pre-hospital services includes elements, such as information provision, casualty transfer, routing, composition and type of specialty of manpower in ambulances, and communication devices, such as wireless, etc. [7]. If all the factors involved in pre-hospital emergency care are properly considered, a lot of mortalities occurring in this phase will be prevented. In most studies on traffic accident mortality, systemic factors, managerial factors, technical defects, delay in diagnosis, and misdiagnosis have been identified as factors influencing preventable deaths [8, 9, 10, 11].
Iran is one of the countries where the highest number of accidents and traffic-related deaths are reported [12]. According to the latest statistics published by forensic medicine, traffic accidents in Iran annually lead to the death of nearly 17,000 people and permanent injury or disability of 300,000 people [13]. According to some reports, 57% of deaths due to traffic accidents in Iran occur in the pre-hospital stage, which is a significant percentage [14].
One of the critical challenges in investigating the preventable deaths of traffic accidents in the pre-hospital stage is the lack of appropriate measurement methods to assess it, i.e. a shortage that is considered a major vacuum in Iran. Measurement of the components affecting preventable deaths in traffic accidents, which is considered one of the critical and vital steps in research, requires the use of appropriate instruments [15]. To achieve this goal, either new instruments should be developed or the available instrument developed abroad should be used after ensuring their validity, reliability, and psychometric properties.
According to the search performed, instruments are available in the field of preventable traffic-related deaths, but because healthcare systems and service conditions are not the same in different countries, and in addition, different Angelo-American and Franco-German structures of pre-hospital systems exist in countries, thus, their full application in translation is not possible [16].
Regarding the importance of the analysis of preventable deaths and the components affecting it, and considering the limited studies in this field in other countries, and especially its absence in the Eastern Mediterranean and Asian countries, this study was conducted to develop and psychometrically evaluate a traffic-related pre-hospital mortality prevention questionnaire (TPMPQ).
2. Methods
The present study was conducted to develop and psychometrically evaluate an instrument to measure traffic-related pre-hospital preventable deaths in Iran in 2019-2020. This study used a mixed quantitative-qualitative design, including a systematic review, qualitative study of conventional content analysis type, Delphi study, and methodology. Instrument items were designed in the qualitative stage and psychometrically assessed in the quantitative stage.
Systematic Review Phase: In the systematic review phase, all factors affecting preventable mortality were identified based on search in databases of Web of Science (WoS), Scopus, PubMed, and Google Scholar, and then similar cases were either merged or deleted. To critically evaluate the articles, the research team evaluated the quality of all components of the articles using the critical appraisal skills programme (CASP) as an instrument to measure paper quality. Finally, the remaining content was classified into 3 main categories and 6 subcategories. Based on the findings of the study, three main categories, including “systemic defects, human errors, and the patient’s clinical condition” were extracted from codes in the systematic review stage.
Qualitative Interviews: Unstructured qualitative interviews were conducted with 26 participants who were selected by purposive sampling using the opinion of experts and specialists in this field. The interviewees included 26 people with an age range of 31-55 years. They had at least 5 years of work experience in traffic accident management, road traffic police, Red Crescent, fire brigade, technicians and pre-hospital emergency staff, emergency medicine specialists, and emergency department nurses. Four traffic accident victims were interviewed. Expert sampling was performed using purposive sampling until data saturation was achieved. After verbatim transcription of the interviews, they were imported into MAXQDA10 to classify the extracted codes. Subsequently, the main categories and subcategories were inductively extracted from the data.
Delphi: By combining the results of the systematic review [17] and qualitative interviews [18], the primary instrument was finally developed to use in Delphi rounds. In the Delphi stage, the study population included experts in the field of traffic accidents and pre-hospital emergencies at the macro and national levels. Three group discussions of the research team were held to summarize the extracted components. Ultimately, the 5-point Likert instrument was developed (strongly agree to strongly disagree) and entered the second round of Delphi. In the second round, the initial instrument designed in a focus group session was investigated for four hours with 15 experts in the field of traffic accidents. Moreover, an email was sent to 10 national experts of traffic accidents. After completing the instrument, the items that received an average of 2.5 and above entered the third round of Delphi. Besides, the answers to the open-ended items were examined with the research team and their opinions were applied in the form of editing the items of the instrument. In the third round, the remaining items from the second round were sent to 25 experts in the form of instruments to receive for and against comments. Of these, 22 instruments were returned, and finally, the items with a %75+ of the agreement were accepted.
Psychometric Evaluation: After extracting the items obtained from the Delphi method, to determine their face and content validity, the opinions of experts were collected. The target population in the psychometric phase also included subject matter experts, technicians, and prehospital emergency supervisors.
Face Validity: Qualitative and quantitative methods were used to establish face validity. To determine the qualitative face validity, 10 pre-hospital emergency technicians and supervisors were asked to comment on the fluency, clarity, and comprehensibility of the components and the need for removing or integrating the instrument components. After modifying the required items, the quantitative method of item impact (impact score = Frequency (%) × Importance) was used to determine the importance of each phrase. In this method, the five-point Likert scale was considered, quite important = 5, somewhat important = 4, moderately important = 3, slightly important = 2, and not important at all = 1. If the impact score was considered equal to or greater than 1.5, the phrase was deemed appropriate for subsequent analyses.
Content Validity: Two qualitative and quantitative methods were used to determine the content validity. In this study, content validity was determined based on experts’ judgments. In the qualitative method of determining content validity, the experts reviewed the items, and the necessary corrections were applied to them. To determine content validity by quantitative method, content validity ratio (CVR) and content validity index (CVI) were used. To determine the content validity ratio quantitatively, at least 10 experts were asked to respond to each of the instrument items in the range of “necessary, useful but not necessary, and not necessary”. An item score higher than 0.79 was rendered acceptable. Based on the Lawshe’s (1975) table, the minimum content validity ratio value was determined and the content validity ratio for all items was calculated using the following formula [19].
To calculate the content validity index, the experts commented on the three criteria of relevance or specificity, simplicity and fluency, and clarity or transparency based on the four-point Likert scale. A score higher than 0.79 was considered sufficient for accepting the items. Options included the following:
Not relevant=1, relatively relevant=2, relevant=3, fully relevant=4.
The method of item score calculation was such that the evaluators who gave three or four points to the items were divided by the total evaluators [20].
Reliability: The internal consistency coefficient was used to evaluate the reliability of the instrument in the present study. To determine internal consistency, Cronbach’s α was calculated for the whole instrument and its subscales. A total of 20 psychometrically finalized instruments were completed by the technicians present at the scene of the traffic accident and then Cronbach’s α was measured using SPSS software, version 22. Cronbach’s α above 0.7 was considered satisfactory for internal consistency [21]. The closer it is to 1, the more reliable it is.
3. Results
Systematic review
Initially, in the systematic review phase, 7247 papers were obtained from the mentioned databases. In addition, 1902 duplicated papers were excluded. A total of 5 355 titles and abstracts were examined and 218 full-text papers were explored of which, 12 were finalized for analysis. The rest of the papers were omitted because they were irrelevant or did not observe the inclusion criteria. Two more articles entered the study after examining the reference lists. Ultimately, 14 relevant papers were analyzed. Evaluation of the studies resulted in the production of three main categories, “systemic defects, human errors, and the patient’s clinical condition”. Seven subcategories also emerged. (The article of the systematic review stage was published in Trauma Monthly journal) [17].
Qualitative interviews
Based on the demographic information of the interviews in the qualitative interviews, 13 people (54%) were in the age group of 40-50 years, 15 people (63%) were men, 15 people (62%) were specialists/doctors and 17 people (71%) had a work experience of more than 15 years.
The participants’ experiences showed that considering things, such as accurate clinical assessment of the victim at the scene, appropriate quality care, legal guarantee, and necessary protocols, coordination of the involved organizations, and complete management of the accident scene through the incident commander and creating the highest level of scene safety in preventing pre-hospital deaths is effective.
In the qualitative interviews, six main categories were extracted as the major challenges of preventable deaths in road traffic injuries in the pre-hospital phase, including “poor management of the crash scene” with two subcategories of lack of rapid access to the patient and lack of scene safety, “lack of adequate rules and regulations” with two subcategories of lack of protocols and guidelines and lack of clear duties checklists, “poor management of time” with two subcategories of elongated response time at the crash scene and elongated time of victim transport, “low quality of training” with two subcategories of insufficient training of emergency medical services (EMS) staff and inadequate public training, “poor communication and coordination” with two subcategories of poor communication of EMS staff and lack of uniform commandership at the crash scene, and “low quality of victim management” with two subcategories of low quality of clinical care and lack of accurate clinical assessment (the article of the qualitative stage was published in archives of academic emergency medicine journal) [18].
Delphi
After integrating and classifying the results of the systematic review and qualitative interviews, an instrument consisting of 71 items was used in the initial round of Delphi. After analyzing the items using the average score based on the Likert scale from the first round, the instrument entered the third round of Delphi with 44 items, and finally in the third round, out of 44 items from the second round, 39 items with 75+% agreements were selected as the final items.
Psychometric Evaluation: In the first stage of face validity review, according to the opinions of emergency medical experts and technicians, the wording of six components was corrected, and since the impact score of all components was more than 1.5, no components were removed in the face validity stage. In the content validity stage, out of 39 components, 4 components with CVR of less than 0.6 were removed and the total components was reduced to 35. In the next stage, the CVI of no component was less than 0.79 and thus, no component was removed at this stage. The reliability of all items was above 0.7, and the final reliability was 0.84 (Table 1).
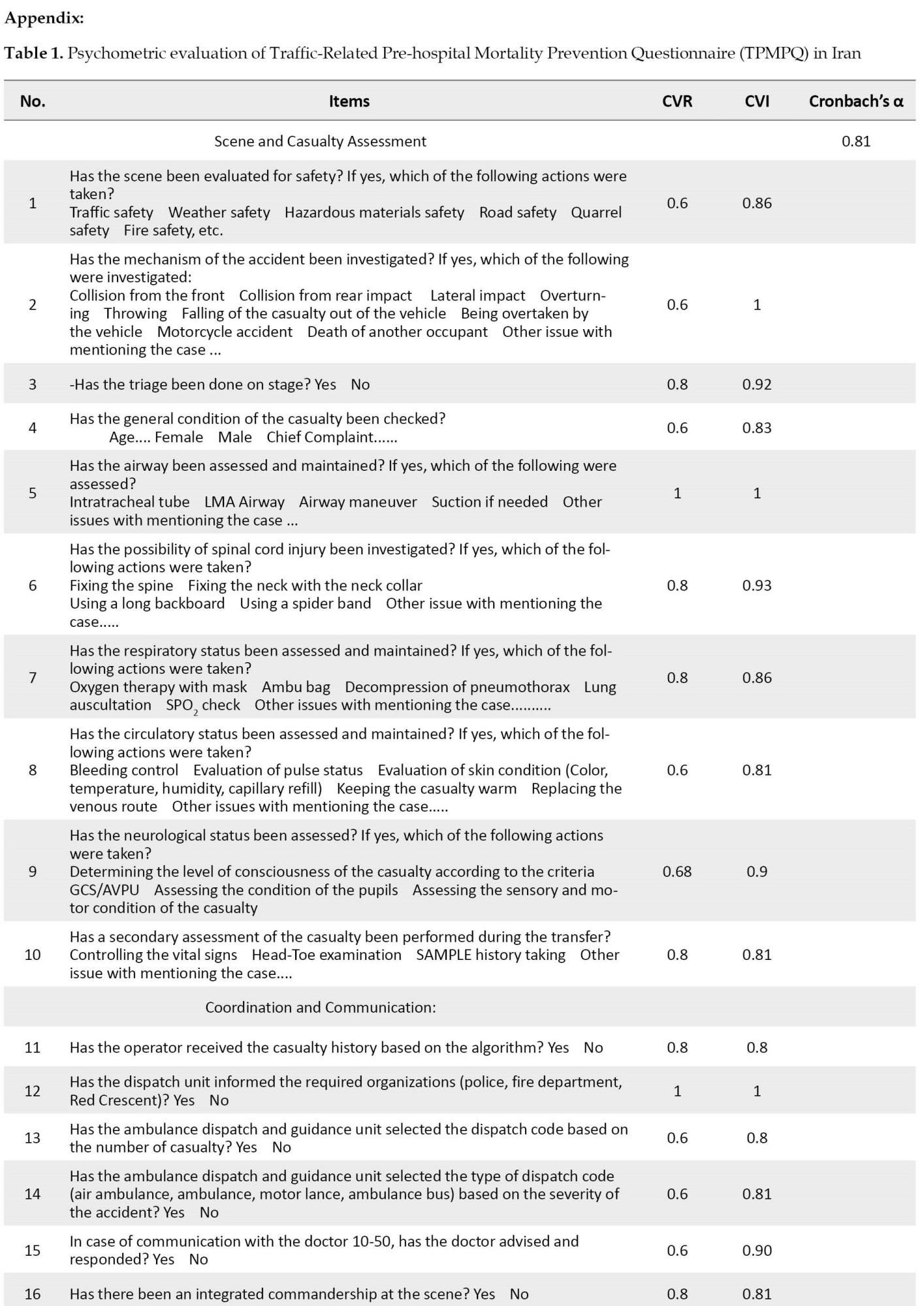
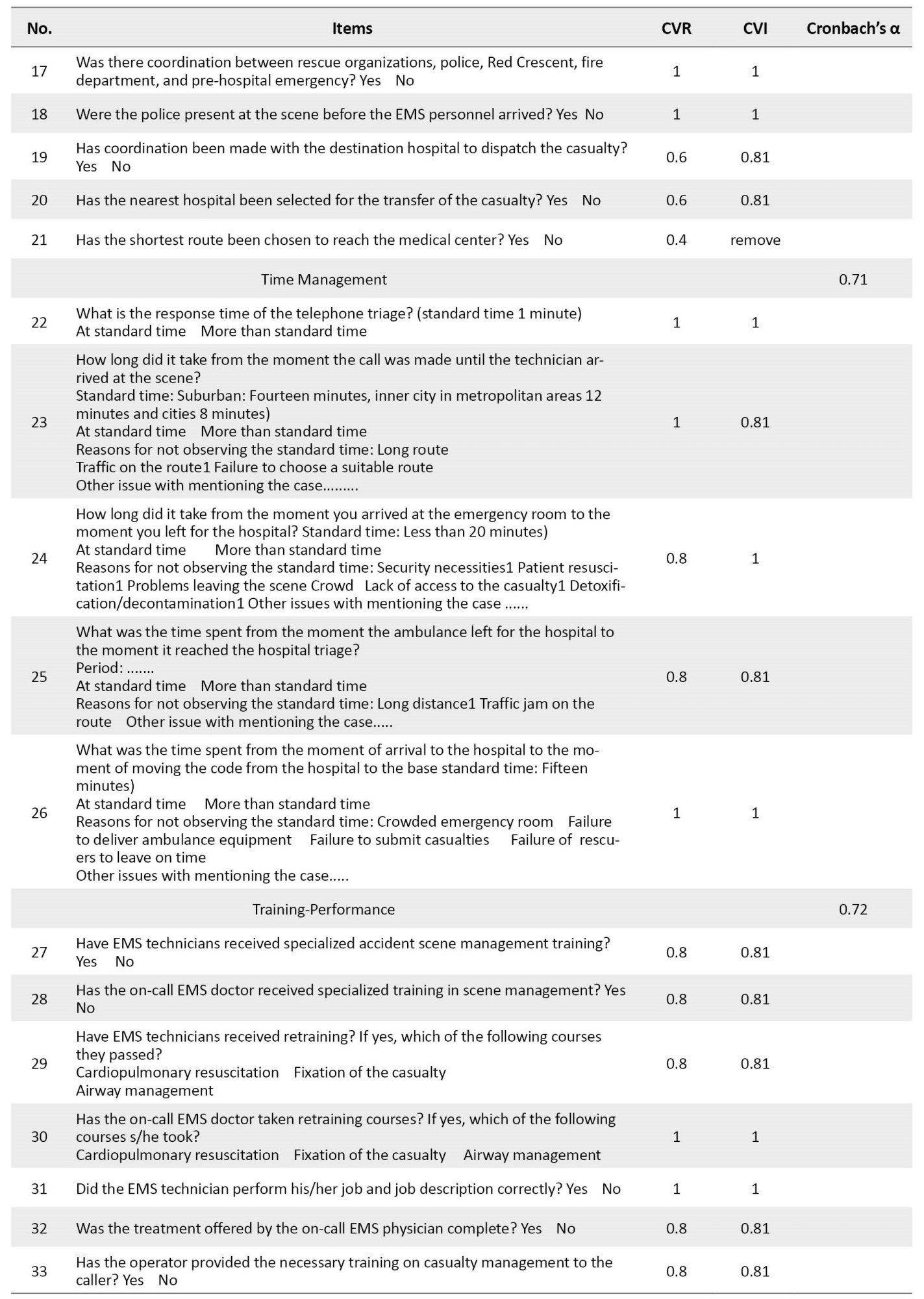
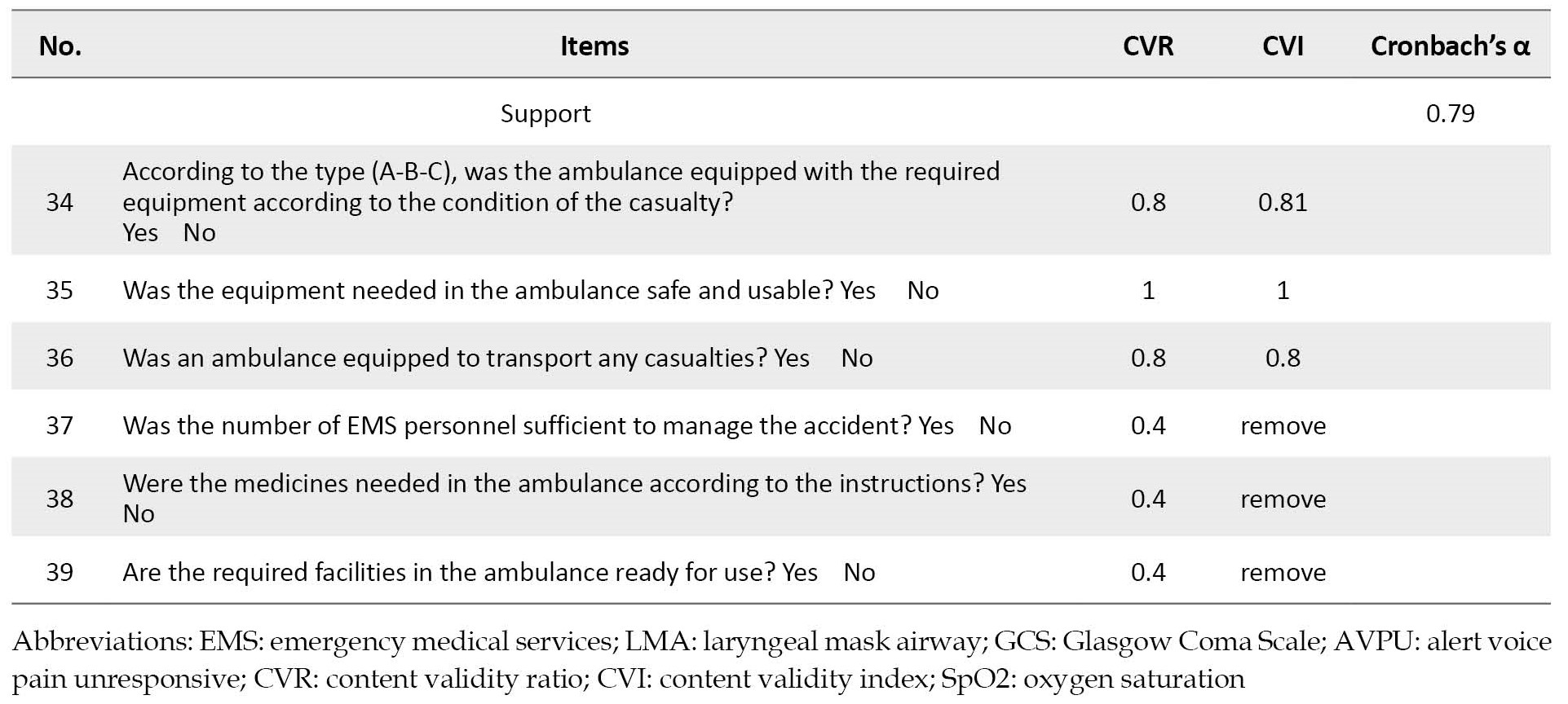
Finally, the instrument: Traffic-related pre-hospital mortality prevention questionnaire (TPMPQ) was approved after removing items 21, 37, 38, and 39 with 35 items and five dimensions.
4. Discussion
The present study was conducted using a mixed method for the first time by integrating systematic review, qualitative study, and Delphi study in 3 stages. The instrument developed in this study has high validity and reliability because, at each stage of validation, the experts’ opinions in instrument correction were considered and applied.
According to the first component in the present study, the assessment of trauma emergencies in various incidents includes scene assessment and casualty assessment. In assessing pre-hospital trauma casualties according to the pre-hospital trauma life support (PHTLS) guidelines, examining the scene, the mechanism of injury, and the primary and secondary assessment of the casualty are among the necessary factors that must be performed correctly [22]. Scene assessment means trying to establish scene security and paying close attention to the true nature of the situation. The primary assessment of the casualty also means that after an overview of the patient in terms of age, observations, and chief complaint, operations should be performed thoroughly, including assessment of the airway, spine and cervical vertebrae, respiratory status, blood circulation, and neurological status according to emergency technicians [23].
The efficiency and efficacy of medical care at the scene of an accident require the presence of paramedics and rescuers who can initially assess the scene and the condition of the casualty and have enough experience to make the right decision to reduce a significant proportion of prehospital mortality. After the initial assessment and ensuring that the casualty is not seriously threatened, a secondary assessment should be performed, which includes controlling vital signs, taking a medical history, and examining the casualty. This indicates the need for more attention from prehospital emergency officials to the method of emergency medical personnel about neurological examinations of trauma victims, especially cervical trauma and multiple trauma at the scene, and immobilization of cervical vertebrae using the cervical collar to prevent the formation or spread of spinal cord injuries. The results of a prospective study conducted by Fredø et al. in Norway showed that in 68% of trauma patients transferred to medical centers by the prehospital emergency, a cervical collar was used for immobilization, and in 5%, no therapeutic intervention was performed [24].
Taking a correct medical history is one of the effective factors in the second assessment of the casualty. According to experts, it was one of the cases with a high agreement coefficient and is vital in the quality of clinical services of emergency medical centers. In one study aimed at analyzing the causes of medical history errors in patients hospitalized in Iran’s pre-hospital emergency centers, 8 causes were stated as the reasons for not taking a proper history in the pre-hospital phase, “lack of sufficient knowledge, lack of ability to structure the history, inattention, poor communication with the patient, lack of motivation, lack of communication and adequate time, and inadequate environment” [25].
Weakness in scene management is rendered as another crucial and influential challenge in preventable deaths in the findings of the present study. In the present study, one of the effective challenges to death due to traffic accidents was the delay in the access to the casualty in the scene, which is influenced by factors, such as crowds or pile-ups in the scene and the lack of open access to the casualty. In a study conducted to improve the provision of pre-hospital emergency services, people’s interventions on the scene were expressed as effective factors in controlling or facilitating preventive care against traffic accidents [26]. In a study conducted to examine pre-hospital services in the developed and developing countries, the presence of people on the scene due to personal curiosity, eagerness for humanitarian aid, excitement, and rushing in the scene were expressed as factors leading to the crowded scene and poor communication [27]. Some studies have shown that the irrational gathering of people and pile-up at the scene of an accident is one of the factors fostering the weakness of the process of helping victims of traffic accidents and reducing the security of the scene [28, 29, 30].
Lack of communication and coordination is one of the intervening challenges in preventable deaths. The research findings also confirmed its significant effects. Proper communication and coordination can increase the readiness to provide pre-hospital care [31, 32]. The research results related to the challenge of managing the scene of traffic accidents in Iran also showed that the involvement of non-specialists, lack of coordination and cooperation, inadequate prehospital services, and defects in infrastructures have been among the causes of pre-hospital mortality [33].
Depending on the type of traffic accident, different organs are present on the scene and there should be a comprehensive system with powerful management and a single unit as a commander to coordinate the scene. The accident commander must act in such a way that he actively manages the accident scene and the resulting crowd throughout the accident until the accident returns to its original state. The police have been introduced as the coordinating organ at the scene of accidents to manage the scene of road accidents and the factors affecting the management of the scene of the accident [34, 35]. The commander of the accident may be different depending on the type of accident, but what is crucial is that due to the existence of different organs, the commander of the accident can be determined depending on the type of accident by developing the necessary processes and instructions.
Another effective factor in the coordination and communication subset is the early coordination with the hospital for transferring the casualty. In a study aimed at investigating the nature of pre-hospital medical interventions conducted in Tabriz Province, Iran, almost all casualties were transferred to the hospital without coordination with the receiving hospital. Considering that coordination, before the casualty arrives at the hospital, prepares the members of the treatment team to provide the desired services to the casualty, thus, this issue requires serious attention to improve communication in the pre-hospital stage between the casualty transfer team and medical centers [36]. According to the research, to investigate response time and delay consequences in EMS missions in Shiraz City, Iran, the following were suggested to reduce the response time of pre-hospital emergencies, “familiarity of technicians with peripheral routes and shortcuts, use of satellite systems, radar and automatic radio system (Trunking) to find the best and most appropriate way in case of emergency, educating people via the media to work with the EMS and give way to ambulances, considering special lanes for ambulances on busy streets, and using alternatives, such as motor lances on old or busy roads [37]. Familiarity of emergency technicians with peripheral routes and shortcuts, the use of satellite systems, radar, global positioning system (GPS), and high-frequency waves to find the best and most appropriate way in emergencies, are among the helpful solutions in this field [37].
In addition to teaching the management skills required by rescue personnel, operational training necessary to provide services on the scene is emphasized. In the research conducted to assess the educational needs of EMS technicians, most technicians referred to drug information and possible side-effects of their use in the dimension of knowledge, ability, and capacity in inserting endotracheal tubes in skill dimension, and professional interest in participating in in-service training courses to improve their academic level in the field of practical skills in attitude dimension [38]. Special pre-hospital emergency work topics, such as scene assessment, identifying the tasks of emergency workgroups, identifying patient assessment components, and triage should be included in the curriculum for students in areas that can potentially be considered rescue personnel (such as nursing or emergency medicine). Pre-hospital instant care (PHIC), prehospital trauma life supports (PHTLS), and basic cardiopulmonary resuscitation (BCPR) courses are specifically among the essential courses for pre-hospital care providers in different countries [3].
Based on the results of the present study, educating people about first aid will also be a great asset in diminishing deaths on the scene. Training should be based on the specific needs of communities and available resources. Besides, the training method should be simple and local about the transfer of vital skills to trainees in scene management, bleeding control, primary cardiopulmonary resuscitation, lifting and transfer of open fractures, and triage. Acquiring these skills by these people is effective as efficient first aid in the absence of trained healthcare professionals immediately after a traffic accident. Furthermore, educating people on the scene, the police, and acquiring first aid training skills to help improve patient’s outcomes in the pre-hospital phase are also identified as the effective factors [40, 41].
Adequate and sufficient equipment is one of the effective support components in fostering the goals of any system. The study conducted by Vaitkaitis, which examined the most acute problems in EMS in Lithuania, showed that the obsolescence and oldness of existing ambulances and the lack of integrated standards for medical education and treatment as influential components led to poor performance of medical services in the country [42].
5. Conclusion
The results of the present study revealed that the instrument developed with the dimensions of “scene and casualty assessment, coordination and communication, time management, training performance, and support” has acceptable validity and reliability to measure traffic-related pre-hospital preventable mortality. This instrument can measure the factors affecting the preventable deaths in the traffic accidents. By rendering preventable mortality as a measurable variable, it can serve as an effective instrument. Numerous factors at the managerial and therapeutic levels are crucial in reducing the preventable deaths due to traffic accidents in the pre-hospital phase. By identifying and planning for proper preparation or appropriate response in the scene, giant strands can be taken in this regard. Empowering the management of preventable deaths due to traffic accidents, accurate clinical assessments for the casualty at the scene without any negligence, providing quality and accurate services, coordinating the organs involved in defining the job description of each organ, complete accident scene management with integrated commandment approach and creating the highest security in the scene are necessary measures. Moreover, they also mentioned that the authorities should consider increasing the scientific and practical skills of the rescue personnel and the training of first aid for the people present on the scene.
The main limitation of this study is the lack of construct validity, which requires sampling and factor analysis to determine the sub-structures of the tool.
Ethical Considerations
Compliance with ethical guidelines
This article is approved by the Ethics Committee at Shahid Sadoughi University of Medical Sciences with the code: IR.SSU.SPH.REC.1397.038 dated 18.6.2018.
Funding
The paper was extracted from the doctoral thesis of Adel Eftekhari, Department of Nursing, Meybod School of Nursing, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Authors' contributions
Participating in the initial design of the study: Adel Eftekhari, Davood Khorasani, Abbas Ali Dehghani, and Khadijeh Nasiriani; Data collection and interviews: Adel Eftekhari, Davood Khorasani, Majid Haji Maghsoudi, and Khadijeh Nasiriani; Interviews and data analysis: Adel Eftekhari, Khadijeh Nasiriani, Davood Khorasani, and Hossein Fallahzadeh; Writing of the article and its content: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the experts and professionals who took the time for the interviews.
References
Mortality related to traffic accidents is one of the current challenges worldwide imposing a lot of costs on the economy of countries [1, 2]. Comparatively, more than 90% of deaths due to traffic accidents occur in low- and middle-income countries [3]. According to estimates based on the death time of the casualties, 80% of these deaths occur in the pre-hospital phase [4].
According to the studies and predictions, pre-hospital care is vital in the effective management of these deaths to provide higher quality care and reduce injuries and death of casualties [5]; therefore in the case of traffic accident management and provision of comprehensive and timely services in the pre-hospital stage, at least 39% of these deaths are potentially preventable [6].
The system of providing pre-hospital services includes elements, such as information provision, casualty transfer, routing, composition and type of specialty of manpower in ambulances, and communication devices, such as wireless, etc. [7]. If all the factors involved in pre-hospital emergency care are properly considered, a lot of mortalities occurring in this phase will be prevented. In most studies on traffic accident mortality, systemic factors, managerial factors, technical defects, delay in diagnosis, and misdiagnosis have been identified as factors influencing preventable deaths [8, 9, 10, 11].
Iran is one of the countries where the highest number of accidents and traffic-related deaths are reported [12]. According to the latest statistics published by forensic medicine, traffic accidents in Iran annually lead to the death of nearly 17,000 people and permanent injury or disability of 300,000 people [13]. According to some reports, 57% of deaths due to traffic accidents in Iran occur in the pre-hospital stage, which is a significant percentage [14].
One of the critical challenges in investigating the preventable deaths of traffic accidents in the pre-hospital stage is the lack of appropriate measurement methods to assess it, i.e. a shortage that is considered a major vacuum in Iran. Measurement of the components affecting preventable deaths in traffic accidents, which is considered one of the critical and vital steps in research, requires the use of appropriate instruments [15]. To achieve this goal, either new instruments should be developed or the available instrument developed abroad should be used after ensuring their validity, reliability, and psychometric properties.
According to the search performed, instruments are available in the field of preventable traffic-related deaths, but because healthcare systems and service conditions are not the same in different countries, and in addition, different Angelo-American and Franco-German structures of pre-hospital systems exist in countries, thus, their full application in translation is not possible [16].
Regarding the importance of the analysis of preventable deaths and the components affecting it, and considering the limited studies in this field in other countries, and especially its absence in the Eastern Mediterranean and Asian countries, this study was conducted to develop and psychometrically evaluate a traffic-related pre-hospital mortality prevention questionnaire (TPMPQ).
2. Methods
The present study was conducted to develop and psychometrically evaluate an instrument to measure traffic-related pre-hospital preventable deaths in Iran in 2019-2020. This study used a mixed quantitative-qualitative design, including a systematic review, qualitative study of conventional content analysis type, Delphi study, and methodology. Instrument items were designed in the qualitative stage and psychometrically assessed in the quantitative stage.
Systematic Review Phase: In the systematic review phase, all factors affecting preventable mortality were identified based on search in databases of Web of Science (WoS), Scopus, PubMed, and Google Scholar, and then similar cases were either merged or deleted. To critically evaluate the articles, the research team evaluated the quality of all components of the articles using the critical appraisal skills programme (CASP) as an instrument to measure paper quality. Finally, the remaining content was classified into 3 main categories and 6 subcategories. Based on the findings of the study, three main categories, including “systemic defects, human errors, and the patient’s clinical condition” were extracted from codes in the systematic review stage.
Qualitative Interviews: Unstructured qualitative interviews were conducted with 26 participants who were selected by purposive sampling using the opinion of experts and specialists in this field. The interviewees included 26 people with an age range of 31-55 years. They had at least 5 years of work experience in traffic accident management, road traffic police, Red Crescent, fire brigade, technicians and pre-hospital emergency staff, emergency medicine specialists, and emergency department nurses. Four traffic accident victims were interviewed. Expert sampling was performed using purposive sampling until data saturation was achieved. After verbatim transcription of the interviews, they were imported into MAXQDA10 to classify the extracted codes. Subsequently, the main categories and subcategories were inductively extracted from the data.
Delphi: By combining the results of the systematic review [17] and qualitative interviews [18], the primary instrument was finally developed to use in Delphi rounds. In the Delphi stage, the study population included experts in the field of traffic accidents and pre-hospital emergencies at the macro and national levels. Three group discussions of the research team were held to summarize the extracted components. Ultimately, the 5-point Likert instrument was developed (strongly agree to strongly disagree) and entered the second round of Delphi. In the second round, the initial instrument designed in a focus group session was investigated for four hours with 15 experts in the field of traffic accidents. Moreover, an email was sent to 10 national experts of traffic accidents. After completing the instrument, the items that received an average of 2.5 and above entered the third round of Delphi. Besides, the answers to the open-ended items were examined with the research team and their opinions were applied in the form of editing the items of the instrument. In the third round, the remaining items from the second round were sent to 25 experts in the form of instruments to receive for and against comments. Of these, 22 instruments were returned, and finally, the items with a %75+ of the agreement were accepted.
Psychometric Evaluation: After extracting the items obtained from the Delphi method, to determine their face and content validity, the opinions of experts were collected. The target population in the psychometric phase also included subject matter experts, technicians, and prehospital emergency supervisors.
Face Validity: Qualitative and quantitative methods were used to establish face validity. To determine the qualitative face validity, 10 pre-hospital emergency technicians and supervisors were asked to comment on the fluency, clarity, and comprehensibility of the components and the need for removing or integrating the instrument components. After modifying the required items, the quantitative method of item impact (impact score = Frequency (%) × Importance) was used to determine the importance of each phrase. In this method, the five-point Likert scale was considered, quite important = 5, somewhat important = 4, moderately important = 3, slightly important = 2, and not important at all = 1. If the impact score was considered equal to or greater than 1.5, the phrase was deemed appropriate for subsequent analyses.
Content Validity: Two qualitative and quantitative methods were used to determine the content validity. In this study, content validity was determined based on experts’ judgments. In the qualitative method of determining content validity, the experts reviewed the items, and the necessary corrections were applied to them. To determine content validity by quantitative method, content validity ratio (CVR) and content validity index (CVI) were used. To determine the content validity ratio quantitatively, at least 10 experts were asked to respond to each of the instrument items in the range of “necessary, useful but not necessary, and not necessary”. An item score higher than 0.79 was rendered acceptable. Based on the Lawshe’s (1975) table, the minimum content validity ratio value was determined and the content validity ratio for all items was calculated using the following formula [19].
To calculate the content validity index, the experts commented on the three criteria of relevance or specificity, simplicity and fluency, and clarity or transparency based on the four-point Likert scale. A score higher than 0.79 was considered sufficient for accepting the items. Options included the following:
Not relevant=1, relatively relevant=2, relevant=3, fully relevant=4.
The method of item score calculation was such that the evaluators who gave three or four points to the items were divided by the total evaluators [20].
Reliability: The internal consistency coefficient was used to evaluate the reliability of the instrument in the present study. To determine internal consistency, Cronbach’s α was calculated for the whole instrument and its subscales. A total of 20 psychometrically finalized instruments were completed by the technicians present at the scene of the traffic accident and then Cronbach’s α was measured using SPSS software, version 22. Cronbach’s α above 0.7 was considered satisfactory for internal consistency [21]. The closer it is to 1, the more reliable it is.
3. Results
Systematic review
Initially, in the systematic review phase, 7247 papers were obtained from the mentioned databases. In addition, 1902 duplicated papers were excluded. A total of 5 355 titles and abstracts were examined and 218 full-text papers were explored of which, 12 were finalized for analysis. The rest of the papers were omitted because they were irrelevant or did not observe the inclusion criteria. Two more articles entered the study after examining the reference lists. Ultimately, 14 relevant papers were analyzed. Evaluation of the studies resulted in the production of three main categories, “systemic defects, human errors, and the patient’s clinical condition”. Seven subcategories also emerged. (The article of the systematic review stage was published in Trauma Monthly journal) [17].
Qualitative interviews
Based on the demographic information of the interviews in the qualitative interviews, 13 people (54%) were in the age group of 40-50 years, 15 people (63%) were men, 15 people (62%) were specialists/doctors and 17 people (71%) had a work experience of more than 15 years.
The participants’ experiences showed that considering things, such as accurate clinical assessment of the victim at the scene, appropriate quality care, legal guarantee, and necessary protocols, coordination of the involved organizations, and complete management of the accident scene through the incident commander and creating the highest level of scene safety in preventing pre-hospital deaths is effective.
In the qualitative interviews, six main categories were extracted as the major challenges of preventable deaths in road traffic injuries in the pre-hospital phase, including “poor management of the crash scene” with two subcategories of lack of rapid access to the patient and lack of scene safety, “lack of adequate rules and regulations” with two subcategories of lack of protocols and guidelines and lack of clear duties checklists, “poor management of time” with two subcategories of elongated response time at the crash scene and elongated time of victim transport, “low quality of training” with two subcategories of insufficient training of emergency medical services (EMS) staff and inadequate public training, “poor communication and coordination” with two subcategories of poor communication of EMS staff and lack of uniform commandership at the crash scene, and “low quality of victim management” with two subcategories of low quality of clinical care and lack of accurate clinical assessment (the article of the qualitative stage was published in archives of academic emergency medicine journal) [18].
Delphi
After integrating and classifying the results of the systematic review and qualitative interviews, an instrument consisting of 71 items was used in the initial round of Delphi. After analyzing the items using the average score based on the Likert scale from the first round, the instrument entered the third round of Delphi with 44 items, and finally in the third round, out of 44 items from the second round, 39 items with 75+% agreements were selected as the final items.
Psychometric Evaluation: In the first stage of face validity review, according to the opinions of emergency medical experts and technicians, the wording of six components was corrected, and since the impact score of all components was more than 1.5, no components were removed in the face validity stage. In the content validity stage, out of 39 components, 4 components with CVR of less than 0.6 were removed and the total components was reduced to 35. In the next stage, the CVI of no component was less than 0.79 and thus, no component was removed at this stage. The reliability of all items was above 0.7, and the final reliability was 0.84 (Table 1).
Finally, the instrument: Traffic-related pre-hospital mortality prevention questionnaire (TPMPQ) was approved after removing items 21, 37, 38, and 39 with 35 items and five dimensions.
4. Discussion
The present study was conducted using a mixed method for the first time by integrating systematic review, qualitative study, and Delphi study in 3 stages. The instrument developed in this study has high validity and reliability because, at each stage of validation, the experts’ opinions in instrument correction were considered and applied.
According to the first component in the present study, the assessment of trauma emergencies in various incidents includes scene assessment and casualty assessment. In assessing pre-hospital trauma casualties according to the pre-hospital trauma life support (PHTLS) guidelines, examining the scene, the mechanism of injury, and the primary and secondary assessment of the casualty are among the necessary factors that must be performed correctly [22]. Scene assessment means trying to establish scene security and paying close attention to the true nature of the situation. The primary assessment of the casualty also means that after an overview of the patient in terms of age, observations, and chief complaint, operations should be performed thoroughly, including assessment of the airway, spine and cervical vertebrae, respiratory status, blood circulation, and neurological status according to emergency technicians [23].
The efficiency and efficacy of medical care at the scene of an accident require the presence of paramedics and rescuers who can initially assess the scene and the condition of the casualty and have enough experience to make the right decision to reduce a significant proportion of prehospital mortality. After the initial assessment and ensuring that the casualty is not seriously threatened, a secondary assessment should be performed, which includes controlling vital signs, taking a medical history, and examining the casualty. This indicates the need for more attention from prehospital emergency officials to the method of emergency medical personnel about neurological examinations of trauma victims, especially cervical trauma and multiple trauma at the scene, and immobilization of cervical vertebrae using the cervical collar to prevent the formation or spread of spinal cord injuries. The results of a prospective study conducted by Fredø et al. in Norway showed that in 68% of trauma patients transferred to medical centers by the prehospital emergency, a cervical collar was used for immobilization, and in 5%, no therapeutic intervention was performed [24].
Taking a correct medical history is one of the effective factors in the second assessment of the casualty. According to experts, it was one of the cases with a high agreement coefficient and is vital in the quality of clinical services of emergency medical centers. In one study aimed at analyzing the causes of medical history errors in patients hospitalized in Iran’s pre-hospital emergency centers, 8 causes were stated as the reasons for not taking a proper history in the pre-hospital phase, “lack of sufficient knowledge, lack of ability to structure the history, inattention, poor communication with the patient, lack of motivation, lack of communication and adequate time, and inadequate environment” [25].
Weakness in scene management is rendered as another crucial and influential challenge in preventable deaths in the findings of the present study. In the present study, one of the effective challenges to death due to traffic accidents was the delay in the access to the casualty in the scene, which is influenced by factors, such as crowds or pile-ups in the scene and the lack of open access to the casualty. In a study conducted to improve the provision of pre-hospital emergency services, people’s interventions on the scene were expressed as effective factors in controlling or facilitating preventive care against traffic accidents [26]. In a study conducted to examine pre-hospital services in the developed and developing countries, the presence of people on the scene due to personal curiosity, eagerness for humanitarian aid, excitement, and rushing in the scene were expressed as factors leading to the crowded scene and poor communication [27]. Some studies have shown that the irrational gathering of people and pile-up at the scene of an accident is one of the factors fostering the weakness of the process of helping victims of traffic accidents and reducing the security of the scene [28, 29, 30].
Lack of communication and coordination is one of the intervening challenges in preventable deaths. The research findings also confirmed its significant effects. Proper communication and coordination can increase the readiness to provide pre-hospital care [31, 32]. The research results related to the challenge of managing the scene of traffic accidents in Iran also showed that the involvement of non-specialists, lack of coordination and cooperation, inadequate prehospital services, and defects in infrastructures have been among the causes of pre-hospital mortality [33].
Depending on the type of traffic accident, different organs are present on the scene and there should be a comprehensive system with powerful management and a single unit as a commander to coordinate the scene. The accident commander must act in such a way that he actively manages the accident scene and the resulting crowd throughout the accident until the accident returns to its original state. The police have been introduced as the coordinating organ at the scene of accidents to manage the scene of road accidents and the factors affecting the management of the scene of the accident [34, 35]. The commander of the accident may be different depending on the type of accident, but what is crucial is that due to the existence of different organs, the commander of the accident can be determined depending on the type of accident by developing the necessary processes and instructions.
Another effective factor in the coordination and communication subset is the early coordination with the hospital for transferring the casualty. In a study aimed at investigating the nature of pre-hospital medical interventions conducted in Tabriz Province, Iran, almost all casualties were transferred to the hospital without coordination with the receiving hospital. Considering that coordination, before the casualty arrives at the hospital, prepares the members of the treatment team to provide the desired services to the casualty, thus, this issue requires serious attention to improve communication in the pre-hospital stage between the casualty transfer team and medical centers [36]. According to the research, to investigate response time and delay consequences in EMS missions in Shiraz City, Iran, the following were suggested to reduce the response time of pre-hospital emergencies, “familiarity of technicians with peripheral routes and shortcuts, use of satellite systems, radar and automatic radio system (Trunking) to find the best and most appropriate way in case of emergency, educating people via the media to work with the EMS and give way to ambulances, considering special lanes for ambulances on busy streets, and using alternatives, such as motor lances on old or busy roads [37]. Familiarity of emergency technicians with peripheral routes and shortcuts, the use of satellite systems, radar, global positioning system (GPS), and high-frequency waves to find the best and most appropriate way in emergencies, are among the helpful solutions in this field [37].
In addition to teaching the management skills required by rescue personnel, operational training necessary to provide services on the scene is emphasized. In the research conducted to assess the educational needs of EMS technicians, most technicians referred to drug information and possible side-effects of their use in the dimension of knowledge, ability, and capacity in inserting endotracheal tubes in skill dimension, and professional interest in participating in in-service training courses to improve their academic level in the field of practical skills in attitude dimension [38]. Special pre-hospital emergency work topics, such as scene assessment, identifying the tasks of emergency workgroups, identifying patient assessment components, and triage should be included in the curriculum for students in areas that can potentially be considered rescue personnel (such as nursing or emergency medicine). Pre-hospital instant care (PHIC), prehospital trauma life supports (PHTLS), and basic cardiopulmonary resuscitation (BCPR) courses are specifically among the essential courses for pre-hospital care providers in different countries [3].
Based on the results of the present study, educating people about first aid will also be a great asset in diminishing deaths on the scene. Training should be based on the specific needs of communities and available resources. Besides, the training method should be simple and local about the transfer of vital skills to trainees in scene management, bleeding control, primary cardiopulmonary resuscitation, lifting and transfer of open fractures, and triage. Acquiring these skills by these people is effective as efficient first aid in the absence of trained healthcare professionals immediately after a traffic accident. Furthermore, educating people on the scene, the police, and acquiring first aid training skills to help improve patient’s outcomes in the pre-hospital phase are also identified as the effective factors [40, 41].
Adequate and sufficient equipment is one of the effective support components in fostering the goals of any system. The study conducted by Vaitkaitis, which examined the most acute problems in EMS in Lithuania, showed that the obsolescence and oldness of existing ambulances and the lack of integrated standards for medical education and treatment as influential components led to poor performance of medical services in the country [42].
5. Conclusion
The results of the present study revealed that the instrument developed with the dimensions of “scene and casualty assessment, coordination and communication, time management, training performance, and support” has acceptable validity and reliability to measure traffic-related pre-hospital preventable mortality. This instrument can measure the factors affecting the preventable deaths in the traffic accidents. By rendering preventable mortality as a measurable variable, it can serve as an effective instrument. Numerous factors at the managerial and therapeutic levels are crucial in reducing the preventable deaths due to traffic accidents in the pre-hospital phase. By identifying and planning for proper preparation or appropriate response in the scene, giant strands can be taken in this regard. Empowering the management of preventable deaths due to traffic accidents, accurate clinical assessments for the casualty at the scene without any negligence, providing quality and accurate services, coordinating the organs involved in defining the job description of each organ, complete accident scene management with integrated commandment approach and creating the highest security in the scene are necessary measures. Moreover, they also mentioned that the authorities should consider increasing the scientific and practical skills of the rescue personnel and the training of first aid for the people present on the scene.
The main limitation of this study is the lack of construct validity, which requires sampling and factor analysis to determine the sub-structures of the tool.
Ethical Considerations
Compliance with ethical guidelines
This article is approved by the Ethics Committee at Shahid Sadoughi University of Medical Sciences with the code: IR.SSU.SPH.REC.1397.038 dated 18.6.2018.
Funding
The paper was extracted from the doctoral thesis of Adel Eftekhari, Department of Nursing, Meybod School of Nursing, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Authors' contributions
Participating in the initial design of the study: Adel Eftekhari, Davood Khorasani, Abbas Ali Dehghani, and Khadijeh Nasiriani; Data collection and interviews: Adel Eftekhari, Davood Khorasani, Majid Haji Maghsoudi, and Khadijeh Nasiriani; Interviews and data analysis: Adel Eftekhari, Khadijeh Nasiriani, Davood Khorasani, and Hossein Fallahzadeh; Writing of the article and its content: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the experts and professionals who took the time for the interviews.
References
- Aderamo AJ. Assessing the trends in road traffic accident casualties on Nigerian roads. Journal of Social Sciences. 2012; 31(1):19-25. [DOI:10.1080/09718923.2012.11893011]
- Harmon T, Bahar GB, Gross FB. Crash costs for highway safety analysis. Washington: Federal Highway Administration. Office of Safety; 2018. [Link]
- Jamalian M, Eslamdost M, Rezaee A, Alizadeh S. [Investigating the causes of death in the injured of traffic accidents referred to Vali-Asr Hospital in Arak, based on oral autopsy and forensic autopsy (Persian)]. Journal of Arak University of Medical Sciences. 2020; 23(3):338-47. [DOI:10.32598/jams.23.3.5986.1]
- Sam EF, Blay DK, Antwi S, Anaafi C, Adoma JA. Prehospital and trauma care to road traffic accident victims: Experiences of residents living along accident-prone highways in Ghana. Emergency Medicine and Trauma. 2019; 10(34):234-8. [DOI:10.5772/intechopen.86118]
- Rahmani K, Hashemi Nazari SS, Ghadirzadeh MR. [Trend analysis of traffic accident deaths in Iran during 2006-2012: Hospital or prehospital occurred deaths (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2016; 15(2):115-28. [Link]
- Haghparast Bidgoli H, Bogg L, Hasselberg M. Pre-hospital trauma care resources for road traffic injuries in a middle-income country--a province based study on need and access in Iran. Injury. 2011; 42(9):879-84. [DOI:10.1016/j.injury.2010.04.024] [PMID]
- Bakke HK, Wisborg T. Rural high north: A high rate of fatal injury and prehospital death. World Journal of Surgery. 2011; 35(7):1615-20. [DOI:10.1007/s00268-011-1102-y] [PMID] [PMCID]
- McDermott FT, Cooper GJ, Hogan PL, Cordner SM, Tremayne AB. Evaluation of the prehospital management of road traffic fatalities in Victoria, Australia. Prehospital and Disaster Medicine. 2005; 20(4):219-27. [DOI:10.1017/S1049023X00002570] [PMID]
- Michiue T, Ishikawa T, Quan L, Zhu BL, Maeda H. Forensic pathological evaluation of injury severity and fatal outcome in traffic accidents: Five illustrative autopsy cases of clinically unexpected death. Forensic Science, Medicine, and Pathology. 2008; 4(3):153-8. [DOI:10.1007/s12024-007-9025-5] [PMID]
- Rivara FP, Maier RV, Mueller BA, Luna GA, Dicker BG, Herman CM, et al. Evaluation of potentially preventable deaths among pedestrian and bicyclist fatalities. JAMA. 1989; 261(4):566-70. [DOI:10.1001/jama.1989.03420040104028] [PMID]
- Rosenfeld JV, McDermott FT, Laidlaw JD, Cordner SM, Tremayne AB. The preventability of death in road traffic fatalities with head injury in Victoria, Australia. The Consultative Committee on Road Traffic Fatalities. Journal of Clinical Neuroscience. 2000; 7(6):507-14. [DOI:10.1054/jocn.1999.0694] [PMID]
- Isazadehfar K, Salamati P, Zafarghandi MR, Rahimi-Movaghar V, Khormali M, Baigi V. Insurance status and traumatized patients’ outcomes: A report from the national trauma registry of Iran. BMC Health Services Research. 2023.; 23(1):392. [PMID]
- Zargar M, Khaji A, Karbakhsh M. Pattern of motorcycle-related injuries in Tehran, 1999 to 2000: A study in 6 hospitals. Eastern Mediterranean Health Journal. 2006; 12(1-2):81-7. [PMID]
- Montazeri A. Road-traffic-related mortality in Iran: A descriptive study. Public Health. 2004; 118(2):110-3.[DOI:10.1016/S0033-3506(03)00173-2] [PMID]
- Shamsi M, Headarnia A, Niknami S, Rafiee M. [Development and psychometric assessment of an oral health instrument based on health belief model in pregnant women (Persian)]. Journal of Arak University of Medical Sciences. 2012; 15(6):45-56. [Link]
- Shirinabadi Farahani A, Rassouli M, Yaghmaei F, Alavi Majd H. [Index for selecting an appropriate instrument to conduct research in health sciences: Introducing the COSMIN checklist (Persian)]. Journal of Health Promotion Management. 2015; 4(4):1-13. [Link]
- Eftekhari A, Dehghani Tafti AA, Khorasani-Zavareh D, Nasiriani K, Hajimaghsoudi M, Falahzadeh H. Root causes of preventable prehospital deaths in road traffic injuries: A systematic review. Trauma Monthly. 2019; 24(4):1-8. [DOI:10.5812/traumamon.88412]
- Eftekhari A, DehghaniTafti A, Nasiriani K, Hajimaghsoudi M, Fallahzadeh H, Khorasani-Zavareh D. Identification and prioritization of key components influencing prehospital emergency related to preventable road traffic injuries deaths in Iran; A Delphi Study. Bulletin of Emergency and Trauma. 2019; 7(4):381-9. [DOI:10.29252/beat-070407] [PMID] [PMCID]
- Vakili MM, Hidarnia AR, Niknami S. [Development and psychometrics of an interpersonal communication skills scale (ASMA) among Zanjan health volunteers (Persian)]. Hayat. 2012; 18(1):5-19. [Link]
- Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Research in Nursing & Health. 2007; 30(4):459-67. [DOI:10.1002/nur.20199] [PMID]
- Cronbach LJ, Meehl PE. Construct validity in psychological tests. Psychological Bulletin. 1955; 52(4):281-302. [DOI:10.1037/h0040957] [PMID]
- Advancing the EMS profession (NAEMT). Prehospital trauma life support [Internet]. 2014 [Updated 2023 May 20]. Available from: [Link]
- Proehl JA. Emergency Nursing procedures E-Book. Amsterdam: Elsevier; 2008. [Link]
- Fredø HL, Rizvi SA, Lied B, Rønning P, Helseth E. The epidemiology of traumatic cervical spine fractures: a prospective population study from Norway. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2012; 20:85. [DOI:10.1186/1757-7241-20-85] [PMID] [PMCID]
- Khalili Z, Sadrollahi A, Ahmadi Khatir M. [Analysis of the causes of error in receiving medical history from patients in emergency centers Kardkoy hospital (Persian)]. Health care Management. 2016; 6(1):29-41. [Link]
- Haghani F, Sadeghi N. [Training in pre-hospital emergency: Needs and truths (Persian)]. Iranian Journal of Medical Education. 2011; 10(5):1273-80. [Link]
- Khankeh HR, Alinia SH, Masoumi GHR, Ranjbar M, Daddoost L, Hosseini SA, et al. [Prehospital services by focus on road traffic accidents: Assessment developed and developing countries (Persian)]. Journal of Health Promotion Management. 2013; 2(2):71-9. [Link]
- Balikuddembe JK, Ardalan A, Khorasani-Zavareh D, Nejati A, Raza O. Weaknesses and capacities affecting the Prehospital emergency care for victims of road traffic incidents in the greater Kampala metropolitan area: A cross-sectional study. BMC Emergency Medicine. 2017; 17(1):29. [DOI:10.1186/s12873-017-0137-2] [PMID] [PMCID]
- Khorasani-Zavareh D, Mohammadi R, Bohm K. Factors influencing pre-hospital care time intervals in Iran: A qualitative study. Journal of Injury & Violence Research. 2018; 10(2):83-90. [PMID] [DOI:10.5249/jivr.v10i2.953]
- Ebben RH, Vloet LC, Verhofstad MH, Meijer S, Mintjes-de Groot JA, van Achterberg T. Adherence to guidelines and protocols in the prehospital and emergency care setting: A systematic review. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2013; 21:9. [DOI:10.1186/1757-7241-21-9] [PMID] [PMCID]
- Jayaraman S, Mabweijano JR, Lipnick MS, Caldwell N, Miyamoto J, Wangoda R, et al. Current patterns of prehospital trauma care in Kampala, Uganda and the feasibility of a lay-first-responder training program. World Journal of Surgery. 2009; 33(12):2512-21. [DOI:10.1007/s00268-009-0180-6] [PMID]
- Tannvik TD, Bakke HK, Wisborg T. A systematic literature review on first aid provided by laypeople to trauma victims. Acta Anaesthesiologica Scandinavica. 2012; 56(10):1222-7. [DOI:10.1111/j.1399-6576.2012.02739.x] [PMID] [PMCID]
- Mostafanejad R, Janati A, Sadeghi-Bazargani H, Babaie J. Challenges of scene management in road traffic accidents: A systematic literature review. Journal of Injury and Violence Research. 2019; 11(4 Suppl 2):61. [Link]
- Esmaeili A, Azizi H, Zahiri M. [Investigating the role of road policing in the field of road accident management: Ardabil province (Persian)]. Quarterly Journal of Traffic Management Studies. 2011; 5(17):1-23. [Link]
- Amiri M, Khankeh H, Momeni E, Eini E. [Factors affecting crash scenario management: A study of theory of land in the Islamic Republic of Iran (Persian)]. Scientific Quarterly of Rahvar. 2015; 3(11):11-30. [Link]
- Dadashzadeh A, Dehghannejhad J, Shams Vahdati S, Soheili A, Sadeghi Bazarghani H. [The nature of prehospital medical interventions delivered to traumatic patients in Tabriz (Persian)]. Nursing And Midwifery Journal. 2017; 15(3):159-67. [Link]
- Moradian MJ, Peyravi MR, Ettehadi R, Pourmohammadi K. [Studying the time of response and results of delay in emergency medical system's (EMS) missions in Shiraz (Persian)]. Quarterly Scientific Journal of Rescue & Relief. 2013; 5(2):30-9. [Link]
- Rabari AS, Shamseddini MT, Saberi Anari SM, Ghaedi Heidari F. [Assessing educational needs of emergency medical technicians (Persian)]. Iranian Journal of Emergency Medicine. 2016; 4(3):111-7. [DOI:10.22037/ijem.v2i1.15833]
- Bai Z, Wang L, Yu B, Xing D, Su J, Qin H. The success rate of cardiopulmonary resuscitation and its correlated factors in patients with emergency prehospital cardiac arrest. Biotechnology & Genetic Engineering Reviews. 2023; 2:1-10. [PMID]
- Zargar M, Kalantar Motamedi SM, Karbakhsh M, Ghodsi SM, Rahimi-Movaghar V, Panahi F, et al. Trauma care system in Iran. Chinese Journal of Traumatology. 2011; 14(3):131-6. [PMID]
- Husum H, Gilbert M, Wisborg T. Training pre-hospital trauma care in low-income countries: The 'village university' experience. Medical Teacher. 2003; 25(2):142-8. [DOI:10.1080/0142159031000092526] [PMID]
- Vaitkaitis D. EMS systems in Lithuania. Resuscitation. 2008; 76(3):329-32. [DOI:10.1016/j.resuscitation.2007.07.028] [PMID]
Type of Study: Orginal Article |
Subject:
● Health Systems
Received: 2022/12/20 | Accepted: 2023/03/12 | Published: 2023/06/29
Received: 2022/12/20 | Accepted: 2023/03/12 | Published: 2023/06/29
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
