

Volume 13, Issue 3 (May & Jun 2023)
J Research Health 2023, 13(3): 219-226 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Darbandi M T, Mansoorian M, Rostamian M, Noori R. The Effect of Family-centered Education on Stress and Anxiety in Caregivers of Patients With COVID-19. J Research Health 2023; 13 (3) :219-226
URL: http://jrh.gmu.ac.ir/article-1-2218-en.html
URL: http://jrh.gmu.ac.ir/article-1-2218-en.html



1- Nursing Research Center, Gonabad University of Medical Sciences, Gonabad, Iran.
2- Department of English, Faculty of Medicine, Nursing Research Center, Gonabad University of Medical Scinences, Gonabad, Iran.
3- Nursing Research Center, Gonabad University of Medical Sciences, Gonabad, Iran. ,rnoori68@gmail.com
2- Department of English, Faculty of Medicine, Nursing Research Center, Gonabad University of Medical Scinences, Gonabad, Iran.
3- Nursing Research Center, Gonabad University of Medical Sciences, Gonabad, Iran. ,
Full-Text [PDF 559 kb]
(539 Downloads)
| Abstract (HTML) (1467 Views)
Full-Text: (466 Views)
1. Introduction
Mental health plays an important role in the vitality and efficiency of any society. Mental health is the key to happiness and increasing the sense of self-confidence in families. Poor mental health will cause anxiety, stress, apprehension, and despair [1]. Selye defined stress as the body’s non-specific response to any stimulus imposed. This stimulus can be either internal, cognitive, or external and environmental, including the stressors [2]. Anxiety is also a widespread, unpleasant, and vague feeling of anxiety or instability, which can be triggered by the experience of an acute or chronic disease [3, 4]. Approximately 1 out of 5 people suffer from anxiety disorders worldwide every year. COVID-19 has caused a lot of anxiety and stress in the general population in recent years [5].
COVID-19 can infect the patient and present as mild respiratory disease or acute forms such as severe acute respiratory syndrome. In December 2019, the outbreak of COVID-19 began in Wuhan, China, and has infected many parts of the world ever since. In Iran, the disease has also been highly prevalent [6]. The fear of the unknown produces more anxiety in people. More than 50% of people experience anxiety during epidemics [7]. COVID-19 has also contributed to the spread of psychological disorders such as stress, anxiety, depression, post-traumatic stress, insomnia, and fear of contagion [8, 9]. It has changed the lifestyle of millions of people in the world. The rapid transmission of the disease and the resulting mortality added to the public fear of affliction with the disease. The stress caused by this disease has dominated the mental well-being and adaptation of all age groups [9].
Stress is a risk factor for cardiovascular diseases, disorders in the digestive system, immune system failures, and mood swings [2]. Research has shown that the level of public health concern and anxiety during COVID-19 is high [10, 11]. Therefore, in this chaotic condition created by the spread of the disease, people may consider themselves infected without actually being so. This condition can increase the intensity of anxiety and its symptoms [7]. Anxiety can adversely affect the immune system, create a negative attitude, and reduce adherence to medication [12]. The reduced quality of life and performance is another adverse effect of anxiety and stress [6, 12]. The family members of the COVID-19 patients and the deceased cases are more susceptible to anxiety than other populations [13]. A family is an integrated system, and a family member’s disease can threaten the whole system [14].
Anxiety can interfere with the family member’s ability to obtain information and understand it, maintain proper family functioning, use coping strategies effectively, and provide positive support to the patient [8]. It is important to pay close attention to the health of people in contact with infected cases. These individuals had lower health, more distress, and less life satisfaction [8]. Family-centered educational intervention is used in anxiety and stress disorders [15, 16, 17]. This education is a main concept in nursing and aims to provide exceptional care for each patient. In the family-based educational method, the family plays an active role in assessing and identifying educational needs [18]. Keeping social distance is the main strategy to reduce the transmission of the disease, which has a negative effect on family-based care in hospitals, because the care systems must severely limit the presence of the family for all patients to protect the family and the patient [19]. Providing evidence-based and scientific strategies to policymakers can help them devise effective measures to mitigate psychological problems during the pandemic [8].
Although the anxiety and stress induced by COVID-19 are common health issues in patients and their families, based on the literature, there is a lack of research on the educational needs of COVID-19 patients’ caregivers. Therefore, the present study aimed to determine the effect of family-based education on stress and anxiety in the families of COVID-19 patients’ caregivers.
2. Methods
The present clinical trial with two randomized research groups was conducted on 50 family caregivers of COVID-19 patients in 2022. The sample size was estimated at 25 for each group at a 95% of the confidence interval and 80% of test power. The inclusion criteria were the definite diagnosis of COVID-19 by a doctor and admission to Bohlool Gonabadi Hospital, Gonabad City, Iran. The inclusion criteria for the caregivers were being a close relative, acting as the main caregiver of patients hospitalized in the infectious ward, lacking a history of mental disorders, having at least an elementary school education level (according to the patients’ reports), not any healthcare-related post, not providing care for someone else at the same time, being 18 to 70 years old, and lacking a history of family members’ death by the COVID-19. The exclusion criteria for the patient were his/her death during the study or discharge in less than 4 days of hospitalization in the infectious ward. The exclusion criteria for the patient’s caregiver included unwillingness to continue participating in the research and substituting the main caregiver. All the participants were present until the end of the study, with 25 participants in each group.
The data collection instruments included the sample selection form, demographic information profile, and the depression, anxiety, and stress scale (DASS). The content validity of the demographic information profile was checked and confirmed by the Nursing Faculty members of Gonabad University of Medical Sciences. Lavibond first developed DASS in 1995. In Iran, Ghafari et al. substantiated its face and content validity using the views of 10 nursing professors at Tarbiat Modares University and Tehran University. Also, the reliability of the questionnaire was confirmed using the test-retest method with a reliability coefficient of r=0.91 [20]. Also, in Moradipanah et al.’s study, the estimated Cronbach α coefficients for depression, anxiety, and stress were 0.94, 0.92, and 0.82, respectively [21]. In this study, the estimated Cronbach α coefficient was 0.90 for anxiety and 0.84 for stress.
After obtaining permission from Gonabad University of Medical Sciences, caregivers were selected through a convenience sampling method based on the inclusion criteria of the patients hospitalized in Allameh Bohlool Gonabadi Hospital. First, the patients were randomly assigned to the two research groups. The patients hospitalized on Saturdays, Mondays, and Wednesdays were assigned to the experimental group, and those hospitalized on Sundays, Tuesdays, and Thursdays were assigned to the control group. Eligible subjects were included in the study after a face-to-face explanation of the research and obtaining written informed consent. The researcher completed the individual profile form for these patients in a waiting room through an interview.
The educational intervention was implemented in the experimental group when the patient was hospitalized and continued for 4 full days. During the hospitalization, the researcher was present with the family members and answered their questions and concerns. On the first and second days of hospitalization, caregivers were taught about the nature of the disease, common symptoms, treatment and ways of transmitting the disease, and particularly the preventive measures when visiting the patient. The focus of the third and fourth days was post-discharge care, which included patient care during quarantine, proper use of personal protection for the patient and family members, how to disinfect the environment, clothes, and the patient’s personal stuff, and an appropriate diet for the patient and family members. The hazardous symptoms and the patient’s return to the hospital were taught to the caregivers, and an educational pamphlet was given to the patients. All training sessions were conducted face-to-face by a nurse and in compliance with health and safety protocols in the meeting room of the ward in a quiet place for 30 minutes during the patient’s hospitalization. For training, we used the guide for diagnosis, treatment, and care of COVID-19 in hospitalized patients provided by the Ministry of Health, Medical Education and Training of Iran. In the control group, care was provided according to the current routine protocol of the ward. At the beginning of the patient’s hospitalization and the end of the fourth day, the caregiver’s stress and anxiety were assessed using the DASS in two groups.
After coding and recording the data in the statistical package, descriptive statistics were calculated, including the frequency, Mean±SD. The Kolmogorov-Smirnov test was used to test the normality of quantitative variables. Inferential statistics were used, including independent samples t-test, paired samples t-test, Mann-Whitney U test, Chi-squared test, and Wilcoxon’s test to test the normality of quantitative variables. The relationships between the variables were assessed too. The data analysis was done in SPSS software, version 22.
3. Results
The Mean±SD of the patients’ age was 55.8±12.9 years in the experimental group and 58.2±12.6 years in the control group. The independent samples t-test did not show this difference as statistically significant (P=0.501), and the two groups were homogeneous. In the experimental group, 14 participants (0.56%), and in the control group, 13 participants (52%) were female caregivers, and the two groups were homogeneous in terms of the caregiver’s sex frequency (P=1.000).
The Mean±SD of the caregivers’ age in the experimental group was 43.6±10.0 years, and in the control group was 43.4±8.3 years. The independent samples t-test did not show this difference as statistically significant (P=0.915), and the two groups were homogeneous in this respect. As for sex, 18 participants (72.0%) in the experimental group and 14 caregivers (56.0%) in the control group were female, and the two groups were homogeneous (P=0.377). Also, concerning the ratio of the main caregiver to the patient, in the experimental group, 12 participants (48%), and in the control group, 15 participants (60%) were the patients’ children. The exact Chi-square test did not reveal any statistically significant difference (P=0.779), and the two groups were homogeneous. The other demographic information is summarized in Table 1.

Before the intervention, theMean±SD of the caregivers’ stress in the experimental group was 11.7±0.3; in the control group, it was 13.6±3.7, and the two groups were homogeneous (P=0.061). Yet, after the intervention, the Mean±SD of caregivers’ stress was 5.9±2.0 in the experimental group and 10.1±3.4 in the control group. The independent samples t-test showed this difference to be significant (P<0.001). Also, after the intervention, the caregivers’ stress decreased by 5.8±2.7 in the experimental group and 3.5±1.9 in the control group. The between-group difference was statistically significant (P=0.001) (Table 2).

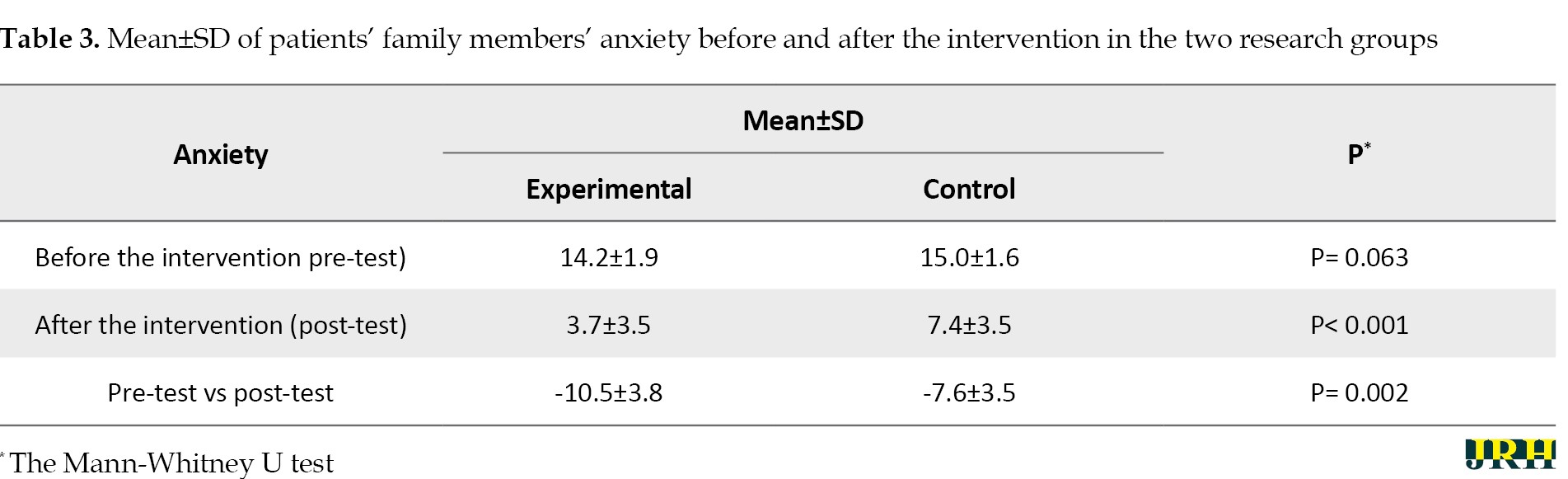
As for the anxiety of patients’ caregivers, before the intervention, the Mean±SD in the experimental and control groups were 14.2±1.9 and 15.0±1.6, respectively. The Mann-Whitney U test revealed no statistically significant difference between the two groups (P=0.063). However, after the intervention, the Mean±SD of caregivers’ anxiety in the experimental and control groups were 3.7±3.5 and 7.4±3.5, respectively. The Mann-Whitney U test showed this difference to be statistically significant (P<0.001). Also, the caregivers’ anxiety was reduced in the post-test compared to the pre-test by 10.5±3.8 in the experimental group and 7.6±3.5 in the control group. The Mann-Whitney U test showed this difference to be statistically significant (P=0.002) (Table 3).
4. Discussion
The present study aimed to explore the effect of family-based education on the stress and anxiety of COVID-19 patients’ caregivers in 2022. The findings showed that the family-based educational program held for the caregivers of COVID-19 patients could significantly reduce stress in the intervention group compared to the control group. The results of a similar study by Navidian et al. proved the positive effect of a supportive educational intervention on the psychological reactions of the family members of ICU patients. Thus, providing the family with needed information could increase their understanding and reduce their psychological symptoms, including stress [22]. Azizi et al., in their study entitled “the effectiveness of informational support on the level of anxiety in family caregivers of hemiplegic stroke patients”, showed that the educational intervention and information provision about the nature of the disease, symptoms, treatment, and the required care could significantly reduce stress in the intervention group [23]. In another similar study, Shoushi et al. implemented a family-centered care program on depression, anxiety, and stress of family caregivers of open-heart surgery patients. This study confirmed the program’s effectiveness in reducing caregivers’ stress [24]. Considering that part of the stress and anxiety in epidemic diseases is induced by the unknown nature of the disease and the fear of infection of the disease [8, 25], educational support and family-based training are essential to reduce stress and anxiety induced for the reasons mentioned above.
As the present study showed, implementing the family-centered educational program decreased anxiety in the experimental group compared to the control. The findings reported by Jabbarpour et al. also showed that providing information about the patient’s condition reduced anxiety in the intervention group [26]. Zakerimoghadam et al. also showed that implementing the nursing support program can reduce depression and anxiety in patients’ families during surgery [27]. Also, the research findings by Shoushi et al. confirmed the reduction of anxiety in a patient’s caregiver during an open-heart surgery following the implementation of a family-based care program [24].
Asgharpoor et al. and Lim Chiang et al. managed to reduce anxiety in the families of intensive care unit patients using mobile phones and an educational program [28, 29].
Because part of the anxiety of the patient’s family is due to the lack of knowledge about the process of the disease and the patient’s condition, the family-centered educational program can be effective in reducing the anxiety of the patient’s caregivers by providing the necessary information about the disease and the patient’s condition.
Golaghaie et al. also explored the effect of a family-centered clinical intervention on the anxiety of family members of patients admitted to the intensive care units (ICUs). This study showed a significant difference between the mean anxiety score on the second day of intervention and the control group. Yet, the anxiety score of the intervention group on the sixth day of hospitalization was higher than the control group. This finding is not in agreement with the present study [30]. The reason may be due to the prolonged contact of the family with the patient during the stay in the ICU, as patients in the ICU are in a worse condition than those infected with COVID-19, and observing critical conditions, equipment connected to the patient’s body, and seeing other patients can significantly add to the anxiety. Moreover, the family members feel helpless in the ICUs, and any talk about or news from the staff acts as a stressor which can lead to an anxiety-provoking reaction. Also, individual training for caregivers and providing information may be another reason for the different findings. The limitations of this study included receiving information from other sources and individual differences and the psychological state of the research units when answering the questions, which could affect their answers. Also, this study was conducted on caregivers of hospitalized patients, and therefore it is suggested that further studies be conducted on caregivers of hospitalized patients at home under similar conditions.
5. Conclusion
Regarding the present findings, educating caregivers of patients with COVID-19 can reduce their stress and anxiety by raising their awareness of self- and patient-care. It lowers the psychological burden and improves their adaptation. Therefore, it is suggested to use this program as a part of the healthcare system to reduce the patients’ and families’ problems and increase the efficiency of the health system.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted following the guidelines of the Declaration of Helsinki, and all procedures involving study participants was approved by the Deputy of Research at Gonabad University of Medical Sciences (Code: IR.GMU.REC.1399.118). Verbal informed consent was obtained from all subjects
Funding
This paper is part of the Mohammadjamal Tayarani Darbandi’s master’s thesis and was approved by Gonabad University of Medical Sciences (Code: 275/99).
Authors' contributions
Conceptualization, design, data collection, result interpretation, writing the first draft of the paper, and final approval: Mohammadjamal Tayarani Darbandi; Work supervision, writing the initial draft of the paper and final approval: Reza Noori; Project design, data analysis, and interpretation: Morteza Rostamian and Mohammadreza Mansoorian; Reading and approval of the final manuscript: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express gratitude to the staff of the inpatient ward of COVID-19 patients in Allameh Bohlool Gonabadi Hospital, who cooperated in this research, and the research participants.
References
Mental health plays an important role in the vitality and efficiency of any society. Mental health is the key to happiness and increasing the sense of self-confidence in families. Poor mental health will cause anxiety, stress, apprehension, and despair [1]. Selye defined stress as the body’s non-specific response to any stimulus imposed. This stimulus can be either internal, cognitive, or external and environmental, including the stressors [2]. Anxiety is also a widespread, unpleasant, and vague feeling of anxiety or instability, which can be triggered by the experience of an acute or chronic disease [3, 4]. Approximately 1 out of 5 people suffer from anxiety disorders worldwide every year. COVID-19 has caused a lot of anxiety and stress in the general population in recent years [5].
COVID-19 can infect the patient and present as mild respiratory disease or acute forms such as severe acute respiratory syndrome. In December 2019, the outbreak of COVID-19 began in Wuhan, China, and has infected many parts of the world ever since. In Iran, the disease has also been highly prevalent [6]. The fear of the unknown produces more anxiety in people. More than 50% of people experience anxiety during epidemics [7]. COVID-19 has also contributed to the spread of psychological disorders such as stress, anxiety, depression, post-traumatic stress, insomnia, and fear of contagion [8, 9]. It has changed the lifestyle of millions of people in the world. The rapid transmission of the disease and the resulting mortality added to the public fear of affliction with the disease. The stress caused by this disease has dominated the mental well-being and adaptation of all age groups [9].
Stress is a risk factor for cardiovascular diseases, disorders in the digestive system, immune system failures, and mood swings [2]. Research has shown that the level of public health concern and anxiety during COVID-19 is high [10, 11]. Therefore, in this chaotic condition created by the spread of the disease, people may consider themselves infected without actually being so. This condition can increase the intensity of anxiety and its symptoms [7]. Anxiety can adversely affect the immune system, create a negative attitude, and reduce adherence to medication [12]. The reduced quality of life and performance is another adverse effect of anxiety and stress [6, 12]. The family members of the COVID-19 patients and the deceased cases are more susceptible to anxiety than other populations [13]. A family is an integrated system, and a family member’s disease can threaten the whole system [14].
Anxiety can interfere with the family member’s ability to obtain information and understand it, maintain proper family functioning, use coping strategies effectively, and provide positive support to the patient [8]. It is important to pay close attention to the health of people in contact with infected cases. These individuals had lower health, more distress, and less life satisfaction [8]. Family-centered educational intervention is used in anxiety and stress disorders [15, 16, 17]. This education is a main concept in nursing and aims to provide exceptional care for each patient. In the family-based educational method, the family plays an active role in assessing and identifying educational needs [18]. Keeping social distance is the main strategy to reduce the transmission of the disease, which has a negative effect on family-based care in hospitals, because the care systems must severely limit the presence of the family for all patients to protect the family and the patient [19]. Providing evidence-based and scientific strategies to policymakers can help them devise effective measures to mitigate psychological problems during the pandemic [8].
Although the anxiety and stress induced by COVID-19 are common health issues in patients and their families, based on the literature, there is a lack of research on the educational needs of COVID-19 patients’ caregivers. Therefore, the present study aimed to determine the effect of family-based education on stress and anxiety in the families of COVID-19 patients’ caregivers.
2. Methods
The present clinical trial with two randomized research groups was conducted on 50 family caregivers of COVID-19 patients in 2022. The sample size was estimated at 25 for each group at a 95% of the confidence interval and 80% of test power. The inclusion criteria were the definite diagnosis of COVID-19 by a doctor and admission to Bohlool Gonabadi Hospital, Gonabad City, Iran. The inclusion criteria for the caregivers were being a close relative, acting as the main caregiver of patients hospitalized in the infectious ward, lacking a history of mental disorders, having at least an elementary school education level (according to the patients’ reports), not any healthcare-related post, not providing care for someone else at the same time, being 18 to 70 years old, and lacking a history of family members’ death by the COVID-19. The exclusion criteria for the patient were his/her death during the study or discharge in less than 4 days of hospitalization in the infectious ward. The exclusion criteria for the patient’s caregiver included unwillingness to continue participating in the research and substituting the main caregiver. All the participants were present until the end of the study, with 25 participants in each group.
The data collection instruments included the sample selection form, demographic information profile, and the depression, anxiety, and stress scale (DASS). The content validity of the demographic information profile was checked and confirmed by the Nursing Faculty members of Gonabad University of Medical Sciences. Lavibond first developed DASS in 1995. In Iran, Ghafari et al. substantiated its face and content validity using the views of 10 nursing professors at Tarbiat Modares University and Tehran University. Also, the reliability of the questionnaire was confirmed using the test-retest method with a reliability coefficient of r=0.91 [20]. Also, in Moradipanah et al.’s study, the estimated Cronbach α coefficients for depression, anxiety, and stress were 0.94, 0.92, and 0.82, respectively [21]. In this study, the estimated Cronbach α coefficient was 0.90 for anxiety and 0.84 for stress.
After obtaining permission from Gonabad University of Medical Sciences, caregivers were selected through a convenience sampling method based on the inclusion criteria of the patients hospitalized in Allameh Bohlool Gonabadi Hospital. First, the patients were randomly assigned to the two research groups. The patients hospitalized on Saturdays, Mondays, and Wednesdays were assigned to the experimental group, and those hospitalized on Sundays, Tuesdays, and Thursdays were assigned to the control group. Eligible subjects were included in the study after a face-to-face explanation of the research and obtaining written informed consent. The researcher completed the individual profile form for these patients in a waiting room through an interview.
The educational intervention was implemented in the experimental group when the patient was hospitalized and continued for 4 full days. During the hospitalization, the researcher was present with the family members and answered their questions and concerns. On the first and second days of hospitalization, caregivers were taught about the nature of the disease, common symptoms, treatment and ways of transmitting the disease, and particularly the preventive measures when visiting the patient. The focus of the third and fourth days was post-discharge care, which included patient care during quarantine, proper use of personal protection for the patient and family members, how to disinfect the environment, clothes, and the patient’s personal stuff, and an appropriate diet for the patient and family members. The hazardous symptoms and the patient’s return to the hospital were taught to the caregivers, and an educational pamphlet was given to the patients. All training sessions were conducted face-to-face by a nurse and in compliance with health and safety protocols in the meeting room of the ward in a quiet place for 30 minutes during the patient’s hospitalization. For training, we used the guide for diagnosis, treatment, and care of COVID-19 in hospitalized patients provided by the Ministry of Health, Medical Education and Training of Iran. In the control group, care was provided according to the current routine protocol of the ward. At the beginning of the patient’s hospitalization and the end of the fourth day, the caregiver’s stress and anxiety were assessed using the DASS in two groups.
After coding and recording the data in the statistical package, descriptive statistics were calculated, including the frequency, Mean±SD. The Kolmogorov-Smirnov test was used to test the normality of quantitative variables. Inferential statistics were used, including independent samples t-test, paired samples t-test, Mann-Whitney U test, Chi-squared test, and Wilcoxon’s test to test the normality of quantitative variables. The relationships between the variables were assessed too. The data analysis was done in SPSS software, version 22.
3. Results
The Mean±SD of the patients’ age was 55.8±12.9 years in the experimental group and 58.2±12.6 years in the control group. The independent samples t-test did not show this difference as statistically significant (P=0.501), and the two groups were homogeneous. In the experimental group, 14 participants (0.56%), and in the control group, 13 participants (52%) were female caregivers, and the two groups were homogeneous in terms of the caregiver’s sex frequency (P=1.000).
The Mean±SD of the caregivers’ age in the experimental group was 43.6±10.0 years, and in the control group was 43.4±8.3 years. The independent samples t-test did not show this difference as statistically significant (P=0.915), and the two groups were homogeneous in this respect. As for sex, 18 participants (72.0%) in the experimental group and 14 caregivers (56.0%) in the control group were female, and the two groups were homogeneous (P=0.377). Also, concerning the ratio of the main caregiver to the patient, in the experimental group, 12 participants (48%), and in the control group, 15 participants (60%) were the patients’ children. The exact Chi-square test did not reveal any statistically significant difference (P=0.779), and the two groups were homogeneous. The other demographic information is summarized in Table 1.
Before the intervention, theMean±SD of the caregivers’ stress in the experimental group was 11.7±0.3; in the control group, it was 13.6±3.7, and the two groups were homogeneous (P=0.061). Yet, after the intervention, the Mean±SD of caregivers’ stress was 5.9±2.0 in the experimental group and 10.1±3.4 in the control group. The independent samples t-test showed this difference to be significant (P<0.001). Also, after the intervention, the caregivers’ stress decreased by 5.8±2.7 in the experimental group and 3.5±1.9 in the control group. The between-group difference was statistically significant (P=0.001) (Table 2).
As for the anxiety of patients’ caregivers, before the intervention, the Mean±SD in the experimental and control groups were 14.2±1.9 and 15.0±1.6, respectively. The Mann-Whitney U test revealed no statistically significant difference between the two groups (P=0.063). However, after the intervention, the Mean±SD of caregivers’ anxiety in the experimental and control groups were 3.7±3.5 and 7.4±3.5, respectively. The Mann-Whitney U test showed this difference to be statistically significant (P<0.001). Also, the caregivers’ anxiety was reduced in the post-test compared to the pre-test by 10.5±3.8 in the experimental group and 7.6±3.5 in the control group. The Mann-Whitney U test showed this difference to be statistically significant (P=0.002) (Table 3).
4. Discussion
The present study aimed to explore the effect of family-based education on the stress and anxiety of COVID-19 patients’ caregivers in 2022. The findings showed that the family-based educational program held for the caregivers of COVID-19 patients could significantly reduce stress in the intervention group compared to the control group. The results of a similar study by Navidian et al. proved the positive effect of a supportive educational intervention on the psychological reactions of the family members of ICU patients. Thus, providing the family with needed information could increase their understanding and reduce their psychological symptoms, including stress [22]. Azizi et al., in their study entitled “the effectiveness of informational support on the level of anxiety in family caregivers of hemiplegic stroke patients”, showed that the educational intervention and information provision about the nature of the disease, symptoms, treatment, and the required care could significantly reduce stress in the intervention group [23]. In another similar study, Shoushi et al. implemented a family-centered care program on depression, anxiety, and stress of family caregivers of open-heart surgery patients. This study confirmed the program’s effectiveness in reducing caregivers’ stress [24]. Considering that part of the stress and anxiety in epidemic diseases is induced by the unknown nature of the disease and the fear of infection of the disease [8, 25], educational support and family-based training are essential to reduce stress and anxiety induced for the reasons mentioned above.
As the present study showed, implementing the family-centered educational program decreased anxiety in the experimental group compared to the control. The findings reported by Jabbarpour et al. also showed that providing information about the patient’s condition reduced anxiety in the intervention group [26]. Zakerimoghadam et al. also showed that implementing the nursing support program can reduce depression and anxiety in patients’ families during surgery [27]. Also, the research findings by Shoushi et al. confirmed the reduction of anxiety in a patient’s caregiver during an open-heart surgery following the implementation of a family-based care program [24].
Asgharpoor et al. and Lim Chiang et al. managed to reduce anxiety in the families of intensive care unit patients using mobile phones and an educational program [28, 29].
Because part of the anxiety of the patient’s family is due to the lack of knowledge about the process of the disease and the patient’s condition, the family-centered educational program can be effective in reducing the anxiety of the patient’s caregivers by providing the necessary information about the disease and the patient’s condition.
Golaghaie et al. also explored the effect of a family-centered clinical intervention on the anxiety of family members of patients admitted to the intensive care units (ICUs). This study showed a significant difference between the mean anxiety score on the second day of intervention and the control group. Yet, the anxiety score of the intervention group on the sixth day of hospitalization was higher than the control group. This finding is not in agreement with the present study [30]. The reason may be due to the prolonged contact of the family with the patient during the stay in the ICU, as patients in the ICU are in a worse condition than those infected with COVID-19, and observing critical conditions, equipment connected to the patient’s body, and seeing other patients can significantly add to the anxiety. Moreover, the family members feel helpless in the ICUs, and any talk about or news from the staff acts as a stressor which can lead to an anxiety-provoking reaction. Also, individual training for caregivers and providing information may be another reason for the different findings. The limitations of this study included receiving information from other sources and individual differences and the psychological state of the research units when answering the questions, which could affect their answers. Also, this study was conducted on caregivers of hospitalized patients, and therefore it is suggested that further studies be conducted on caregivers of hospitalized patients at home under similar conditions.
5. Conclusion
Regarding the present findings, educating caregivers of patients with COVID-19 can reduce their stress and anxiety by raising their awareness of self- and patient-care. It lowers the psychological burden and improves their adaptation. Therefore, it is suggested to use this program as a part of the healthcare system to reduce the patients’ and families’ problems and increase the efficiency of the health system.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted following the guidelines of the Declaration of Helsinki, and all procedures involving study participants was approved by the Deputy of Research at Gonabad University of Medical Sciences (Code: IR.GMU.REC.1399.118). Verbal informed consent was obtained from all subjects
Funding
This paper is part of the Mohammadjamal Tayarani Darbandi’s master’s thesis and was approved by Gonabad University of Medical Sciences (Code: 275/99).
Authors' contributions
Conceptualization, design, data collection, result interpretation, writing the first draft of the paper, and final approval: Mohammadjamal Tayarani Darbandi; Work supervision, writing the initial draft of the paper and final approval: Reza Noori; Project design, data analysis, and interpretation: Morteza Rostamian and Mohammadreza Mansoorian; Reading and approval of the final manuscript: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express gratitude to the staff of the inpatient ward of COVID-19 patients in Allameh Bohlool Gonabadi Hospital, who cooperated in this research, and the research participants.
References
- Nasirzadeh M, Akhondi M, Jamalizadeh Nooq A, Khorramnia S. [A survey on stress, anxiety, depression and resilience due to the prevalence of COVID-19 among Anar City households in 2020: A short report (Persian)]. J Rafsanjan Univ Med Sci. 2020; 19(8):889-98. [DOI:10.29252/jrums.19.8.889]
- Tafet GE. Introduction to the study of stress. In: Tafet GE, editor. Neuroscience of stress. New York: Springer; 2022. [Link]
- Santabarbara J, Idoiaga N, Ozamiz-Etxebarria N, Bueno-Notivol J. Prevalence of anxiety in dental students during the COVID-19 outbreak: A meta-analysis. Int J Environ Res Public Health. 2021; 18(20):10978. [DOI:10.3390/ijerph182010978] [PMID] [PMCID]
- Rehman U, Shahnawaz MG, Khan NH, Kharshiing KD, Khursheed M, Gupta K, et al. Depression, anxiety and stress among Indians in times of Covid-19 lockdown. Community Ment Health J. 2021; 57(1):42-8. [DOI:10.1007/s10597-020-00664-x] [PMID] [PMCID]
- Jani S, mikaeili N, Rahimi P. [The effectiveness of internet-delivered cognitive behaviour therapy on reducing corona-related anxiety in parsabad health care workers (Persian)]. Inf Commun Technol Educ Sci. 2020; 10(40):129-45. [Link]
- Amirfakhraei A, Masoumifard M, Esmaeilishad B, DashtBozorgi Z, Darvish Baseri L. [Prediction of corona virus anxiety based on health concern, psychological hardiness, and positive meta-emotion in diabetic patients (Persian)]. J Diabetes Nurs. 2020; 8(2):1072-83. [Link]
- Mohammadi MT, Shahyad S. [Health anxiety during viral contagious diseases and COVID-19 outbreak: Narrative review (Persian)]. J Mil Med. 2020; 22(6):623-31. [DOI:10.30491/JMM.22.6.623]
- Karimi L, Khalili R, Nir MS. [Prevalence of various psychological disorders during the COVID-19 pandemic: Systematic review (Persian)]. J Mil Med. 2020; 22(6):648-62. [DOI:10.30491/JMM.22.6.648]
- Abolmaali Alhosseini K. [Psychological and instructional consequences of corona disease (Covid-19) and coping strategies with them (Persian)]. Educ Psychol. 2020; 16(55):157-93. [DOI:10.22054/jep.2020.52371.2993]
- Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020; 51:102083 [DOI:10.1016/j.ajp.2020.102083] [PMID] [PMCID]
- Rajkumar RP. COVID-19 and mental health: A review of the existing literature. Asian J Psychiatr. 2020; 52:102066.[DOI:10.1016/j.ajp.2020.102066] [PMID] [PMCID]
- Ma YF, Li W, Deng HB, Wang L, Wang Y, Wang PH, et al. Prevalence of depression and its association with quality of life in clinically stable patients with COVID-19. J Affect Disord. 2020; 275:145-48. [DOI:10.1016/j.jad.2020.06.033] [PMID] [PMCID]
- Nie XD, Wang Q, Wang MN, Zhao S, Liu L, Zhu YL, et al. Anxiety and depression and its correlates in patients with coronavirus disease 2019 in Wuhan. Int J Psychiatry Clin Pract. 2021; 25(2):109-14. [DOI:10.1080/13651501.2020.1791345] [PMID]
- Madani FS, Zarani F. [Managing chronic illness in the family: A systematic review (Persian)]. J Fam Res. 2022; 18(1):57-73. [DOI:10.52547/JFR.18.1.57]
- Rajabzadeh Z, Moudi Z, Abbasi A , Miri-Aliabad G. The effect of family-centered educational supportive intervention on parental stress of premature infants hospitalized in the NICU. Med Surg Nurs J. 2020; 9(3):e111847. [DOI:10.5812/msnj.111847]
- Lin CJ, Cheng YI, Garvie PA, D'Angelo LJ, Wang J, Lyon ME. The effect of family-centered (FACE®) pediatric advanced care planning intervention on family anxiety: A randomized controlled clinical trial for adolescents with HIV and their families. J Fam Nurs. 2020; 26(4):315-26.[DOI:10.1177/1074840720964093] [PMID] [PMCID]
- Heydarpour S, Salari N, Abasi P, Shadab P. The effect of supportive-educational interventions on stress and adaptation to maternal role: A quasi-experimental study. Matern Child Health J. 2022; 26(12):2466-75. [DOI:10.1007/s10995-022-03512-4] [PMID]
- Kaslow NJ, Dunn SE, Henry T, Partin C, Newsome J, O'Donnell C, et al. Collaborative patient- and family-centered care for hospitalized individuals: Best practices for hospitalist care teams. Fam Syst Health. 2020; 38(2):200-8. [DOI:10.1037/fsh0000479] [PMID]
- Hart JL, Turnbull AE, Oppenheim IM, Courtright KR. Family-centered care during the COVID-19 Era. J Pain Symptom Manage. 2020; 60(2):e93-7. [DOI:10.1016/j.jpainsymman.2020.04.017] [PMID] [PMCID]
- Ghafari S, Ahmadi F, Nabavi M, Memarian R. [Effects of applying progressive muscle relaxation technique on depression, anxiety and stress of multiple sclerosis patients in Iran National MS Society (Persian)]. Res Med. 2008; 32(1):45-53. [Link]
- Moradipanah F, Mohammadi E, Mohammadil AZ. Effect of music on anxiety, stress, and depression levels in patients undergoing coronary angiography. East Mediterr Health J. 2009; 15(3):639-47. [DOI:10.26719/2009.15.3.639] [PMID]
- Navidian A, Rezaei J, Payan H. [Efficacy of supportive - educational intervention on psychological reactions of family members of intensive care unit patients (Persian)]. J Nurs Educ. 2016; 5(4):51-8. [DOI:10.21859/jne-05047]
- Azizi A, Khatiban M, Mollai Z, Mohammadi Y. Effect of informational support on anxiety in family caregivers of patients with hemiplegic stroke. J Stroke Cerebrovasc Dis. 2020; 29(9):105020. [DOI:10.1016/j.jstrokecerebrovasdis.2020.105020] [PMID]
- Shoushi F, Jannati Y, Mousavinasab N, Shafipour V. [The impact of family centered care on depression, anxiety and stress of family caregivers of patients undergoing open heart surgery (Persian)]. Iran J Rehabil Res Nurs. 2017; 3(2):53-60. [Link]
- Alipour A, Ghadami A, Alipour Z, Abdollahzadeh H. [Preliminary validation of the corona disease anxiety scale (CDAS) in the Iranian sample (Persian)]. J Health Psychol. 2020; 8(32):163-74. [DOI:10.30473/hpj.2020.52023.4756]
- Jabbarpour M, Abdoli F, Kazemi M. [The effect of providing information about the patient’s condition on the anxiety level of the family members of hospitalized patients with traumatic brain injury (Persian)]. Hayat. 2018; 24(2):127-39. [Link]
- Zakerimoghadam M, Ghiasvandian S, Salahshoor P, kazemnezhad A. [The effect of supportive nursing program on depression, anxiety and stress of family members of patients during coronary artery bypass graft (CABG) surgery (Persian)]. Cardiovasc Nurs J. 2014; 3(1):50-8. [Link]
- Asghar Poor R, Hemmati Maslakpak M, Alinejad V. [The effect of needs - based training on the level of the anxiety of families of patients undergoing coronary artery bypass graft surgery (Persian)]. J Nurs Midwifery Urmia Univ Med Sci. 2016; 14(8):665-73. [Link]
- Chiang VCL, Lee RLP, Ho MF, Leung CK, Tang PY, Wong SW, et al. Fulfilling the psychological and information need of the family members of critically ill patients using interactive mobile technology: A randomised controlled trial. Intensive Crit Care Nurs. 2017; 41:77-83. [DOI:10.1016/j.iccn.2017.03.006] [PMID]
- Golaghaie F, Hekmatpour D, Vafaie M, Rafeie M, Rafiei F. [Effect of a family-centered clinical intervention on the anxiety of family members of the patients hospitalized in critical care units (Persian)]. J Gorgan Univ Med Sci. 2016; 18(3):7-13. [Link]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2023/01/1 | Accepted: 2023/03/1 | Published: 2023/05/28
Received: 2023/01/1 | Accepted: 2023/03/1 | Published: 2023/05/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
