

Volume 13, Issue 4 (Jul & Aug 2023)
J Research Health 2023, 13(4): 263-272 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gharibi F, Imani A, Haghi M, Khezri A, Joudyian N, Ebrahimi Tavani M et al . Quality of Life and Its Relative Factors Among Patients With Multiple Sclerosis: A Cross-sectional Study in Northwest Iran. J Research Health 2023; 13 (4) :263-272
URL: http://jrh.gmu.ac.ir/article-1-2241-en.html
URL: http://jrh.gmu.ac.ir/article-1-2241-en.html
Farid Gharibi1 

 , Ali Imani2 , Mehdi Haghi3 , Ali Khezri4 , Nasrin Joudyian5 , Masoumeh Ebrahimi Tavani6 , Koustuv Dalal7
, Ali Imani2 , Mehdi Haghi3 , Ali Khezri4 , Nasrin Joudyian5 , Masoumeh Ebrahimi Tavani6 , Koustuv Dalal7
, Ali Imani2 , Mehdi Haghi3 , Ali Khezri4 , Nasrin Joudyian5 , Masoumeh Ebrahimi Tavani6 , Koustuv Dalal7
1- Social Determinants of Health Research Center, Semnan University of Medical Sciences, Semnan, Iran.
2- Tabriz Health Services Management Research Center, Tabriz University of Medical Sciences, Tabriz, Iran. ,ali58imani@gmail.com
3- Social Determinants of Health Research Center, School of Health and Nutrition, Lorestan University of Medical Sciences, Khorramabad, Iran.
4- Clinical Research Development Unit of Tabriz Valiasr Hospital, Tabriz University of Medical Sciences, Tabriz, Iran.
5- Department of Health Services Management, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, Iran.
6- Department of Quality Improvement, Monitoring and Evaluation, Center of Health Network Management, Deputy of Public Health, Ministry of Health & Medical Education, Tehran, Iran.
7- Department of Public Health Science, School of Health Sciences, University of Skovde, Sweden and Higher School of Public Health, Kazakh National University, Almaty, Kazakhstan.
2- Tabriz Health Services Management Research Center, Tabriz University of Medical Sciences, Tabriz, Iran. ,
3- Social Determinants of Health Research Center, School of Health and Nutrition, Lorestan University of Medical Sciences, Khorramabad, Iran.
4- Clinical Research Development Unit of Tabriz Valiasr Hospital, Tabriz University of Medical Sciences, Tabriz, Iran.
5- Department of Health Services Management, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, Iran.
6- Department of Quality Improvement, Monitoring and Evaluation, Center of Health Network Management, Deputy of Public Health, Ministry of Health & Medical Education, Tehran, Iran.
7- Department of Public Health Science, School of Health Sciences, University of Skovde, Sweden and Higher School of Public Health, Kazakh National University, Almaty, Kazakhstan.
Full-Text [PDF 830 kb]
(863 Downloads)
| Abstract (HTML) (3273 Views)
Full-Text: (972 Views)
1. Introduction
Multiple sclerosis (MS) is a complicated chronic and inflammatory disorder of the central nervous system (CNS) with the main characteristic of demyelination and loss of neuronal axons, resulting in malfunction and disabilities [1, 2]. Epidemiological studies have shown that the prevalence of MS is about 150 100 000 people [3]. MS generally affects young adults causing long-lasting disabilities during the productive age of the patients and imposing many clinical and socioeconomic burdens [4].
The cause of MS is still unclear and the prognosis of its improvement is very difficult. Although MS does not affect life expectancy, 50% of the cases, after 10 years of the diagnosis, face main problems of movement and need others’ support [5]. Most patients with major disabilities need informal and specialized care services from their families [5]. MS has significant negative effects on the quality of life (QoL) among patients. For instance, in Switzerland, it causes a loss of 0.3 in the quality-adjusted life years (QALY) index of different ages and genders [6]. By the QoL, we mean “patients’ perception of their life conditions demonstrated according to their expectations, goals, norms, and concerns” [7].
With high prevalence, early occurrence in productive ages, long-term survival after the diagnosis, and destructive effects on patients and families, MS is one of the main challenges of public health in different societies [8, 9]. It is the second cause of neurodegenerative disorders in working-age among adults making 50% to 80% of patients to be unemployed 10 years after the disease occurrence. MS usually begins with symptoms, such as sensory disturbances, inflammation of unilateral optic neuritis, diplopia, lhermitte, limb weakness, poor coordination, and gait ataxia [10, 11].
MS causes progressive disorder whose symptoms appear gradually. About half of the patients are unable to do their home and work tasks after ten years of disease occurrence. After 15 years, half of them cannot walk without help. After 25 years and half of them need to use a wheelchair [12]. MS also causes a wide range of other disorders, such as depression, disappointment, cognitive disorders, lack of independence, pain, fatigue, anxiety, dysthymia, social problems, lack of confidence, and neuronal symptoms [13]. This emphasizes proper evaluation and management of the effects on different physical, psychological, behavioural, and social features of MS patients [14]. Studies are available from the Organization for Economic Co-operation and Development (OECD) countries [15]. However, there is a dearth of literature from the low- and middle-income countries (LMICs), such as Iran [16].
Objectives
Therefore, the current study was conducted to assess the QoL of MS patients in East Azerbaijan Province, Iran. Also, the relationship between QoL and demographic and background variables of the MS patients was explored.
2. Methods
Participants
The current cross-sectional study was conducted between April 21 and May 28, 2018. Three hundred patients were randomly selected from the MS patients register in East Azerbaijan Province, Iran. The sample size was allocated using the Morgan table [15]. The inclusion criteria were that the MS patient was registered in the MS society and had received medical treatment for at least one year. The exclusion criteria of the patients from the study included their suffering from skeletal-muscular diseases.
Selection
All MS patients are registered in the MS society of the East Azerbaijan Province. First, we have assigned numerical codes to all the 1200 registered MS patients. We have determined a sample size of 300 MS patients. Second, we selected patient number two as the first selected randomly. Finally, we have selected every fourth patient starting from two (e.g. 2, 6, 10, 14....) to reach 300 MS patients. If any selected MS patient was not willing to participate, we invited the next person for the study interview.
Study tool
This study was conducted using the Multiple Sclerosis Quality of Life-54 (MSQoL-54) Iranian standard version [11]. Questions on the demographic and background variables of patients were added. Twelve dimensions of the questionnaire were divided into two parts of physical health (physical problems, physical role limitations, pain, health perception, and sexual function), and psychological health (emotional role limitation, emotional well-being, cognitive function, social function, health distress, and life satisfaction). QoL scores were 0-100 with the highest number indicating the highest quality. Data were collected via interview with the MS patients.
Data analysis
Mean±SD was presented. We used the t-test, analysis of variance (ANOVA), and Tukey test to assign the relationships between the score of QoL and demographic variables. SPSS software, version 19 was used. P˂0.05 was considered to be significant.
3. Results
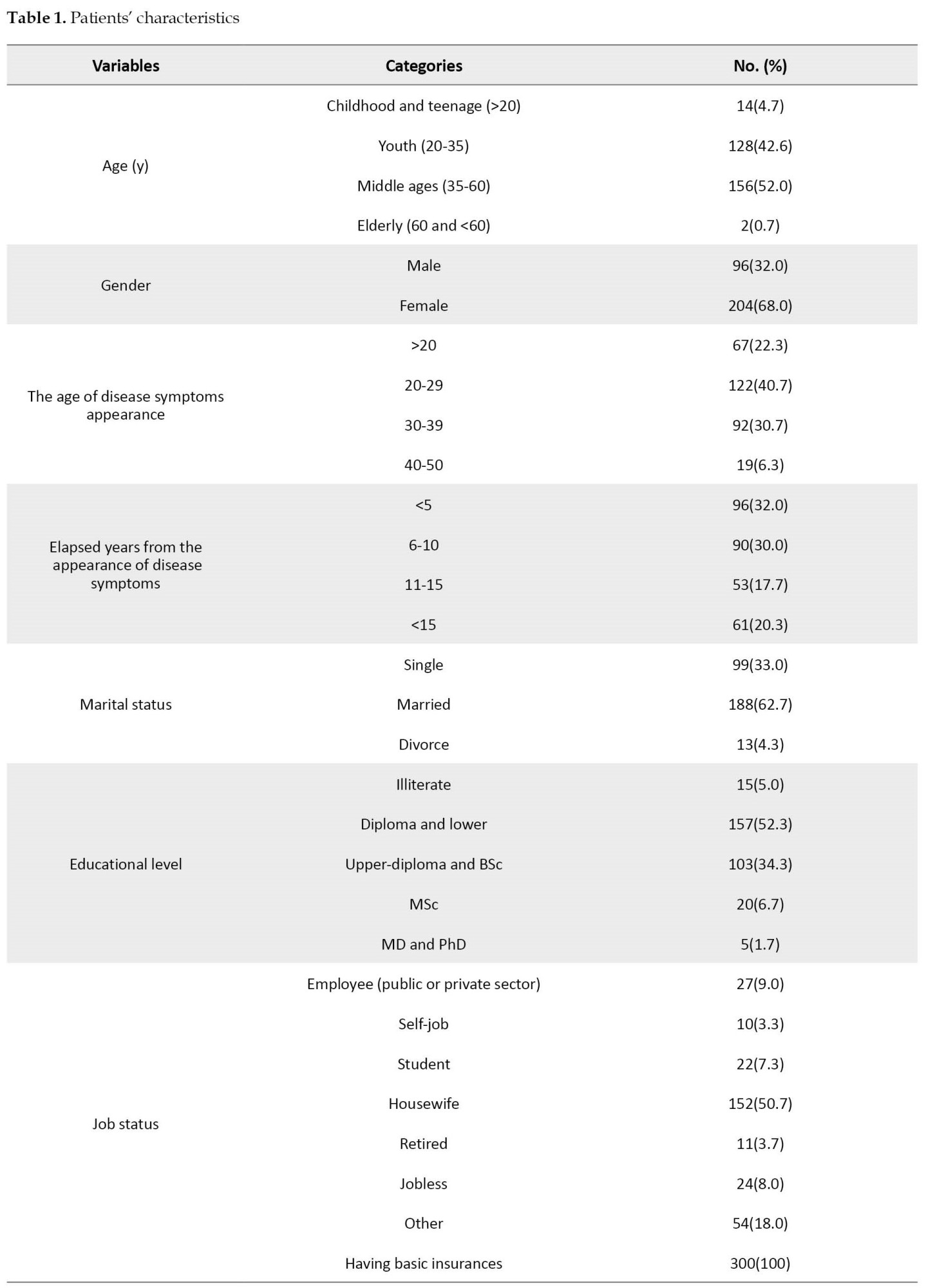
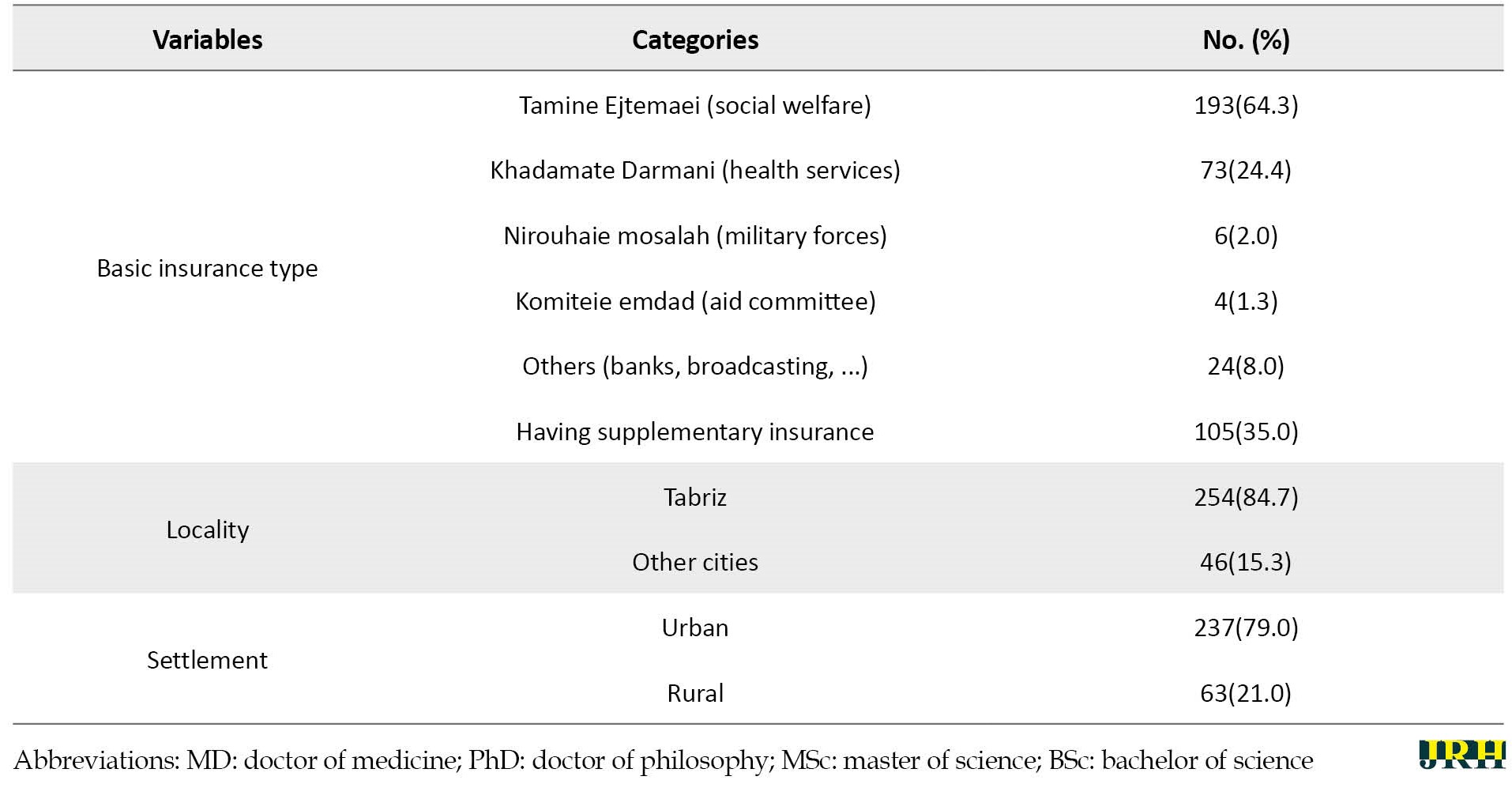
Most of the patients were middle-aged and about two third of them were women. Most patients were 20-40 years old, married, housewives, urban, and residents of Tabriz City, Iran, and had diploma and lower levels of education. All patients had basic social security insurance and one-third of them had supplementary insurance (Table 1).
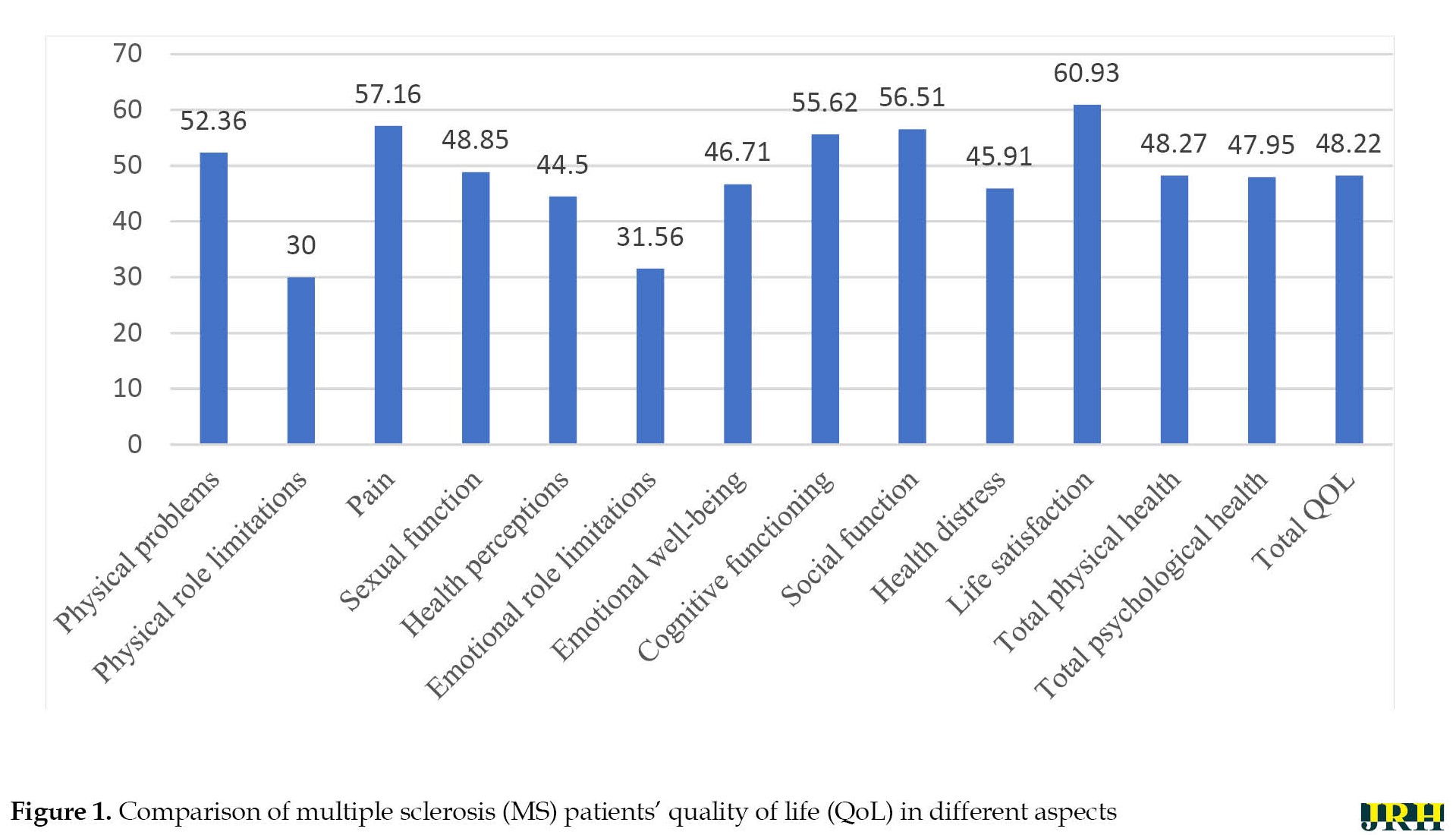
By studying QoL among the patients in different dimensions, it was revealed that they had the most problems with “physical role limitations”, “emotional role limitations” and “health perception” and fewer problems with “life satisfaction”, “pain”, and “social function”. Dimensions of “total physical health”, “total psychological health” and “total QoL” obtained 48.27± 26.28, 47.95±21.39, and 48.22±22.48 score, respectively (Table 2).
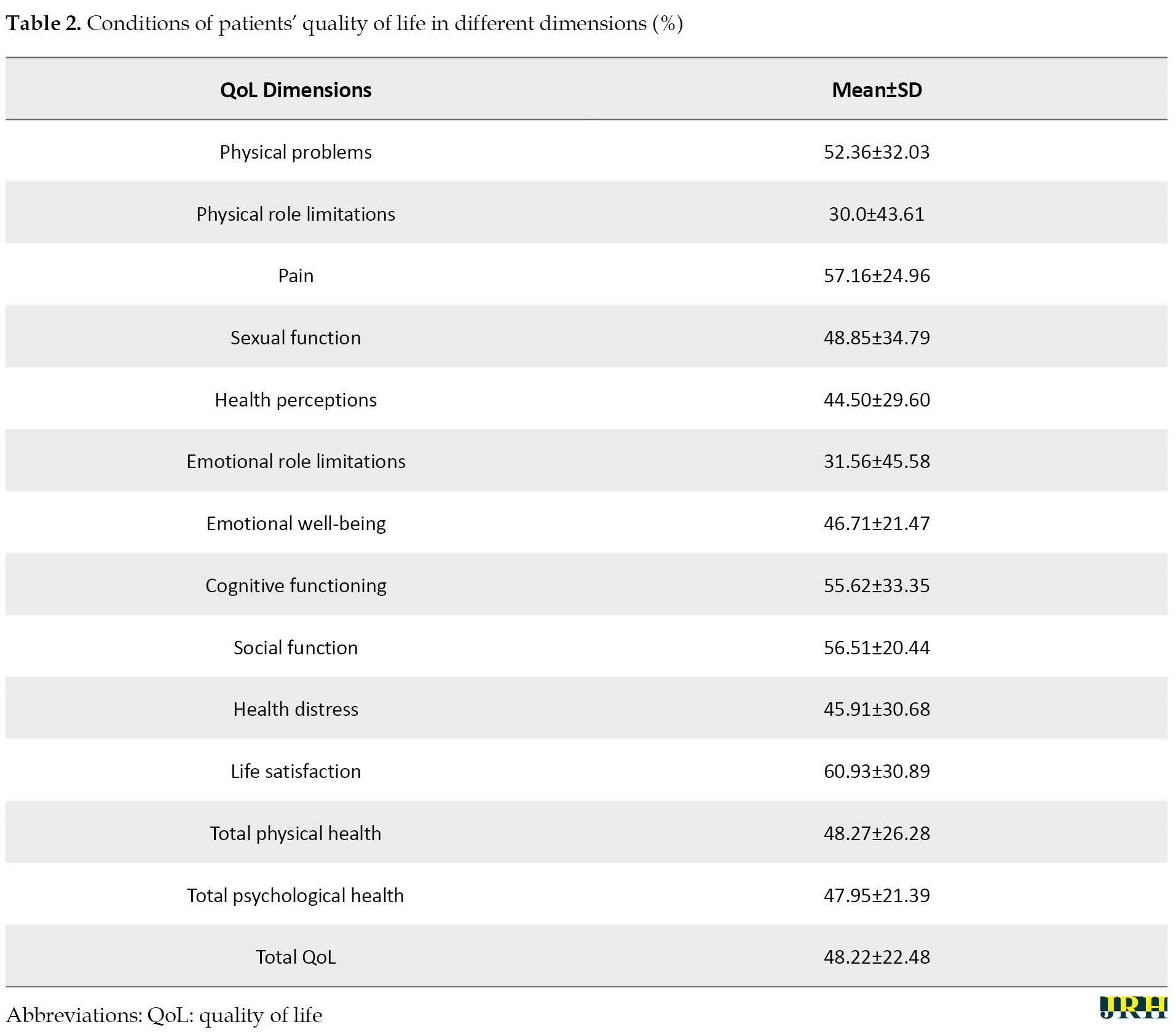
Figure 1 illustrates QoL of MS patients in different dimensions using bar chart.
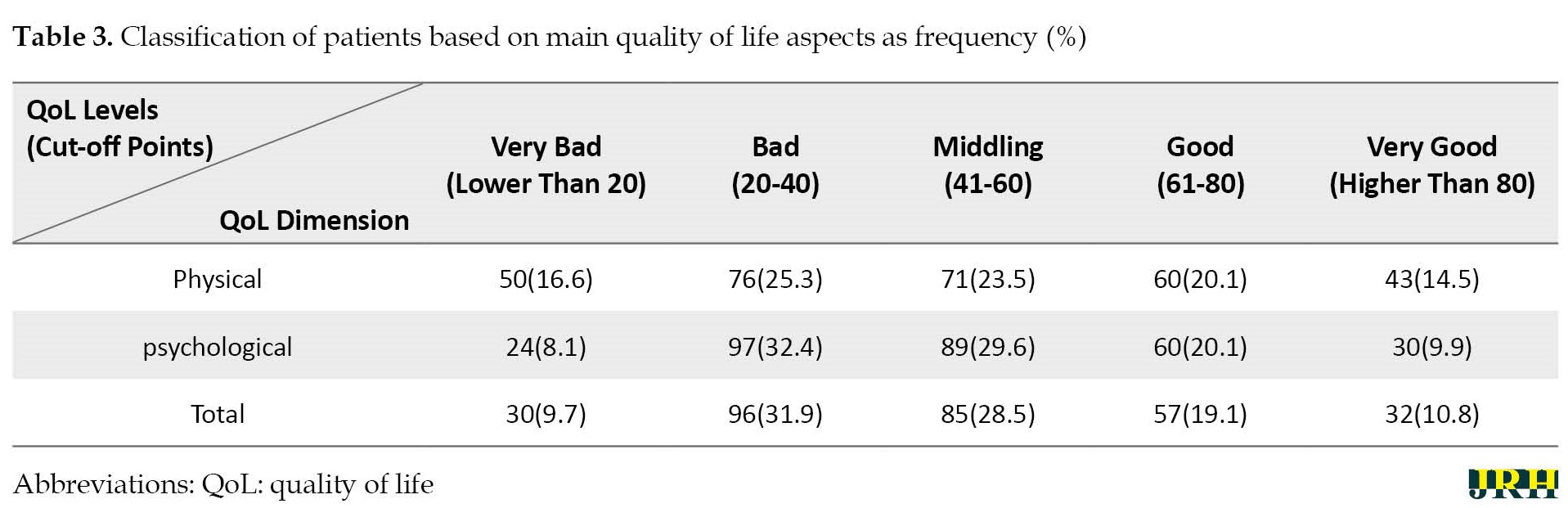
 Based on the ratings of scores of QoL, more than 40% of the MS patients had poor QoL. Only 30% evaluated that their QoL was at the appropriate level (Table 3).
Based on the ratings of scores of QoL, more than 40% of the MS patients had poor QoL. Only 30% evaluated that their QoL was at the appropriate level (Table 3).
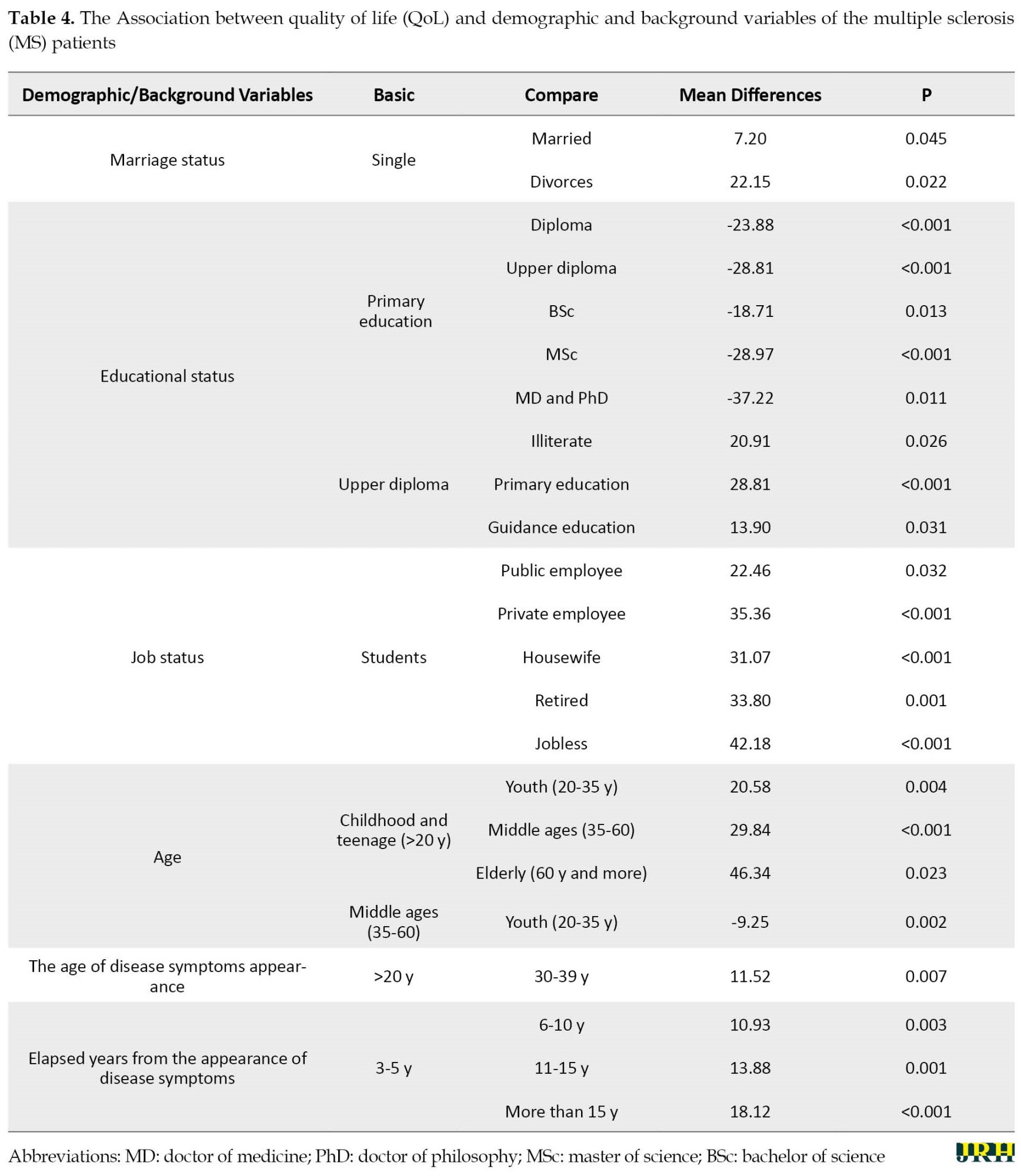
A statistically significant relationship was observed between marital status, education, job, age of disease symptoms appearance, and disease elapsed years (P˂0.05). The type of insurance, gender, basic and supplementary insurance, and urban or native patients did not affect the score of their QoL (P˃0.05). Single people had significantly higher levels of QoL compared to married and especially divorced people. MS patients with primary school education had lower levels of QoL compared to their peers with diploma and university degrees. People with post-diploma degree had better QoL than patients with high school degrees of education. Patients who were university or school students had higher QoL compared to the others. Age was another affecting variable on QoL. Children and teens had significantly higher levels of QoL compared to other age groups. The same trend was present when we compared young patients with middle-aged patients. People who diagnosed their MS when they were ˂20 years had higher level of QoL compared to the people who were living in the fourth decade of their lives. People with less than 5 years of post-disease diagnosis had also higher levels of QoL compared to the others (Table 4).
4. Discussion
The present study was conducted to investigate QoL in MS patients in East Azerbaijan Province. The results showed that dimensions of “total physical health”, “total psychological health” and “total QoL” obtained 48.27%, 47.95%, and 48.22%, respectively. A study conducted by Choobforouszade et al calculated these scores to be 51.34%, 45.06%, and 55.96%, respectively [17]. Also, the mean score of total QoL was 56.2 in the study conducted by Haresabadi et al [16], it was 44.8 in Masoodi et al’s study [18], it was 65.5 in Mohammad et al.’s study [19], it was 48.5 in Hazrati et al’s study [20], and it was calculated to be 22.7 in Marghati Khoei et al.’s study [21]. In high-income countries, such as Italy, Netherlands, Spain, France, Turkey, and the United States, the score of QoL among MS patients was reported to be more than 65 [22]. QoL among MS patients in Iran is lower than patients from America and European countries. The probable reason can be insufficient quality and ineffective quantity of healthcare services received by the Iranian MS patients and the absence of socioeconomic support.
The current study indicates that “life satisfaction” has the highest and “physical role limitations“ has the lowest score of QoL. In the study conducted by Haresabadi et al, the lowest and highest score was respectively related to “physical role limitation” and “cognitive functioning” [16]. Marghati Khoei et al. also allocated the highest score to “emotional role limitations” and the lowest score to “health perceptions” and “emotional well-being” jointly [21]. In the study conducted by Sangelaji et al., the highest and lowest scores of QoL were respectively related to “pain” and “physical role limitations” [23]. Choobforouszade et al.’s study allocated the highest and lowest QoL scores to “social function” and “physical role limitations”, respectively [17]. The lowest and highest scores were related to “social function” and “physical role limitations” in the study conducted by Mohammad et al. [19]. In most studies conducted in other countries, physical problems, especially fatigue was considered the most disturbing negative consequences of MS [22]. Comparison of present findings with other literature (especially inside the country) suggested that “physical role limitations” was the worst dimension of QoL among the MS patients in Iran because they receive insufficient healthcare which is not enough to solve their physical problems for performing their jobs. Single MS patients had the highest level of QoL compared to divorced and married individuals.
The current study has demonstrated a statistically significant relationship between education, age, gender, and disease elapsed time with QoL scores, which is consistent with the study conducted by Choobforouszade et al. [17] or by Pfaffenberger et al. [24].
The present study was the first evaluation of the QoL among MS patients in the northwest of Iran that tried to investigate the relationship between a wide range of demographic and background variables and MS patients’ QoL. The limitation was the problem of interviewing the sick and home-staying MS patients due to their unwillingness to participate in the study. Based on the results, suggestions, such as promoting a basic and supplementary insurance system upon United Healthcare (UHC) principles, promoting social security system, enhancing governmental and charitable support, and promoting and developing social work system by considering MS patients’ physical capabilities, designing MS care centers for providing comprehensively and quality cares, and on-time supply of MS drugs are warranted. Similar studies in other parts of the country and in low and middle-income countries are warranted to identify different dimensions of disease and to better recognize the clinical and socioeconomic consequences of the disease.
5. Conclusion
This investigation showed that QoL among East Azerbaijan MS patients is not at its desired level and different factors play a vital role. The current results can help health policymakers to eliminate existing challenges faced by MS patients and provide them with more quality clinical care and desired socioeconomic support.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted after approving by the Ethics Committee and receiving an ethical code from Tabriz University of Medical Science (Code: IR.TBZMED.REC.1396.101).
Funding
The study was supported financially by Tabriz University of Medical Science.
Authors' contributions
Study design: Farid Gharibi, Ali Imani, Koustuv Dalal; Data collection: Farid Gharibi, Mehdi Haghi, Ali Khezri, Nasrin Joudyian, Masoumeh Ebrahimi Tavani; Data analysis: Farid Gharibi, Koustuv Dalal, Mehdi Haghi, Masoumeh Ebrahimi Tavani; Drafting of the manuscript: Farid Gharibi, Ali Imani, Ali Khezri, Nasrin Joudyian; Critical appraisal: Koustuv Dalal, Mehdi Haghi, Masoumeh Ebrahimi Tavani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank all the patients for their participation in this study, and Tabriz Health Services Management Research Center for its financial support.
References
Multiple sclerosis (MS) is a complicated chronic and inflammatory disorder of the central nervous system (CNS) with the main characteristic of demyelination and loss of neuronal axons, resulting in malfunction and disabilities [1, 2]. Epidemiological studies have shown that the prevalence of MS is about 150 100 000 people [3]. MS generally affects young adults causing long-lasting disabilities during the productive age of the patients and imposing many clinical and socioeconomic burdens [4].
The cause of MS is still unclear and the prognosis of its improvement is very difficult. Although MS does not affect life expectancy, 50% of the cases, after 10 years of the diagnosis, face main problems of movement and need others’ support [5]. Most patients with major disabilities need informal and specialized care services from their families [5]. MS has significant negative effects on the quality of life (QoL) among patients. For instance, in Switzerland, it causes a loss of 0.3 in the quality-adjusted life years (QALY) index of different ages and genders [6]. By the QoL, we mean “patients’ perception of their life conditions demonstrated according to their expectations, goals, norms, and concerns” [7].
With high prevalence, early occurrence in productive ages, long-term survival after the diagnosis, and destructive effects on patients and families, MS is one of the main challenges of public health in different societies [8, 9]. It is the second cause of neurodegenerative disorders in working-age among adults making 50% to 80% of patients to be unemployed 10 years after the disease occurrence. MS usually begins with symptoms, such as sensory disturbances, inflammation of unilateral optic neuritis, diplopia, lhermitte, limb weakness, poor coordination, and gait ataxia [10, 11].
MS causes progressive disorder whose symptoms appear gradually. About half of the patients are unable to do their home and work tasks after ten years of disease occurrence. After 15 years, half of them cannot walk without help. After 25 years and half of them need to use a wheelchair [12]. MS also causes a wide range of other disorders, such as depression, disappointment, cognitive disorders, lack of independence, pain, fatigue, anxiety, dysthymia, social problems, lack of confidence, and neuronal symptoms [13]. This emphasizes proper evaluation and management of the effects on different physical, psychological, behavioural, and social features of MS patients [14]. Studies are available from the Organization for Economic Co-operation and Development (OECD) countries [15]. However, there is a dearth of literature from the low- and middle-income countries (LMICs), such as Iran [16].
Objectives
Therefore, the current study was conducted to assess the QoL of MS patients in East Azerbaijan Province, Iran. Also, the relationship between QoL and demographic and background variables of the MS patients was explored.
2. Methods
Participants
The current cross-sectional study was conducted between April 21 and May 28, 2018. Three hundred patients were randomly selected from the MS patients register in East Azerbaijan Province, Iran. The sample size was allocated using the Morgan table [15]. The inclusion criteria were that the MS patient was registered in the MS society and had received medical treatment for at least one year. The exclusion criteria of the patients from the study included their suffering from skeletal-muscular diseases.
Selection
All MS patients are registered in the MS society of the East Azerbaijan Province. First, we have assigned numerical codes to all the 1200 registered MS patients. We have determined a sample size of 300 MS patients. Second, we selected patient number two as the first selected randomly. Finally, we have selected every fourth patient starting from two (e.g. 2, 6, 10, 14....) to reach 300 MS patients. If any selected MS patient was not willing to participate, we invited the next person for the study interview.
Study tool
This study was conducted using the Multiple Sclerosis Quality of Life-54 (MSQoL-54) Iranian standard version [11]. Questions on the demographic and background variables of patients were added. Twelve dimensions of the questionnaire were divided into two parts of physical health (physical problems, physical role limitations, pain, health perception, and sexual function), and psychological health (emotional role limitation, emotional well-being, cognitive function, social function, health distress, and life satisfaction). QoL scores were 0-100 with the highest number indicating the highest quality. Data were collected via interview with the MS patients.
Data analysis
Mean±SD was presented. We used the t-test, analysis of variance (ANOVA), and Tukey test to assign the relationships between the score of QoL and demographic variables. SPSS software, version 19 was used. P˂0.05 was considered to be significant.
3. Results
Most of the patients were middle-aged and about two third of them were women. Most patients were 20-40 years old, married, housewives, urban, and residents of Tabriz City, Iran, and had diploma and lower levels of education. All patients had basic social security insurance and one-third of them had supplementary insurance (Table 1).
By studying QoL among the patients in different dimensions, it was revealed that they had the most problems with “physical role limitations”, “emotional role limitations” and “health perception” and fewer problems with “life satisfaction”, “pain”, and “social function”. Dimensions of “total physical health”, “total psychological health” and “total QoL” obtained 48.27± 26.28, 47.95±21.39, and 48.22±22.48 score, respectively (Table 2).
Figure 1 illustrates QoL of MS patients in different dimensions using bar chart.
A statistically significant relationship was observed between marital status, education, job, age of disease symptoms appearance, and disease elapsed years (P˂0.05). The type of insurance, gender, basic and supplementary insurance, and urban or native patients did not affect the score of their QoL (P˃0.05). Single people had significantly higher levels of QoL compared to married and especially divorced people. MS patients with primary school education had lower levels of QoL compared to their peers with diploma and university degrees. People with post-diploma degree had better QoL than patients with high school degrees of education. Patients who were university or school students had higher QoL compared to the others. Age was another affecting variable on QoL. Children and teens had significantly higher levels of QoL compared to other age groups. The same trend was present when we compared young patients with middle-aged patients. People who diagnosed their MS when they were ˂20 years had higher level of QoL compared to the people who were living in the fourth decade of their lives. People with less than 5 years of post-disease diagnosis had also higher levels of QoL compared to the others (Table 4).
4. Discussion
The present study was conducted to investigate QoL in MS patients in East Azerbaijan Province. The results showed that dimensions of “total physical health”, “total psychological health” and “total QoL” obtained 48.27%, 47.95%, and 48.22%, respectively. A study conducted by Choobforouszade et al calculated these scores to be 51.34%, 45.06%, and 55.96%, respectively [17]. Also, the mean score of total QoL was 56.2 in the study conducted by Haresabadi et al [16], it was 44.8 in Masoodi et al’s study [18], it was 65.5 in Mohammad et al.’s study [19], it was 48.5 in Hazrati et al’s study [20], and it was calculated to be 22.7 in Marghati Khoei et al.’s study [21]. In high-income countries, such as Italy, Netherlands, Spain, France, Turkey, and the United States, the score of QoL among MS patients was reported to be more than 65 [22]. QoL among MS patients in Iran is lower than patients from America and European countries. The probable reason can be insufficient quality and ineffective quantity of healthcare services received by the Iranian MS patients and the absence of socioeconomic support.
The current study indicates that “life satisfaction” has the highest and “physical role limitations“ has the lowest score of QoL. In the study conducted by Haresabadi et al, the lowest and highest score was respectively related to “physical role limitation” and “cognitive functioning” [16]. Marghati Khoei et al. also allocated the highest score to “emotional role limitations” and the lowest score to “health perceptions” and “emotional well-being” jointly [21]. In the study conducted by Sangelaji et al., the highest and lowest scores of QoL were respectively related to “pain” and “physical role limitations” [23]. Choobforouszade et al.’s study allocated the highest and lowest QoL scores to “social function” and “physical role limitations”, respectively [17]. The lowest and highest scores were related to “social function” and “physical role limitations” in the study conducted by Mohammad et al. [19]. In most studies conducted in other countries, physical problems, especially fatigue was considered the most disturbing negative consequences of MS [22]. Comparison of present findings with other literature (especially inside the country) suggested that “physical role limitations” was the worst dimension of QoL among the MS patients in Iran because they receive insufficient healthcare which is not enough to solve their physical problems for performing their jobs. Single MS patients had the highest level of QoL compared to divorced and married individuals.
The current study has demonstrated a statistically significant relationship between education, age, gender, and disease elapsed time with QoL scores, which is consistent with the study conducted by Choobforouszade et al. [17] or by Pfaffenberger et al. [24].
The present study was the first evaluation of the QoL among MS patients in the northwest of Iran that tried to investigate the relationship between a wide range of demographic and background variables and MS patients’ QoL. The limitation was the problem of interviewing the sick and home-staying MS patients due to their unwillingness to participate in the study. Based on the results, suggestions, such as promoting a basic and supplementary insurance system upon United Healthcare (UHC) principles, promoting social security system, enhancing governmental and charitable support, and promoting and developing social work system by considering MS patients’ physical capabilities, designing MS care centers for providing comprehensively and quality cares, and on-time supply of MS drugs are warranted. Similar studies in other parts of the country and in low and middle-income countries are warranted to identify different dimensions of disease and to better recognize the clinical and socioeconomic consequences of the disease.
5. Conclusion
This investigation showed that QoL among East Azerbaijan MS patients is not at its desired level and different factors play a vital role. The current results can help health policymakers to eliminate existing challenges faced by MS patients and provide them with more quality clinical care and desired socioeconomic support.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted after approving by the Ethics Committee and receiving an ethical code from Tabriz University of Medical Science (Code: IR.TBZMED.REC.1396.101).
Funding
The study was supported financially by Tabriz University of Medical Science.
Authors' contributions
Study design: Farid Gharibi, Ali Imani, Koustuv Dalal; Data collection: Farid Gharibi, Mehdi Haghi, Ali Khezri, Nasrin Joudyian, Masoumeh Ebrahimi Tavani; Data analysis: Farid Gharibi, Koustuv Dalal, Mehdi Haghi, Masoumeh Ebrahimi Tavani; Drafting of the manuscript: Farid Gharibi, Ali Imani, Ali Khezri, Nasrin Joudyian; Critical appraisal: Koustuv Dalal, Mehdi Haghi, Masoumeh Ebrahimi Tavani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank all the patients for their participation in this study, and Tabriz Health Services Management Research Center for its financial support.
References
- Svendsen B, Myhr KM, Nyland H, Aarseth JH. The cost of multiple sclerosis in Norway. The European Journal of Health Economics. 2012; 13(1):81-91. [DOI:10.1007/s10198-010-0286-7] [PMID] [PMCID]
- Dobson R, Giovannoni G. Multiple sclerosis - a review. European Journal of Neurology. 2019; 26(1):27-40. [DOI:10.1111/ene.13819] [PMID]
- Grytten N, Glad SB, Aarseth JH, Nyland H, Midgard R, Myhr KM. A 50-year follow-up of the incidence of multiple sclerosis in Hordaland County, Norway. Neurology. 2006; 66(2):182-6. [DOI:10.1212/01.wnl.0000195549.95448.b9] [PMID]
- Oh J, Vidal-Jordana A, Montalban X. Multiple sclerosis: Clinical aspects. Current Opinion in Neurology. 2018; 31(6):752-9.[DOI:10.1097/WCO.0000000000000622] [PMID]
- Howard J, Trevick S, Younger DS. Epidemiology of multiple sclerosis. Neurol Clinics. 2016; 34(4):919-39. [DOI:10.1016/j.ncl.2016.06.016] [PMID]
- Young CA, Mills R, Rog D, Sharrack B, Majeed T, Constantinescu CS, et al. Quality of life in multiple sclerosis is dominated by fatigue, disability and self-efficacy. Journal of the Neurological Sciences. 2021; 15(426):117437. [DOI:10.1016/j.jns.2021.117437] [PMID]
- Rosiak K, Zagożdżon P. Quality of life and social support in patients with multiple sclerosis. Psychiatria Polska. 2017; 51(5):923-35. [DOI:10.12740/PP/64709] [PMID]
- Koch-Henriksen N, Magyari M. Apparent changes in the epidemiology and severity of multiple sclerosis. Nature Reviews Neurology. 2021; 17(11):676-88. [DOI:10.1038/s41582-021-00556-y] [PMID]
- Doshi A, Chataway J. Multiple sclerosis, a treatable disease. Clinical Medicine. 2016; 16(Suppl 6):s53-9. [DOI:10.7861/clinmedicine.16-6-s53] [PMID]
- Topcu G, Buchanan H, Aubeeluck A, Garip G. Caregiving in multiple sclerosis and quality of life: A meta-synthesis of qualitative research. Psychology & Health. 2016; 31(6):693-710. [DOI:10.1080/08870446.2016.1139112] [PMID]
- Imani A, Gharibi F, Khezri A, Joudyian N, Dalal K. Economic costs incurred by the patients with multiple sclerosis at different levels of the disease: A cross-sectional study in northwest Iran. BMC Neurology. 2020; 20(1):205. [DOI:10.1186/s12883-020-01790-5] [PMID] [PMCID]
- Confavreux C, Vukusic S, Moreau T, Adeleine P. Relapses and progression of disability in multiple sclerosis.The New England Journal of Medicine. 2000; 343(20):1430-8. [DOI:10.1056/NEJM200011163432001] [PMID]
- Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of life and its assessment in multiple sclerosis: Integrating physical and psychological components of wellbeing. The Lancet Neurology. 2005; 4(9):556-66. [DOI:10.1016/S1474-4422(05)70166-6] [PMID]
- Solari A. Role of health-related quality of life measures in the routine care of people with multiple sclerosis. Health and Quality of Life Outcomes. 2005; 3:16. [DOI:10.1186/1477-7525-3-16] [PMID] [PMCID]
- Gharibi F, Imani A, Dalal K. The catastrophic out-of-pocket health expenditure of multiple sclerosis patients in Iran. BMC Health Services Research. 2021; 21(1):257. [DOI:10.1186/s12913-021-06251-4] [PMID] [PMCID]
- Haresabadi M, Karimi Monaghi H, Froghipor M, Mazlom SR. [Quality of life in patients with multiple sclerosis referring to Ghaem Hospital, Mashhad in 2009 (Persian)]. Journal of North Khorasan University of Medical Sciences. 2011; 2(4):7-12. [DOI:10.29252/jnkums.2.4.7]
- Choobforouszade A, Neshatdoos H, Molavi H, Abedi MR. [Examine the quality of life among multiple sclerosis patients in Yazd MS Association, Iran (Persian)]. Tolou-e-Behdasht Journal. 2016; 14(5):131-40. [Link]
- Masoodi R, Mohammadi E, Nabavi SM, Ahmadi F. [The effect of Orem based self-care program on physical quality of life in multiple sclerosis patients (Persian)]. Shahrekord University of Medical Sciences Journal. 2008; 2(10):21-9. [Link]
- Mohammad K, Rimaz S, Dastoorpour M, Sadeghi M, Majdzadeh SR. [Quality of life and related factors among multiple sclerosis patients (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2014; 11(4):1-14. [Link]
- Hazrati M, Zahmatkeshan N, Dejbakhsh T, Nikseresht A, Zeyghami B. [The effect of rehabilitation process on the quality of life in multiple sclerosis patients (Persian)]. Armaghan-e-Danesh. 2005; 10(3):53-65. [Link]
- Merghati Khoei E, Qaderi K, Amini L, Haghani H. [Study on sexual behavior and quality of life of women with multiple sclerosis referred to Iran MS society in Tehran in 2010 (Persian)]. The Iranian Journal of Obstetrics, Genecology and Infertility. 2012; 15(5):7-14. [DOI:10.22038/IJOGI.2012.5726]
- Janardhan V, Bakshi R. Quality of life in patients with multiple sclerosis: The impact of fatigue and depression. Journal of the Neurological Sciences. 2002; 205(1):51-8. [DOI:10.1016/S0022-510X(02)00312-X] [PMID]
- Sangelaji B, Salimi Y, Dastoorpour M, Mansouri T, Ashrafinia F, Esmaeilzadeh N, et al. The relationship between disability and quality of life in multiple sclerosis patients. Health and Development Journal. 2013; 2(3):203-13. [Link]
- Pfaffenberger N, Pfeiffer KP, Deibl M, Höfer S, Günther V, Ulmer H. Association of factors influencing health-related quality of life in MS. Acta Neurologica Scandinavica. 2006; 114(2):102-8. [DOI:10.1111/j.1600-0404.2006.00659.x] [PMID]
Type of Study: Orginal Article |
Subject:
● Disease Control
Received: 2023/01/17 | Accepted: 2023/04/9 | Published: 2023/06/29
Received: 2023/01/17 | Accepted: 2023/04/9 | Published: 2023/06/29
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
