

Volume 14, Issue 5 (Sep & Oct 2024)
J Research Health 2024, 14(5): 457-466 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadeghi R, Khanjani N, Imani_Goghary Z, Mahmoodabadi F, Masoodi M R, Momenabadi V. Exploring the Experiences of the Employees of Golgohar Industrial Mining Company During the COVID-19 Epidemic. J Research Health 2024; 14 (5) :457-466
URL: http://jrh.gmu.ac.ir/article-1-2343-en.html
URL: http://jrh.gmu.ac.ir/article-1-2343-en.html
Reza Sadeghi1 

 , Narges Khanjani2 , Zahra Imani_Goghary3 , Fatemeh Mahmoodabadi4 , Mahmoud Reza Masoodi5 , Victoria Momenabadi6
, Narges Khanjani2 , Zahra Imani_Goghary3 , Fatemeh Mahmoodabadi4 , Mahmoud Reza Masoodi5 , Victoria Momenabadi6
, Narges Khanjani2 , Zahra Imani_Goghary3 , Fatemeh Mahmoodabadi4 , Mahmoud Reza Masoodi5 , Victoria Momenabadi6
1- Department of Public Health, Sirjan School of Medical Sciences, Sirjan, Iran.
2- Department of Medical Education, Paul L. Foster School of Medicine, Texas Tech Health Sciences Center El Paso, Texas, United States.
3- Department of Nursing and Midwifery, Sirjan School of Medical Sciences, Sirjan, Iran. ,imanigoghary@yahoo.ca
4- Department of Nursing and Midwifery, Sirjan School of Medical Sciences, Sirjan, Iran.
5- Department of Internal Medicine, Sirjan School of Medical Sciences, Sirjan, Iran.
6- Department of Public Health, Bam University of Medical Sciences, Bam, Iran.
2- Department of Medical Education, Paul L. Foster School of Medicine, Texas Tech Health Sciences Center El Paso, Texas, United States.
3- Department of Nursing and Midwifery, Sirjan School of Medical Sciences, Sirjan, Iran. ,
4- Department of Nursing and Midwifery, Sirjan School of Medical Sciences, Sirjan, Iran.
5- Department of Internal Medicine, Sirjan School of Medical Sciences, Sirjan, Iran.
6- Department of Public Health, Bam University of Medical Sciences, Bam, Iran.
Full-Text [PDF 757 kb]
(753 Downloads)
| Abstract (HTML) (3565 Views)
Full-Text: (1086 Views)
Introduction
The coronavirus disease 2019 (COVID-19) rapidly spread around the world and was declared a global emergency by the World Health Organization (WHO) and the International Health Regulations (IHR) Emergency Committee [1]. The COVID-19 pandemic created enormous health, economic, environmental, and social challenges for the entire human population [2, 3]. Some COVID-19 patients exhibit mild or severe symptoms, and some may die because of multiple organ dysfunction; however, a large portion of them are asymptomatic carriers, which can lead to the infection of many others [4].
The COVID‐19 epidemic had a negative impact on occupational health, business sustainability, and individual employment [5, 6]. Employees had to take care of themselves, and their families while maintaining their job positions [7]. Some studies have reported that during the pandemic the need for childcare increased because children had to stay at home, and required attention. Additional responsibilities, including working longer hours and new fears about virus exposure, led to an increase in both work and family demands. Consequently, employees experience work-family conflicts, which can negatively impact their physical and mental well-being [7, 8]. Furthermore, little guidance is available on how resilience levers (i.e. supervision, support, policies, and organizational preparedness for the crisis) may promote worker’s well-being during the COVID-19 pandemic [6].
The COVID-19 pandemic has had an extreme effect on the economy and has caused a drastic reduction in the size and scope of economic activity as well [9]. Some employees were required to take immediate action to change their work styles under the instructions of their companies or organizations. Sasaki et al. suggested that workplace rules and policies may help promote and maintain the mental health and work performance of employees during the COVID-19 epidemic [10]. However, Wong et al. showed that many employees were not satisfied with workplace policies because of their incompleteness, untimeliness, and ambiguity [9]. Previous studies have also stated that workplace policies should be supported by both governmental and organizational settings [9].
Industries are a vital part of a country’s economy and cannot be closed under all circumstances [11]. Despite the challenges posed by the COVID-19 pandemic, many workers were expected to be present at their workplaces. Surprisingly, very few studies have investigated the experiences of industrial workers during this unprecedented time. Sirjan is one of the cities in Iran with large mining industries, such as the Golgohar Industrial Mining Complex, which is known as the largest iron company in the Middle East. This mine, with a reserve of about 1200 million tons, is located in an area approximately 10 km long and approximately 4 km wide. The number of workers and employees exceeds 16,000, who work in two shifts. The incidence of COVID-19 was high among the employees of this complex.
It is important to explore the experiences of industrial employees during the pandemic to identify the weaknesses and strengths of disease control from their perspective. These narratives may help recognize the problems and find solutions to manage unexpected conditions and preserve the well-being of workers. This study aimed to explore the experiences of the employees of Golgohar Mining and Industrial Co. during the COVID-19 pandemic.
Methods
This qualitative content analysis study was conducted in Sirjan, Iran from March 2021 to October 2021.
Population and sampling procedure
Participants were 20 employees of the Golgohar Industrial Mining Company in Sirjan, selected by purposeful sampling. Sampling continued until data saturation was reached, at which point no new information was obtained from the interviews.
The aim of the study was explained to participants, who then signed an informed consent form. Based on the participants’ preferences, a comfortable and private environment was chosen for the interviews, which included the participants’ homes, workplaces, or the campus of Sirjan School of Medical Sciences.
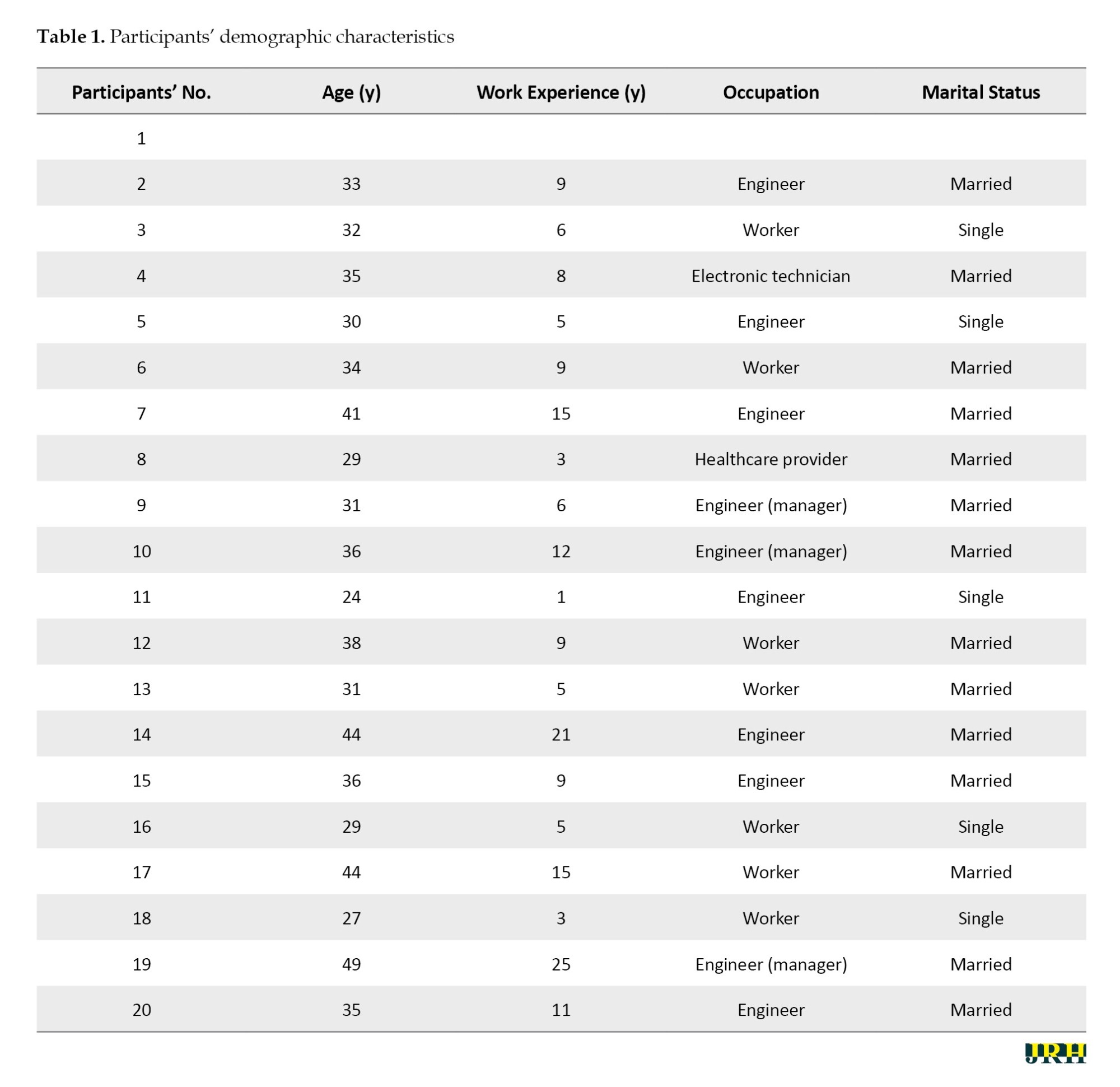
Inclusion criteria included the willingness to participate in the study, being employed by Golgohar Industrial Mining Co., and living in Sirjan. Participants’ demographic characteristics are presented in Table 1.
Data collection method
Data were collected through semi-structured interviews. After greetings, the researcher asked general questions, such as the participants’ age, occupation, and work experience. Then, specific questions related to the main purpose of the research were asked. For example, “How did the COVID-19 epidemic affect your work? What factors contributed to the spread of COVID-19 in your workplace? What interventions were implemented in your workplace for the prevention of COVID-19?” Participants were asked to provide detailed information and explain their responses thoroughly.
Interviews lasted 35 to 50 minutes. In this study, data saturation was achieved from the researchers’ perspective after the 10th interview. However, to ensure greater certainty, a total of 20 interviews were conducted.
Content analysis
Content analysis is a qualitative data analysis method [12]. It includes a systematic process of coding, identification of subcategories and categories, and finally, description of the social reality through the creation of themes [13, 14].
Data analysis
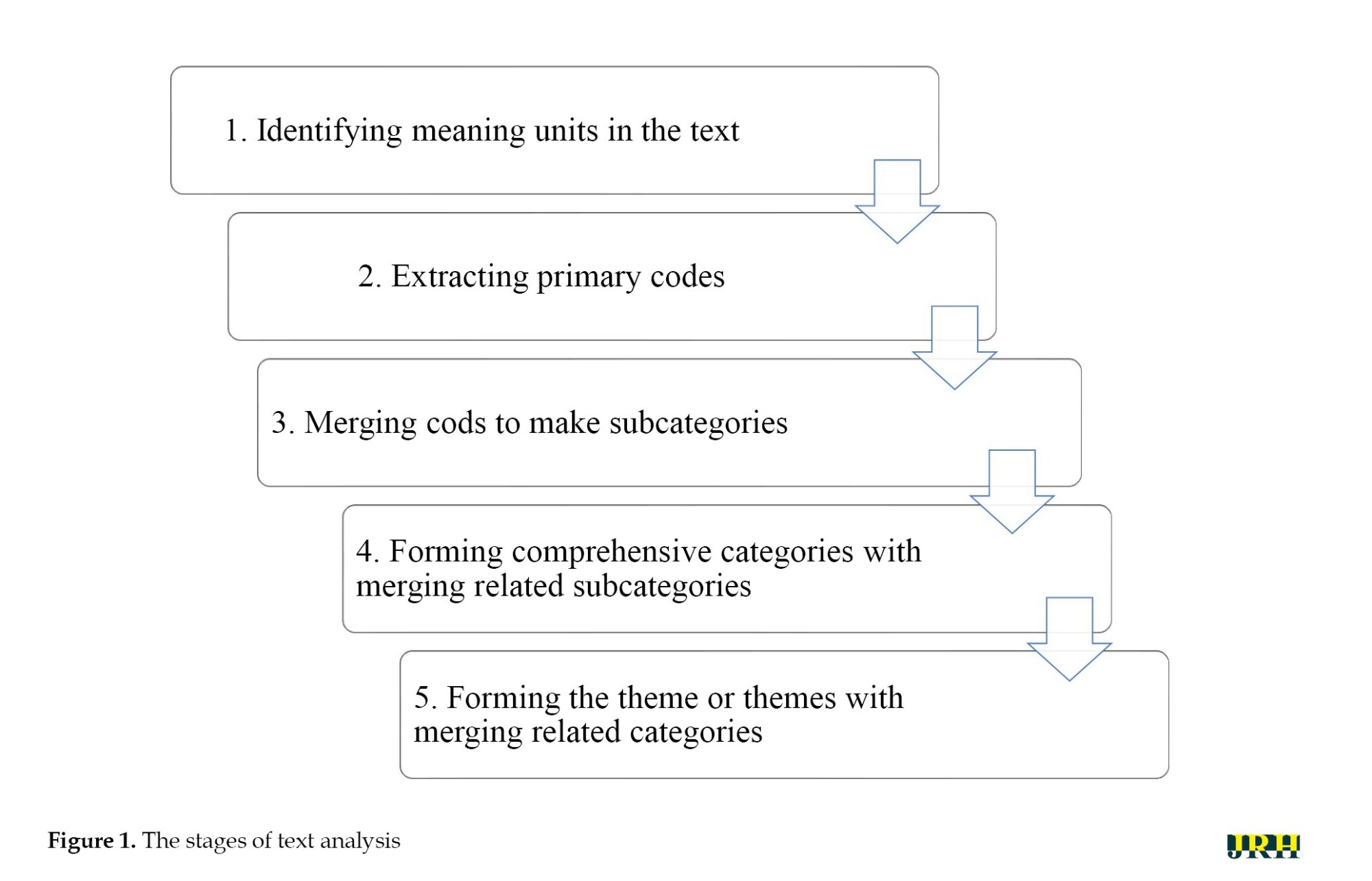
Data analysis was performed concurrently with data collection, according to the method proposed by Graneheim and Lundman, which suggests five steps for qualitative data analysis [15]. According to this method, the interviews were transcribed. The full text of each interview was then read several times to gain a general understanding of its content, followed by an analysis of the interviews (Figure 1).
Rigor
The four criteria of credibility, dependability, confirmability, and transferability were used to ensure the trustworthiness of the data [16]. Credibility was enhanced through interaction with participants, allocating sufficient time for data gathering using open questions, audio recordings of the interviews, and transcribing the interviews word for word, along with analyzing the data using the constant comparative method. Participant reviews and member checks were also used to verify the data and codes. For this purpose, the text of two interpretations was returned to the participants to ensure that the researcher had understood the context, and some corrections were made based on the participants’ comments. The transcripts of the interviews, as well as the extracted codes and categories, were also reviewed by two faculty members, and agreement was achieved. Participants were selected from different ages, genders, various administrative positions, and different recruitment sites. Confirmability and transferability were enhanced by documenting the research process and all related activities, as well as clearly describing the study process and inviting different occupational groups to participate in the study. The findings were recorded in as much detail as possible.
Results
The participants were workers, engineers, healthcare providers, and managers of the Golgohar Copper Complex. They were all male, and their ages ranged from 24 to 49 years. They had between 1 and 24 years of experience.
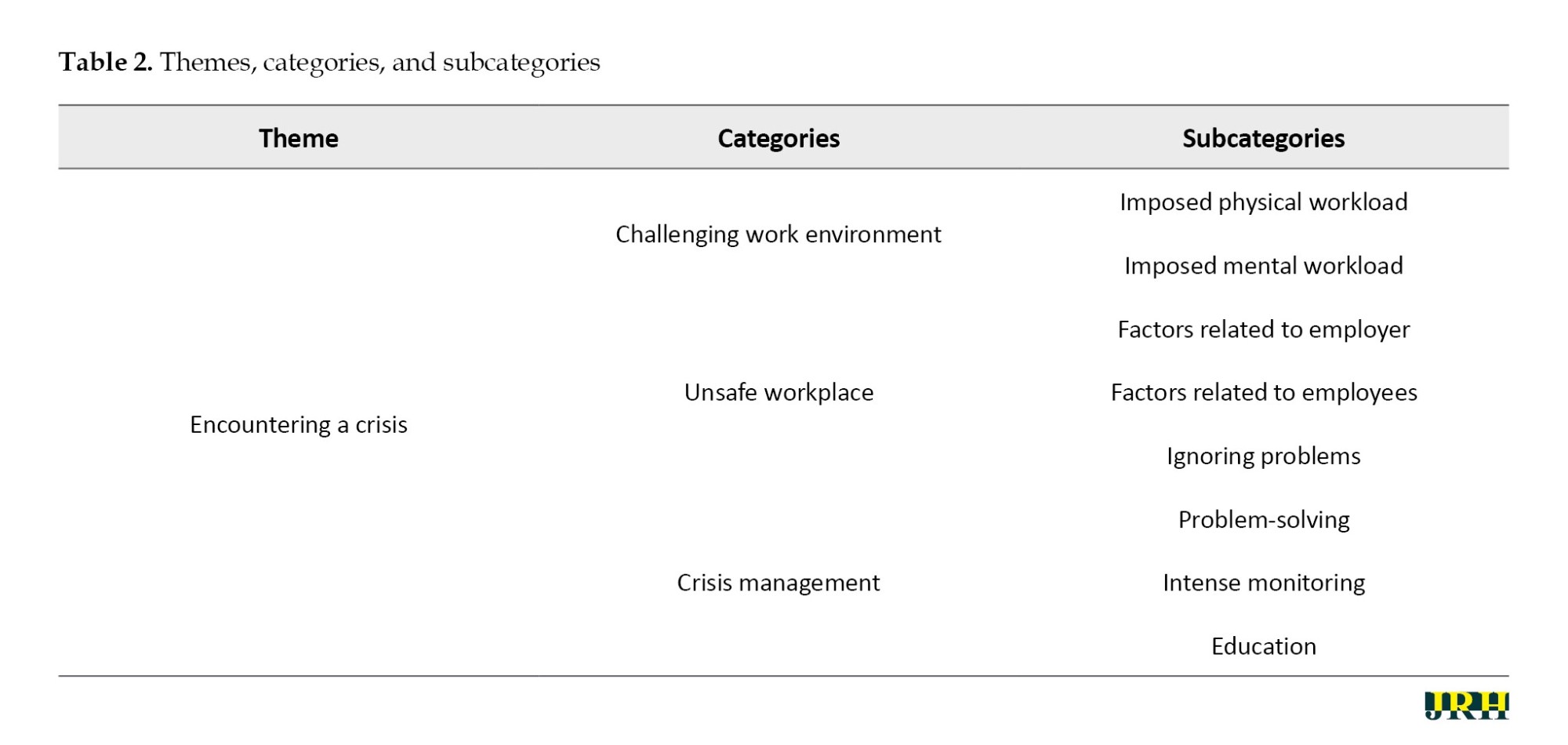
Participants believed that the COVID-19 epidemic represented a crisis in their working lives. Three themes—“challenging work environment,” “unsafe workplace,” and “crisis management”—emerged from the qualitative data analysis, all of which referred to the difficult situations that the workers had to confront. The themes and categories are listed in Table 2.
Challenging work environment
Two categories “imposed physical workload» and «imposed mental workload” formed this category and highlighted the intense physical and mental burdens that employees faced.
Imposed physical workload
According to participants’ narratives, the reduction in the number of workers, along with increased working hours, imposed a physical burden on them.
One of the workers said: “Reducing the number of workers in order to reduce the [population] density, despite the fact that the workload remains constant, has led to imposing the work-load of two people on one person, and this makes the work shifts exhausting for us. Applying limitations in the numbers of staff and the sick leaves [taken by ill workers], especially in the COVID-19 incidence peaks, increased the workload on [other] workers …”.
Another worker said: “If one person takes [sick] leave, there is no replacement and his work is divided among the others ...”
Imposed mental workload
On the other hand, from the participants’ perspective, news about the COVID-19 epidemic, fear of getting sick, and its consequences caused mental stress for workers. These daily stresses, combined with the necessity of working to meet financial needs and the fear of losing their jobs due to the potential reduction in the workforce during the pandemic, created a mental burden for participants. Some even reported abnormal behaviors as a result of their fear of developing COVID-19.
An engineer explained: “Some had developed obsessive behaviors, for example, our colleague, would disinfect his own wireless phone which only he himself used, several times a day and washed his hands constantly. Then, he developed dermatitis and had to be treated.”
One of the workers said: “We were very scared when we heard about the beginning of the disease in the city. I was afraid of any contact with colleagues ... we were wearing masks, we were taking disinfectants with us, we stayed away from each other, … we were very stressed”.
Unsafe workplace
This category included “causes related to the employer”, “causes related to employees”, and “ignoring problems”.
Factors related to the employer
The continuation of the COVID epidemic and the inability to control the disease was another dimension of this crisis. Participants reported the presence of multiple contractors in industrial companies with different management methods, inadequate knowledge related to COVID-19 control, a lack of adherence to similar protocols, and an unfair distribution of facilities and protection equipment. One of the workers stated:
“Because of the large number of contractors and the fact that some of them are temporary contractors … with little information about disease control, and do not care about anything other than the progress of their work, …they do not care about disease control either”.
An engineer said: “The distribution of disinfectants and masks is not fair. In general, those who work in the central building of Golgohar have better conditions”.
Another factor contributing to the continuation of the epidemic, from the participants’ perspective, was employers’ non-adherence to health and safety protocols.
A healthcare provider said: “Non-native staff live in the boarding houses. Gatherings in the boarding houses and the non-observance of the protocols by the workers are the cause of the spread of the disease”.
One of the engineers stated: “One of the reasons that the disease spread is trust. We always trust our co-workers. Many times, when we are alone in the room with our colleague, we take off our masks, and the presumption is that our colleague is healthy, while many patients, … got sick from their co-worker”.
Ignoring problems
Over time, some participants began to perceive the conditions as normal and did not take safety instructions seriously, failing to follow safety protocols. Over time, some participants began to perceive the conditions as normal and did not take safety instructions seriously, failing to follow safety protocols.
One of the managers explained: “In my opinion, it does not matter whether you adhere to protocols or not! We have a co-worker who was very prudent, he even opened the door with his feet, but now he is sick and his lungs are involved, while I behave as normal and I am not afraid”.
Another participant also stated: “When we are at work, we get so busy that we forget Corona. I got positive twice, but I got better. You shouldn’t worry too much”.
Crisis management
Crisis management, as another category, refers to some actions taken during the COVID-19 crisis and includes three subcategories: “Complying with health guidelines”, “intense monitoring”, and “education”.
Managers attempted to implement initiatives based on the available facilities and working conditions. Some of the strategies implemented included social distancing, reducing the number of workers in each workshop, decreasing commuting, providing protective equipment, and reducing the number of work shifts in exchange for increasing working hours.
One of the managers explained, “Our workers were tested for COVID-19 without cost by the local university labs, based on a memorandum of understanding”. A technician added, “Our shifts have been changed, not by reducing working hours, but by extending them to twelve hours, in order to minimize the number of commuting times. They have provided us with masks and disinfection equipment. The number of buses has also increased, and efforts are being made to ensure that people sit at a distance inside the buses”.
In addition, managers monitored the activities of their employees to ensure compliance with safety protocols. They believed that intense monitoring forces everybody to respect rules and protocols. In this regard, another manager said:
“If someone does not comply with rules and does not have a mask, the safety unit calls on him and controls the situation. In addition, screening such as measuring fever and blood oxygen is done regularly for some staff, such as those who work in the restaurant and if they have COVID-19 symptoms, they should go on leave for two weeks”.
Participants pointed to education as an effective factor in controlling the epidemic in their workplace. They stated that holding training workshops for employees, contractors, and managers gradually changed their behavior. Participants identified education as an effective factor in controlling the epidemic in their workplace. They stated that holding training workshops for employees, contractors, and managers gradually changed their behavior.
Another manager stated: “On the first days after the outbreak of disease, there were many incorrect information and rumors going around, …. the information was from unreliable sources, but little by little the training helped us to solve this problem.”
The continuity of training during the outbreak, as well as the preparation of guidelines for maintaining a safe workplace for workers, was mentioned by participants as one of the effective factors in controlling the epidemic. Teaching and education helped identify health and safety hazards in the workplace and control the spread of disease.
In this regard, a worker said: “Education is effective when repeated again and again and causes durable changes in behavior, one of the things that poor education led to, was hiding the symptoms, as some had a series of symptoms that they hid this from their colleagues, [but this wrong behavior] improved over time.”
Discussion
According to the findings of this study, with the onset of the COVID-19 epidemic and the subsequent limitations and problems, employees in business, administrative, and industrial centers faced various challenges. The onset of the epidemic disrupted the normal work process, imposed restrictions, such as reducing manpower in working shifts, and inflicted a significant physical and mental burden on employees. Labor shortages have always been a concern in industries [17], but this concern was exacerbated by the COVID-19 epidemic, as a percentage of employees became infected with the virus and were unable to work. In addition, the development of COVID-19 led to anxiety about getting sick and transmitting the infection to their co-workers, family members, or clients [18].
Concerns related to the COVID-19 epidemic and its consequences, insufficient knowledge about the disease, worries about the future of their jobs, and changes in the daily work process were some of the factors that caused stress among workers, as mentioned by the participants in this study. Furthermore, the complexity of the situation was heightened by the company’s size and the large number of employees. The continuation of stressors can harm both the mental and physical health of employees [19] and can lead to burnout among employees in various professions [20]. Physical problems and insomnia have also been reported as a result of work stress and mental workload resulting from the COVID-19 epidemic [21]. Pamidimukkala and Kermanshachi stated workers’ job stress and burnout following the outbreak of COVID-19 have led to increased fatigue and decreased motivation [22]. Other studies have indicated that exposure to constant news and speculation at the beginning of the COVID-19 outbreak made workers feel fearful. Furthermore, mental health is affected not only during a crisis or epidemic but also long after the crisis has ended [22].
Poor prevention practices regarding COVID-19 have been identified as an effective factor in perpetuating the epidemic and subsequent occupational and economic problems. In the workplace, a comprehensive plan is needed to prevent the spread of COVID-19, which should be developed by top-level managers and health policymakers, with employees required to comply [23]. Personal protective strategies, such as the optimal use of face masks, proper ventilation of the workplace, and physical distancing, should be implemented by employers. If a worker shows signs of possible infection, they should be identified and kept away from others [24]. However, the study participants stated that there is insufficient adherence to safety protocols due to the large number of temporary work agencies with short-term contracts in large industrial companies, such as Golgohar, as well as a lack of knowledge about the disease. Another study showed that employers tend to follow instructions that are mandated or inspected by a government agency [25], highlighting the need for more training and oversight of employers’ compliance with protocols by government agencies such as the Ministries of Health.
Participants in this study described injustice in the distribution of resources and protective equipment as one of the causes of inadequate disease control in industrial workplaces. McClure et al. stated that workers from ethnic, racial, and immigrant minorities do not have adequate personal protective equipment and are more likely to develop COVID-19 [26]. The unavailability of personal protective equipment has been cited as an important factor affecting the epidemic spread in different work groups [27]. In another study in Iran, the lack of access to protective equipment for industrial workers was identified as one of the reasons for employees’ non-adherence to protocols [28]. the lack of access to COVID-19 diagnostic tests and unfair vaccination practices are also mentioned as significant factors in the failure to control the epidemic [26]. Governments must take action to prevent the unfair distribution of services.
On the other hand, trivializing the situation and the improper adherence of employees to health protocols is another factor that can affect the prevalence of COVID-19 among employees and subsequently in the community [29]. According to the results of the present study, some employees did not have a proper attitude toward observing the protocols, and some had begun to trivialize them over time. Complaints from some employees about shortness of breath and sensitivity when using masks, or discomfort when working with gloves, have been cited in other studies as justifications for not following the protocols [28]. Other studies have identified male gender and young age as effective factors in not adhering to preventive protocols [30]. The attitudes and beliefs of individuals were also mentioned as significant factors influencing compliance with the rules in other studies [30]. For example, in this study, some misconceptions were observed, such as the belief that following or not following protocols does not matter because they will get infected anyway, or that if one of two workers working closely together wears a mask, the other does not need to wear one. Unfortunately, this issue is common not only among workers but also among some employers and supervisors. Ignorance of protocols by employers and supervisors can encourage employees to neglect the use of personal protective equipment [31].
Another sub-category extracted from the interview analysis was “crisis management”, which refers to remedial measures to control the epidemic. Crises are unexpected events that can harm organizations and need correct, scientific, and effective management [32]. In a crisis, problems should be identified, and appropriate solutions should subsequently be provided to overcome these issues [33]. In a situation, like the COVID-19 epidemic, where there is limited knowledge, making the best evidence-based decisions is necessary to achieve the best results with the least damage [33]. Managers are committed to providing a safe workplace for employees, and employees must always adhere to safety strategies while also considering the survival of the business. This can be accomplished by identifying problems, resources, and constraints, as well as by implementing more effective safety protocols [34] and screening suspected cases.
According to our data, strict monitoring of the implementation of health protocols by the safety unit in the workplace was another plan conducted at Golgohar Complex. Results from another study showed that not only should the monitoring of protocol implementation be conducted, but the processes of diagnosis and treatment of individuals should also be monitored [35]. In general, by identifying vulnerable sectors in the industry and considering the possibility of disease transmission from the workplace to the community, emphasis should be placed on implementing public health interventions in the workplace [36].
This study also suggested that providing adequate training to contractors and personnel, along with the repetition of training sessions until the desired behavior change occurs among employees, contractors, and managers, is necessary. Lack of knowledge about COVID-19, and its high contagion rates have been reported as effective factors in the transmission and spread of the disease [37]. Therefore, education about the disease should be conducted continuously and following updated information. Installing banners and educational posters for employees can also provide opportunities for ongoing training in any location and situation. Teaching health principles has been identified in many studies as an effective method for promoting the knowledge and attitudes of individuals, thereby enhancing the safety culture during the COVID-19 era [38]. Training has also been shown to be effective in increasing awareness, attitude, and the use of protective devices among workers [39].
Conclusion
The COVID-19 pandemic was regarded as a crisis in occupational settings. Workers experienced various physical and mental difficulties in their work, along with inadequate disease control. Many workers did not realize the seriousness of the pandemic and lacked sufficient information about the disease, which contributed to the spread of infection. Teaching problem-solving strategies and behavior control, combined with training on disease prevention, can be effective in crisis management.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Standing Ethics Committee of Sirjan School of Medical Sciences (Code: IR.SIRUMS.REC.1399.036). The aim of the study was explained to the participants, and informed consent was obtained.
Funding
This study was financially supported by the Research and Technology Department of Sirjan School of Medical Sciences (Grant No.: 99000078).
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers would like to thank the Research Deputy of Sirjan School of Medical Sciences for financially supporting this research, as well as all the individuals who participated in the study.
References
The coronavirus disease 2019 (COVID-19) rapidly spread around the world and was declared a global emergency by the World Health Organization (WHO) and the International Health Regulations (IHR) Emergency Committee [1]. The COVID-19 pandemic created enormous health, economic, environmental, and social challenges for the entire human population [2, 3]. Some COVID-19 patients exhibit mild or severe symptoms, and some may die because of multiple organ dysfunction; however, a large portion of them are asymptomatic carriers, which can lead to the infection of many others [4].
The COVID‐19 epidemic had a negative impact on occupational health, business sustainability, and individual employment [5, 6]. Employees had to take care of themselves, and their families while maintaining their job positions [7]. Some studies have reported that during the pandemic the need for childcare increased because children had to stay at home, and required attention. Additional responsibilities, including working longer hours and new fears about virus exposure, led to an increase in both work and family demands. Consequently, employees experience work-family conflicts, which can negatively impact their physical and mental well-being [7, 8]. Furthermore, little guidance is available on how resilience levers (i.e. supervision, support, policies, and organizational preparedness for the crisis) may promote worker’s well-being during the COVID-19 pandemic [6].
The COVID-19 pandemic has had an extreme effect on the economy and has caused a drastic reduction in the size and scope of economic activity as well [9]. Some employees were required to take immediate action to change their work styles under the instructions of their companies or organizations. Sasaki et al. suggested that workplace rules and policies may help promote and maintain the mental health and work performance of employees during the COVID-19 epidemic [10]. However, Wong et al. showed that many employees were not satisfied with workplace policies because of their incompleteness, untimeliness, and ambiguity [9]. Previous studies have also stated that workplace policies should be supported by both governmental and organizational settings [9].
Industries are a vital part of a country’s economy and cannot be closed under all circumstances [11]. Despite the challenges posed by the COVID-19 pandemic, many workers were expected to be present at their workplaces. Surprisingly, very few studies have investigated the experiences of industrial workers during this unprecedented time. Sirjan is one of the cities in Iran with large mining industries, such as the Golgohar Industrial Mining Complex, which is known as the largest iron company in the Middle East. This mine, with a reserve of about 1200 million tons, is located in an area approximately 10 km long and approximately 4 km wide. The number of workers and employees exceeds 16,000, who work in two shifts. The incidence of COVID-19 was high among the employees of this complex.
It is important to explore the experiences of industrial employees during the pandemic to identify the weaknesses and strengths of disease control from their perspective. These narratives may help recognize the problems and find solutions to manage unexpected conditions and preserve the well-being of workers. This study aimed to explore the experiences of the employees of Golgohar Mining and Industrial Co. during the COVID-19 pandemic.
Methods
This qualitative content analysis study was conducted in Sirjan, Iran from March 2021 to October 2021.
Population and sampling procedure
Participants were 20 employees of the Golgohar Industrial Mining Company in Sirjan, selected by purposeful sampling. Sampling continued until data saturation was reached, at which point no new information was obtained from the interviews.
The aim of the study was explained to participants, who then signed an informed consent form. Based on the participants’ preferences, a comfortable and private environment was chosen for the interviews, which included the participants’ homes, workplaces, or the campus of Sirjan School of Medical Sciences.
Inclusion criteria included the willingness to participate in the study, being employed by Golgohar Industrial Mining Co., and living in Sirjan. Participants’ demographic characteristics are presented in Table 1.
Data collection method
Data were collected through semi-structured interviews. After greetings, the researcher asked general questions, such as the participants’ age, occupation, and work experience. Then, specific questions related to the main purpose of the research were asked. For example, “How did the COVID-19 epidemic affect your work? What factors contributed to the spread of COVID-19 in your workplace? What interventions were implemented in your workplace for the prevention of COVID-19?” Participants were asked to provide detailed information and explain their responses thoroughly.
Interviews lasted 35 to 50 minutes. In this study, data saturation was achieved from the researchers’ perspective after the 10th interview. However, to ensure greater certainty, a total of 20 interviews were conducted.
Content analysis
Content analysis is a qualitative data analysis method [12]. It includes a systematic process of coding, identification of subcategories and categories, and finally, description of the social reality through the creation of themes [13, 14].
Data analysis
Data analysis was performed concurrently with data collection, according to the method proposed by Graneheim and Lundman, which suggests five steps for qualitative data analysis [15]. According to this method, the interviews were transcribed. The full text of each interview was then read several times to gain a general understanding of its content, followed by an analysis of the interviews (Figure 1).
Rigor
The four criteria of credibility, dependability, confirmability, and transferability were used to ensure the trustworthiness of the data [16]. Credibility was enhanced through interaction with participants, allocating sufficient time for data gathering using open questions, audio recordings of the interviews, and transcribing the interviews word for word, along with analyzing the data using the constant comparative method. Participant reviews and member checks were also used to verify the data and codes. For this purpose, the text of two interpretations was returned to the participants to ensure that the researcher had understood the context, and some corrections were made based on the participants’ comments. The transcripts of the interviews, as well as the extracted codes and categories, were also reviewed by two faculty members, and agreement was achieved. Participants were selected from different ages, genders, various administrative positions, and different recruitment sites. Confirmability and transferability were enhanced by documenting the research process and all related activities, as well as clearly describing the study process and inviting different occupational groups to participate in the study. The findings were recorded in as much detail as possible.
Results
The participants were workers, engineers, healthcare providers, and managers of the Golgohar Copper Complex. They were all male, and their ages ranged from 24 to 49 years. They had between 1 and 24 years of experience.
Participants believed that the COVID-19 epidemic represented a crisis in their working lives. Three themes—“challenging work environment,” “unsafe workplace,” and “crisis management”—emerged from the qualitative data analysis, all of which referred to the difficult situations that the workers had to confront. The themes and categories are listed in Table 2.
Challenging work environment
Two categories “imposed physical workload» and «imposed mental workload” formed this category and highlighted the intense physical and mental burdens that employees faced.
Imposed physical workload
According to participants’ narratives, the reduction in the number of workers, along with increased working hours, imposed a physical burden on them.
One of the workers said: “Reducing the number of workers in order to reduce the [population] density, despite the fact that the workload remains constant, has led to imposing the work-load of two people on one person, and this makes the work shifts exhausting for us. Applying limitations in the numbers of staff and the sick leaves [taken by ill workers], especially in the COVID-19 incidence peaks, increased the workload on [other] workers …”.
Another worker said: “If one person takes [sick] leave, there is no replacement and his work is divided among the others ...”
Imposed mental workload
On the other hand, from the participants’ perspective, news about the COVID-19 epidemic, fear of getting sick, and its consequences caused mental stress for workers. These daily stresses, combined with the necessity of working to meet financial needs and the fear of losing their jobs due to the potential reduction in the workforce during the pandemic, created a mental burden for participants. Some even reported abnormal behaviors as a result of their fear of developing COVID-19.
An engineer explained: “Some had developed obsessive behaviors, for example, our colleague, would disinfect his own wireless phone which only he himself used, several times a day and washed his hands constantly. Then, he developed dermatitis and had to be treated.”
One of the workers said: “We were very scared when we heard about the beginning of the disease in the city. I was afraid of any contact with colleagues ... we were wearing masks, we were taking disinfectants with us, we stayed away from each other, … we were very stressed”.
Unsafe workplace
This category included “causes related to the employer”, “causes related to employees”, and “ignoring problems”.
Factors related to the employer
The continuation of the COVID epidemic and the inability to control the disease was another dimension of this crisis. Participants reported the presence of multiple contractors in industrial companies with different management methods, inadequate knowledge related to COVID-19 control, a lack of adherence to similar protocols, and an unfair distribution of facilities and protection equipment. One of the workers stated:
“Because of the large number of contractors and the fact that some of them are temporary contractors … with little information about disease control, and do not care about anything other than the progress of their work, …they do not care about disease control either”.
An engineer said: “The distribution of disinfectants and masks is not fair. In general, those who work in the central building of Golgohar have better conditions”.
Another factor contributing to the continuation of the epidemic, from the participants’ perspective, was employers’ non-adherence to health and safety protocols.
A healthcare provider said: “Non-native staff live in the boarding houses. Gatherings in the boarding houses and the non-observance of the protocols by the workers are the cause of the spread of the disease”.
One of the engineers stated: “One of the reasons that the disease spread is trust. We always trust our co-workers. Many times, when we are alone in the room with our colleague, we take off our masks, and the presumption is that our colleague is healthy, while many patients, … got sick from their co-worker”.
Ignoring problems
Over time, some participants began to perceive the conditions as normal and did not take safety instructions seriously, failing to follow safety protocols. Over time, some participants began to perceive the conditions as normal and did not take safety instructions seriously, failing to follow safety protocols.
One of the managers explained: “In my opinion, it does not matter whether you adhere to protocols or not! We have a co-worker who was very prudent, he even opened the door with his feet, but now he is sick and his lungs are involved, while I behave as normal and I am not afraid”.
Another participant also stated: “When we are at work, we get so busy that we forget Corona. I got positive twice, but I got better. You shouldn’t worry too much”.
Crisis management
Crisis management, as another category, refers to some actions taken during the COVID-19 crisis and includes three subcategories: “Complying with health guidelines”, “intense monitoring”, and “education”.
Managers attempted to implement initiatives based on the available facilities and working conditions. Some of the strategies implemented included social distancing, reducing the number of workers in each workshop, decreasing commuting, providing protective equipment, and reducing the number of work shifts in exchange for increasing working hours.
One of the managers explained, “Our workers were tested for COVID-19 without cost by the local university labs, based on a memorandum of understanding”. A technician added, “Our shifts have been changed, not by reducing working hours, but by extending them to twelve hours, in order to minimize the number of commuting times. They have provided us with masks and disinfection equipment. The number of buses has also increased, and efforts are being made to ensure that people sit at a distance inside the buses”.
In addition, managers monitored the activities of their employees to ensure compliance with safety protocols. They believed that intense monitoring forces everybody to respect rules and protocols. In this regard, another manager said:
“If someone does not comply with rules and does not have a mask, the safety unit calls on him and controls the situation. In addition, screening such as measuring fever and blood oxygen is done regularly for some staff, such as those who work in the restaurant and if they have COVID-19 symptoms, they should go on leave for two weeks”.
Participants pointed to education as an effective factor in controlling the epidemic in their workplace. They stated that holding training workshops for employees, contractors, and managers gradually changed their behavior. Participants identified education as an effective factor in controlling the epidemic in their workplace. They stated that holding training workshops for employees, contractors, and managers gradually changed their behavior.
Another manager stated: “On the first days after the outbreak of disease, there were many incorrect information and rumors going around, …. the information was from unreliable sources, but little by little the training helped us to solve this problem.”
The continuity of training during the outbreak, as well as the preparation of guidelines for maintaining a safe workplace for workers, was mentioned by participants as one of the effective factors in controlling the epidemic. Teaching and education helped identify health and safety hazards in the workplace and control the spread of disease.
In this regard, a worker said: “Education is effective when repeated again and again and causes durable changes in behavior, one of the things that poor education led to, was hiding the symptoms, as some had a series of symptoms that they hid this from their colleagues, [but this wrong behavior] improved over time.”
Discussion
According to the findings of this study, with the onset of the COVID-19 epidemic and the subsequent limitations and problems, employees in business, administrative, and industrial centers faced various challenges. The onset of the epidemic disrupted the normal work process, imposed restrictions, such as reducing manpower in working shifts, and inflicted a significant physical and mental burden on employees. Labor shortages have always been a concern in industries [17], but this concern was exacerbated by the COVID-19 epidemic, as a percentage of employees became infected with the virus and were unable to work. In addition, the development of COVID-19 led to anxiety about getting sick and transmitting the infection to their co-workers, family members, or clients [18].
Concerns related to the COVID-19 epidemic and its consequences, insufficient knowledge about the disease, worries about the future of their jobs, and changes in the daily work process were some of the factors that caused stress among workers, as mentioned by the participants in this study. Furthermore, the complexity of the situation was heightened by the company’s size and the large number of employees. The continuation of stressors can harm both the mental and physical health of employees [19] and can lead to burnout among employees in various professions [20]. Physical problems and insomnia have also been reported as a result of work stress and mental workload resulting from the COVID-19 epidemic [21]. Pamidimukkala and Kermanshachi stated workers’ job stress and burnout following the outbreak of COVID-19 have led to increased fatigue and decreased motivation [22]. Other studies have indicated that exposure to constant news and speculation at the beginning of the COVID-19 outbreak made workers feel fearful. Furthermore, mental health is affected not only during a crisis or epidemic but also long after the crisis has ended [22].
Poor prevention practices regarding COVID-19 have been identified as an effective factor in perpetuating the epidemic and subsequent occupational and economic problems. In the workplace, a comprehensive plan is needed to prevent the spread of COVID-19, which should be developed by top-level managers and health policymakers, with employees required to comply [23]. Personal protective strategies, such as the optimal use of face masks, proper ventilation of the workplace, and physical distancing, should be implemented by employers. If a worker shows signs of possible infection, they should be identified and kept away from others [24]. However, the study participants stated that there is insufficient adherence to safety protocols due to the large number of temporary work agencies with short-term contracts in large industrial companies, such as Golgohar, as well as a lack of knowledge about the disease. Another study showed that employers tend to follow instructions that are mandated or inspected by a government agency [25], highlighting the need for more training and oversight of employers’ compliance with protocols by government agencies such as the Ministries of Health.
Participants in this study described injustice in the distribution of resources and protective equipment as one of the causes of inadequate disease control in industrial workplaces. McClure et al. stated that workers from ethnic, racial, and immigrant minorities do not have adequate personal protective equipment and are more likely to develop COVID-19 [26]. The unavailability of personal protective equipment has been cited as an important factor affecting the epidemic spread in different work groups [27]. In another study in Iran, the lack of access to protective equipment for industrial workers was identified as one of the reasons for employees’ non-adherence to protocols [28]. the lack of access to COVID-19 diagnostic tests and unfair vaccination practices are also mentioned as significant factors in the failure to control the epidemic [26]. Governments must take action to prevent the unfair distribution of services.
On the other hand, trivializing the situation and the improper adherence of employees to health protocols is another factor that can affect the prevalence of COVID-19 among employees and subsequently in the community [29]. According to the results of the present study, some employees did not have a proper attitude toward observing the protocols, and some had begun to trivialize them over time. Complaints from some employees about shortness of breath and sensitivity when using masks, or discomfort when working with gloves, have been cited in other studies as justifications for not following the protocols [28]. Other studies have identified male gender and young age as effective factors in not adhering to preventive protocols [30]. The attitudes and beliefs of individuals were also mentioned as significant factors influencing compliance with the rules in other studies [30]. For example, in this study, some misconceptions were observed, such as the belief that following or not following protocols does not matter because they will get infected anyway, or that if one of two workers working closely together wears a mask, the other does not need to wear one. Unfortunately, this issue is common not only among workers but also among some employers and supervisors. Ignorance of protocols by employers and supervisors can encourage employees to neglect the use of personal protective equipment [31].
Another sub-category extracted from the interview analysis was “crisis management”, which refers to remedial measures to control the epidemic. Crises are unexpected events that can harm organizations and need correct, scientific, and effective management [32]. In a crisis, problems should be identified, and appropriate solutions should subsequently be provided to overcome these issues [33]. In a situation, like the COVID-19 epidemic, where there is limited knowledge, making the best evidence-based decisions is necessary to achieve the best results with the least damage [33]. Managers are committed to providing a safe workplace for employees, and employees must always adhere to safety strategies while also considering the survival of the business. This can be accomplished by identifying problems, resources, and constraints, as well as by implementing more effective safety protocols [34] and screening suspected cases.
According to our data, strict monitoring of the implementation of health protocols by the safety unit in the workplace was another plan conducted at Golgohar Complex. Results from another study showed that not only should the monitoring of protocol implementation be conducted, but the processes of diagnosis and treatment of individuals should also be monitored [35]. In general, by identifying vulnerable sectors in the industry and considering the possibility of disease transmission from the workplace to the community, emphasis should be placed on implementing public health interventions in the workplace [36].
This study also suggested that providing adequate training to contractors and personnel, along with the repetition of training sessions until the desired behavior change occurs among employees, contractors, and managers, is necessary. Lack of knowledge about COVID-19, and its high contagion rates have been reported as effective factors in the transmission and spread of the disease [37]. Therefore, education about the disease should be conducted continuously and following updated information. Installing banners and educational posters for employees can also provide opportunities for ongoing training in any location and situation. Teaching health principles has been identified in many studies as an effective method for promoting the knowledge and attitudes of individuals, thereby enhancing the safety culture during the COVID-19 era [38]. Training has also been shown to be effective in increasing awareness, attitude, and the use of protective devices among workers [39].
Conclusion
The COVID-19 pandemic was regarded as a crisis in occupational settings. Workers experienced various physical and mental difficulties in their work, along with inadequate disease control. Many workers did not realize the seriousness of the pandemic and lacked sufficient information about the disease, which contributed to the spread of infection. Teaching problem-solving strategies and behavior control, combined with training on disease prevention, can be effective in crisis management.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Standing Ethics Committee of Sirjan School of Medical Sciences (Code: IR.SIRUMS.REC.1399.036). The aim of the study was explained to the participants, and informed consent was obtained.
Funding
This study was financially supported by the Research and Technology Department of Sirjan School of Medical Sciences (Grant No.: 99000078).
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers would like to thank the Research Deputy of Sirjan School of Medical Sciences for financially supporting this research, as well as all the individuals who participated in the study.
References
- Zumla A, Niederman MS. Editorial: The explosive epidemic outbreak of novel coronavirus disease 2019 (COVID-19) and the persistent threat of respiratory tract infectious diseases to global health security. Current Opinion in Pulmonary Medicine. 2020; 26(3):193-6. [DOI:10.1097/MCP.0000000000000676] [PMID] [PMCID]
- Chakraborty I, Maity P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. The Science of the Total Environment. 2020; 728:138882. [DOI:10.1016/j.scitotenv.2020.138882] [PMID] [PMCID]
- Sadeghi R, Masoudi M, Khanjani N, Bamir M. Neglect of other health services during the corona crisis. Environmental Health Engineering and Management Journal. 2021; 8(1):65-6. [DOI:10.34172/EHEM.2021.09]
- Ciotti M, Ciccozzi M, Terrinoni A, Jiang WC, Wang CB, Bernardini S. The COVID-19 pandemic. Critical Reviews in Clinical Laboratory Sciences. 2020; 57(6):365-88. [DOI:10.1080/10408363.2020.1783198] [PMID]
- Tamin J, Samuel O, Suraya A, Ebuenyi ID, Naicker N, Rajput-Ray M. Vulnerable workers and COVID-19: Insights from a survey of members of the international commission for occupational health. International Journal of Environmental Research and Public Health. 2021; 18(1):346. [DOI:10.3390/ijerph18010346] [PMID] [PMCID]
- Ekpanyaskul C, Padungtod C. Occupational health problems and lifestyle changes among novice working-from-home workers amid the COVID-19 pandemic. Safety and Health at Work. 2021; 12(3):384-9. [DOI:10.1016/j.shaw.2021.01.010] [PMID] [PMCID]
- Buselli R, Baldanzi S, Corsi M, Chiumiento M, Del Lupo E, Carmassi C, et al. Psychological care of health workers during the COVID-19 outbreak in Italy: Preliminary report of an occupational health department (AOUP) responsible for monitoring hospital staff condition. Sustainability. 2020; 12(12):5039. [DOI:10.3390/su12125039]
- Pacheco T, Coulombe S, Khalil C, Meunier S, Doucerain M, Auger E, et al. Job security and the promotion of workers’ wellbeing in the midst of the COVID-19 pandemic: A study with Canadian workers one to two weeks after the initiation of social distancing measures. International Journal of Wellbeing. 2020; 10(3):58-76. [DOI:10.5502/ijw.v10i3.1321]
- Wong EL, Ho KF, Wong SY, Cheung AW, Yau PS, Dong D, et al. Views on workplace policies and its impact on health-related quality of life during coronavirus disease (COVID-19) pandemic: Cross-sectional survey of employees. International Journal of Health Policy and Management. 2022; 11(3):344-53. [DOI:org/10.34172/ijhpm.2020.127] [PMID] [PMCID]
- Sasaki N, Kuroda R, Tsuno K, Kawakami N. Workplace responses to COVID-19 associated with mental health and work performance of employees in Japan. Journal of Occupational Health. 2020; 62(1):e12134. [DOI:10.1002/1348-9585.12134] [PMID] [PMCID]
- Goodell JW, Huynh TLD. Did congress trade ahead? Considering the reaction of US industries to COVID-19. Finance Research Letters. 2020; 36:101578. [DOI:10.1016/j.frl.2020.101578] [PMID] [PMCID]
- Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative content analysis: A focus on trustworthiness. SAGE open. 2014; 4(1):2158244014522633. [DOI:10.1177/2158244014522633]
- Vaismoradi M, Jones J, Turunen H, Snelgrove S. Theme development in qualitative content analysis and thematic analysis. Journal of Nursing Education and Practice. 2016; 6(5):100-10. [DOI:10.5430/jnep.v6n5p100]
- Assarroudi A, Heshmati Nabavi F, Armat MR, Ebadi A, Vaismoradi M. Directed qualitative content analysis: The description and elaboration of its underpinning methods and data analysis process. Journal of Research in Nursing. 2018; 23(1):42-55. [DOI:10.1177/1744987117741667] [PMID] [PMCID]
- Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: A discussion paper. Nurse Education Today. 2017; 56:29-34. [DOI:10.1016/j.nedt.2017.06.002] [PMID]
- Ravenek MJ, Rudman DL. Bridging conceptions of quality in moments of qualitative research. International Journal of Qualitative Methods. 2013; 12(1):436-56. [DOI:10.1177/160940691301200122]
- Karimi Z, Fereidouni Z, Behnammoghadam M, Alimohammadi N, Mousavizadeh A, Salehi T, et al. The lived experience of nurses caring for patients with COVID-19 in Iran: A phenomenological study. Risk Management and Healthcare Policy. 2020; 13:1271-8. [DOI:10.2147/RMHP.S258785] [PMID] [PMCID]
- Shanafelt T, Ripp J, Trockel M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA. 2020; 323(21):2133-4. [DOI:10.1001/jama.2020.5893] [PMID]
- O'Connor RC, Wetherall K, Cleare S, McClelland H, Melson AJ, Niedzwiedz CL, et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 mental health & wellbeing study. The British Journal of Psychiatry. 2021; 218(6):326-33. [DOI:10.1192/bjp.2020.212] [PMID] [PMCID]
- Rodríguez-López AM, Rubio-Valdehita S, Díaz-Ramiro EM. Influence of the CoViD-19 pandemic on mental workload and burnout of fashion retailing workers in Spain. International Journal of Environmental Research and Public Health. 2021; 18(3):983. [DOI:10.3390/ijerph18030983] [PMID] [PMCID]
- Blanco-Donoso LM, Garrosa E, Moreno-Jiménez J, Gálvez-Herrer M, Moreno-Jiménez B. Occupational psychosocial risks of health professionals in the face of the crisis produced by the COVID-19: From the identification of these risks to immediate action. International Journal of Nursing Studies Advances. 2020; 2:100003. [DOI:10.1016/j.ijnsa.2020.100003] [PMID] [PMCID]
- Pamidimukkala A, Kermanshachi S. Impact of covid-19 on field and office workforce in construction industry. Project Leadership and Society. 2021; 2:100018. [DOI:10.1016/j.plas.2021.100018]
- Michaels D, Wagner GR. Occupational safety and health administration (OSHA) and worker safety during the COVID-19 pandemic. JAMA. 2020; 324(14):1389-90. [DOI:10.1001/jama.2020.16343] [PMID]
- Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet. 202; 395(10242):1973-87. [DOI:10.1016/S0140-6736(20)31142-9] [PMID]
- Fragkou PC, Belhadi D, Peiffer-Smadja N, Moschopoulos CD, Lescure FX, Janocha H, et al. Review of trials currently testing treatment and prevention of COVID-19. Clinical Microbiology and Infection. 2020; 26(8):988-98. [DOI:10.1016/j.cmi.2020.05.019] [PMID] [PMCID]
- McClure ES, Vasudevan P, Bailey Z, Patel S, Robinson WR. Racial capitalism within public health-how occupational settings drive COVID-19 disparities. American Journal of Epidemiology. 2020; 189(11):1244-53. [DOI:10.1093/aje/kwaa126] [PMID] [PMCID]
- Kamerow D. Covid-19: The crisis of personal protective equipment in the US. BMJ. 2020; 369:m1367. [DOI:10.1136/bmj.m1367] [PMID]
- Moradi B, Barakat S. [Hygienic performance evaluation and effect of training in order to confronting with the Covid-19 virus in the metal industries staff (Persian)]. Iran Occupational Health. 2020; 17(1):66-80. [Link]
- Sahar Kostis YO, Rinsky-Halivni L, Cohen C, Zack O, Dekel R, Moshe S. Fitness for work during the COVID-19 disease: principles and suggested assistive tool for protecting workers during the pandemic era. International Archives of Occupational and Environmental Health. 2021; 94(6):1233-8. [DOI:10.1007/s00420-021-01722-x] [PMID] [PMCID]
- Czeisler MÉ, Tynan MA, Howard ME, Honeycutt S, Fulmer EB, Kidder DP, et al. Public attitudes, behaviors, and beliefs related to COVID-19, stay-at-home orders, nonessential business closures, and public health guidance-United States, New York City, and Los Angeles, May 5-12, 2020. Morbidity and Mortality Weekly Report. 2020; 69(24):751-8. [DOI:10.15585/mmwr.mm6924e1] [PMID] [PMCID]
- Adham D, Habibzadeh S, Ghobadi H, Jajin SA, Abbasi-Ghahramanloo A, Moradi-Asl E. Epidemiological characteristics and mortality risk factors among COVID-19 patients in Ardabil, Northwest of Iran. BMc Emergency Medicine. 2021; 21(1):67. [DOI:10.1186/s12873-021-00463-x] [PMID] [PMCID]
- Coccia M. Critical decisions in crisis management: Rational strategies of decision making. Journal of Economics Library. 2020; 7(2):81-96. [DOI:10.1453/jel.v7i2.2049]
- Von Krogh G, Kucukkeles B, Ben-Menahem SM. Lessons in rapid innovation from the COVID-19 pandemic. MIT Sloan Management Review. 2020; 61(4):8-10. [Link]
- Hu X, Yan H, Casey T, Wu CH. Creating a safe haven during the crisis: How organizations can achieve deep compliance with COVID-19 safety measures in the hospitality industry. International Journal of Hospitality Management. 2021; 92:102662. [DOI:10.1016/j.ijhm.2020.102662] [PMID] [PMCID]
- Kim S, Parboteeah KP, Cullen JB. The COVID-19 crisis management in the Republic of Korea. In: George B, Mahar Q, editors. International case studies in the management of disasters. LeedsL Emerald Publishing Limited; 2020. [DOI:10.1108/978-1-83982-186-820201014]
- Murti M, Achonu C, Smith BT, Brown KA, Kim JH, Johnson J, et al. COVID-19 workplace outbreaks by industry sector and their associated household transmission, ontario, Canada, January to June, 2020. Journal of Occupational and Environmental Medicine. 2021; 63(7):574-80. [DOI:10.1097/JOM.0000000000002201] [PMID] [PMCID]
- Plantes PJ, Fragala MS, Clarke C, Goldberg ZN, Radcliff J, Goldberg SE. Model for mitigation of workplace transmission of COVID-19 through population-based testing and surveillance. Population Health Management. 2021; 24(S1):S16-25. [DOI:10.1089/pop.2020.0322] [PMID] [PMCID]
- Belingheri M, Paladino ME, Riva MA. COVID-19: Health prevention and control in non-healthcare settings. Occupational Medicine. 2020; 70(2):82-83. [DOI:10.1093/occmed/kqaa048] [PMID] [PMCID]
- Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: A cross-sectional survey. Tropical Medicine and Health. 2020; 48:72. [DOI:10.1186/s41182-020-00254-3] [PMID] [PMCID]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2023/04/21 | Accepted: 2023/09/5 | Published: 2024/09/1
Received: 2023/04/21 | Accepted: 2023/09/5 | Published: 2024/09/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
