

Volume 14, Issue 3 (May & Jun 2024)
J Research Health 2024, 14(3): 249-258 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Charoghchian Khorasani E, Fakhar M, Kamel Khodabande A, Peyman N. The Effect of the Educational Intervention Based on the Theory of Protection Motivation in Preventing Cutaneous Leishmaniasis. J Research Health 2024; 14 (3) :249-258
URL: http://jrh.gmu.ac.ir/article-1-2352-en.html
URL: http://jrh.gmu.ac.ir/article-1-2352-en.html



1- Department of Health Education and Health Promotion, Social Determinants of Health Research Center, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Biostatistics, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Health Education and Health Promotion, Social Determinants of Health Research Center, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran. ,peymann@mums.ac.ir
2- Department of Biostatistics, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Health Education and Health Promotion, Social Determinants of Health Research Center, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran. ,
Full-Text [PDF 607 kb]
(56 Downloads)
| Abstract (HTML) (422 Views)
Full-Text: (26 Views)
Introduction
Leishmaniasis is a common disease between humans and animals. It is caused by different protozoan species of the Leishmania genus and is transmitted by female Phlebotomus mosquitoes and rodents, which are the leading reservoirs and sources, respectively. Leishmaniasis occurs in three forms: Cutaneous (oriental sore), visceral (kala-azar), and mucocutaneous [1, 2, 3]. Although the disease is mainly seen in tropical and subtropical regions, it is endemic in 88 countries worldwide, and 350 million people worldwide are at risk of infection. Fourteen million people are affected by the disease, and there are 1.5 million new cases of cutaneous leishmaniasis (CL) each year [4, 5]. Unlike other infectious diseases, the frequency of this disease is increasing. This increase is mainly due to migration, population movements, infection, global warming, and changes in human ecology. Although the death rate caused by CL is very low, due to the long duration of the wound, the creation of inappropriate scars, and the possibility of secondary infections, it has brought heavy treatment costs to society along with the increase in the length of the treatment period and the complications caused by the use of existing drugs [6, 7].
Due to the unavailability of a safe vaccine to prevent CL, it is necessary to avoid contracting the disease. CL can be prevented by reducing human contact with the vectors or by reducing the number of reservoirs. Nets, mosquito nets, or insect repellants should be used to control the vector. Using insect repellents is a preventive measure for people living in endemic areas[8]. CL is one of Iran’s most common endemic diseases [9]. Among Phlebotomus species in Iran, Phlebotomus papatasi and Phlebotomus sergenti are vectors, and the great gerbil, Meriones hurrianae, Meriones libycus, Meriones persicus, and Nesokia indica contribute as reservoirs in Iran [10, 11].
In Iran, the provinces of Isfahan, Fars, and Khorasan Razavi have the highest frequency of infection with CL in descending order. Khorasan-Razavi Province, is located in the northeast of Iran with a frequency of 1801 people in 2017. The city of Mashhad, the center of Khorasan-Razavi Province, is one of the main areas infected with CL [12]. As mentioned, infection prevention is the most critical measure, and educational interventions can be used to change preventive behaviors against CL [13]. Choosing a model or theory is the best measure in educational planning. This model or theory must be consistent with the purpose of the educational program [14, 15]. One of the theories that focus on the factors affecting the motivation and, finally, the protection behavior of the individual is the protection motivation theory [16].
Since this study was designed to change behavior for prevention, it seems helpful to use this theory. Rogers designed the theory of protection motivation in 1975 [17]. Rogers proposed that fear is influenced by five constructs of protective motivation (perceived sensitivity, perceived severity, perceived response efficacy, protective motivation, and perceived self-efficacy), which ultimately trigger healthy behaviors [18]. This theory investigates the factors affecting the individual’s motivation and behavior. It assumes that protective behavior against health risks is a direct behavior of the people’s motivation to protect themselves [19]. In general, the components of this theory are placed in two cognitive mediating processes: Threat assessment (examination of unhealthy behaviors and factors affecting the possibility of engaging in them) and coping assessment (the ability to deal with and avoid the threatened danger) [20]. The constructs of the theory are as follows: Perceived sensitivity, people’s belief that they are vulnerable to a health threat; perceived severity, people’s belief that the risk is serious; perceived response efficiency, people’s expectations that the adaptive response (protective behavior against health risk) can eliminate the risk; fear, an intermediate variable between sensitivity and severity perceived by threat assessment; and self-efficacy, people’s belief that they can effectively and successfully perform the suggested behavior [21, 22]. According to the constructs of the protection motivation theory and the target group, it seems that this theory can affect the preventive behaviors of CL in adolescent boys because students aged 10 to 15 years are the most vulnerable groups to CL in endemic areas [23]. Because this group is the most vulnerable and most accessible group that can improve the health behaviors of families by acquiring education, they were chosen as the target group. Since the prevention of CL is a simple and inexpensive task compared to its treatment [8], this research was conducted to determine the effect of education based on the theory of protection motivation on the preventative behaviors of the seventh, eighth, or ninth grade male students covered by the health center No. 1 in Mashhad City, Iran, in 2020.
Methods
Research design
This quasi-experimental study was conducted in Mashhad, 950 km from the capital (Tehran City). The city of Mashhad is divided into 5 centers in terms of health. This study was carried out in one of these 5 centers (Health Center No. 1). Through a random cluster sampling, 80 students were selected out of the 23152 students in the seventh, eighth, and ninth graders covered by the Health Center No. 1. In Mashhad, Iran in 2020.
Study participants
The inclusion criteria were as follows: Willingness to participate in the study, filling out a written consent form, being a resident of Mashhad, and being a male student of the seventh, eighth, or ninth grade. The exclusion criteria included unwillingness to continue cooperation during the intervention program and absence of more than one session from the training course.
Based on Maseudi et al. [12] study and considering 95% confidence interval, 80% test power, and 15% loss rate, the sample size was calculated to be 80 using the sampling formula to compare the average values between two study groups (experimental group=40, control group=40) (Equation 1).
The sampling method was a multi-stage random cluster sampling so that among the five Mashhad health centers, one center was randomly selected as a cluster, which was health center number one. Among the comprehensive health service centers of Health Center No. 1, one center was randomly selected as control and one center as experimental. The samples were selected within the comprehensive health services center, so the researcher contacted the people who met the conditions to enter the study. If they were content, they were included in the study.
Data collection
The intervention based on protection motivation theory was the independent variable, and the covariates studied were demographic characteristics, including age, number of family members, education level, father’s education, mother’s education, father’s occupation, and mother’s occupation.
This research used two questionnaires for data collection: The demographic section and CL protection motivation theory constructs. The demographic questionnaire gathered covariates information. The researcher created the CL protection motivation theory constructs questionnaire with 31 questions: Perceived sensitivity (4 questions), perceived intensity (5 questions), fear (4 questions), protection motivation (4 questions), perceived response effectiveness (4 questions), self-efficacy (5 questions), and behavior (5 questions). Questions were evaluated on a 5-point Likert scale (I completely agree=1 to completely disagree=5). To design the protection motivation theory items, we studied the literature on the protection motivation theory. Then, an expert panel of ten specialists in health education and health promotion reviewed the questionnaire. They evaluated the necessity and relevance of all items to quantify the content validity index and content validity ratio. In this investigation, the average content validity ratio of the questionnaire was 0.91, and the content validity index for this questionnaire was 0.90. We pilot-tested the questionnaire with 15 students to evaluate all items based on their clarity, readability, and simplicity. The reliability coefficient (Cronbach α) of preventive behaviors against CL based on the protection motivation theory questionnaire was 0.82, indicating a strong internal consistency of the questionnaire’s criterion. The correlation coefficient between all constructs was more than 0.65, which is considered satisfactory. Eligible participants in both groups completed this questionnaire at baseline (before the intervention), immediately after the intervention, and at 3-month follow-up. The demographic questionnaire was only completed at baseline.
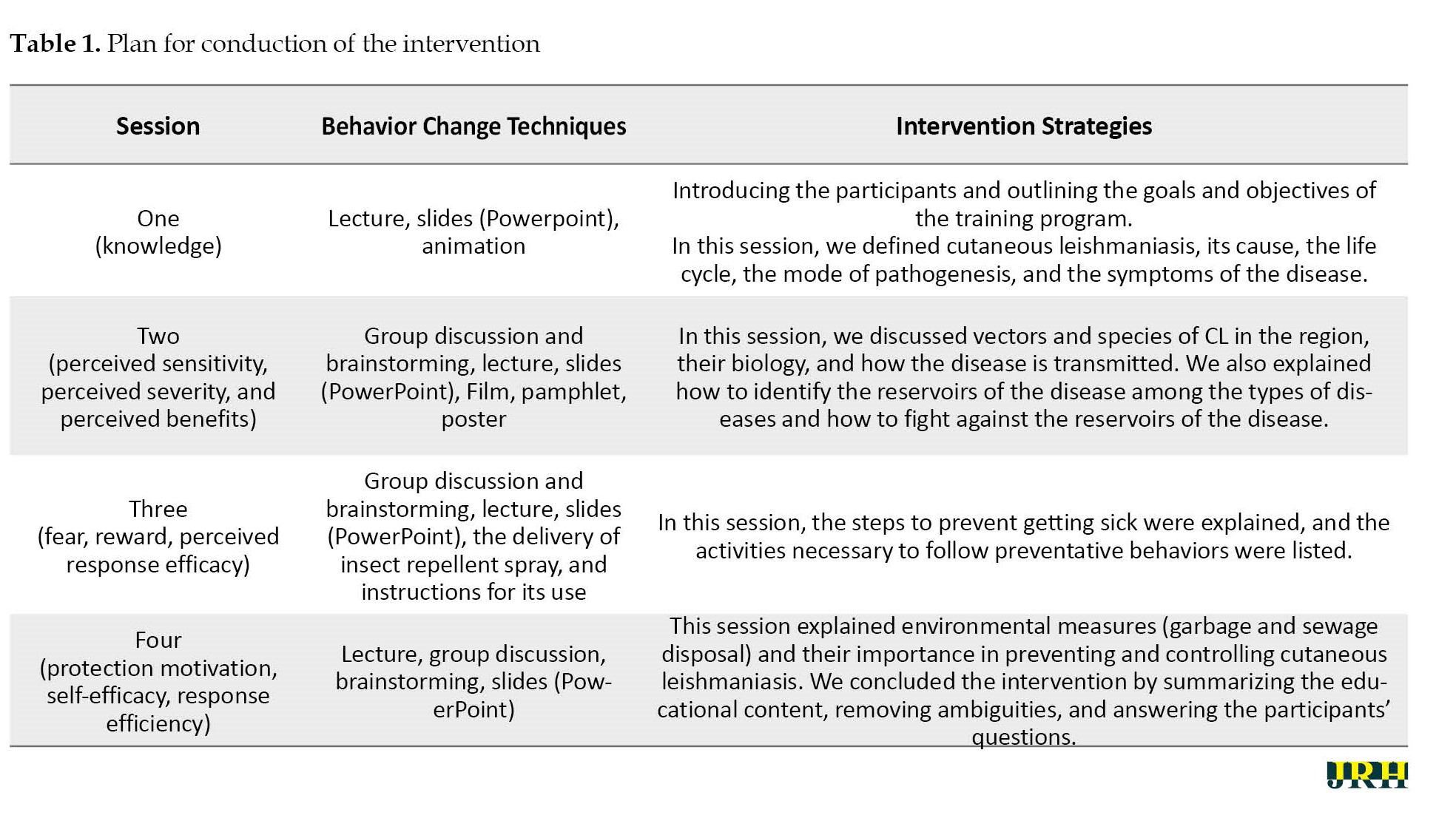
Eligible students were invited to participate in the study by phone. Students who agreed to participate in the study went to the comprehensive health service center they were covered by and completed the questionnaires in three stages (before, immediately after, and three months after the intervention). The intervention group students were invited to one of the schools near the comprehensive health service center and participated in four 60-minute training sessions in the hall of this school. Details of each training session are provided in Table 1.
Data analysis
Before inputting the data into SPSS software, version 24, the normality of the data was checked by the Kolmogorov-Smirnov test. The results of the test showed that the experimental and control groups were similar and had no significant differences. The paired sample t-test and Wilcoxon test were used to compare the mean/median difference of the subscales before and after the intervention. The t-test and Mann-Whitney test were used to compare the mean/median of the subscales between the two groups before and after the intervention. In all tests, the significance level <0.05.
Results
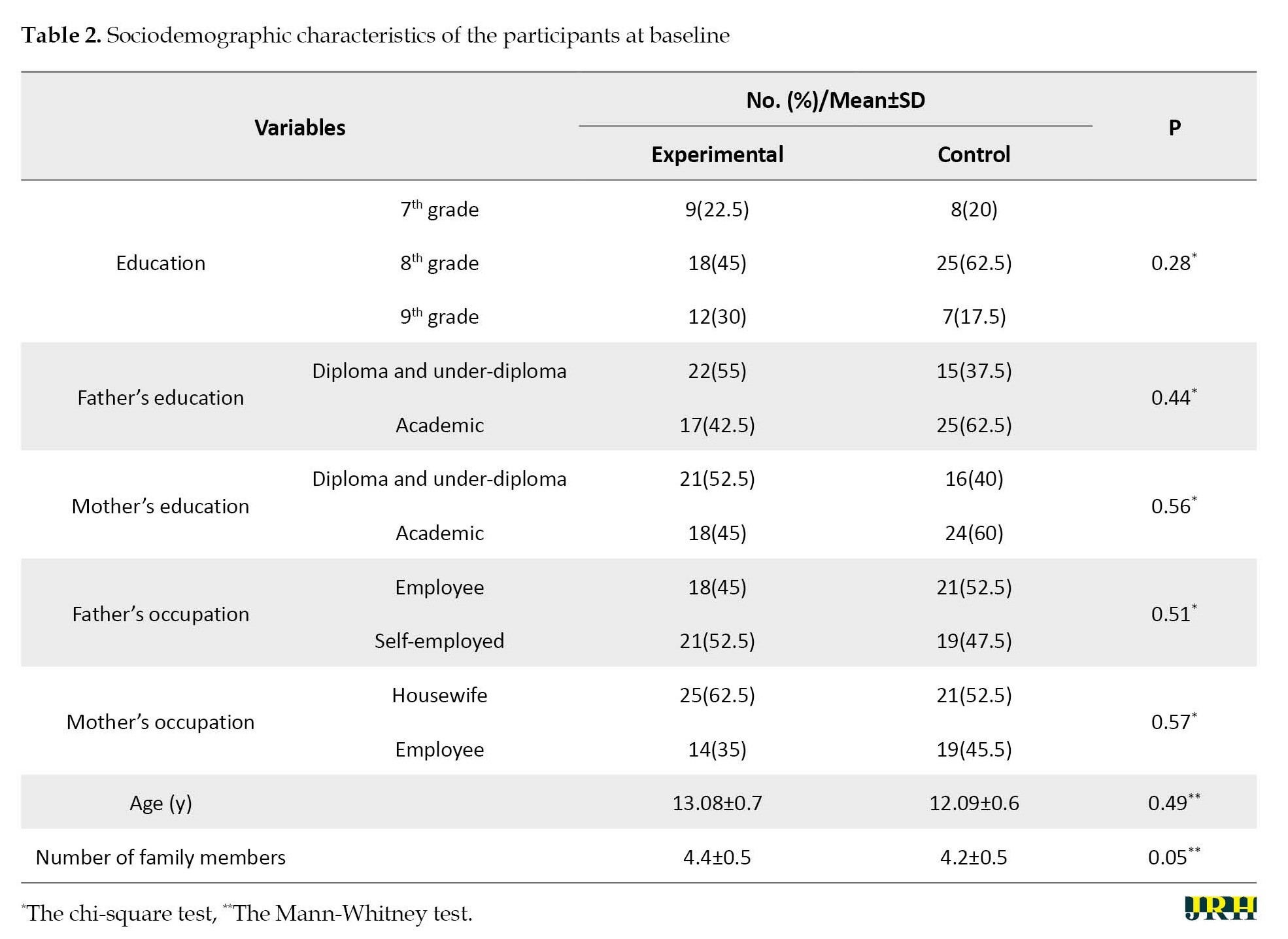
In this study, the Mean±SD age of participants in the control group was 12.9±0.6, and the test group was 13.08±0.7 years, and there was no significant difference between the two groups (P=0.49). Most participants in both groups were in the eighth grade, and there was no significant difference between the two groups in the educational level (P=0.28). There was no significant difference between the two groups in terms of the number of family members, parents’ education, and parents’ occupation (P>0.05) (Table 2).
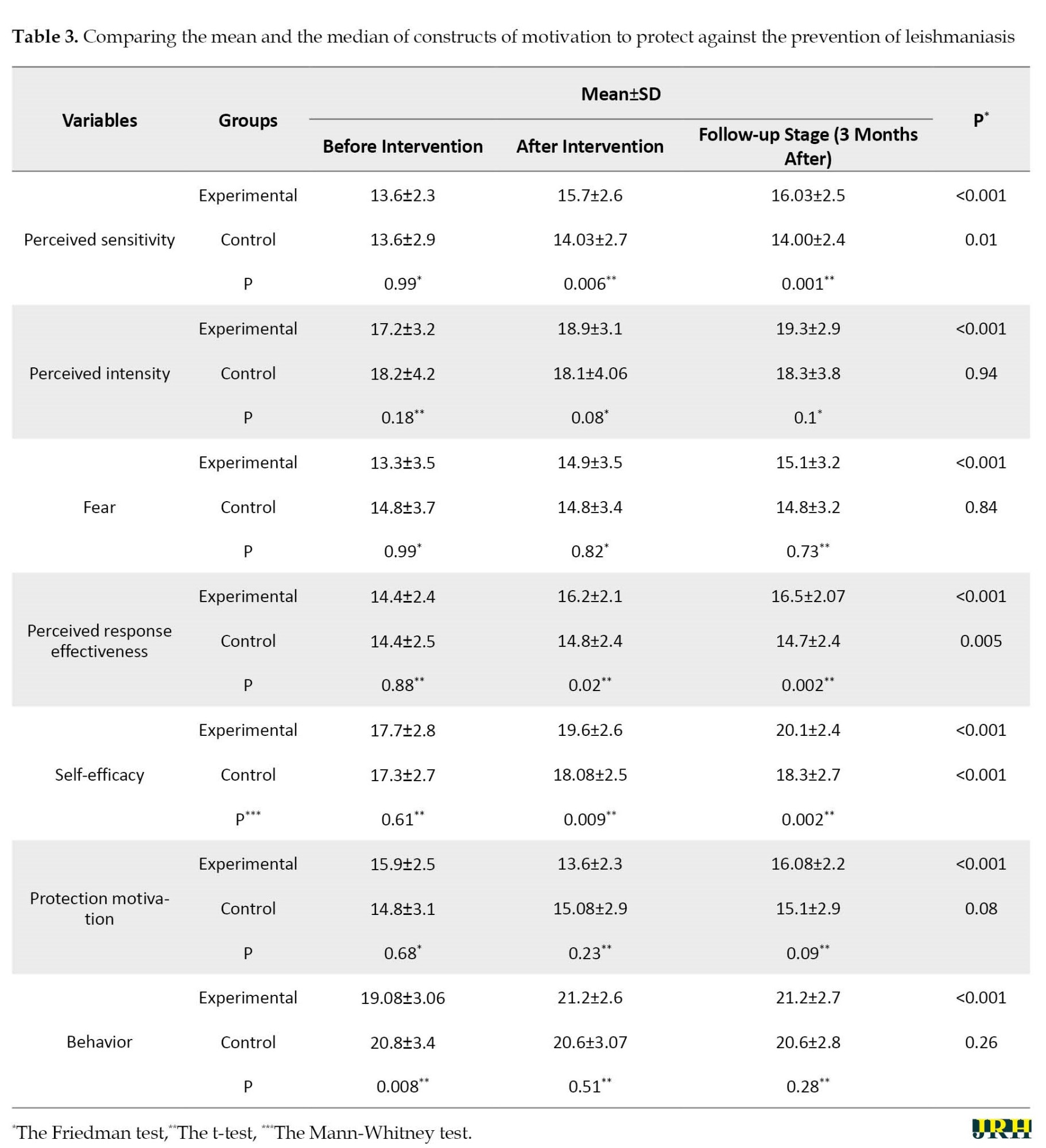
The Mean±SD of the perceived sensitivity score in the experimental group increased from 13.6±2.3 to 16.03±2.5 three months after the intervention, and these changes were significant (P<0.001). However, in the control group, the Mean±SD of the perceived sensitivity score from 13.6±2.9 increased to 14.00±2.4, but these changes were not significant (P=0.01). Regarding the perceived intensity, the Mean±SD score in the experimental group before the intervention was 17.2±3.2, which reached 19.3±2.9 three months after the intervention, and the increase was significant (P<0.001). Still, in the control group, it just increased from 18.2±4.2 to 18.3±3.8, which was not significant (P=0.94). The Mean±SD of the fear score in the experimental group increased from 13.3±3.5 to 15.1±3.2 three months after the intervention, and this change was significant (P<0.001). However, in the control group, the Mean±SD fear score changed from 14.8±3.7 to 14.8±3.2, which was not significant (P=0.84). In the experimental group, the Mean±SD of the perceived response effectiveness before the intervention was 14.4±2.4, and three months after the intervention, it reached 16.5±2.07, which was significant (P<0.001). However, in the control group, this score from 14.4±2.5 reached 14.7±2.4, and these changes were not significant (P=0.005). The Mean±SD self-efficacy score before the training was 17.7±2.8, which three months after the training was improved to 20.1±2.4. This increase was significant (P<0.001), and in the control group, it was 17.3±2.7, which changed to 18.3±2.7, which was also significant (P<0.001). The Mean±SD of the protection motivation score in the experimental group increased from 15.9±2.5 to 16.08±2.2 three months after the intervention, which was significant (P<0.001). However, in the control group, the Mean±SD of the protection motivation score changed from 14.8±3.1 to 15.1±2.9, which was not significant (P=0.08). The Mean±SD behavioral score in the experimental group increased from 19.8±3.06 to 21.2±2.7 three months after the intervention, which was significant (P<0.001). However, in the control group, the Mean±SD of the protection motivation score changed from 20.8±3.4 to 20.6±2.8, which was not significant (P=0.26) (Table 3).
Discussion
This research was carried out to determine the effect of education based on the theory of protection motivation on the preventative behaviors of the CL in the seventh, eighth, and ninth grades male students covered by the health center No. 1 in Mashhad City, Iran, in 2020.
In our study, no significant differences were observed in the perceived sensitivity score of the two groups before the intervention. However, a significant difference was observed between the experimental and control groups immediately and 3 months after the educational intervention. This finding differs from the study of Maseudi et al., which studied the harmful effects of sun rays in male students. In the Maseudi et al. study [12], perceived sensitivity in the test group increased after the educational intervention, and in the control group, the average score of perceived sensitivity decreased. Of course, this study did not check the immediately after the educational intervention in their study and followed up the training two months after the intervention. Still, in our study, the follow-up after the training was done three months after the intervention. Ghahremani et al. [24] also used conservation motivation theory to intervene in malaria prevention behaviors in Kerman City, Iran. In their study, mean scores for perceived sensitivity increased in the control group during the follow-up period, but this increase was not significant. However, in the test group, the increase in the average score of the perceived sensitivity was significant. Consistent with our study, in Jahani Eftekhari et al. study [25], the perceived sensitivity in the experimental and control groups increased compared to before the intervention, but this increase was significant in the experimental group, but not in the control group. Jahani Eftekhari et al. study [25] is different from our study as they investigated the effect of protection motivation theory on pediculosis prevention behaviors in their study and did not complete the questionnaire immediately after the intervention, and the follow-up period of their study was two months. Still, in our study, the questionnaires were completed immediately after the educational intervention, and the follow-up period was three months. Also, in the study by Jahani Eftekhari et al. [25], the target group was fifth-grade female students, which was different from the target group of our study. Malmir et al. [26] conducted an educational intervention based on the theory of motivation to protect against cervical cancer in western Iran. Their study showed that the average score of perceived sensitivity increased in the test and control groups. This increase in the test group means that it was not significant in the control group. Therefore, as seen in some studies, in line with the present study, in the follow-up phase, the perceived sensitivity score increase in both groups; that is, the belief that they are vulnerable to CL increases in the investigated adolescents [24-26]. However, this increase in the perceived harm in the experimental group because it was promoted based on the educational intervention only leads to preventive behaviors in this group and in the control group there is no change in the promotion of CL preventive behaviors and even preventive behaviors are reduced. Therefore, perceived sensitivity should be improved on the basis of scientific training, so that people can have this sense of self-efficacy to deal with this injury.
Regarding the construct of perceived intensity, the results of our study showed that the average score of perceived intensity increased in both groups after the intervention, and these changes were significant in the experimental group but not significant in the control group, which is consistent with some studies [7, 24, 26-28]. However, in some other studies [12, 25, 29, 30], the perceived intensity score of the experimental group increased significantly after the educational intervention, while it was not significant in the control group. The significant increase in the average score of perceived intensity in the experimental group after the educational intervention is similar to our study. Still, the decrease in the average score of perceived intensity in the control group is contrary to our research. According to the theory of protection motivation, perceived sensitivity and perceived severity make up threat evaluation. In the present study, the intensity perceived in the control group was also high. Still, the intensity perceived in the control group in the follow-up phase is lower than in the experimental group. Hence, the belief that the risk is more severe in the experimental group than in the control group is created due to the educational intervention, leading to proper performance in preventing CL.
Our study showed that the average score of the perceived response efficiency structure increased in both the experimental and control groups after the intervention compared to before the intervention; this increase was significant in the experimental group but not significant in the control group, which is in line with some studies [12, 26, 27], but inconsistent with the interventions of some other studies [7, 24, 25, 30].
In our study, self-efficacy increased in both control and test groups after 3 months, and this increase was significant in the experimental group but not in the control group. Some study results [7, 24, 28] are consistent with ours, but some are contrary to ours [12, 25-27, 30].
Regarding the protection motivation component, our study’s results showed that the average score of this component in both groups increased after the study compared to before the study, which is in line with some studies [7, 26, 28]. This increase was significant in the experimental group but not the control group. The results of our research are contrary to some studies [12, 25, 29, 30]. In these studies, the average protection motivation score in the test group increased in the follow-up period compared to before the intervention. However, in the control group, it is reduced in the follow-up period compared to before the intervention. Creating the desired protective motivation to encourage the performance of the target behavior is one of the strategies emphasized in education studies. In the present study, when the mean scores of protection motivation was directly compared, it showed that teenagers in the control group who did not receive the training program were in the same condition regarding the level of protection motivation before and immediately after the intervention. Thus, the educational program has been able to affect positively the motivation to protect teenagers in the test group in the field of preventive behaviors against CL.
In the present study, the average fear score in the test and control groups increases in the follow-up period compared to before the intervention, which is significant in the experimental group but not significant in the control group, which is in line with some studies [7, 26]. In some studies [12, 28, 29], the average fear score in the experimental group before the intervention increases compared to the one after the intervention, which is statistically significant. However, in the control group, mean fear scores decreased before the intervention compared to after the intervention, but this change was not statistically significant. This also contrasts the study [30], in which fear scores in the test and control groups decreased during the follow-up period.
In the present study, the average score of preventive behavior against CL in the experimental group increased 3 months after the educational intervention compared to before the educational intervention, which was statistically significant. However, in the control group, the average score of preventive behavior against CL decreased compared to before the intervention. Ghahremani et al. [24] study results in malaria prevention behaviors were consistent with our study. Khani Jeihooni et al.’s research [7] on skin cancer prevention behaviors and Malmir et al.’s study [26] on regular Pap smears are consistent with this study. But with the study of Jahani Eftekhari et al. regarding behaviors to prevent pediculosis [25] and Maseudi et al. [12]. In the act of protecting against the harmful effects of sunlight, Baghianimoghadam et al. [29] in preventing skin cancer and the Acts of Ansari et al. [30] in action against influenza A, Ebadi Fardazar et al. [27] and Khosravi et al. [28] are inconsistent in prostate cancer prevention behaviors in men. The results of this research showed that in the experimental group, there was a significant difference between the average score of behavior before, immediately, and after the educational intervention three times and the preventative behaviors of CL in these people increased significantly after the intervention.
Conclusion
Finally, based on the research findings, the educational intervention significantly improved the performance of preventive behaviors against contracting CL in adolescents in the test group compared to the control group. This behavior improvement can relate to the theory used and suitable educational methods and materials (lecture, group discussion, brainstorming, question and answer, use of slides, films and animations, pamphlets, posters, and repellent sprays Insects). Therefore, the design and implementation of educational programs during adolescence can significantly increase the type of perceived sensitivity and intensity, the fear of infection, and the motivation to protect against the disease in the preventive behaviors of CL. Therefore, considering the subject’s importance and the educational intervention’s effectiveness, it is suggested that this intervention be carried out in schools for adolescent boys.
Study strengths and limitations
This study is one of the few studies conducted on teenage boys using the protection motivation theory, and the results showed that this intervention had a positive effect on the prevention behaviors of CL. Therefore, such low-cost interventions can be used to prevent this disease, which is expensive and requires extended treatment. One of the limitations of this study is the lack of studies on girls. Also, it was performed only in the age group of 12 to 14 years. Hence, it is suggested that it be done for teenagers in other age groups and female students. Another limitation of the study is the self-reported information gathered before and immediately after the intervention, which may cause a certain percentage of error. Another limitation of this study is the small sample size, limited to one region, leading to low generalizability of the results.
Ethical Considerations
Compliance with ethical guidelines
This study is based on a research project approved by Mashhad University of Medical Sciences (Project Code: IR.MUMS.REC.1399.608).
Funding
The study was supported financially by Mashhad University of Medical Sciences (Grant No.: 991218).
Authors' contributions
Study design and conceptualization: Nooshin Peyman and Mahmood Fakhar; Data analysis and data interpretation: Atiye Kamel Khodabande and Mahmood Fakhar; Writing the original draft: Mahmood Fakhar; Review and editing: Elham Charoghchian Khorasani; Final approving: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their profound appreciation to the students who participated in this study and the Mashhad Health Center No. 1 staff who assisted the authors in running this research project.
References
Leishmaniasis is a common disease between humans and animals. It is caused by different protozoan species of the Leishmania genus and is transmitted by female Phlebotomus mosquitoes and rodents, which are the leading reservoirs and sources, respectively. Leishmaniasis occurs in three forms: Cutaneous (oriental sore), visceral (kala-azar), and mucocutaneous [1, 2, 3]. Although the disease is mainly seen in tropical and subtropical regions, it is endemic in 88 countries worldwide, and 350 million people worldwide are at risk of infection. Fourteen million people are affected by the disease, and there are 1.5 million new cases of cutaneous leishmaniasis (CL) each year [4, 5]. Unlike other infectious diseases, the frequency of this disease is increasing. This increase is mainly due to migration, population movements, infection, global warming, and changes in human ecology. Although the death rate caused by CL is very low, due to the long duration of the wound, the creation of inappropriate scars, and the possibility of secondary infections, it has brought heavy treatment costs to society along with the increase in the length of the treatment period and the complications caused by the use of existing drugs [6, 7].
Due to the unavailability of a safe vaccine to prevent CL, it is necessary to avoid contracting the disease. CL can be prevented by reducing human contact with the vectors or by reducing the number of reservoirs. Nets, mosquito nets, or insect repellants should be used to control the vector. Using insect repellents is a preventive measure for people living in endemic areas[8]. CL is one of Iran’s most common endemic diseases [9]. Among Phlebotomus species in Iran, Phlebotomus papatasi and Phlebotomus sergenti are vectors, and the great gerbil, Meriones hurrianae, Meriones libycus, Meriones persicus, and Nesokia indica contribute as reservoirs in Iran [10, 11].
In Iran, the provinces of Isfahan, Fars, and Khorasan Razavi have the highest frequency of infection with CL in descending order. Khorasan-Razavi Province, is located in the northeast of Iran with a frequency of 1801 people in 2017. The city of Mashhad, the center of Khorasan-Razavi Province, is one of the main areas infected with CL [12]. As mentioned, infection prevention is the most critical measure, and educational interventions can be used to change preventive behaviors against CL [13]. Choosing a model or theory is the best measure in educational planning. This model or theory must be consistent with the purpose of the educational program [14, 15]. One of the theories that focus on the factors affecting the motivation and, finally, the protection behavior of the individual is the protection motivation theory [16].
Since this study was designed to change behavior for prevention, it seems helpful to use this theory. Rogers designed the theory of protection motivation in 1975 [17]. Rogers proposed that fear is influenced by five constructs of protective motivation (perceived sensitivity, perceived severity, perceived response efficacy, protective motivation, and perceived self-efficacy), which ultimately trigger healthy behaviors [18]. This theory investigates the factors affecting the individual’s motivation and behavior. It assumes that protective behavior against health risks is a direct behavior of the people’s motivation to protect themselves [19]. In general, the components of this theory are placed in two cognitive mediating processes: Threat assessment (examination of unhealthy behaviors and factors affecting the possibility of engaging in them) and coping assessment (the ability to deal with and avoid the threatened danger) [20]. The constructs of the theory are as follows: Perceived sensitivity, people’s belief that they are vulnerable to a health threat; perceived severity, people’s belief that the risk is serious; perceived response efficiency, people’s expectations that the adaptive response (protective behavior against health risk) can eliminate the risk; fear, an intermediate variable between sensitivity and severity perceived by threat assessment; and self-efficacy, people’s belief that they can effectively and successfully perform the suggested behavior [21, 22]. According to the constructs of the protection motivation theory and the target group, it seems that this theory can affect the preventive behaviors of CL in adolescent boys because students aged 10 to 15 years are the most vulnerable groups to CL in endemic areas [23]. Because this group is the most vulnerable and most accessible group that can improve the health behaviors of families by acquiring education, they were chosen as the target group. Since the prevention of CL is a simple and inexpensive task compared to its treatment [8], this research was conducted to determine the effect of education based on the theory of protection motivation on the preventative behaviors of the seventh, eighth, or ninth grade male students covered by the health center No. 1 in Mashhad City, Iran, in 2020.
Methods
Research design
This quasi-experimental study was conducted in Mashhad, 950 km from the capital (Tehran City). The city of Mashhad is divided into 5 centers in terms of health. This study was carried out in one of these 5 centers (Health Center No. 1). Through a random cluster sampling, 80 students were selected out of the 23152 students in the seventh, eighth, and ninth graders covered by the Health Center No. 1. In Mashhad, Iran in 2020.
Study participants
The inclusion criteria were as follows: Willingness to participate in the study, filling out a written consent form, being a resident of Mashhad, and being a male student of the seventh, eighth, or ninth grade. The exclusion criteria included unwillingness to continue cooperation during the intervention program and absence of more than one session from the training course.
Based on Maseudi et al. [12] study and considering 95% confidence interval, 80% test power, and 15% loss rate, the sample size was calculated to be 80 using the sampling formula to compare the average values between two study groups (experimental group=40, control group=40) (Equation 1).
The sampling method was a multi-stage random cluster sampling so that among the five Mashhad health centers, one center was randomly selected as a cluster, which was health center number one. Among the comprehensive health service centers of Health Center No. 1, one center was randomly selected as control and one center as experimental. The samples were selected within the comprehensive health services center, so the researcher contacted the people who met the conditions to enter the study. If they were content, they were included in the study.
Data collection
The intervention based on protection motivation theory was the independent variable, and the covariates studied were demographic characteristics, including age, number of family members, education level, father’s education, mother’s education, father’s occupation, and mother’s occupation.
This research used two questionnaires for data collection: The demographic section and CL protection motivation theory constructs. The demographic questionnaire gathered covariates information. The researcher created the CL protection motivation theory constructs questionnaire with 31 questions: Perceived sensitivity (4 questions), perceived intensity (5 questions), fear (4 questions), protection motivation (4 questions), perceived response effectiveness (4 questions), self-efficacy (5 questions), and behavior (5 questions). Questions were evaluated on a 5-point Likert scale (I completely agree=1 to completely disagree=5). To design the protection motivation theory items, we studied the literature on the protection motivation theory. Then, an expert panel of ten specialists in health education and health promotion reviewed the questionnaire. They evaluated the necessity and relevance of all items to quantify the content validity index and content validity ratio. In this investigation, the average content validity ratio of the questionnaire was 0.91, and the content validity index for this questionnaire was 0.90. We pilot-tested the questionnaire with 15 students to evaluate all items based on their clarity, readability, and simplicity. The reliability coefficient (Cronbach α) of preventive behaviors against CL based on the protection motivation theory questionnaire was 0.82, indicating a strong internal consistency of the questionnaire’s criterion. The correlation coefficient between all constructs was more than 0.65, which is considered satisfactory. Eligible participants in both groups completed this questionnaire at baseline (before the intervention), immediately after the intervention, and at 3-month follow-up. The demographic questionnaire was only completed at baseline.
Eligible students were invited to participate in the study by phone. Students who agreed to participate in the study went to the comprehensive health service center they were covered by and completed the questionnaires in three stages (before, immediately after, and three months after the intervention). The intervention group students were invited to one of the schools near the comprehensive health service center and participated in four 60-minute training sessions in the hall of this school. Details of each training session are provided in Table 1.
Data analysis
Before inputting the data into SPSS software, version 24, the normality of the data was checked by the Kolmogorov-Smirnov test. The results of the test showed that the experimental and control groups were similar and had no significant differences. The paired sample t-test and Wilcoxon test were used to compare the mean/median difference of the subscales before and after the intervention. The t-test and Mann-Whitney test were used to compare the mean/median of the subscales between the two groups before and after the intervention. In all tests, the significance level <0.05.
Results
In this study, the Mean±SD age of participants in the control group was 12.9±0.6, and the test group was 13.08±0.7 years, and there was no significant difference between the two groups (P=0.49). Most participants in both groups were in the eighth grade, and there was no significant difference between the two groups in the educational level (P=0.28). There was no significant difference between the two groups in terms of the number of family members, parents’ education, and parents’ occupation (P>0.05) (Table 2).
The Mean±SD of the perceived sensitivity score in the experimental group increased from 13.6±2.3 to 16.03±2.5 three months after the intervention, and these changes were significant (P<0.001). However, in the control group, the Mean±SD of the perceived sensitivity score from 13.6±2.9 increased to 14.00±2.4, but these changes were not significant (P=0.01). Regarding the perceived intensity, the Mean±SD score in the experimental group before the intervention was 17.2±3.2, which reached 19.3±2.9 three months after the intervention, and the increase was significant (P<0.001). Still, in the control group, it just increased from 18.2±4.2 to 18.3±3.8, which was not significant (P=0.94). The Mean±SD of the fear score in the experimental group increased from 13.3±3.5 to 15.1±3.2 three months after the intervention, and this change was significant (P<0.001). However, in the control group, the Mean±SD fear score changed from 14.8±3.7 to 14.8±3.2, which was not significant (P=0.84). In the experimental group, the Mean±SD of the perceived response effectiveness before the intervention was 14.4±2.4, and three months after the intervention, it reached 16.5±2.07, which was significant (P<0.001). However, in the control group, this score from 14.4±2.5 reached 14.7±2.4, and these changes were not significant (P=0.005). The Mean±SD self-efficacy score before the training was 17.7±2.8, which three months after the training was improved to 20.1±2.4. This increase was significant (P<0.001), and in the control group, it was 17.3±2.7, which changed to 18.3±2.7, which was also significant (P<0.001). The Mean±SD of the protection motivation score in the experimental group increased from 15.9±2.5 to 16.08±2.2 three months after the intervention, which was significant (P<0.001). However, in the control group, the Mean±SD of the protection motivation score changed from 14.8±3.1 to 15.1±2.9, which was not significant (P=0.08). The Mean±SD behavioral score in the experimental group increased from 19.8±3.06 to 21.2±2.7 three months after the intervention, which was significant (P<0.001). However, in the control group, the Mean±SD of the protection motivation score changed from 20.8±3.4 to 20.6±2.8, which was not significant (P=0.26) (Table 3).
Discussion
This research was carried out to determine the effect of education based on the theory of protection motivation on the preventative behaviors of the CL in the seventh, eighth, and ninth grades male students covered by the health center No. 1 in Mashhad City, Iran, in 2020.
In our study, no significant differences were observed in the perceived sensitivity score of the two groups before the intervention. However, a significant difference was observed between the experimental and control groups immediately and 3 months after the educational intervention. This finding differs from the study of Maseudi et al., which studied the harmful effects of sun rays in male students. In the Maseudi et al. study [12], perceived sensitivity in the test group increased after the educational intervention, and in the control group, the average score of perceived sensitivity decreased. Of course, this study did not check the immediately after the educational intervention in their study and followed up the training two months after the intervention. Still, in our study, the follow-up after the training was done three months after the intervention. Ghahremani et al. [24] also used conservation motivation theory to intervene in malaria prevention behaviors in Kerman City, Iran. In their study, mean scores for perceived sensitivity increased in the control group during the follow-up period, but this increase was not significant. However, in the test group, the increase in the average score of the perceived sensitivity was significant. Consistent with our study, in Jahani Eftekhari et al. study [25], the perceived sensitivity in the experimental and control groups increased compared to before the intervention, but this increase was significant in the experimental group, but not in the control group. Jahani Eftekhari et al. study [25] is different from our study as they investigated the effect of protection motivation theory on pediculosis prevention behaviors in their study and did not complete the questionnaire immediately after the intervention, and the follow-up period of their study was two months. Still, in our study, the questionnaires were completed immediately after the educational intervention, and the follow-up period was three months. Also, in the study by Jahani Eftekhari et al. [25], the target group was fifth-grade female students, which was different from the target group of our study. Malmir et al. [26] conducted an educational intervention based on the theory of motivation to protect against cervical cancer in western Iran. Their study showed that the average score of perceived sensitivity increased in the test and control groups. This increase in the test group means that it was not significant in the control group. Therefore, as seen in some studies, in line with the present study, in the follow-up phase, the perceived sensitivity score increase in both groups; that is, the belief that they are vulnerable to CL increases in the investigated adolescents [24-26]. However, this increase in the perceived harm in the experimental group because it was promoted based on the educational intervention only leads to preventive behaviors in this group and in the control group there is no change in the promotion of CL preventive behaviors and even preventive behaviors are reduced. Therefore, perceived sensitivity should be improved on the basis of scientific training, so that people can have this sense of self-efficacy to deal with this injury.
Regarding the construct of perceived intensity, the results of our study showed that the average score of perceived intensity increased in both groups after the intervention, and these changes were significant in the experimental group but not significant in the control group, which is consistent with some studies [7, 24, 26-28]. However, in some other studies [12, 25, 29, 30], the perceived intensity score of the experimental group increased significantly after the educational intervention, while it was not significant in the control group. The significant increase in the average score of perceived intensity in the experimental group after the educational intervention is similar to our study. Still, the decrease in the average score of perceived intensity in the control group is contrary to our research. According to the theory of protection motivation, perceived sensitivity and perceived severity make up threat evaluation. In the present study, the intensity perceived in the control group was also high. Still, the intensity perceived in the control group in the follow-up phase is lower than in the experimental group. Hence, the belief that the risk is more severe in the experimental group than in the control group is created due to the educational intervention, leading to proper performance in preventing CL.
Our study showed that the average score of the perceived response efficiency structure increased in both the experimental and control groups after the intervention compared to before the intervention; this increase was significant in the experimental group but not significant in the control group, which is in line with some studies [12, 26, 27], but inconsistent with the interventions of some other studies [7, 24, 25, 30].
In our study, self-efficacy increased in both control and test groups after 3 months, and this increase was significant in the experimental group but not in the control group. Some study results [7, 24, 28] are consistent with ours, but some are contrary to ours [12, 25-27, 30].
Regarding the protection motivation component, our study’s results showed that the average score of this component in both groups increased after the study compared to before the study, which is in line with some studies [7, 26, 28]. This increase was significant in the experimental group but not the control group. The results of our research are contrary to some studies [12, 25, 29, 30]. In these studies, the average protection motivation score in the test group increased in the follow-up period compared to before the intervention. However, in the control group, it is reduced in the follow-up period compared to before the intervention. Creating the desired protective motivation to encourage the performance of the target behavior is one of the strategies emphasized in education studies. In the present study, when the mean scores of protection motivation was directly compared, it showed that teenagers in the control group who did not receive the training program were in the same condition regarding the level of protection motivation before and immediately after the intervention. Thus, the educational program has been able to affect positively the motivation to protect teenagers in the test group in the field of preventive behaviors against CL.
In the present study, the average fear score in the test and control groups increases in the follow-up period compared to before the intervention, which is significant in the experimental group but not significant in the control group, which is in line with some studies [7, 26]. In some studies [12, 28, 29], the average fear score in the experimental group before the intervention increases compared to the one after the intervention, which is statistically significant. However, in the control group, mean fear scores decreased before the intervention compared to after the intervention, but this change was not statistically significant. This also contrasts the study [30], in which fear scores in the test and control groups decreased during the follow-up period.
In the present study, the average score of preventive behavior against CL in the experimental group increased 3 months after the educational intervention compared to before the educational intervention, which was statistically significant. However, in the control group, the average score of preventive behavior against CL decreased compared to before the intervention. Ghahremani et al. [24] study results in malaria prevention behaviors were consistent with our study. Khani Jeihooni et al.’s research [7] on skin cancer prevention behaviors and Malmir et al.’s study [26] on regular Pap smears are consistent with this study. But with the study of Jahani Eftekhari et al. regarding behaviors to prevent pediculosis [25] and Maseudi et al. [12]. In the act of protecting against the harmful effects of sunlight, Baghianimoghadam et al. [29] in preventing skin cancer and the Acts of Ansari et al. [30] in action against influenza A, Ebadi Fardazar et al. [27] and Khosravi et al. [28] are inconsistent in prostate cancer prevention behaviors in men. The results of this research showed that in the experimental group, there was a significant difference between the average score of behavior before, immediately, and after the educational intervention three times and the preventative behaviors of CL in these people increased significantly after the intervention.
Conclusion
Finally, based on the research findings, the educational intervention significantly improved the performance of preventive behaviors against contracting CL in adolescents in the test group compared to the control group. This behavior improvement can relate to the theory used and suitable educational methods and materials (lecture, group discussion, brainstorming, question and answer, use of slides, films and animations, pamphlets, posters, and repellent sprays Insects). Therefore, the design and implementation of educational programs during adolescence can significantly increase the type of perceived sensitivity and intensity, the fear of infection, and the motivation to protect against the disease in the preventive behaviors of CL. Therefore, considering the subject’s importance and the educational intervention’s effectiveness, it is suggested that this intervention be carried out in schools for adolescent boys.
Study strengths and limitations
This study is one of the few studies conducted on teenage boys using the protection motivation theory, and the results showed that this intervention had a positive effect on the prevention behaviors of CL. Therefore, such low-cost interventions can be used to prevent this disease, which is expensive and requires extended treatment. One of the limitations of this study is the lack of studies on girls. Also, it was performed only in the age group of 12 to 14 years. Hence, it is suggested that it be done for teenagers in other age groups and female students. Another limitation of the study is the self-reported information gathered before and immediately after the intervention, which may cause a certain percentage of error. Another limitation of this study is the small sample size, limited to one region, leading to low generalizability of the results.
Ethical Considerations
Compliance with ethical guidelines
This study is based on a research project approved by Mashhad University of Medical Sciences (Project Code: IR.MUMS.REC.1399.608).
Funding
The study was supported financially by Mashhad University of Medical Sciences (Grant No.: 991218).
Authors' contributions
Study design and conceptualization: Nooshin Peyman and Mahmood Fakhar; Data analysis and data interpretation: Atiye Kamel Khodabande and Mahmood Fakhar; Writing the original draft: Mahmood Fakhar; Review and editing: Elham Charoghchian Khorasani; Final approving: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their profound appreciation to the students who participated in this study and the Mashhad Health Center No. 1 staff who assisted the authors in running this research project.
References
- Bhutta ZA, Sommerfeld J, Lassi ZS, Salam RA, Das JK. Global burden, distribution, and interventions for infectious diseases of poverty. Infectious Diseases of Poverty. 2014; 3:21. [DOI:10.1186/2049-9957-3-21] [PMID]
- Vesali Monfared E, Sadeghi R, Sedaghat M M, Saghafipour A, Tol A, Yaseri M. [Effect of educational intervention based on social cognitive theory on promoting preventive behaviors of cutaneous leishmaniasis (Persian)]. Koomesh. 2018; 20(4):692-8. [Link]
- Nasiri Z, Kalantari M, Mohammadi J, Daliri S, Mehrabani D, Azizi K. Cutaneous leishmaniasis in Iran: A review of epidemiological aspects, with emphasis on molecular findings. Parasite. 2022; 29:47. [DOI:10.1051/parasite/2022047] [PMID]
- Norouzinezhad F, Ghaffari F, Norouzinejad A, Kaveh F, Gouya MM. Cutaneous leishmaniasis in Iran: Results from an epidemiological study in urban and rural provinces. Asian Pacific Journal of Tropical Biomedicine. 2016; 6(7):614-9. [DOI:10.1016/j.apjtb.2016.05.005]
- Jafarpour M, Aivazi A, Jalali A, Ghazanfari Z. [Assessing preventive Behaviors of Leishmaniasis in Mehran Countyat 2014: Application of BASNEF Model (Persian)]. Journal of Ilam University of Medical Sciences. 2017; 25(3):23-31. [DOI:10.29252/sjimu.25.3.23]
- Kavoosi F, Shojaeizadeh D. [Effect of the educational interventions on mothers’ knowledge and attitude towards cutaneous leishmaniasis in Mashhad (Persian)]. Journal of Dermatology and Cosmetic. 2016; 4(6):209-20. [Link]
- Khani Jeihooni A, Hatami M, Kashfi SM, Heshmati H. [The effectiveness of education based on BASNEF model program in promotion of preventive behavior of leishmaniasis among health workers and families under health centers coverage(Persian)]. Journal of Advanced Biomedical Sciences. 2012; 2(1):26-33. [Link]
- Alidosti M, Heidari Z, Shahnazi H, Zamani-Alavijeh F. Behaviors and perceptions related to cutaneous leishmaniasis in endemic areas of the world: A review. Acta Tropica. 2021; 223:106090. [DOI:10.1016/j.actatropica.2021.106090] [PMID]
- Bennis I, Thys S, Filali H, De Brouwere V, Sahibi H, Boelaert M. Psychosocial impact of scars due to cutaneous leishmaniasis on high school students in Errachidia province, Morocco. Infectious Diseases of Poverty. 2017; 6(1):46. [DOI:10.1186/s40249-017-0267-5] [PMID]
- Sabzevari S, Mohebali M, Hashemi A. Cutaneous and visceral leishmaniasis: Parasites, vectors and reservoir hosts in endemic foci of North Khorasan, Northeastern Iran-a narrative review. Journal of Medical Microbiology and Infectious Diseases. 2020; 8(2):40-4. [DOI:10.29252/JoMMID.8.2.40]
- Sabzevari S, Mohebali M, Hashemi SA. Mucosal and mucocutaneous leishmaniasis in iran from 1968 to 2018: A narrative review of clinical features, treatments, and outcomes. International Journal of Dermatology. 2020; 59(5):606-12.[PMID]
- Maseudi GR, Hosseini E, Mirzaei R, Shahrakipour M, Hosseini SA. [The effect of education based on protection motivation theory on the harmful effects of solar rays on male students (Persian)]. Iranian Journal of Health Education and Health Promotion. 2015; 2(4):322-30. [Link]
- Alizadeh G, Shahnazi H, Hassanzadeh A. Application of BASNEF model in students training regarding cutaneous leishmaniasis prevention behaviors: A school-based quasi experimental study. BMC Infectious Diseases. 2021; 21(1):1164.[DOI:10.1186/s12879-021-06874-2] [PMID]
- Haghani S, Shahnazi H, Hassanzadeh A. Effects of tailored health education program on overweight elementary school students’ obesity-related lifestyle: A school-based interventional study. Oman Medical Journal. 2017; 32(2):140-7.[DOI:10.5001/omj.2017.25] [PMID]
- Charoghchian Khorasani E, Peyman N, Esmaily H. [Effect of education based on the theory of self-efficacy and health literacy strategies on exclusive breastfeeding: A randomized clinical trial (Persian)]. Koomesh. 2019; 21(4):633-8. [Link]
- Hosseini ZS, Tavakoli Ghouchani H, Mehri A, Mohaddes Hakak HR, Lashkardoost H, Khankolabi M, et al. [Factors related to breast cancer preventive behaviors in middle-aged women: An application of protection motivation theory (Persian)]. Iranian Journal of Breast Diseases. 2022; 14(4):62-74. [Link]
- Azadeh M, Ramezani T, Taheri Kharameh Z. Investigating the factors affecting protective behaviors in the workplace of covid-19 disease in employees of frequent departments in Qom: Application of protection motivation theory. Iran Occupational Health. 2020; 17(1):115-25. [Link]
- Kaviani AH, Roozbahani N, Khorsandi M. [The assessment of the protection motivation theory construct of skin cancer preventive behavior in rural women (Persian)]. Avicenna Journal of Nursing and Midwifery Care. 2016; 24(4):229-37.[DOI:10.21859/nmj-24043]
- Bakht R, Shobeiri F, Roshanaei Gh, Fakori E. [The factors affecting cervical cancer screening among addicted women of Hamedan in 2015: On the basis of Protection Motivation Theory mode (Persian)]. Jorjani Biomedicine Journal. 2017; 4(2):68-80. [Link]
- Zakipour M, Hajalizadeh K, Sirfi MR, Nikparvar M, Abedini S. [The effect of the intervention based on protection theory on the drug compliance of the patients with ischemic heart disease (Persian)]. Medical Journal of Mashhad University of Medical Sciences. 2021; 64(2):2964-73. [DOI:10.22038/MJMS.2021.18506]
- Tazval J, Ghafari M, Mohtashami Yeganeh F, Babazadeh T, Rabati R. [Efficiency of protection motivation theory on prediction of skin cancer and sunlight preventive behaviors in farmers in Ilam county (Persian)]. Journal of Health. 2016; 7(5):656-67. [Link]
- Tehrani H, Dadashi N, Movahedzadeh D, Khorasani EC, Jafari A. The predictors of the use of complementary and alternative medicine among type 2 diabetes patients based on the health belief model. J Diabetes Metab Disord. 2022 Jan 11;21(1):285-292. [DOI: 10.1007/s40200-022-00971-y] [PMID]
- Tesfay K, Mardu F, Berhe B, Negash H, Legese H, Adhanom G, et al. Household knowledge, practice and treatment seeking behaviors towards cutaneous leishmaniasis in the endemic rural communities of Ganta-afeshum district, Tigrai, northern Ethiopia, 2019: A cross-sectional study. Tropical Diseases, Travel Medicine and Vaccines. 2021; 7(1):19. [DOI:10.1186/s40794-021-00144-4] [PMID]
- Ghahremani L, Faryabi R, Kaveh MH. Effect of health education based on the protection motivation theory on malaria preventive behaviors in rural households of Kerman, Iran. International Journal of Preventive Medicine. 2014; 5:463-71. [PMID]
- Jahani Eftekhari M, Peyman N. Effect of educational intervention based on protection motivation theory on promoting pediculosis preventive behaviors among elementary school girls in Neyshabur. Journal of Education and Community Health. 2018; 5(2):1-7. [DOI:10.21859/jech.5.2.1]
- Malmir S, Barati M, Khani Jeihooni A, Bashirian S, Hazavehei SMM. Effect of an educational intervention based on protection motivation theory on preventing cervical cancer among marginalized women in west Iran. Asian Pacific Journal of Cancer Prevention. 2018; 19(3):755-61. [PMID]
- Ebadi Fardazar F, Hashemi SS, Solhi MS, mansori K. [The effect of educational intervention based on protection motivation theory on mothers’ behaviors about prevention of home accidents in children under 5 year old (Persian)]. Journal of Health Research in Community. 2016; 1(4):37-44. [Link]
- Khosravi V, Barati M, Moeini B, Mohammadi Y. [The effect of an educational intervention based on protection motivation theory on prostate cancer prevention behaviors in men 50 to 75 years old (Persian)]. Hayat Journal. 2019; 24(4):342-54. [Link]
- Baghianimoghadam MH, Mohammadi S, Mazloomi Mahmoudabad SS, Norbala MT. [The effect of education based on protection-motivation theory on skin cancer preventive practices among female high school students in Yazd (Persian)]. Internal Medicine Today. 2011; 17(2):27-34. [Link]
- Ansari MA, Gharlipour Z, Mohebi S, Sharifirad GR, Rahbar A. [Effect of education based on the protection motivation theory on preventive behaviors of influenza A among high school students in Qom City, (Iran) (Persian)]. Qom University of Medical Sciences Journal. 2019; 13(4):22-33. [DOI:10.29252/qums.13.4.22]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2023/05/15 | Accepted: 2023/08/27 | Published: 2024/05/1
Received: 2023/05/15 | Accepted: 2023/08/27 | Published: 2024/05/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
