

Volume 14, Issue 5 (Sep & Oct 2024)
J Research Health 2024, 14(5): 479-488 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Oladi F, Saremi A A, Eshraghi A, Karbalaee M H. Effect of Emotionally Focused Couple Therapy on Affective Temperaments in Patients With Coronary Artery Disease. J Research Health 2024; 14 (5) :479-488
URL: http://jrh.gmu.ac.ir/article-1-2405-en.html
URL: http://jrh.gmu.ac.ir/article-1-2405-en.html



1- Department of Psychology, Torbat-e Jam Branch, Islamic Azad University, Torbat-e Jam, Iran.
2- Department of Psychology, Torbat-e Jam Branch, Islamic Azad University, Torbat-e Jam, Iran. ,saremi@iautj.ac.ir
3- Department of Cardiology, School of Medicine, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Psychology, Torbat-e Jam Branch, Islamic Azad University, Torbat-e Jam, Iran. ,
3- Department of Cardiology, School of Medicine, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
Keywords: Coronary artery disease (CAD), Emotionally focused couple therapy (EFCT), Affective temperaments
Full-Text [PDF 603 kb]
(838 Downloads)
| Abstract (HTML) (3366 Views)
Full-Text: (826 Views)
Introduction
Coronary artery disease (CAD) is a cardiovascular condition characterized by the narrowing and hardening of blood vessels, making it difficult to supply blood to the heart. The epidemiology of CAD disease is a common clinical syndrome of a global health priority, and the burden is increasing at an alarming rate worldwide [1]. The prevalence of CAD not only increases mortality, and morbidity and worsens the patient’s quality of life (QoL) but also puts a significant burden on the overall healthcare system. Novel risk factors include cholesterol levels, cigarette smoking, diabetes, obesity, and hypertension, which are the causative agents of CAD. Furthermore, the etiology of CAD is also a very complex process involving several interrelated etiological factors in its pathogenesis [2].
Traditional risk factors, such as smoking, high blood pressure, and high cholesterol do not fully explain the excess burden of cardiovascular diseases (CVD) in the population. Important psychological and social characteristics, including negative emotional states, depression or depressive symptoms, anger and hostility, anxiety, chronic psychosocial stressors, personality type, affective temperaments, occupation or work-related stress, acute life stress, social ties, social support, and social conflict, account for the majority of cardiovascular events, and they are causally related to CVD [3].
Various personality traits have been found to be associated with cardiovascular risk factors and diseases. High trait anxiety and hostility are linked to elevated pulse wave velocity [4], while in the Baltimore longitudinal study of aging, middle-aged adults with suppressed anger had elevated carotid arterial stiffness [5]. Anger, hostility, and anxiety are also documented risk factors for CAD [6, 7]. Moreover, anger and hostility also appear to predict a variety of cardiovascular outcomes [8, 9]. Temperament is regarded as an inherited aspect of personality and represents the biologically stable core of emotional reactivity [10].
Affective temperaments, which include depressive, cyclothymic, hyperthymic, irritable, and anxious dimensions, are subclinical, trait-related manifestations that are common antecedents of minor and major mood disorders [11]. Temperaments are important predictors of psychopathology and suicidal behavior and may be used for better delivery of appropriate care to patients with bipolar disorders in clinical practice [12]. Besides their associations with psychiatric disorders, affective temperaments were recently found to be related to cardiovascular risk factors and diseases as well. In chronic hypertensive patients, elevated blood pressure has been demonstrated to correlate with high cyclothymic temperament, as well as an increased level of arterial stiffening associated with low hyperthymic scores [13]. Furthermore, cyclothymic temperament has also been associated with coronary events in hypertensive patients [14].
Emotionally focused couple therapy (EFCT) identifies restricted interaction patterns and inappropriate emotional responses as the source of couples’ distress. EFCT is an effective couple’s therapy designed to change inappropriate emotional responses and existing patterns [15]. Utilizing humanistic and systemic principles, EFCT aims to create a more secure attachment pattern between couples [16]. Any of the couples may have rejected feelings and accompanying unmet needs. It is assumed that by expressing these needs in therapy, will become more securely attached. As couples become more accessible to each other, they become more sensitive to each other’s feelings and needs, resulting in new cycles of positive interaction while fostering trust [17]. One of the goals of EFCT is to promote the creation of secure bonds between couples, facilitating emotional connection and resilience in the face of difficulties. In light of this explanation, EFCT appears to be an effective therapeutic method for couples coping with the effects of a disease in their lives [18].
Despite the burgeoning evidence indicating that a couple’s healthy relationships are vital for reducing chronic disease incidence and management, the healing hearts together (HHT) program [19] was created to help both cardiac patients and their partners better manage cardiac disease by strengthening the emotional bond between them. The goals of HHT are to assist couples in improving their relationship quality, mental health, QoL, and cardiovascular health. The HHT couples-based intervention is adapted from the hold me tight (HMT): Conversations for connection (HMT) program [20], which is based on emotionally focused therapy (EFT) for couples and is an empirically supported treatment for relationship distress [16]. EFT, HMT, and HHT are based on attachment theory, which states that humans have an innate need for close emotional bonds with significant others [21]. This need becomes especially pertinent when faced with a threat or stress (e.g. a cardiac event). EFT interventions help couples identify and articulate their vulnerability (e.g. “I almost died/I almost lost you”) and respond to these feelings in comforting ways, thereby solidifying their sense of security and emotional connection [22]. Couples who achieve this connection are happier in their relationships and are more effective problem solvers (e.g. managing cardiovascular disease) [23]. Inspired by HMT, the HHT program guides couples through seven conversations based on EFT principles, in which they learn to clearly communicate their need for connection and reassurance, with a focus on heart disease and healthy coping [24].
Couples are responsible for managing the emotions and reactions of two individuals whose behaviors, thoughts, and experiential experiences are in constant interaction, which necessitates a detailed guide when planning their counseling sessions. Training in emotional control and management, especially for couples with CAD, is one of the principles of psychological care for these patients. HHT is a relationship education program for couples that aims to enhance couples’ relationship quality and mental and physical health. HHT seeks to foster emotional responsiveness and engagement between partners after one individual faces a cardiac event or procedure. Given that the effect of this method on affective temperament has not been examined, the purpose of this study is to test the efficacy of the 8-week HHT in improving affective temperaments. Thus, this study aimed to determine the effectiveness of EFCT based on the HHT on affective temperaments in patients with CAD.
Methods
Study design
This two-group semi-experimental study was conducted with a parallel pre-test-post-test-follow-up design in Mashhad in 2022. The research population consisted of patients aged 45 to 60 years old with CAD and their spouses who were referred to three cardiovascular treatment clinics in Mashhad City. First, they were selected through convenience sampling from 211 couples, one of whom was suffering from CAD. A sample size of 30 couples was obtained using G*Power software, version 3.1.9.4, with an effect size of at least 0.2 for the power test and a safety factor of 0.95. Considering a possible dropout rate of at least 10%, a total of 34 couples who were eligible to enter the study had an active care file and were subjected to the final analysis. The random assignment of the research sample to the two intervention and control groups was done based on permutation blocks, such that in each block of four, two allocations were assigned to the intervention group and two allocations were assigned to the control group.
Inclusion and exclusion criteria
The inclusion criteria of the study included having CAD in one of the spouses and not having a debilitating chronic disease, such as cancer, stroke, or chronic obstructive pulmonary disease, as determined by history and examination. A diagnosis of coronary heart disease was required based on the opinion of a cardiologist. Also, couples needed to demonstrate marital incompatibility, as indicated by a score of less than or equal to 47 on the revised Dyadic adjustment questionnaire (RDAS) [25], and also through a clinical interview. Other criteria included having received at least two injections of the COVID-19 vaccine, with a minimum of two weeks having passed since the last vaccination, and each spouse having a secondary or higher level of literacy. Furthermore, at least one year must have passed since the diagnosis of coronary heart disease in one of the patient’s spouses. The exclusion criteria included unwillingness to continue cooperation, absence from more than two sessions in couple therapy sessions, hospitalization during the research period, and incomplete questionnaires.
Research tools
Demographic characteristics questionnaire
This questionnaire included questions about gender, age, education, employment status, and the duration of the patient’s CAD. It was prepared in order to determine the demographic characteristics and to check the inclusion and exclusion criteria, as well as to control variables.
Temperament evaluation of Memphis, Pisa, Paris, and San Diego autoquestionnaire (TEMPS-A)
Affective temperaments were assessed using the TEMPS-A, a self-administered, Likert-type scale consisting of 110 items that measure five subscales, including depressive, cyclothymic, hyperthymic, irritable, and anxious temperaments. This questionnaire has 110 items across five dimensions. For each temperament, there are two possible answers: “Yes” and “no.” A score of 1 is assigned for a “yes” answer, while a score of 0 is assigned for a “no” answer. To obtain the score for each dimension, the scores of the related items are summed and then divided by the number of items for that temperament, resulting in a score between 0 and 1 for each dimension [26].
TEMPS-A has been extensively studied, translated into more than 30 languages, and validated in several of those languages. Similarities and differences have also been found in national samples, suggesting that the distribution of affective temperaments has both universal and cultural-specific characteristics [27]. The reliability of the questionnaire’s dimensions, measured using Cronbach’s α method, ranged from 0.67 to 0.91, while the internal consistency ranged from 0.77 to 0.85 [28]. Psychometric analysis was performed by Khalili et al. in Iran in 2018 [29].
Procedures
For the couples participating in the research, explanations were given about the study, its objectives, and how to conduct it, along with assurances regarding the confidentiality of the information written informed consent was obtained from all participants. First, the demographic questionnaire and the TEMPS-A were completed by the couples. The therapeutic training package, which consisted of an EFCT based on the HHT, was implemented for the intervention group in eight sessions of 120 minutes each, conducted in a group learning format, with one session per week. The treatment and training were done by a PhD student in health psychology who had a specialized certificate in EFCT and has more than five years of experience in counseling and emotional-oriented couple therapy, under the supervision of the program supervisor. It should be mentioned that the HHT educational model was also translated and printed by the researcher with the permission of the author of the book. The educational package included a manual, worksheets, session exercises, homework, a DVD of Dr. Johnson’s emotional therapy couple movie, and a film featuring a couple suffering from cardiovascular disease [19, 30], a portion of the movie was played for the couples in the intervention group during each session, after which the couples expressed their opinions about the movie and engaged in discussion. For the couples in the control group, no intervention was done; however, in terms of compliance with ethical principles, a training booklet summarizing the topics taught to the intervention group was distributed during the follow-up session after completing the questionnaires. The intervention was conducted with the couples in the control group, and the contact number of the researcher was given to the control group for any questions. They were also thanked and appreciated for their cooperation.
The content of the EFCT based on HHT was as follows:
Session 1: Introduction to the HHT program, understanding love and attachment, and their relationship to heart health.
Session 2: Voice of patients and partners; providing an opportunity to share experiences related to cardiovascular disease with partners and peers.
Session 3: Conversation 1; recognizing demon dialogues and interactional cycles of couples in relationships affected by heart disease.
Session 4: Conversation 2; finding the raw spots in demon dialogues, with an explanation of the irritations and vulnerable points associated with chronic diseases such as heart disease.
Session 5: Conversation 3; HMT, investigating spouses’ reactions to heart disease and how it has awakened fundamental fears in them
Session 6: Conversation 4; forgiving injuries, focusing on forgiveness of resentments in a couple’s relationship and rebuilding trust.
Session 7: Conversation 5; bonding through Sex and Touch, discussing the effect of heart disease on the couples’ sexual relationship and addressing anxieties and expectations related to their sexual life.
Session 8: Conversation 6; keeping your love alive and caring for your relationship, writing a couple’s love story for the future about how their relationship will evolve over the next 5 or 10 years.
Statistical analysis
Data were analyzed using SPSS software, version 26, employing the chi-square test, independent t-test, repeated measures ANOVA, and Bonferroni post hoc test at the significance level of 0.05.
Results
In this study, 34 couples, including 16 couples in the intervention group and 18 couples in the control group, were subjected to final examination. In each group, 50% were men and 50% were women. The mean age of patients in the intervention group was 51.68±4.90 years, and the duration of CAD was 4.18±3.03 years. In the control group, the mean age was 52±4.17 years and the duration of CAD was 4.77±5.24 years. The majority of patients in both groups had a diploma and government jobs. The two groups were homogeneous in terms of age, education, gender, occupation, and duration of CAD, and there was no significant statistical difference between the two groups in terms of demographic variables (P>0.05).
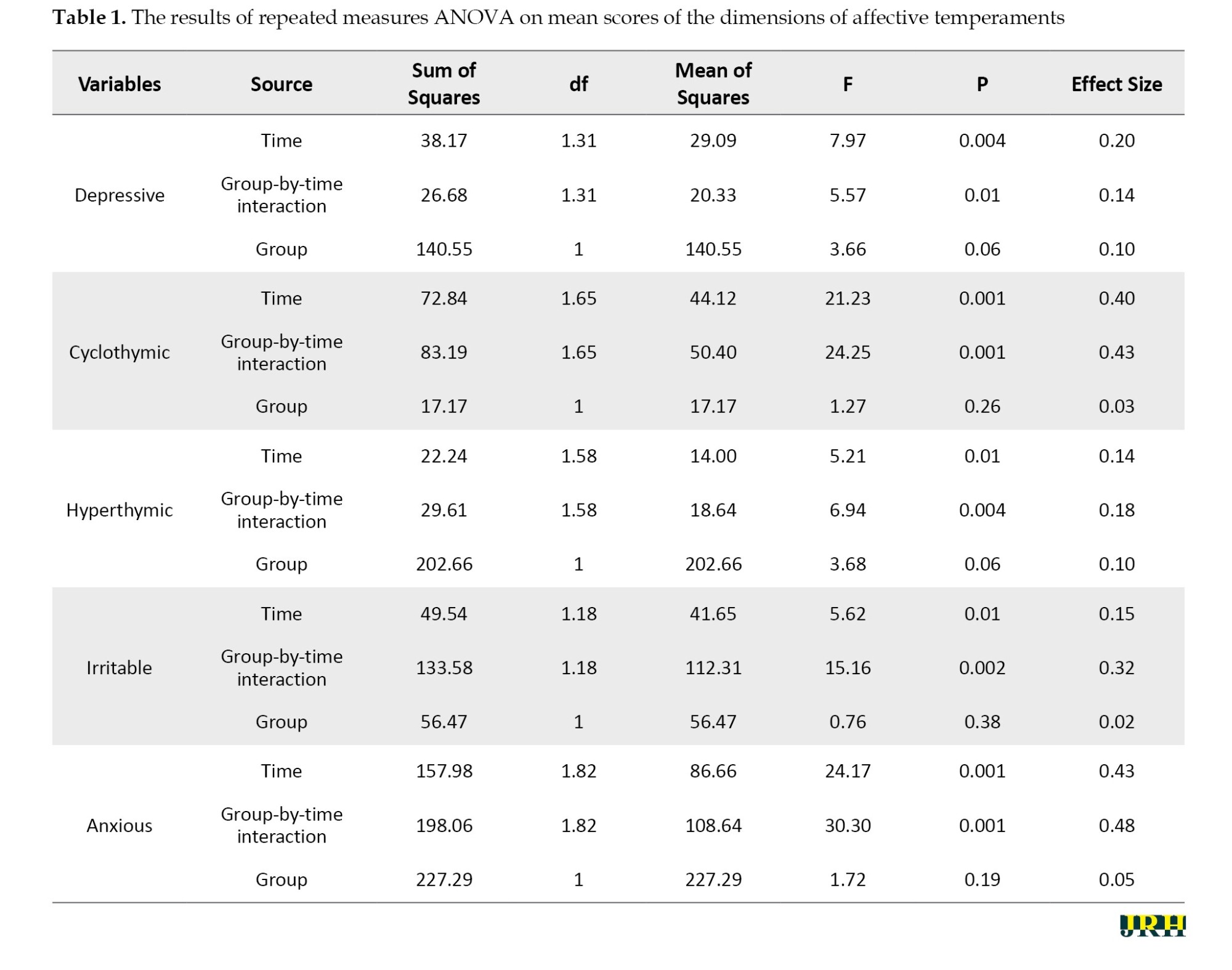
To assess the assumption of normality, skewness and kurtosis indicators were used to investigate the normality of the research variables. The skewness and kurtosis of the research variables were no higher than 2 and -2, respectively, indicating that the normality of the research variables was confirmed. The second assumption was the equality of variances of the research variables. The Levene’s test was used to investigate this assumption. The non-significant results of this test indicated that this assumption was upheld. According to the results of repeated measures ANOVA, significant effects were found in all dimensions of affective temperaments, including the effect of time and the group-by-time interaction effect (P<0.05). This means that there was a significant difference in these variables from the pre-test stage to the follow-up (time effect), indicating different performances of the groups during the pre-test, post-test, and follow-up stages (group-by-time interaction effect). However, the results showed that the group effect was not significant in all dimensions (P>0.05). The results of the effect size index also showed small to medium effects for significant variables (Table 1).
Based on the results of Bonferroni post hoc test, the comparison of the two intervention and control groups in terms of affective temperament scores during the study process showed that there was no significant difference between the intervention and control groups in the pre-test (P>0.05). However, in the post-test and follow-up, with the exception of the cyclothymic dimension, there was a significant difference between the differential scores of the intervention and control groups in the other dimensions of affective temperaments (P<0.05). This indicates that participants in the intervention group demonstrated less depression, irritability, and anxiety, and they also experienced more hyperthymia compared to the control group in the post-test and follow-up phases (Table 2).

Discussion
The results of the study showed that in the pre-test, there was no significant difference between the scores of affective temperaments and their various dimensions in the intervention and control groups. However, in the post-test and follow-up (except for the cyclothymic affective temperament), there was a significant difference between the scores of the patients in the intervention and control groups in the dimensions of affective temperaments. This means that the patients of the intervention group showed lower scores in the dimensions of depression, irritability, and anxiety in the post-test and follow-up phase compared to the control group. Also, they obtained a higher score in the dimension of hyperthymic compared to the control group. According to the results obtained, the HHT-based EFCT plays a role in the affective temperaments of CAD patients.
The results of this study are consistent with those of a previous study on the relationship between the dimensions of affective temperaments and the severity of CAD. The researchers concluded that elevated hyperthymic affective temperament scores significantly decreased the severity of CAD, while independent positive associations were observed in cases of dyslipidemia and cyclothymic affective temperament scores. However, their study was correlational, examining the correlation between affective temperament and the severity of CAD. Patients with severe coronary artery stenosis had higher scores in the dimensions of affective temperaments, including depressive, cyclothymic, irritability, and anxious compared to patients with mild coronary artery stenosis. It was stated that hyperthymic affective temperament is a protective factor in preventing more severe coronary artery stenosis. They also concluded that the hyperthymic affective temperament significantly reduces the probability of severe CAD, while irritable and cyclothymic affective temperaments have a positive and independent relationship with the disturbances in blood lipids and the severity of CAD [31].
Also, the results of this study are in agreement with those of a descriptive study that examined 200 individuals using coronary computed tomography angiography (CCTA). The hyperthymic affective temperament score was higher in CCTA-negative subjects compared to CCTA-positive subjects. In terms of the type of affective temperament in CAD patients, there is a consistency with the results of the present study, although no intervention was conducted. The hyperthymic affective temperament score showed a significant independent, inverse relationship with coronary atherosclerosis. Our results suggest that hyperthymic affective temperament is independently associated with the absence of CAD. Further research is needed to delineate the mechanisms mediating the effect of hyperthymia on better coronary artery health and to establish potential biochemical or behavioral factors that could be exploited for prevention and treatment purposes. It is plausible that the evaluation of affective temperaments is important in relation to both psychiatric and cardiovascular disorders [32].
In another study, the results indicated that a dominant cyclothymic affective temperament may be an additional risk factor for cardiovascular morbidity. This finding suggests that further assessment may be warranted to identify at-risk patients and formulate a more individualized treatment approach; however, no intervention was made to examine its impact on affective temperaments [33]. Our study showed that it is possible to adjust the affective temperament dimensions of patients with CAD through proper training.
In another study, the moderating role of affective temperaments in the relationship between biomarkers (troponin, white blood cell count, and neutrophil-to-lymphocyte ratio) and the severity of CAD was determined. Based on the findings of this study, affective temperaments affect the relationship between biomarkers and the severity of CAD. Therefore, as a psychological factor, they could play an important role in preventing CAD and reducing mortality rates and annual costs associated with this disease. Although there was no intervention in this study, it highlights the role of affective temperaments as a risk factor for CAD, indicating the need for psychological interventions [34].
Along with the physical risk factors of heart disease, such as age, gender, body mass index, smoking, inactivity, and diabetes, psychological risk factors should also be considered. Personality traits are related to heart disease risk factors, with high levels of anxiety and hostility predicting an increased risk of heart disease. Suppressed anger can lead to increased vasoconstriction. Anger, hostility, and anxiety are risk factors for heart disease. Each person’s reaction to stressful situations is unique. Affective temperaments are considered an inherited aspect of the personality and represent the stable biological core of emotional reactivity. Depressive, cyclothymic, irritable, and anxious affective temperaments are subclinical manifestations that serve as a background for minor and major mood disorders [32].
One of the strengths of the present study is the high cooperation from patients in all stages of the research. Long-term follow-up was not possible due to operational limitations and difficulties in re-accessing the participants. Since the data collection tool used in this research is a self-report questionnaire, it is possible that the responses may not be sufficiently accurate in some cases. Another limitation is that no intervention was conducted for the control group as a placebo to neutralize the effects of therapy; this group only received the physician’s advice. Implementing suitable psychological interventions to solve emotional and communication problems between couples can play an important role in controlling and coping with CAD. It is also recommended to conduct cohort studies with repeated psychological interventions to determine their effectiveness in patients with CAD and compare different interventions and identify effective strategies based on social, cultural, and geographical conditions. Considering the significant role of the spouse in addition to medical treatments, it is suggested to establish EFCT based on the educational model of HHT for couples where one partner is suffering from heart disease. These interventions may help improve the effectiveness of medical treatments, reduce the psychological risk factors associated with CVD, enhance the QoL, and increase the life expectancy of heart patients.
Conclusion
Based on the results of this research, EFCT (based on the educational model of HHT) increased the scores of the hyperthymic dimension and decreased the scores of the irritability, anxious, and depressive dimensions of affective temperaments in CAD patients. This therapy helps couples resolve conflicts and manage negative emotions that can adversely affect the health of patients with CAD, thereby improving their affective temperaments. Attention to psychological interventions, such as EFCT in couples, where one partner has CAD, can be effective in maintaining and promoting health as well as enhancing the QoL for these patients. The support of a partner can provide the patient with greater motivation for treatment, leading to increased marital satisfaction. Therefore, paying attention to mental health and psychological assessments, such as EFCT for patients with CAD alongside therapeutic interventions by cardiologists, can promote better health outcomes for these patients.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Torbat-e Jam Branch (Code: IR.IAU.TJ.REC.1401.034) and informed consent was obtained from every participant.
Funding
The present study was extracted from the PhD dissertation of Fereshteh Oladi, approved by the Department of Psychology, Islamic Azad University, Torbat-e Jam Branch, Torbat-e Jam, Iran.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to express their gratitude to the esteemed cardiologists, the couples involved, and all others who assisted them in this research project.
References
Coronary artery disease (CAD) is a cardiovascular condition characterized by the narrowing and hardening of blood vessels, making it difficult to supply blood to the heart. The epidemiology of CAD disease is a common clinical syndrome of a global health priority, and the burden is increasing at an alarming rate worldwide [1]. The prevalence of CAD not only increases mortality, and morbidity and worsens the patient’s quality of life (QoL) but also puts a significant burden on the overall healthcare system. Novel risk factors include cholesterol levels, cigarette smoking, diabetes, obesity, and hypertension, which are the causative agents of CAD. Furthermore, the etiology of CAD is also a very complex process involving several interrelated etiological factors in its pathogenesis [2].
Traditional risk factors, such as smoking, high blood pressure, and high cholesterol do not fully explain the excess burden of cardiovascular diseases (CVD) in the population. Important psychological and social characteristics, including negative emotional states, depression or depressive symptoms, anger and hostility, anxiety, chronic psychosocial stressors, personality type, affective temperaments, occupation or work-related stress, acute life stress, social ties, social support, and social conflict, account for the majority of cardiovascular events, and they are causally related to CVD [3].
Various personality traits have been found to be associated with cardiovascular risk factors and diseases. High trait anxiety and hostility are linked to elevated pulse wave velocity [4], while in the Baltimore longitudinal study of aging, middle-aged adults with suppressed anger had elevated carotid arterial stiffness [5]. Anger, hostility, and anxiety are also documented risk factors for CAD [6, 7]. Moreover, anger and hostility also appear to predict a variety of cardiovascular outcomes [8, 9]. Temperament is regarded as an inherited aspect of personality and represents the biologically stable core of emotional reactivity [10].
Affective temperaments, which include depressive, cyclothymic, hyperthymic, irritable, and anxious dimensions, are subclinical, trait-related manifestations that are common antecedents of minor and major mood disorders [11]. Temperaments are important predictors of psychopathology and suicidal behavior and may be used for better delivery of appropriate care to patients with bipolar disorders in clinical practice [12]. Besides their associations with psychiatric disorders, affective temperaments were recently found to be related to cardiovascular risk factors and diseases as well. In chronic hypertensive patients, elevated blood pressure has been demonstrated to correlate with high cyclothymic temperament, as well as an increased level of arterial stiffening associated with low hyperthymic scores [13]. Furthermore, cyclothymic temperament has also been associated with coronary events in hypertensive patients [14].
Emotionally focused couple therapy (EFCT) identifies restricted interaction patterns and inappropriate emotional responses as the source of couples’ distress. EFCT is an effective couple’s therapy designed to change inappropriate emotional responses and existing patterns [15]. Utilizing humanistic and systemic principles, EFCT aims to create a more secure attachment pattern between couples [16]. Any of the couples may have rejected feelings and accompanying unmet needs. It is assumed that by expressing these needs in therapy, will become more securely attached. As couples become more accessible to each other, they become more sensitive to each other’s feelings and needs, resulting in new cycles of positive interaction while fostering trust [17]. One of the goals of EFCT is to promote the creation of secure bonds between couples, facilitating emotional connection and resilience in the face of difficulties. In light of this explanation, EFCT appears to be an effective therapeutic method for couples coping with the effects of a disease in their lives [18].
Despite the burgeoning evidence indicating that a couple’s healthy relationships are vital for reducing chronic disease incidence and management, the healing hearts together (HHT) program [19] was created to help both cardiac patients and their partners better manage cardiac disease by strengthening the emotional bond between them. The goals of HHT are to assist couples in improving their relationship quality, mental health, QoL, and cardiovascular health. The HHT couples-based intervention is adapted from the hold me tight (HMT): Conversations for connection (HMT) program [20], which is based on emotionally focused therapy (EFT) for couples and is an empirically supported treatment for relationship distress [16]. EFT, HMT, and HHT are based on attachment theory, which states that humans have an innate need for close emotional bonds with significant others [21]. This need becomes especially pertinent when faced with a threat or stress (e.g. a cardiac event). EFT interventions help couples identify and articulate their vulnerability (e.g. “I almost died/I almost lost you”) and respond to these feelings in comforting ways, thereby solidifying their sense of security and emotional connection [22]. Couples who achieve this connection are happier in their relationships and are more effective problem solvers (e.g. managing cardiovascular disease) [23]. Inspired by HMT, the HHT program guides couples through seven conversations based on EFT principles, in which they learn to clearly communicate their need for connection and reassurance, with a focus on heart disease and healthy coping [24].
Couples are responsible for managing the emotions and reactions of two individuals whose behaviors, thoughts, and experiential experiences are in constant interaction, which necessitates a detailed guide when planning their counseling sessions. Training in emotional control and management, especially for couples with CAD, is one of the principles of psychological care for these patients. HHT is a relationship education program for couples that aims to enhance couples’ relationship quality and mental and physical health. HHT seeks to foster emotional responsiveness and engagement between partners after one individual faces a cardiac event or procedure. Given that the effect of this method on affective temperament has not been examined, the purpose of this study is to test the efficacy of the 8-week HHT in improving affective temperaments. Thus, this study aimed to determine the effectiveness of EFCT based on the HHT on affective temperaments in patients with CAD.
Methods
Study design
This two-group semi-experimental study was conducted with a parallel pre-test-post-test-follow-up design in Mashhad in 2022. The research population consisted of patients aged 45 to 60 years old with CAD and their spouses who were referred to three cardiovascular treatment clinics in Mashhad City. First, they were selected through convenience sampling from 211 couples, one of whom was suffering from CAD. A sample size of 30 couples was obtained using G*Power software, version 3.1.9.4, with an effect size of at least 0.2 for the power test and a safety factor of 0.95. Considering a possible dropout rate of at least 10%, a total of 34 couples who were eligible to enter the study had an active care file and were subjected to the final analysis. The random assignment of the research sample to the two intervention and control groups was done based on permutation blocks, such that in each block of four, two allocations were assigned to the intervention group and two allocations were assigned to the control group.
Inclusion and exclusion criteria
The inclusion criteria of the study included having CAD in one of the spouses and not having a debilitating chronic disease, such as cancer, stroke, or chronic obstructive pulmonary disease, as determined by history and examination. A diagnosis of coronary heart disease was required based on the opinion of a cardiologist. Also, couples needed to demonstrate marital incompatibility, as indicated by a score of less than or equal to 47 on the revised Dyadic adjustment questionnaire (RDAS) [25], and also through a clinical interview. Other criteria included having received at least two injections of the COVID-19 vaccine, with a minimum of two weeks having passed since the last vaccination, and each spouse having a secondary or higher level of literacy. Furthermore, at least one year must have passed since the diagnosis of coronary heart disease in one of the patient’s spouses. The exclusion criteria included unwillingness to continue cooperation, absence from more than two sessions in couple therapy sessions, hospitalization during the research period, and incomplete questionnaires.
Research tools
Demographic characteristics questionnaire
This questionnaire included questions about gender, age, education, employment status, and the duration of the patient’s CAD. It was prepared in order to determine the demographic characteristics and to check the inclusion and exclusion criteria, as well as to control variables.
Temperament evaluation of Memphis, Pisa, Paris, and San Diego autoquestionnaire (TEMPS-A)
Affective temperaments were assessed using the TEMPS-A, a self-administered, Likert-type scale consisting of 110 items that measure five subscales, including depressive, cyclothymic, hyperthymic, irritable, and anxious temperaments. This questionnaire has 110 items across five dimensions. For each temperament, there are two possible answers: “Yes” and “no.” A score of 1 is assigned for a “yes” answer, while a score of 0 is assigned for a “no” answer. To obtain the score for each dimension, the scores of the related items are summed and then divided by the number of items for that temperament, resulting in a score between 0 and 1 for each dimension [26].
TEMPS-A has been extensively studied, translated into more than 30 languages, and validated in several of those languages. Similarities and differences have also been found in national samples, suggesting that the distribution of affective temperaments has both universal and cultural-specific characteristics [27]. The reliability of the questionnaire’s dimensions, measured using Cronbach’s α method, ranged from 0.67 to 0.91, while the internal consistency ranged from 0.77 to 0.85 [28]. Psychometric analysis was performed by Khalili et al. in Iran in 2018 [29].
Procedures
For the couples participating in the research, explanations were given about the study, its objectives, and how to conduct it, along with assurances regarding the confidentiality of the information written informed consent was obtained from all participants. First, the demographic questionnaire and the TEMPS-A were completed by the couples. The therapeutic training package, which consisted of an EFCT based on the HHT, was implemented for the intervention group in eight sessions of 120 minutes each, conducted in a group learning format, with one session per week. The treatment and training were done by a PhD student in health psychology who had a specialized certificate in EFCT and has more than five years of experience in counseling and emotional-oriented couple therapy, under the supervision of the program supervisor. It should be mentioned that the HHT educational model was also translated and printed by the researcher with the permission of the author of the book. The educational package included a manual, worksheets, session exercises, homework, a DVD of Dr. Johnson’s emotional therapy couple movie, and a film featuring a couple suffering from cardiovascular disease [19, 30], a portion of the movie was played for the couples in the intervention group during each session, after which the couples expressed their opinions about the movie and engaged in discussion. For the couples in the control group, no intervention was done; however, in terms of compliance with ethical principles, a training booklet summarizing the topics taught to the intervention group was distributed during the follow-up session after completing the questionnaires. The intervention was conducted with the couples in the control group, and the contact number of the researcher was given to the control group for any questions. They were also thanked and appreciated for their cooperation.
The content of the EFCT based on HHT was as follows:
Session 1: Introduction to the HHT program, understanding love and attachment, and their relationship to heart health.
Session 2: Voice of patients and partners; providing an opportunity to share experiences related to cardiovascular disease with partners and peers.
Session 3: Conversation 1; recognizing demon dialogues and interactional cycles of couples in relationships affected by heart disease.
Session 4: Conversation 2; finding the raw spots in demon dialogues, with an explanation of the irritations and vulnerable points associated with chronic diseases such as heart disease.
Session 5: Conversation 3; HMT, investigating spouses’ reactions to heart disease and how it has awakened fundamental fears in them
Session 6: Conversation 4; forgiving injuries, focusing on forgiveness of resentments in a couple’s relationship and rebuilding trust.
Session 7: Conversation 5; bonding through Sex and Touch, discussing the effect of heart disease on the couples’ sexual relationship and addressing anxieties and expectations related to their sexual life.
Session 8: Conversation 6; keeping your love alive and caring for your relationship, writing a couple’s love story for the future about how their relationship will evolve over the next 5 or 10 years.
Statistical analysis
Data were analyzed using SPSS software, version 26, employing the chi-square test, independent t-test, repeated measures ANOVA, and Bonferroni post hoc test at the significance level of 0.05.
Results
In this study, 34 couples, including 16 couples in the intervention group and 18 couples in the control group, were subjected to final examination. In each group, 50% were men and 50% were women. The mean age of patients in the intervention group was 51.68±4.90 years, and the duration of CAD was 4.18±3.03 years. In the control group, the mean age was 52±4.17 years and the duration of CAD was 4.77±5.24 years. The majority of patients in both groups had a diploma and government jobs. The two groups were homogeneous in terms of age, education, gender, occupation, and duration of CAD, and there was no significant statistical difference between the two groups in terms of demographic variables (P>0.05).
To assess the assumption of normality, skewness and kurtosis indicators were used to investigate the normality of the research variables. The skewness and kurtosis of the research variables were no higher than 2 and -2, respectively, indicating that the normality of the research variables was confirmed. The second assumption was the equality of variances of the research variables. The Levene’s test was used to investigate this assumption. The non-significant results of this test indicated that this assumption was upheld. According to the results of repeated measures ANOVA, significant effects were found in all dimensions of affective temperaments, including the effect of time and the group-by-time interaction effect (P<0.05). This means that there was a significant difference in these variables from the pre-test stage to the follow-up (time effect), indicating different performances of the groups during the pre-test, post-test, and follow-up stages (group-by-time interaction effect). However, the results showed that the group effect was not significant in all dimensions (P>0.05). The results of the effect size index also showed small to medium effects for significant variables (Table 1).
Based on the results of Bonferroni post hoc test, the comparison of the two intervention and control groups in terms of affective temperament scores during the study process showed that there was no significant difference between the intervention and control groups in the pre-test (P>0.05). However, in the post-test and follow-up, with the exception of the cyclothymic dimension, there was a significant difference between the differential scores of the intervention and control groups in the other dimensions of affective temperaments (P<0.05). This indicates that participants in the intervention group demonstrated less depression, irritability, and anxiety, and they also experienced more hyperthymia compared to the control group in the post-test and follow-up phases (Table 2).
Discussion
The results of the study showed that in the pre-test, there was no significant difference between the scores of affective temperaments and their various dimensions in the intervention and control groups. However, in the post-test and follow-up (except for the cyclothymic affective temperament), there was a significant difference between the scores of the patients in the intervention and control groups in the dimensions of affective temperaments. This means that the patients of the intervention group showed lower scores in the dimensions of depression, irritability, and anxiety in the post-test and follow-up phase compared to the control group. Also, they obtained a higher score in the dimension of hyperthymic compared to the control group. According to the results obtained, the HHT-based EFCT plays a role in the affective temperaments of CAD patients.
The results of this study are consistent with those of a previous study on the relationship between the dimensions of affective temperaments and the severity of CAD. The researchers concluded that elevated hyperthymic affective temperament scores significantly decreased the severity of CAD, while independent positive associations were observed in cases of dyslipidemia and cyclothymic affective temperament scores. However, their study was correlational, examining the correlation between affective temperament and the severity of CAD. Patients with severe coronary artery stenosis had higher scores in the dimensions of affective temperaments, including depressive, cyclothymic, irritability, and anxious compared to patients with mild coronary artery stenosis. It was stated that hyperthymic affective temperament is a protective factor in preventing more severe coronary artery stenosis. They also concluded that the hyperthymic affective temperament significantly reduces the probability of severe CAD, while irritable and cyclothymic affective temperaments have a positive and independent relationship with the disturbances in blood lipids and the severity of CAD [31].
Also, the results of this study are in agreement with those of a descriptive study that examined 200 individuals using coronary computed tomography angiography (CCTA). The hyperthymic affective temperament score was higher in CCTA-negative subjects compared to CCTA-positive subjects. In terms of the type of affective temperament in CAD patients, there is a consistency with the results of the present study, although no intervention was conducted. The hyperthymic affective temperament score showed a significant independent, inverse relationship with coronary atherosclerosis. Our results suggest that hyperthymic affective temperament is independently associated with the absence of CAD. Further research is needed to delineate the mechanisms mediating the effect of hyperthymia on better coronary artery health and to establish potential biochemical or behavioral factors that could be exploited for prevention and treatment purposes. It is plausible that the evaluation of affective temperaments is important in relation to both psychiatric and cardiovascular disorders [32].
In another study, the results indicated that a dominant cyclothymic affective temperament may be an additional risk factor for cardiovascular morbidity. This finding suggests that further assessment may be warranted to identify at-risk patients and formulate a more individualized treatment approach; however, no intervention was made to examine its impact on affective temperaments [33]. Our study showed that it is possible to adjust the affective temperament dimensions of patients with CAD through proper training.
In another study, the moderating role of affective temperaments in the relationship between biomarkers (troponin, white blood cell count, and neutrophil-to-lymphocyte ratio) and the severity of CAD was determined. Based on the findings of this study, affective temperaments affect the relationship between biomarkers and the severity of CAD. Therefore, as a psychological factor, they could play an important role in preventing CAD and reducing mortality rates and annual costs associated with this disease. Although there was no intervention in this study, it highlights the role of affective temperaments as a risk factor for CAD, indicating the need for psychological interventions [34].
Along with the physical risk factors of heart disease, such as age, gender, body mass index, smoking, inactivity, and diabetes, psychological risk factors should also be considered. Personality traits are related to heart disease risk factors, with high levels of anxiety and hostility predicting an increased risk of heart disease. Suppressed anger can lead to increased vasoconstriction. Anger, hostility, and anxiety are risk factors for heart disease. Each person’s reaction to stressful situations is unique. Affective temperaments are considered an inherited aspect of the personality and represent the stable biological core of emotional reactivity. Depressive, cyclothymic, irritable, and anxious affective temperaments are subclinical manifestations that serve as a background for minor and major mood disorders [32].
One of the strengths of the present study is the high cooperation from patients in all stages of the research. Long-term follow-up was not possible due to operational limitations and difficulties in re-accessing the participants. Since the data collection tool used in this research is a self-report questionnaire, it is possible that the responses may not be sufficiently accurate in some cases. Another limitation is that no intervention was conducted for the control group as a placebo to neutralize the effects of therapy; this group only received the physician’s advice. Implementing suitable psychological interventions to solve emotional and communication problems between couples can play an important role in controlling and coping with CAD. It is also recommended to conduct cohort studies with repeated psychological interventions to determine their effectiveness in patients with CAD and compare different interventions and identify effective strategies based on social, cultural, and geographical conditions. Considering the significant role of the spouse in addition to medical treatments, it is suggested to establish EFCT based on the educational model of HHT for couples where one partner is suffering from heart disease. These interventions may help improve the effectiveness of medical treatments, reduce the psychological risk factors associated with CVD, enhance the QoL, and increase the life expectancy of heart patients.
Conclusion
Based on the results of this research, EFCT (based on the educational model of HHT) increased the scores of the hyperthymic dimension and decreased the scores of the irritability, anxious, and depressive dimensions of affective temperaments in CAD patients. This therapy helps couples resolve conflicts and manage negative emotions that can adversely affect the health of patients with CAD, thereby improving their affective temperaments. Attention to psychological interventions, such as EFCT in couples, where one partner has CAD, can be effective in maintaining and promoting health as well as enhancing the QoL for these patients. The support of a partner can provide the patient with greater motivation for treatment, leading to increased marital satisfaction. Therefore, paying attention to mental health and psychological assessments, such as EFCT for patients with CAD alongside therapeutic interventions by cardiologists, can promote better health outcomes for these patients.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Torbat-e Jam Branch (Code: IR.IAU.TJ.REC.1401.034) and informed consent was obtained from every participant.
Funding
The present study was extracted from the PhD dissertation of Fereshteh Oladi, approved by the Department of Psychology, Islamic Azad University, Torbat-e Jam Branch, Torbat-e Jam, Iran.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to express their gratitude to the esteemed cardiologists, the couples involved, and all others who assisted them in this research project.
References
- Ullah M, Wahab A, Khan SU, Zaman U, Rehman KU, Hamayun S, et al. Stent as a novel technology for coronary artery disease and their clinical manifestation. Current Problems in Cardiology. 2023; 48(1):101415. [DOI:10.1016/j.cpcardiol.2022.101415] [PMID]
- Barrett-Connor E. Gender differences and disparities in all-cause and coronary heart disease mortality: Epidemiological aspects. Best Practice & Research. 2013; 27(4):481-500. [DOI:10.1016/j.beem.2013.05.013] [PMID] [PMCID]
- Okereke OI, Manson JE. Psychosocial factors and cardiovascular disease risk: An opportunity in women's health. Circulation Research. 2017; 120(12):1855-6. [DOI:10.1161/CIRCRESAHA.117.311113] [PMID] [PMCID]
- Midei AJ, Matthews KA. Social relationships and negative emotional traits are associated with central adiposity and arterial stiffness in healthy adolescents. Health Psychology. 2009; 28(3):347-53. [DOI:10.1037/a0014214] [PMID] [PMCID]
- Dasa O, Mahmoud AN, Kaufmann PG, Ketterer M, Light KC, Raczynski J, et al. Relationship of psychological characteristics to daily life ischemia: An analysis from the national heart, lung, and blood institute psychophysiological investigations in myocardial ischemia. Psychosomatic Medicine. 2022; 84(3):359-67. [DOI:10.1097/PSY.0000000000001044] [PMID] [PMCID]
- Pejtersen JH, Burr H, Hannerz H, Fishta A, Hurwitz Eller N. Update on work-related psychosocial factors and the development of ischemic heart disease: A systematic review. Cardiology in Review. 2015; 23(2):94-8. [DOI:10.1097/CRD.0000000000000033] [PMID]
- Suls J. Toxic affect: Are anger, anxiety, and depression independent risk factors for cardiovascular disease? Emotion Review. 2018; 10(1):6-17. [DOI:10.1177/1754073917692863]
- Williams JE, Nieto FJ, Sanford CP, Couper DJ, Tyroler HA. The association between trait anger and incident stroke risk: The atherosclerosis risk in communities (ARIC) study. Stroke. 2002; 33(1):13-9. [DOI:10.1161/hs0102.101625] [PMID]
- Chida Y, Steptoe A. The association of anger and hostility with future coronary heart disease: A meta-analytic review of prospective evidence. Journal of the American College of Cardiology. 2009; 53(11):936-46. [DOI:10.1016/j.jacc.2008.11.044] [PMID]
- Hirsh JB. Environmental sustainability and national personality. Journal of Environmental Psychology. 2014; 38:233-40. [DOI:10.1016/j.jenvp.2014.02.005]
- Moccia L, Janiri D, Pepe M, Dattoli L, Molinaro M, De Martin V, et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain, Behavior, and Immunity. 2020; 87:75-79. [DOI:10.1016/j.bbi.2020.04.048] [PMID] [PMCID]
- Pompili M, Rihmer Z, Akiskal H, Amore M, Gonda X, Innamorati M, et al. Temperaments mediate suicide risk and psychopathology among patients with bipolar disorders. Comprehensive Psychiatry. 2012; 53(3):280-5. [DOI:10.1016/j.comppsych.2011.04.004] [PMID]
- László A, Tabák Á, Kőrösi B, Eörsi D, Torzsa P, Cseprekál O, et al. Association of affective temperaments with blood pressure and arterial stiffness in hypertensive patients: A cross-sectional study. BMC Cardiovascular Disorders. 2016; 16(1):158. [DOI:10.1186/s12872-016-0337-9] [PMID] [PMCID]
- Eory A, Rozsa S, Torzsa P, Kalabay L, Gonda X, Rihmer Z. Affective temperaments contribute to cardiac complications in hypertension independently of depression. Psychotherapy and Psychosomatics. 2014; 83(3):187-9. [DOI:10.1159/000357364] [PMID]
- Bodenmann G, Kessler M, Kuhn R, Hocker L, Randall AK. Cognitive-behavioral and emotion-focused couple therapy: Similarities and differences. Clinical Psychology in Europe. 2020; 2(3):e2741. [DOI:10.32872/cpe.v2i3.2741] [PMID] [PMCID]
- Wiebe SA, Johnson SM. A review of the research in emotionally focused therapy for couples. Family Process. 2016; 55(3):390-407. [DOI:10.1111/famp.12229] [PMID]
- Johnson SM. Emotionally focused couple therapy. In: Gurman AS, editor. Clinical handbook of couple therapy. New York: The Guilford Press; 2008. [Link]
- Şenol A, Gürbüz F, Tuzgöl Dost M. Emotion-focused couple therapy: A review of theory and practice. Current Approaches in Psychiatry. 2023; 15(1):146-60. [DOI:10.18863/pgy.1090793]
- Tulloch H, Greenman P, Demidenko N, Johnson SM. Healing hearts together relationship education program: Facilitator’s guide for small groups. Ottawa: International Centre for Excellence in Emotionally Focused Therapy; 2017.
- Johnson SM. The facilitator's guide for the hold me tight program: Conversations for connection. Ottawa: International Centre for Excellence in Emotionally Focused Therapy; 2010.
- Ross EA. Social control: A survey of the foundations of order. New York: Routledge; 2017. [DOI:10.4324/9781315129488]
- Conradi HJ, Dingemanse P, Noordhof A, Finkenauer C, Kamphuis JH. Effectiveness of the 'hold me tight' relationship enhancement program in a self-referred and a clinician-referred sample: An emotionally focused couples therapy-based approach. Family Process. 2018; 57(3):613-28. [DOI:10.1111/famp.12305] [PMID]
- Dalgleish TL, Johnson SM, Burgess Moser M, Lafontaine MF, Wiebe SA, Tasca GA. Predicting change in marital satisfaction throughout emotionally focused couple therapy. Journal of Marital and Family Therapy. 2015; 41(3):276-91. [DOI:10.1111/jmft.12077] [PMID]
- Lalande K, Greenman PS, Bouchard K, Johnson SM, Tulloch H. The healing hearts together randomized controlled trial and the COVID-19 pandemic: A tutorial for transitioning from an in-person to a web-based intervention. Journal of Medical Internet Research. 2021; 23(4):e25502. [DOI:10.2196/25502] [PMID] [PMCID]
- Yoosefi N. [Investigation of psychometric properties of the revised dyadic adjustment scales (RDAS) (Persian)]. Research in Clinical Psychology and Counseling. 2012; 1(2):183-200. [Link]
- Fico G, Luciano M, Sampogna G, Zinno F, Steardo L Jr, Perugi G, et al. Validation of the brief TEMPS-M temperament questionnaire in a clinical Italian sample of bipolar and cyclothymic patients. Journal of Affective Disorders. 2020; 260:458-62. [DOI:10.1016/j.jad.2019.09.034] [PMID]
- Vázquez GH, Tondo L, Mazzarini L, Gonda X. Affective temperaments in general population: A review and combined analysis from national studies. Journal of Affective Disorders. 2012; 139(1):18-22. [DOI:10.1016/j.jad.2011.06.032] [PMID]
- Jiménez E, Bonnín CDM, Solé B, Sánchez-Moreno J, Reinares M, Torrent C, et al. Spanish validation of the Barcelona TEMPS-A questionnaire in patients with bipolar disorder and general population. Journal of Affective Disorders. 2019; 249:199-207. [DOI:10.1016/j.jad.2019.02.037] [PMID]
- Khalili N, Panjalizadeh ME, Jahani Y. Validation of the brief Persian version of the affective temperament auto-questionnaire TEMPS-A. Iranian Journal of Psychiatry and Clinical Psychology. 2018; 24(1):92-107. [DOI:10.29252/nirp.ijpcp.24.1.92]
- Johnson S. Attachment in action-changing the face of 21st century couple therapy. Current Opinion in Psychology. 2019; 25:101-4. [DOI:10.1016/j.copsyc.2018.03.007] [PMID]
- Vecsey-Nagy M, Szilveszter B, Kolossváry M, Boussoussou M, Vattay B, Gonda X, et al. Association between affective temperaments and severe coronary artery disease. Journal of Affective Disorders. 2021; 295:914-9. [DOI:10.1016/j.jad.2021.08.063] [PMID]
- Nemcsik J, Vecsey-Nagy M, Szilveszter B, Kolossváry M, Karády J, László A, et al. Inverse association between hyperthymic affective temperament and coronary atherosclerosis: A coronary computed tomography angiography study. Journal of Psychosomatic Research. 2017; 103:108-12. [DOI:10.1016/j.jpsychores.2017.10.013] [PMID]
- Eory A, Gonda X, Lang Z, Torzsa P, Kalman J Jr, Kalabay L, et al. Personality and cardiovascular risk: Association between hypertension and affective temperaments-a cross-sectional observational study in primary care settings. The European Journal of General Practice. 2014; 20(4):247-52. [DOI:10.3109/13814788.2013.868431] [PMID]
- Darvishi-Lord M, Besharat MA, Zahed-Mehr A, Farahani H. [The relationship between biomarkers and the severity of coronary artery disease: The moderating role of affective temperament (Persian)]. Iranian Journal of Cardiovascular Nursing. 2021; 10(1):50-60. [Link]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2023/08/6 | Accepted: 2023/10/25 | Published: 2024/09/1
Received: 2023/08/6 | Accepted: 2023/10/25 | Published: 2024/09/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
