

Volume 14, Issue 2 (Mar & Apr 2024)
J Research Health 2024, 14(2): 161-168 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fathima A, Daniel A, Kumar S. A Cross Sectional Study of Junk Food Consumption among Children and Adolescents in the Rural and Urban service areas of a Tertiary Care Hospital in Puducherry. J Research Health 2024; 14 (2) :161-168
URL: http://jrh.gmu.ac.ir/article-1-2411-en.html
URL: http://jrh.gmu.ac.ir/article-1-2411-en.html



1- Aarupadai Veedu Medical College, India. , aumrinfathima1993@gmail.com
2- Aarupadai Veedu Medical College, India.
2- Aarupadai Veedu Medical College, India.
Full-Text [PDF 804 kb]
(1565 Downloads)
| Abstract (HTML) (3814 Views)
Full-Text: (2619 Views)
Introduction
Junk food consumption has emerged as an essential part of the diet of Indian children and adolescents due to more attraction to the tempting advertising for junk foods [1]. Harmful behaviors acquired at this age usually continue throughout later stages of life. Undernutrition was a significant problem for public health in India. Historically, women in India were ignored in many aspects of life, even in nourishment. Almost 50% of Indian girls in adolescence are underweight [2]. Undernutrition during adolescence can impair physical and sexual development, which are consequences of malnourishment during infants and children. It also contributes to nutrition deficiency anaemia, and the prevalence of nutritional anaemia for Indian females was 63.7% [3]. This was perhaps related to knowledge about dietary requirements and the economic situation. Overweight children tend to be highly likely to become obese adults. Most overweight adolescents in India vary from 10% to 30% [4]. India has dealt with the twin burden of undernutrition and obesity in children and adolescents.
Junk food has been proven to contain an energy density that is more than double what is required for children daily. Junk food consumption is associated with various health hazards among children, leading to increased noncommunicable diseases, such as childhood obesity, hypertension, and juvenile diabetes [5]. Due to excessive sugar in junk foods, tooth caries is another common condition among school-going children. Food additives in fast foods are cancer-causing and allergenic, which may lead to asthmatic and dermatitis in children. Also, challenges, including poor infrastructure and poor hygiene, exist in cooking and storing food in the street vendors.
The parents, neighbors, school systems, and friends in a child’s surroundings should promote healthy lifestyle behaviors in nutrition and physical activity and educate them about the health problems of junk foods even from the school level onwards. Children are future citizens; it is necessary to tackle the issues influencing their health. This study was conducted to explore the magnitude of junk food consumption among children and adolescents and sociodemographic factors influencing junk food consumption.
Methods
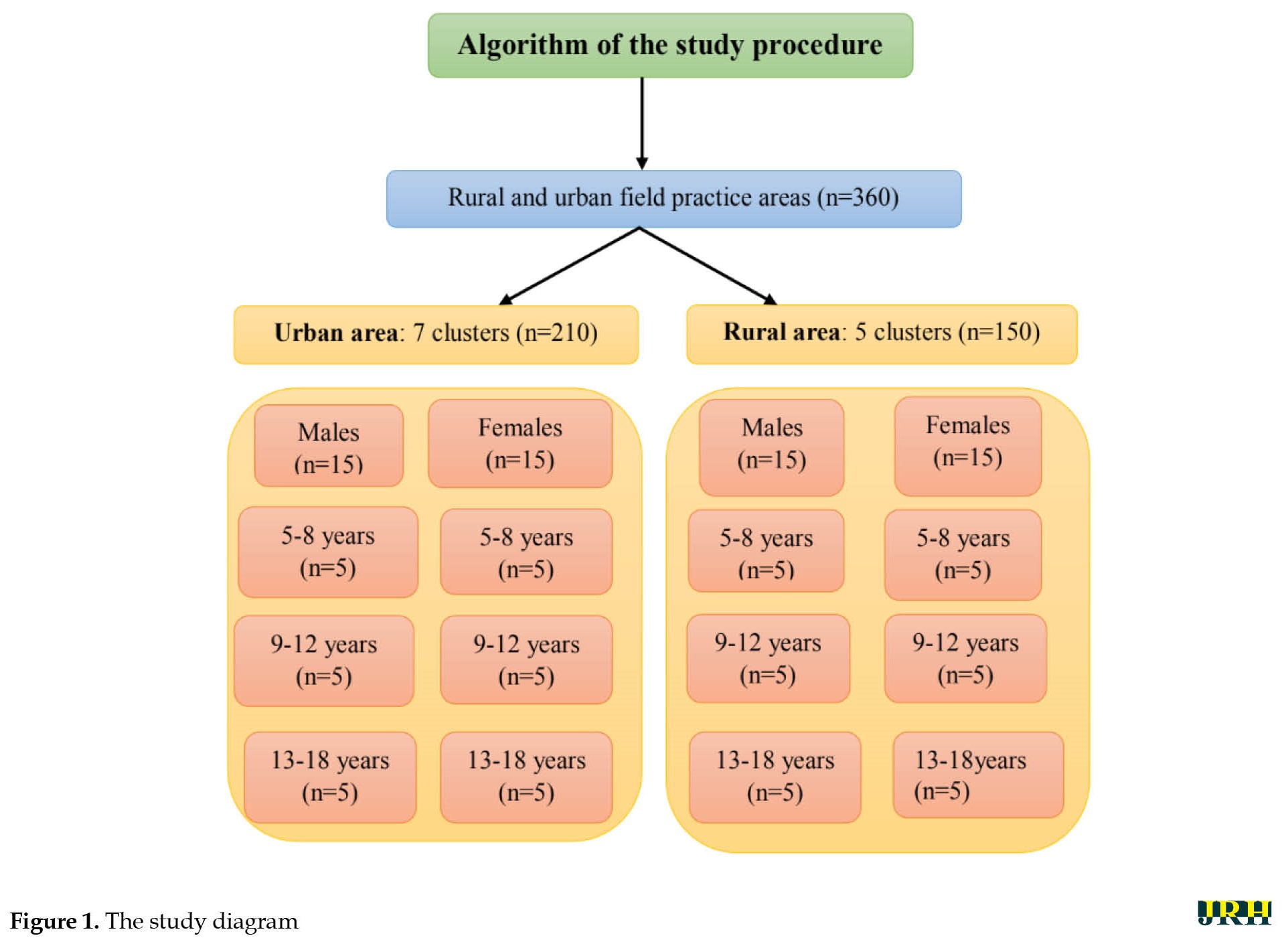
A community-based, cross-sectional study was conducted with all children (5-12 years old) and adolescents (13-18 years old) in rural (chinnakanganangkuppam) and urban (ariyankuppam) field practicing areas of our tertiary care facility (aarupadai veedu medical college and hospital) from December 2020 to October 2022 (1 year and 10 months). The inclusion criteria included children under the age of 5-12 years and adolescents aged 13-18 who dwell in the rural and urban field practicing regions (Figure 1).
 The exclusion criteria included children with eating disorders or mental retardation, children in locked residences while visiting, and those not consenting to participate in the study. Based on the previous prevalence of junk food addiction of 16% in a study conducted by Masthi et al. [6] in Bengaluru, Karnataka, a 95% confidence limit, 5% alpha error, and design effect were considered (1.6) (Equation 1):
The exclusion criteria included children with eating disorders or mental retardation, children in locked residences while visiting, and those not consenting to participate in the study. Based on the previous prevalence of junk food addiction of 16% in a study conducted by Masthi et al. [6] in Bengaluru, Karnataka, a 95% confidence limit, 5% alpha error, and design effect were considered (1.6) (Equation 1):
1. N=4pq/d2
P=16%, absolute precision d=5%, confidence limits=95%, level of significance=5%
N=4×16×84/5×5=215
Design effect (DEFF)=1+δ (n-1) (n-1)
δ=interclass correlation=0.02
n=cluster size=30
DEFF=1+0.02 (30-1)=1.6
Hence the effective sample size=calculated sample size×DEFF=215×1.6=344
This was rounded off to a total sample size of 360.
The sampling technique used was the cluster sampling technique. The selected children or adults were interviewed using a quasi-structured questionnaire after obtaining informed assent and consent from the parents. The rural field practice area, Chinnakanganankuppam, has 5 clusters in the rural area. The urban field practice area, Ariyankuppam, has 7 clusters in the urban region. Using a stratified random sampling technique within each cluster, 30 samples were taken from each cluster. Ten individuals from the age groups of 5-8 years, 9-12 years, and 13–18 years were chosen to represent each age group in the age stratification technique. The selection of 15 men and 15 women from each cluster served as the basis for gender stratification.
Statistical analysis
Data entry was performed in Excel. Analysis was performed using SPSS software version 28. Data were represented as percentages and frequencies in Tables and Figures. The categorical variables were differentiated using the non-parametric chi-square test. Multiple logistic regression analysis was performed to study the influence of various socio-demographic factors on junk food consumption and addiction. A P obtained through chi-square test and P<0.05 was considered significant.
Results
Table 1 presents the type of junk food consumption.
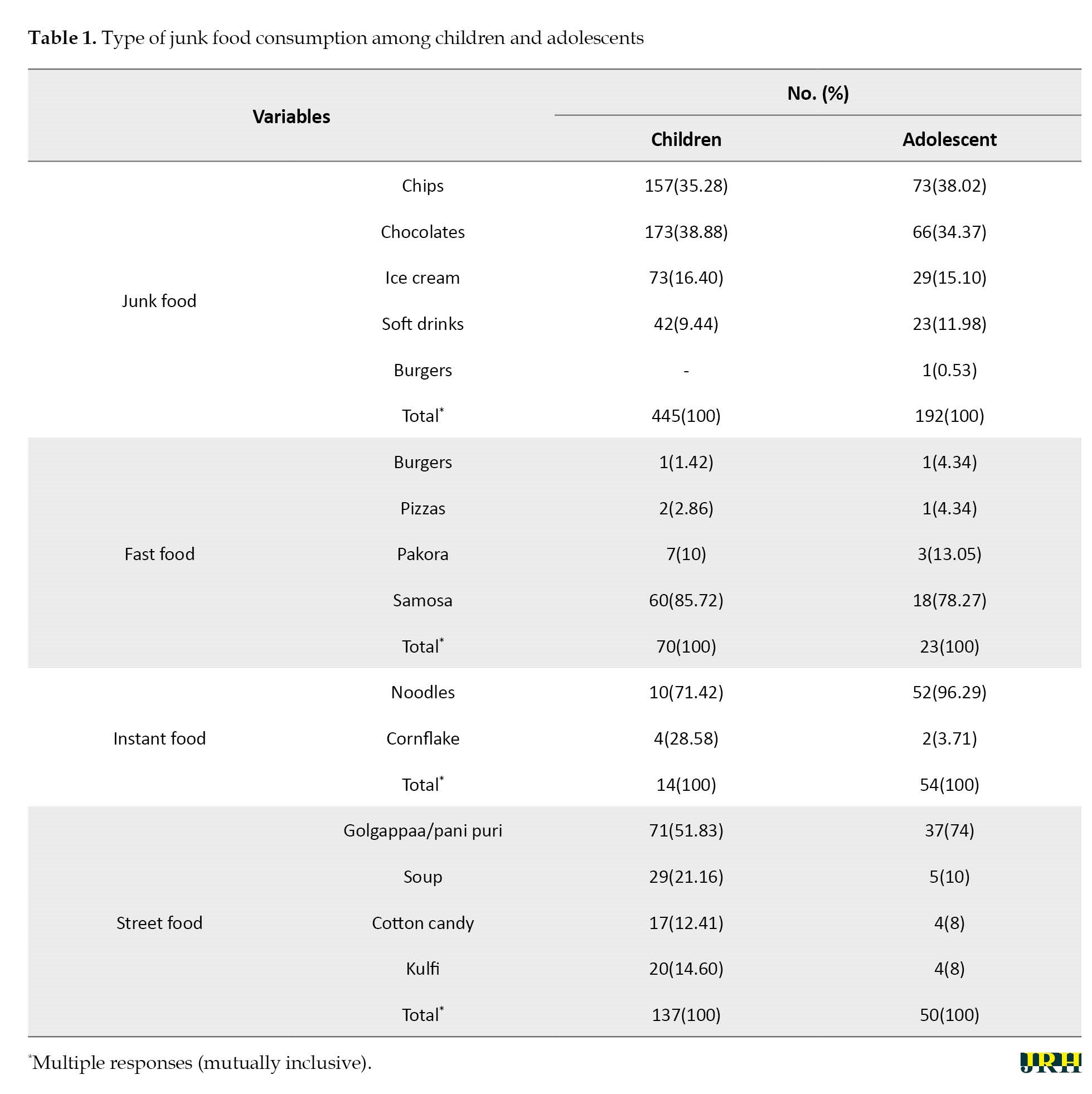
The most common junk food eaten by 173 children was chocolate (38.88%) and in 73 adolescents, it was chips (38.02%). The most common fast food eaten by the 60 children (85.72%) and 18 adolescents (78.27%) was samosa. The most common instant food eaten by 10 children (71.42%) and 52 adolescents (96.29%) was noodles. The most common street food for 71 children (51.83%) and 37 adolescents (74%) was golgappaa/pani puri.
Figure 2 shows junk food consumption based on the weekly distribution.
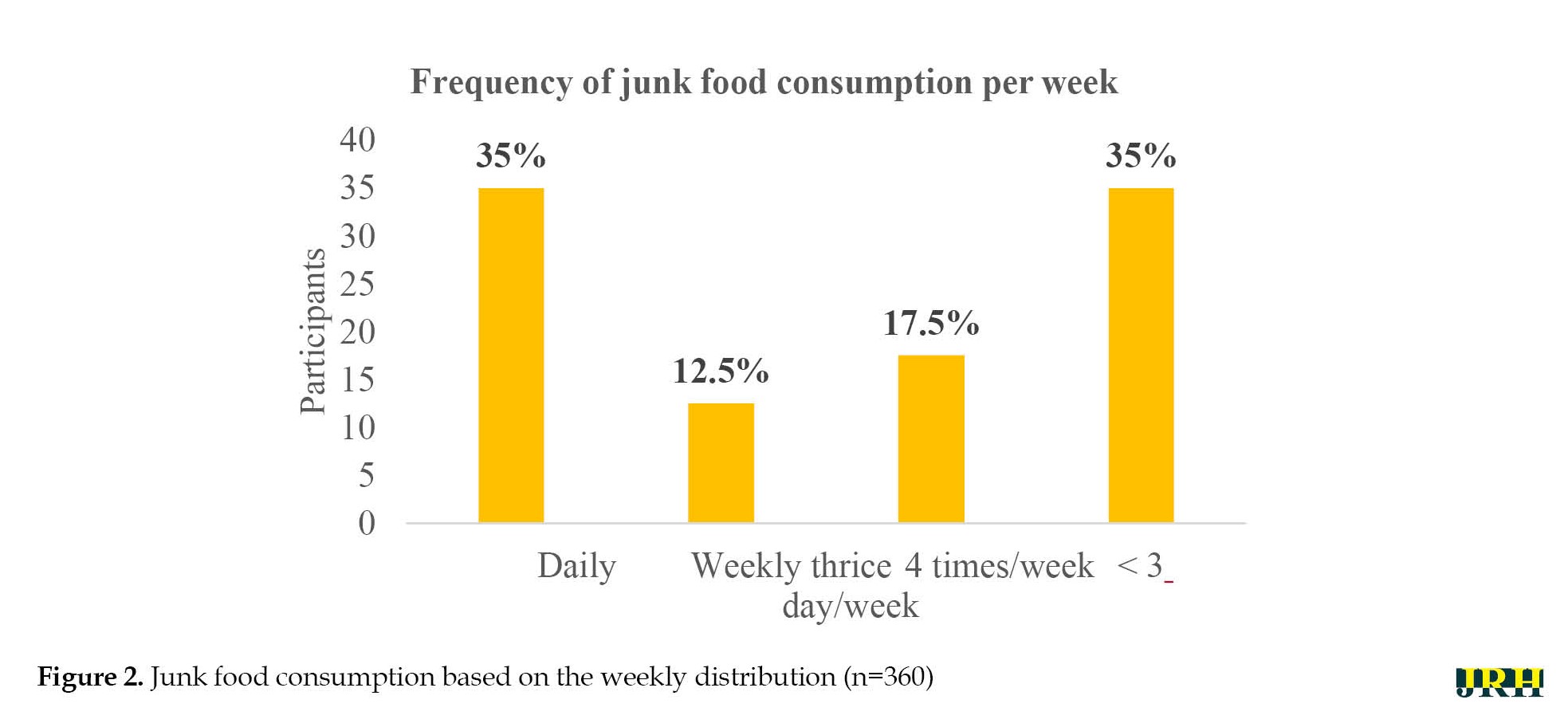 Statistically, significant junk food consumption is more frequent daily and less than 3 days a week compared to the weekly thrice and 4 times frequency of junk consumption per week (P<0.001).
Statistically, significant junk food consumption is more frequent daily and less than 3 days a week compared to the weekly thrice and 4 times frequency of junk consumption per week (P<0.001).
Table 2 presents junk food consumption based on age and gender distribution.
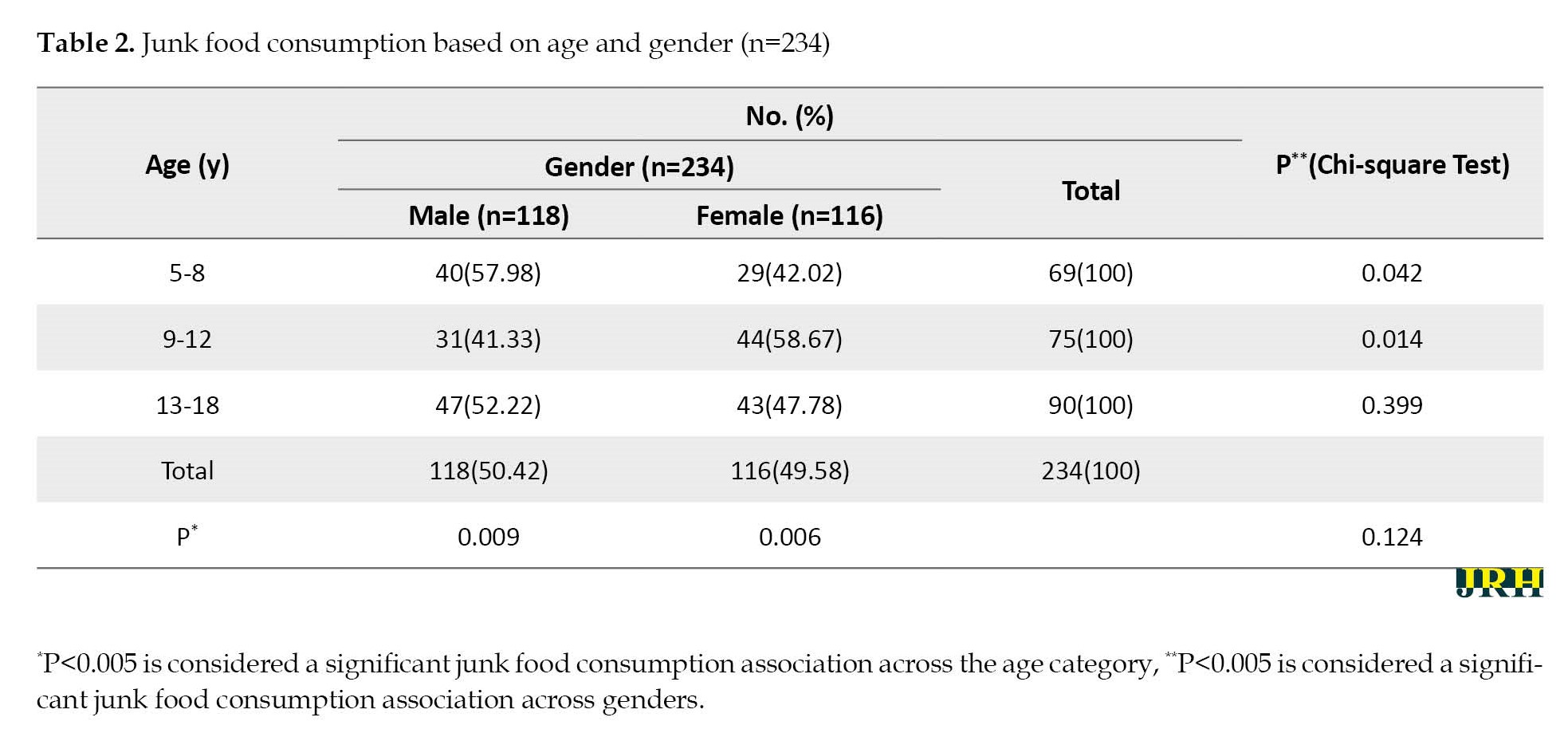
The prevalence of junk food consumption in 144 children (5-12 years old) was 40% and in 90 adolescents (13-18 years old), it was 25%. Junk food consumption is increased in men in the 13-18 age category compared to other age categories. This difference was statistically significant (P=0.009). Junk food consumption is increased in women in the 9-12 age category compared to other age categories. This difference was statistically significant (P=0.006).
Table 3 presents a comparison of junk food consumption among children and adolescents in urban and rural.
Increased relationship between junk food consumption in urban and children increased. A significant increase was observed in junk food consumption in urban among 101 children (63.53%), compared to 58 adolescents (36.47%). The difference was statistically significant (P=0.015). Increased junk food consumption was observed in 101 children (63.53%) in urban, compared to 43 children (57.33%) in rural. It was statistically significant.
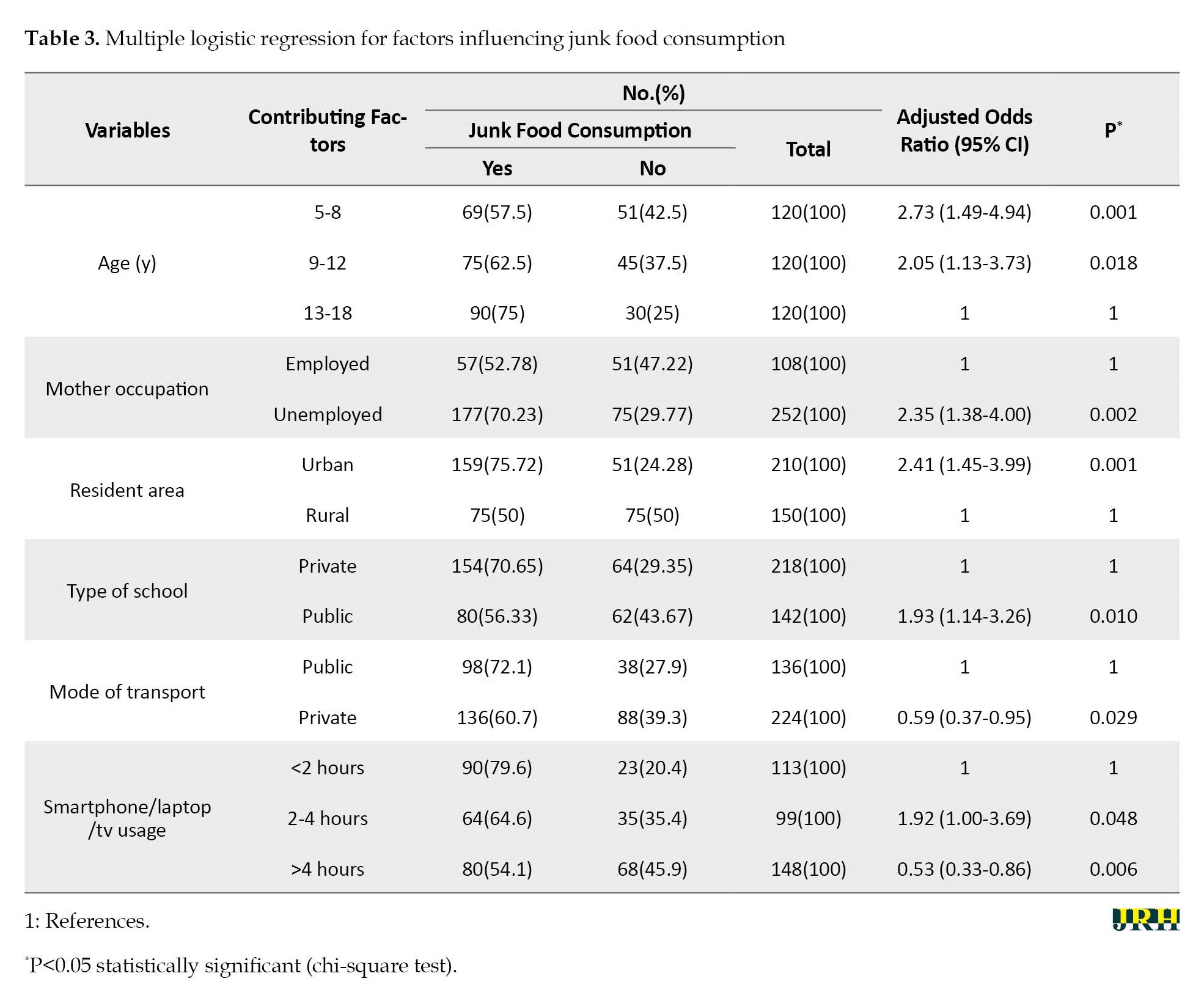
Table 3 presents multiple logistic regressions for factors influencing junk food consumption. The age category of 5-8 years had 2.73 higher junk food consumption compared to the age category of 13-18 years of age and it was statistically significant (P=0.001). The age category of 9-12 years had 2.05 higher junk food consumption than the age category of 13-18 years and it was statistically significant (P=0.018). The children of unemployed mothers had 2.35 higher junk food consumption compared to the children of employed mothers and were statistically significant (P=0.002). Urban had 2.41 higher junk food consumption compared to rural, which is statistically significant (P=0.001). The public school students had 1.93 higher junk food consumption than private school, which was statistically significant (P=0.010). The private transport used by the students had 0.59 higher junk food consumption than public transport, which was statistically significant (P=0.029). The smartphone/laptop/tv usage of 2-4 hours had 1.92 higher junk food consumption than smartphone/laptop/tv usage of <2 hours, which was statistically significant (P=0.048). The age category of 5-8 years and 9-12 years, unemployed mother, urban area, private school, smartphone/laptop/tv usage of 2-4 hours and >4 hours were statistically significant with factors influencing junk food consumption.
Discussion
The pattern of junk food consumption was similar to the previous studies.
Bohara et al. [7] showed that eaten foods, such as fast foods, salty snacks, chocolates, and sweetened drinks were often consumed. Expenditure per week, consumption while traveling, when partying, consumption locations, and timing were all studied. Sapkota et al. [8] found the most common chat pat, followed by biscuits, chocolate, ice cream, and cold beverages. Sahu et al. [9] noted that chips 16%), ice cream (13.5%), chocolate (6.7%), and puchka (6.4%) were the most common foods purchased with pocket money. Despite knowing the harmful effects of unhealthy foods, they continued to eat junk food due to their taste preference and desire to do so. Parents should encourage children to practice good eating habits themselves and act as role models for their kids to create a home environment that is nutrition-conscious and supportive [9].
In our study, the prevalence of junk food consumption was 65%, similar to Masthi et al [6]. and Antony et al. [10] conducted in Karnataka and Maharashtra, respectively. The prevalence of the present study was more significant compared to Chandra et al. [11] and Gupta et al. [12] This may be due to nutritional transition due to lifestyle changes are contributing factors. Metabolic alterations, including obesity, high blood pressure, and diabetes, damage health as the altering consumption pattern shifts away from traditional cuisine toward processed and high-calorie meals. Lesser prevalence may also be due to the inclusion of the rural area under the study.
The present study showed that children were consuming increased junk food compared to adolescents, similar to Masthi et al. [6] and Fryar et al. [13] in Atlanta. Junk food intake declined with age. Male predominance was observed in the present study, similar to Fryar et al [13]. In contrast, Sapkota et al. [8] showed female predominance. In our study, most junk food consumers were literate parents. They had middle socioeconomic status, similar to Arumugam et al. [14]. In contrast, Singh et al. [15] showed that illiterate parents and lower socioeconomic status influenced junk food consumption. This difference may be possible due to the favored taste, the ability to be eaten instantly, the ease of access, and the effect of ads, all of which play a significant part in eating junk food.
Most junk food consumption was from urban. Urban had 2.41 times the risk of junk food consumption compared to rural, which is statistically significant (P=0.001), similar to a study conducted by Pandey et al. [16] in India. In contrast, Tripathy et al. [17] stated that no such differences were determined. The variety of food preferences, enhanced market accessibility, and women’s time spent working in cities also influenced junk food consumption. Contrarily, irregular vendors are observed in rural schools, which led to a reduction in the intake of junk food in rural areas.
In the present study, most children and adolescents who consumed junk food were from private schools, similar to the study conducted by Ganle et al. [18] among schoolchildren in Ghana, Africa. It was inconsistent with the study conducted by Bohara et al. [7] on public schools with junk food consumption. This difference may be because the children never brought lunch to class and ate junk food, which is inexpensive and conveniently accessible close to the school. Since no restrictions are observed in school, more retail establishments are selling chips close to the school. If the school does not offer a nutritious mid-day meal, students should bring lunch boxes filled with healthful foods. In a formal system, all schools should encourage balanced diets and draw attention to the adverse effects of junk food. Government should take the initiative to substitute healthy raw materials in junk food packets (for e.g. substituting wheat instead of Maida in biscuits) and fortification in junk food with healthy tips labeling (e.g. adding fibre rich content in noodles) and prevent sales of harmful addictive-junk foods in the premise of schools.
Conclusion
The most common junk food, fast food, instant food, and street food eaten by children and adolescents were chocolate and chips, samosa, noodles, and golgappaa/pani puri, respectively. Junk food consumption was higher in children and urban compared to adolescents and rural, respectively. The literate father and unemployed mother were associated with increased. Students should be advised to avoid eating while viewing a smartphone/laptop/television. If the school does not offer a nutritious mid-day meal, students should bring lunch boxes filled with healthful foods. In a formal system, all schools should encourage balanced diets and draw attention to the adverse effects of junk food. Parents should encourage children to practice good eating habits themselves and act as role models for their kids to create a home environment that is nutrition-conscious and supportive. Government should take the initiative to substitute healthy raw materials in junk food packets (for e.g. substituting wheat instead of Maida in biscuits) and fortification in junk food with healthy tips labeling (e.g. adding fibre rich content in noodles) and prevent sales of harmful addictive-junk foods in the premise of schools.
Strength
It is a large-scale study conducted in a community comparing the urban and rural differences in junk food consumption. The study delineated boundaries between junk food consumption and addiction and estimated stratified prevalences in various age groups. Smartphone usage, schooling, and many other lifestyle factors were studied, and their influences were associated. The morbidity pattern was compared between junk food users and non-users.
Limitation
The entire study was based on a subjective assessment of junk food consumption. A source of recall bias during the interview was observed. Associations were made based on cross-sectional data and hence further follow-up studies are needed to confirm the association.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The study was approved by the Research Ethics Committees of Aarupadai Veedu Medical College (IEC No.: AV/IEC/2020/130). Written consent was obtained before the data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision and analysis: Arun Daniel; Data collection, data interpretation and manuscript writing: Aumrin Fathima; Investigation: Sevvanthi Kumar.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Aarupadai Veedu Medical College for providing us with resources and transport for data collection. The authors also thank the social worker who accompanied them during the data collection. Lastly, thank all participants who are involved in this study.
References
Junk food consumption has emerged as an essential part of the diet of Indian children and adolescents due to more attraction to the tempting advertising for junk foods [1]. Harmful behaviors acquired at this age usually continue throughout later stages of life. Undernutrition was a significant problem for public health in India. Historically, women in India were ignored in many aspects of life, even in nourishment. Almost 50% of Indian girls in adolescence are underweight [2]. Undernutrition during adolescence can impair physical and sexual development, which are consequences of malnourishment during infants and children. It also contributes to nutrition deficiency anaemia, and the prevalence of nutritional anaemia for Indian females was 63.7% [3]. This was perhaps related to knowledge about dietary requirements and the economic situation. Overweight children tend to be highly likely to become obese adults. Most overweight adolescents in India vary from 10% to 30% [4]. India has dealt with the twin burden of undernutrition and obesity in children and adolescents.
Junk food has been proven to contain an energy density that is more than double what is required for children daily. Junk food consumption is associated with various health hazards among children, leading to increased noncommunicable diseases, such as childhood obesity, hypertension, and juvenile diabetes [5]. Due to excessive sugar in junk foods, tooth caries is another common condition among school-going children. Food additives in fast foods are cancer-causing and allergenic, which may lead to asthmatic and dermatitis in children. Also, challenges, including poor infrastructure and poor hygiene, exist in cooking and storing food in the street vendors.
The parents, neighbors, school systems, and friends in a child’s surroundings should promote healthy lifestyle behaviors in nutrition and physical activity and educate them about the health problems of junk foods even from the school level onwards. Children are future citizens; it is necessary to tackle the issues influencing their health. This study was conducted to explore the magnitude of junk food consumption among children and adolescents and sociodemographic factors influencing junk food consumption.
Methods
A community-based, cross-sectional study was conducted with all children (5-12 years old) and adolescents (13-18 years old) in rural (chinnakanganangkuppam) and urban (ariyankuppam) field practicing areas of our tertiary care facility (aarupadai veedu medical college and hospital) from December 2020 to October 2022 (1 year and 10 months). The inclusion criteria included children under the age of 5-12 years and adolescents aged 13-18 who dwell in the rural and urban field practicing regions (Figure 1).
1. N=4pq/d2
P=16%, absolute precision d=5%, confidence limits=95%, level of significance=5%
N=4×16×84/5×5=215
Design effect (DEFF)=1+δ (n-1) (n-1)
δ=interclass correlation=0.02
n=cluster size=30
DEFF=1+0.02 (30-1)=1.6
Hence the effective sample size=calculated sample size×DEFF=215×1.6=344
This was rounded off to a total sample size of 360.
The sampling technique used was the cluster sampling technique. The selected children or adults were interviewed using a quasi-structured questionnaire after obtaining informed assent and consent from the parents. The rural field practice area, Chinnakanganankuppam, has 5 clusters in the rural area. The urban field practice area, Ariyankuppam, has 7 clusters in the urban region. Using a stratified random sampling technique within each cluster, 30 samples were taken from each cluster. Ten individuals from the age groups of 5-8 years, 9-12 years, and 13–18 years were chosen to represent each age group in the age stratification technique. The selection of 15 men and 15 women from each cluster served as the basis for gender stratification.
Statistical analysis
Data entry was performed in Excel. Analysis was performed using SPSS software version 28. Data were represented as percentages and frequencies in Tables and Figures. The categorical variables were differentiated using the non-parametric chi-square test. Multiple logistic regression analysis was performed to study the influence of various socio-demographic factors on junk food consumption and addiction. A P obtained through chi-square test and P<0.05 was considered significant.
Results
Table 1 presents the type of junk food consumption.
The most common junk food eaten by 173 children was chocolate (38.88%) and in 73 adolescents, it was chips (38.02%). The most common fast food eaten by the 60 children (85.72%) and 18 adolescents (78.27%) was samosa. The most common instant food eaten by 10 children (71.42%) and 52 adolescents (96.29%) was noodles. The most common street food for 71 children (51.83%) and 37 adolescents (74%) was golgappaa/pani puri.
Figure 2 shows junk food consumption based on the weekly distribution.
Table 2 presents junk food consumption based on age and gender distribution.
The prevalence of junk food consumption in 144 children (5-12 years old) was 40% and in 90 adolescents (13-18 years old), it was 25%. Junk food consumption is increased in men in the 13-18 age category compared to other age categories. This difference was statistically significant (P=0.009). Junk food consumption is increased in women in the 9-12 age category compared to other age categories. This difference was statistically significant (P=0.006).
Table 3 presents a comparison of junk food consumption among children and adolescents in urban and rural.
Increased relationship between junk food consumption in urban and children increased. A significant increase was observed in junk food consumption in urban among 101 children (63.53%), compared to 58 adolescents (36.47%). The difference was statistically significant (P=0.015). Increased junk food consumption was observed in 101 children (63.53%) in urban, compared to 43 children (57.33%) in rural. It was statistically significant.
Table 3 presents multiple logistic regressions for factors influencing junk food consumption. The age category of 5-8 years had 2.73 higher junk food consumption compared to the age category of 13-18 years of age and it was statistically significant (P=0.001). The age category of 9-12 years had 2.05 higher junk food consumption than the age category of 13-18 years and it was statistically significant (P=0.018). The children of unemployed mothers had 2.35 higher junk food consumption compared to the children of employed mothers and were statistically significant (P=0.002). Urban had 2.41 higher junk food consumption compared to rural, which is statistically significant (P=0.001). The public school students had 1.93 higher junk food consumption than private school, which was statistically significant (P=0.010). The private transport used by the students had 0.59 higher junk food consumption than public transport, which was statistically significant (P=0.029). The smartphone/laptop/tv usage of 2-4 hours had 1.92 higher junk food consumption than smartphone/laptop/tv usage of <2 hours, which was statistically significant (P=0.048). The age category of 5-8 years and 9-12 years, unemployed mother, urban area, private school, smartphone/laptop/tv usage of 2-4 hours and >4 hours were statistically significant with factors influencing junk food consumption.
Discussion
The pattern of junk food consumption was similar to the previous studies.
Bohara et al. [7] showed that eaten foods, such as fast foods, salty snacks, chocolates, and sweetened drinks were often consumed. Expenditure per week, consumption while traveling, when partying, consumption locations, and timing were all studied. Sapkota et al. [8] found the most common chat pat, followed by biscuits, chocolate, ice cream, and cold beverages. Sahu et al. [9] noted that chips 16%), ice cream (13.5%), chocolate (6.7%), and puchka (6.4%) were the most common foods purchased with pocket money. Despite knowing the harmful effects of unhealthy foods, they continued to eat junk food due to their taste preference and desire to do so. Parents should encourage children to practice good eating habits themselves and act as role models for their kids to create a home environment that is nutrition-conscious and supportive [9].
In our study, the prevalence of junk food consumption was 65%, similar to Masthi et al [6]. and Antony et al. [10] conducted in Karnataka and Maharashtra, respectively. The prevalence of the present study was more significant compared to Chandra et al. [11] and Gupta et al. [12] This may be due to nutritional transition due to lifestyle changes are contributing factors. Metabolic alterations, including obesity, high blood pressure, and diabetes, damage health as the altering consumption pattern shifts away from traditional cuisine toward processed and high-calorie meals. Lesser prevalence may also be due to the inclusion of the rural area under the study.
The present study showed that children were consuming increased junk food compared to adolescents, similar to Masthi et al. [6] and Fryar et al. [13] in Atlanta. Junk food intake declined with age. Male predominance was observed in the present study, similar to Fryar et al [13]. In contrast, Sapkota et al. [8] showed female predominance. In our study, most junk food consumers were literate parents. They had middle socioeconomic status, similar to Arumugam et al. [14]. In contrast, Singh et al. [15] showed that illiterate parents and lower socioeconomic status influenced junk food consumption. This difference may be possible due to the favored taste, the ability to be eaten instantly, the ease of access, and the effect of ads, all of which play a significant part in eating junk food.
Most junk food consumption was from urban. Urban had 2.41 times the risk of junk food consumption compared to rural, which is statistically significant (P=0.001), similar to a study conducted by Pandey et al. [16] in India. In contrast, Tripathy et al. [17] stated that no such differences were determined. The variety of food preferences, enhanced market accessibility, and women’s time spent working in cities also influenced junk food consumption. Contrarily, irregular vendors are observed in rural schools, which led to a reduction in the intake of junk food in rural areas.
In the present study, most children and adolescents who consumed junk food were from private schools, similar to the study conducted by Ganle et al. [18] among schoolchildren in Ghana, Africa. It was inconsistent with the study conducted by Bohara et al. [7] on public schools with junk food consumption. This difference may be because the children never brought lunch to class and ate junk food, which is inexpensive and conveniently accessible close to the school. Since no restrictions are observed in school, more retail establishments are selling chips close to the school. If the school does not offer a nutritious mid-day meal, students should bring lunch boxes filled with healthful foods. In a formal system, all schools should encourage balanced diets and draw attention to the adverse effects of junk food. Government should take the initiative to substitute healthy raw materials in junk food packets (for e.g. substituting wheat instead of Maida in biscuits) and fortification in junk food with healthy tips labeling (e.g. adding fibre rich content in noodles) and prevent sales of harmful addictive-junk foods in the premise of schools.
Conclusion
The most common junk food, fast food, instant food, and street food eaten by children and adolescents were chocolate and chips, samosa, noodles, and golgappaa/pani puri, respectively. Junk food consumption was higher in children and urban compared to adolescents and rural, respectively. The literate father and unemployed mother were associated with increased. Students should be advised to avoid eating while viewing a smartphone/laptop/television. If the school does not offer a nutritious mid-day meal, students should bring lunch boxes filled with healthful foods. In a formal system, all schools should encourage balanced diets and draw attention to the adverse effects of junk food. Parents should encourage children to practice good eating habits themselves and act as role models for their kids to create a home environment that is nutrition-conscious and supportive. Government should take the initiative to substitute healthy raw materials in junk food packets (for e.g. substituting wheat instead of Maida in biscuits) and fortification in junk food with healthy tips labeling (e.g. adding fibre rich content in noodles) and prevent sales of harmful addictive-junk foods in the premise of schools.
Strength
It is a large-scale study conducted in a community comparing the urban and rural differences in junk food consumption. The study delineated boundaries between junk food consumption and addiction and estimated stratified prevalences in various age groups. Smartphone usage, schooling, and many other lifestyle factors were studied, and their influences were associated. The morbidity pattern was compared between junk food users and non-users.
Limitation
The entire study was based on a subjective assessment of junk food consumption. A source of recall bias during the interview was observed. Associations were made based on cross-sectional data and hence further follow-up studies are needed to confirm the association.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The study was approved by the Research Ethics Committees of Aarupadai Veedu Medical College (IEC No.: AV/IEC/2020/130). Written consent was obtained before the data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision and analysis: Arun Daniel; Data collection, data interpretation and manuscript writing: Aumrin Fathima; Investigation: Sevvanthi Kumar.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the Aarupadai Veedu Medical College for providing us with resources and transport for data collection. The authors also thank the social worker who accompanied them during the data collection. Lastly, thank all participants who are involved in this study.
References
- Harris JL, Graff SK. Protecting young people from junk food advertising: Implications of psychological research for first amendment law. American Journal of Public Health. 2012; 102(2):214-22. [DOI:10.2105/AJPH.2011.300328] [PMID]
- Anand D, Anuradha RK. Malnutrition status of adolescent girls in India: A need for the hour. International Journal of Science and Research. 2013; 5(3):642-6. [Link]
- Vijaya Kumar U, Budaya Kiran MS, Lakshmana Rao N. A community study on prevalence and knowledge regarding anaemia among adolescent girls in a rural area of Rajahmundry, Andhra Pradesh. Indian Journal of Public Health Research and Development. 2015; 6(1):261-6. [Link]
- Kotian MS, S GK, Kotian SS. Prevalence and determinants of overweight and obesity among adolescent school children of South Karnataka, India. Indian Journal of Community Medicine. 2010; 35(1):176-8. [DOI:10.4103/0970-0218.62587] [PMID]
- Singh SA, Dhanasekaran D, Ganamurali NL P, Sabarathinam S. Junk food-induced obesity-a growing threat to youngsters during the pandemic. Obesity Medicine. 2021; 26:100364. [DOI:10.1016/j.obmed.2021.100364] [PMID]
- Masthi NR, Jahan A. Junk food addiction across generations in urban Karnataka, India. Journal of Communicable Diseases. 2020; 52(1):65-71.[DOI:10.24321/0019.5138.202008]
- Bohara SS, Thapa K, Bhatt LD, Dhami SS, Wagle S. Determinants of junk food consumption among adolescents in Pokhara Valley, Nepal. Frontiers in Nutrition. 2021; 8:644650. [DOI:10.3389/fnut.2021.644650] [PMID]
- Sapkota SD, Neupane S. Junk food consumption among secondary level students, Chitwan. Journal of Nepal Paediatric Society. 2017; 37(2):147-52. [Link]
- Sahu PK, Das BR. Consumption pattern and knowledge about Ill effects of junk food amongst school children in urban area of Jorhat. International Journal of Health Sciences and Research. 2018; 8:7-13. [Link]
- Antony M, Bhatti RK. Junk food consumption and knowledge about its ill effects among teenagers: A descriptive study. International Journal of Science and Research. 2015; 4(6):1133-6. [Link]
- Chandar D, Naik BN, Thumati G, Sarkar S. Assessment of dietary habits and nutritional status among adolescent girls in a rural area of Puducherry: A community-based cross- sectional study. International Journal of Adolescent Medicine and Health. 2018; 32(5). [DOI:10.1515/ijamh-2018-0001] [PMID]
- Gupta A, Kapil U, Singh G. Consumption of junk foods by school-aged children in rural Himachal Pradesh, India. Indian Journal of Public Health. 2018; 62(1):65-7. [DOI:10.4103/ijph.IJPH_343_16] [PMID]
- Fryar CD, Hughes JP, Herrick KA, Ahluwalia N. Fast food consumption among adults in the United States, 2013-2016. NCHS Data Brief. 2018; 322:1-8. [Link]
- Arumugam B, Suganya A, Nagalingam S, Suveka V. Fast food addiction-The junk enslavement. International Archives of Integrated Medicine. 2015; 2(1):62-70. [Link]
- Singh UK, Gautam N, Bhandari TR, Sapkota N. Educational intervention of intention change for consumption of junk food among school adolescents in Birgunj Metropolitan City, Nepal, based on theory of planned behaviors. Journal of Nutrition and Metabolism. 2020; 2020:7932324.[DOI:10.1155/2020/7932324] [PMID]
- Pandey B, Reba M, Joshi PK, Seto KC. Urbanization and food consumption in India. Scientific Reports. 2020; 10(1):17241; [DOI:10.1038/s41598-020-73313-8] [PMID]
- Tripathy JP, Thakur JS, Jeet G, Chawla S, Jain S, Prasad R. Urban rural differences in diet, physical activity and obesity in India: Are we witnessing the great Indian equalisation? Results from a cross-sectional STEPS survey. BMC Public Health. 2016; 16(1):816. [DOI:10.1186/s12889-016-3489-8] [PMID]
- Ganle JK, Boakye PP, Baatiema L. Childhood obesity in urban Ghana: Evidence from a cross-sectional survey of in-school children aged 5-16 years. BMC Public Health. 2019; 19(1):1561. [DOI:10.1186/s12889-019-7898-3] [PMID]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2023/08/25 | Accepted: 2023/10/7 | Published: 2024/03/1
Received: 2023/08/25 | Accepted: 2023/10/7 | Published: 2024/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
