

Volume 14, Issue 5 (Sep & Oct 2024)
J Research Health 2024, 14(5): 449-456 |
Back to browse issues page



Ethics code: IR.GMU.REC.1400.101
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zamani R, Esmaeili R, Moghimi Shahri E, Mokhtari A M. Impact of the COVID-19 Pandemic on Receiving Dental Care Services From Community Health Centers in Iran. J Research Health 2024; 14 (5) :449-456
URL: http://jrh.gmu.ac.ir/article-1-2465-en.html
URL: http://jrh.gmu.ac.ir/article-1-2465-en.html



1- Department of Public Health, Social Development and Health Promotion Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran.
2- Department of Epidemiology and Biostatistics, Social Development and Health Promotion Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran. ,Mokhtariam67@yahoo.com
2- Department of Epidemiology and Biostatistics, Social Development and Health Promotion Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran. ,
Keywords: COVID-19, Dental care, Dental service, Check-up, Tooth extraction, Dental restoration, Dental scaling
Full-Text [PDF 598 kb]
(513 Downloads)
| Abstract (HTML) (3453 Views)
Full-Text: (810 Views)
Introduction
A virus originating in Wuhan, China, was first reported in late 2019 [1] and quickly spread to other cities in China and various countries globally. The World Health Organization (WHO) named the resulting disease as COVID-19 and declared it a pandemic [2, 3]. COVID-19 cases have been reported in many countries worldwide, affecting over 768 million individuals and claiming the lives of more than 6,945,000 people as of June 2023 [4].
Although this new virus is mainly transmitted through the large nasal or oral droplets of symptomatic patients [5], it is important to note that asymptomatic patients can also spread the disease [6, 7]. Because of the rapid spread of COVID-19, people in most countries have been recommended to limit their visits to crowded places as much as possible to prevent the transmission of the virus. Additionally, the fear of contracting coronavirus, fueled by the swift spread of the disease, has influenced people’s choices regarding visiting crowded locations such as hospitals or facilities offering medical and dental services [8, 9].
Dental procedures are recognized as potential avenues for disease transmission due to contaminated equipment, as suspended particles generated by dental instruments can land on various surfaces and facilitate virus transmission [10]. Dentists and other members of dental teams involved in procedures that generate aerosols can directly transmit the virus to individuals who are not infected [11].
At the onset of the COVID-19 pandemic, dentists worldwide were recommended to limit their professional activities to emergencies only and postpone non-emergency dental treatments until there was a relative decrease in the prevalence of the disease [9]. However, this practice can lead to health consequences such as a significant increase in oral and dental infections [8, 12]. For example, the results of a study in China showed that demand for dental services dramatically declined at the onset of the COVID-19 pandemic [9]. Another study has also indicated a sharp decline in visits to emergency departments in the US during the initial month after the beginning of the COVID-19 pandemic [13].
Since the first case of COVID-19 in Iran was reported in Qom in February 2020 [14], Iran has recorded over 7 million cases of COVID-19 and more than 146,000 deaths attributed to the disease [4]. Community health centers (CHCs) within the Iran healthcare system play a crucial role in providing primary dental care services, especially for vulnerable groups, such as children, pregnant women, and the elderly [15-17]. Therefore, a significant decrease in dental visits is concerning as it can lead to adverse outcomes Due to the restrictions on private dental care centers during the COVID-19 pandemic in Iran, it is unlikely that private dental care facilities will be able to offset the decrease in dental services provided by CHCs. Moreover, given the high costs associated with dental care services provided by private centers in Iran, the increase in out-of-pocket expenses for dental care services has become a serious concern [18].
The recommendations for dentists to prioritize emergency cases and the public’s fear of contracting COVID-19 in dental settings have significantly decreased the frequency of dental visits. This reduction in visits can lead to health implications, including a shift towards more invasive procedures. Several studies in Iran have explored the decline in dental appointments following the COVID-19 pandemic [19]. Therefore, this study aims to compare dental visit frequencies before and during the pandemic and examine the effects of COVID-19 on dental care utilization patterns in the Gonabad community health centers.
Methods
This cross-sectional study was conducted on clients receiving dental services at public CHCs in Gonabad, Iran, whose information is registered in the integrated health system of Iran’s Ministry of Health and Medical Education (SIB). The COVID-19 pandemic (before and during COVID-19) was regarded as an independent variable and dental visits and services were regarded as a dependent variable (outcome variable).
The main purpose of this study was to investigate the effects of the COVID-19 pandemic on dental visits and services. Some factors that could potentially skew the results include variations in the number of operational centers during the two periods being compared, along with factors influencing the volume of visitors to these centers (such as the saffron harvest season). Therefore, in order to reduce potential biases, we tried to choose the time frames where these factors were similar. Also, we made efforts to minimize the influence of confounding variables (like the type of services offered) to enhance the comparability between the two periods. Therefore, participants across all age groups were selected from among those who visited these centers between December 2019 and January and February 2020 (pre-COVID-19 period) and between December 2020 and January and February 2021 (during the COVID-19 pandemic period).
The first case of COVID-19 in Iran was confirmed in February 2020. Due to the closure of dental centers at the onset of the pandemic, specifically from March 10, 2020, to May 30, 2020, and again from July 4, 2020, to August 22, 2020, with only elective services available to clients in specific centers (Shahid Fayyazbakhsh and Shahid Aghaei centers), the period from February to November 2020 was not considered as part of the COVID-19 pandemic period. Moreover, the timeframe from October to November was also excluded because the decrease in dental visits in this period could partly be attributed to the involvement of some individuals from Gonabad in the harvest of saffron (a significant activity in this region).
Since some health centers are less visited by people and some others are visited more and also the qualities and performance of dentists and dental healthcare professionals may vary from center to center, the required data were equally obtained from all 16 health centers affiliated with the Gonabad University of Medical Sciences.
Inclusion and exclusion criterion
The checklist used in this study included items, such as the number of clients and the number of dental care services, such as check-ups, tooth extractions, tooth restorations, and scaling, all of which are routinely documented in the SIB system. Therefore, the only inclusion criterion was receiving dental care services at the centers affiliated with the Gonabad University of Medical Sciences during the two studied periods with registered information in the SIB. The incompleteness of the information recorded in the SIB system was also regarded as an exclusion criterion.
The data were extracted from the SIB, recorded on a checklist, and inputted into SPSS software, version 22. Both descriptive and analytical statistics were used to analyze the data at a significance level of <0.05. Initially, the normality of the quantitative data was assessed, and independent-sample t-test applied to normal variables and the Mann-Whitney test used for other variables. The figures were drawn by the SigmaPlot software, version 11.
Results
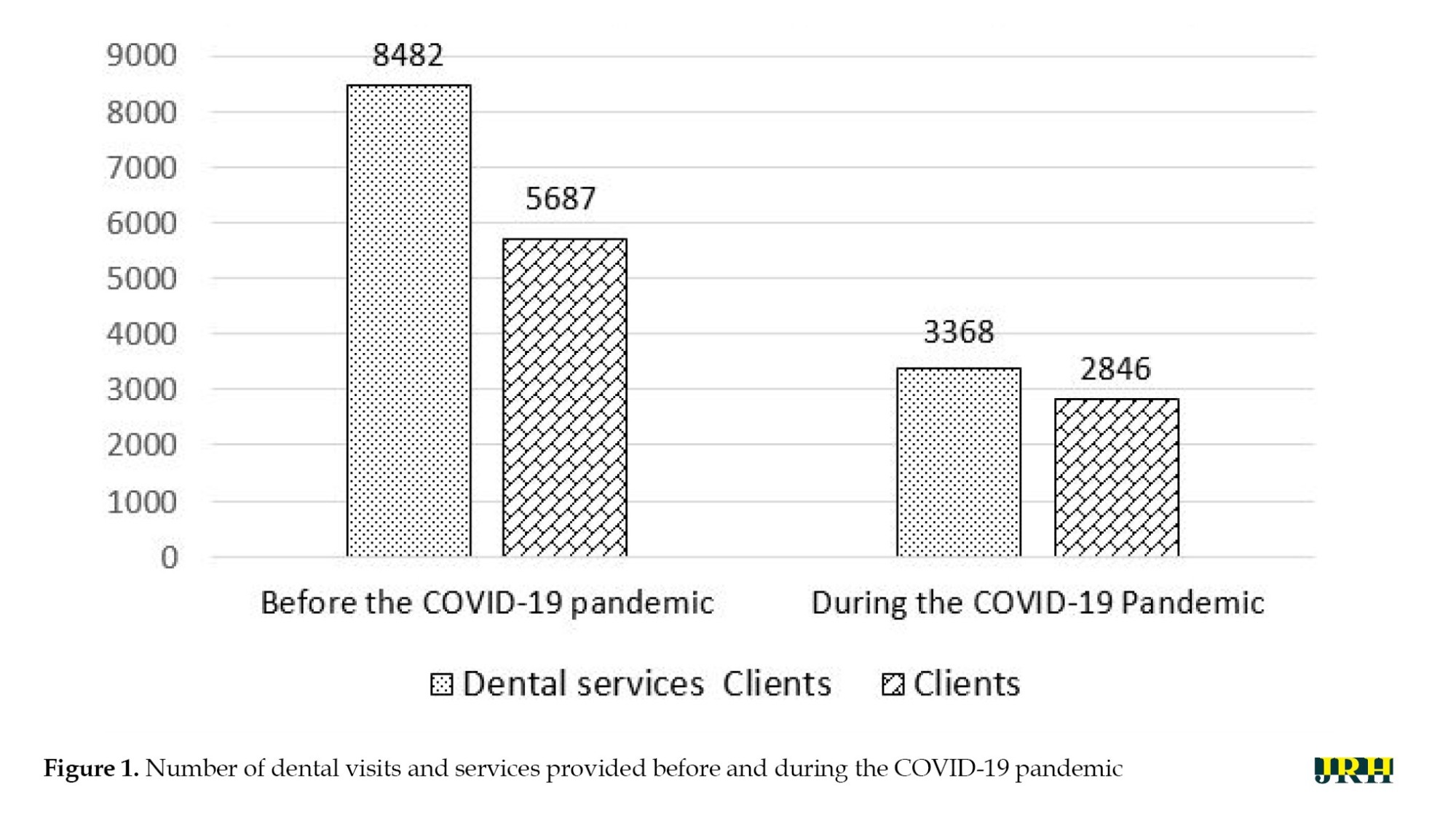
In this study, the data related to 8,533 clients (5,687 clients in the first period and 2,846 clients in the second period) and 11,850 dental care services (8,482 cases in the first period and 3,368 in the second period) were investigated over a three-month period before and during the COVID-19 pandemic (Figure 1).
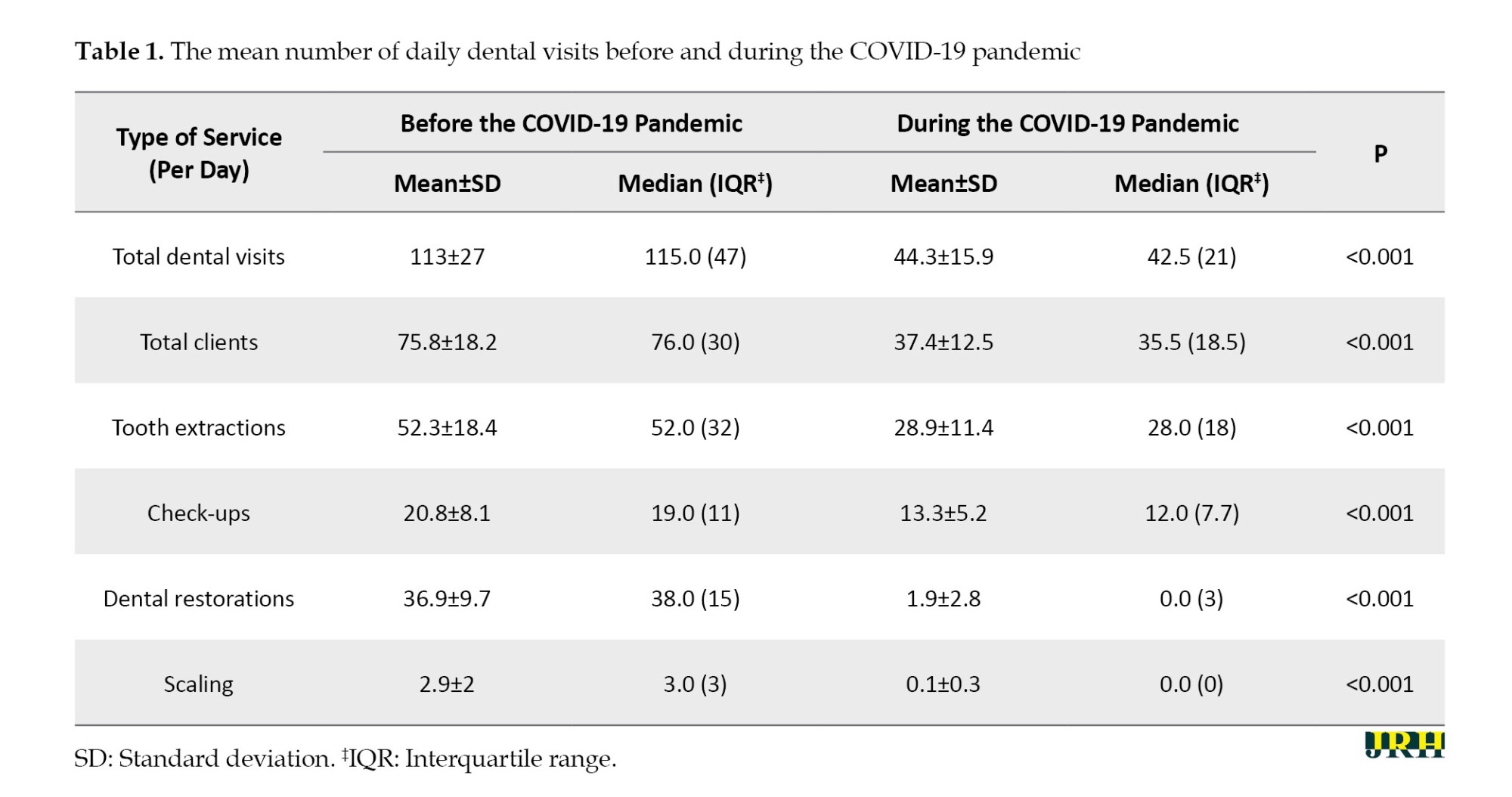
The results showed that dental visits during the COVID-19 pandemic substantially reduced compared to the period preceding it. As shown in Table 1, the mean dental visits (44.3±15.9) in the second period (during the COVID-19 pandemic) significantly reduced compared to the first period (before the COVID-19 pandemic) (113.0±27.0) (P<0.001). The mean daily cases of tooth extraction were 52.3±18.4 before the COVID-19 pandemic and 28.9±11.4 during the COVID-19 pandemic, indicating a significant reduction in the second period (P<0.001). In addition, the mean daily cases of dental restorations during the COVID-19 pandemic (1.9±2.8) significantly reduced compared to those before the COVID-19 pandemic (36.9±9.7).
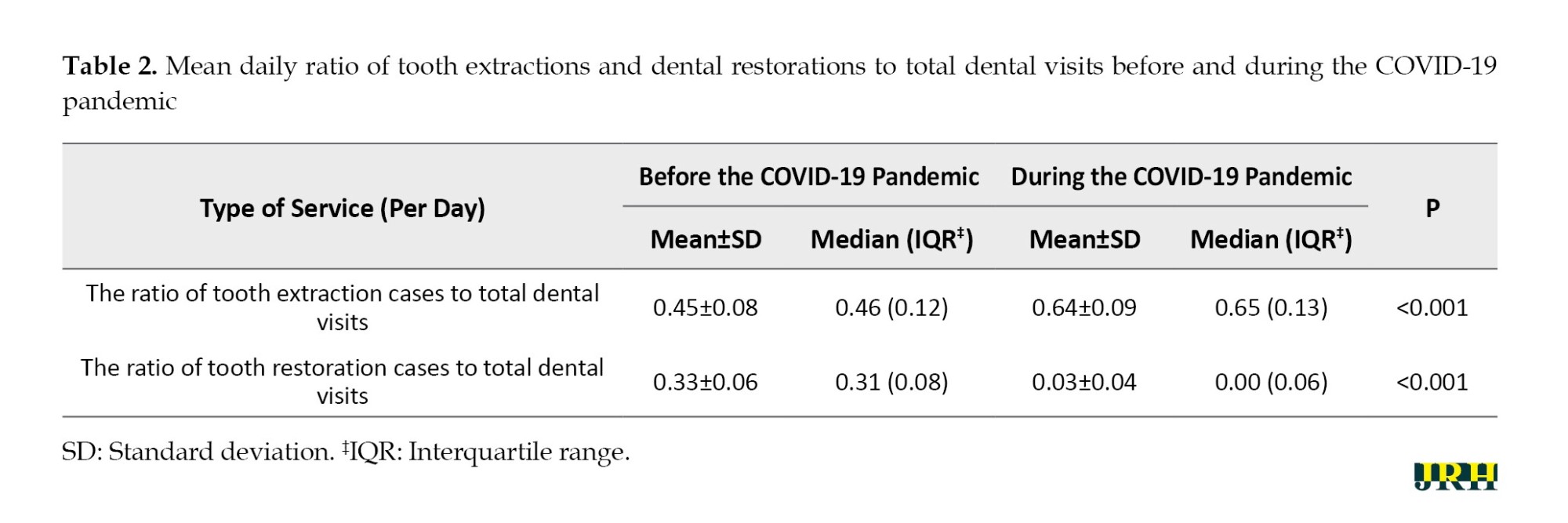
The daily ratio of tooth extraction cases to total dental visits was 0.45 in the first period and 0.64 in the second period. Before the COVID-19 pandemic, 45% of daily visits were for tooth extractions, a figure that significantly rose to 64% during the pandemic (P<0.001). On the other hand, the daily ratio of tooth restoration cases to total dental visits was 0.33 before the COVID-19 pandemic and 0.03 during the pandemic. In the initial period, 33% of daily visits were for tooth restorations, a percentage that notably dropped to 3% (Table 2).
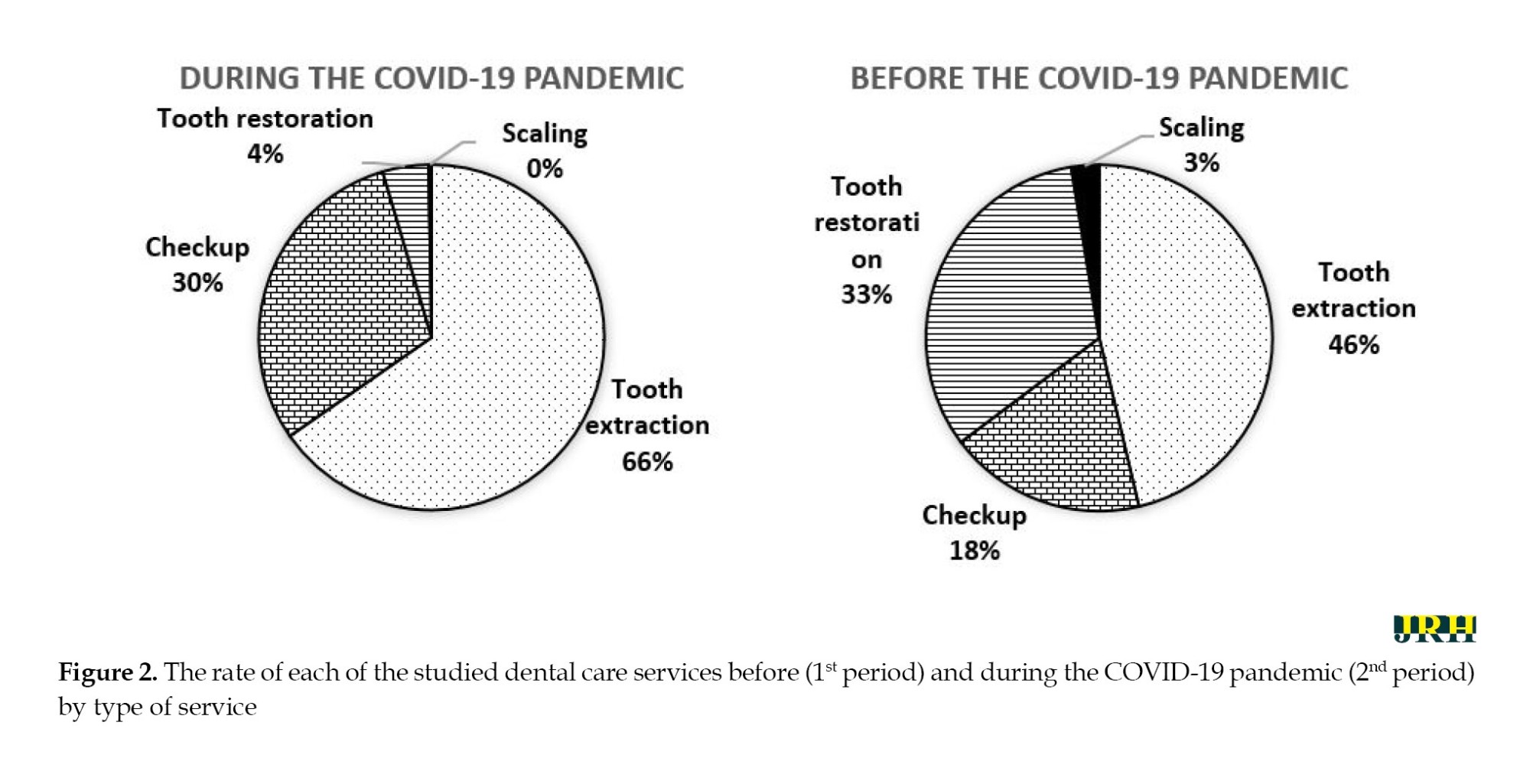
The rate of each of the studied dental care services in the two periods before and after the COVID-19 pandemic (Figure 2).
Discussion
This study showed that the frequency of visits to CHCs for dental care services substantially reduced during the COVID-19 pandemic. The notable reduction can be attributed to factors such as mandatory physical distancing measures, lockdowns implemented post-pandemic onset, and guidance from officials and health experts advocating for home quarantine and the deferral of non-emergency visits to medical facilities [20]. This finding is consistent with that of Guo et al. who reported a 38% reduction in the total number of visits for emergency dental services in China during the COVID-19 pandemic [9]. Similarly, a study in Pakistan indicated that the number of visits for dental care services significantly reduced among people aged over 50 years during the COVID-19 pandemic. This trend seems to be due to media reports emphasizing the heightened vulnerability of older individuals or those with underlying health conditions to COVID-19 [12].
Therefore, it is imperative to educate the public, particularly vulnerable populations and at-risk patients, on self-care practices and tele-dentistry approaches to uphold community oral health standards during such challenging times.
In this study, the highest frequency of dental visits during the COVID-19 pandemic was related to tooth extractions. One of the reasons why people avoid or postpone visiting CHCs is the fear of virus transmission. Existing literature also supports the trend of postponed dental appointments during the COVID-19 pandemic [21], which likely contributes to the increased demand for emergency dental services like tooth extractions. Ali et al. recommended the suspension of elective dental care services during the COVID-19 pandemic, advocating for dental care services to be limited to emergencies only with necessary precautions [22].
This study also demonstrated a significant reduction in dental visits for tooth restoration during the COVID-19 pandemic, suggesting that tooth restoration was not among the main priorities of people visiting dental care centers during this period. Consistent adherence to good oral hygiene practices can help prevent dental emergencies stemming from bacterial infections. Regular oral hygiene practices, such as tooth brushing, using mouthwash with special solutions, flossing, and reducing consumption of sticky and sweet foods, can effectively reduce the risk of dental and oral infections during the COVID-19 pandemic [23, 24].
The results also revealed a shift in treatment needs during the COVID-19 pandemic; the proportion of tooth extractions as part of total dental services significantly increased during the COVID-19 pandemic, while the proportions of check-ups, tooth restoration, and scaling decreased during the same period. One of the reasons for this issue is the delay in people’s visits due to the concerns about contracting the coronavirus and the restrictions placed on healthcare facilities during the pandemic. In other words, people have minimized visits to healthcare centers unless in emergencies, and as a result, leading to a rise in the possibility of tooth extractions. Since dental health is one of the basics of the general health of humans, the reduced proportion of consulting and restorative services and the increased proportion of more invasive services, e.g. tooth extractions raises concerns about potential long-term negative impacts on public health. Previous studies have also reported the need for changes in pediatric dental treatment needs at a specialized hospital in India [25] and changes in the spectrum of dental issues at a dental emergency service center in China [9].
Considering the uniformity of dental service packages provided by Iranian CHCs, the continuation of the existing pattern of dental visits for primary dental services can affect the oral health indicators at the regional and national levels and even reduce public health outcomes in the long term. To address this challenge, it is essential to ensure the continuous delivery of dental care services through dental professionals, mobile clinics, or teledentistry systems. Adjusting the affordability of dental services, particularly in private centers, and promoting dental self-care practices are crucial steps in mitigating the potential negative effects. Future studies are recommended to identify the age and gender patterns of dental visits and investigate the oral health status of clients to determine the priority levels for dental services. Moreover, with a potential surge in demand for dental care services post-COVID-19 pandemic, health officials and policymakers are advised to anticipate and develop programs to meet the forthcoming dental treatment needs effectively.
One of the limitations of our study was the periods selected for comparison. Due to the closure of health centers in some periods during the COVID-19 pandemic, it was not possible to select all the months before and during the COVID-19 pandemic. However, the number of active centers and dentists providing dental care services was almost the same in the two studied periods. The number of active centers before and during the pandemic was equal to 16. Moreover, the number of dentists providing dental care services was almost the same in these two periods (30 dentists before and 33 dentists during the pandemic).
As the prevalence of COVID-19 decreases, the number of dental visits may rise. Therefore, future studies are recommended to conduct surveys of Iranian families to understand the challenges faced in accessing dental care during the COVID-19 pandemic or similar crises from their perspectives.
Conclusion
With the proportion of tooth restoration decreasing and extraction increasing, it seems that the COVID-19 pandemic has caused people to postpone their visits to dental care centers, resulting in a shift in demand from restorative to more invasive services like tooth extraction. In other words, people have been avoiding non-emergency visits to healthcare facilities as much as possible. Therefore, it is necessary to take measures and develop programs to reduce unnecessary cases of tooth extraction and prevent similar cases in the future.
Ethical Considerations
Compliance with ethical guidelines
As data collection did not involve direct interaction with individuals, there was no requirement for completing informed consent forms. It is important to note that access to the data was anonymous, and information was reported in an aggregated manner, not individually. This study was approved by the Ethics Committee of Gonabad University of Medical Sciences (Code: IR.GMU.REC.1400.101).
Funding
This work was supported by Gonabad University of Medical Sciences (Grant No.: 741).
Authors' contributions
Conceptualization, methodology, data analysis, funding acquisition, resources and supervision: Roya Zamani, Reza Esmaeili and Ali Mohammad Mokhtari; Data collection: Elahe Moghimi Shahri, and Roya Zamani; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate the collaboration of the Research and Technology Deputy of Gonabad University of Medical Sciences.
References
A virus originating in Wuhan, China, was first reported in late 2019 [1] and quickly spread to other cities in China and various countries globally. The World Health Organization (WHO) named the resulting disease as COVID-19 and declared it a pandemic [2, 3]. COVID-19 cases have been reported in many countries worldwide, affecting over 768 million individuals and claiming the lives of more than 6,945,000 people as of June 2023 [4].
Although this new virus is mainly transmitted through the large nasal or oral droplets of symptomatic patients [5], it is important to note that asymptomatic patients can also spread the disease [6, 7]. Because of the rapid spread of COVID-19, people in most countries have been recommended to limit their visits to crowded places as much as possible to prevent the transmission of the virus. Additionally, the fear of contracting coronavirus, fueled by the swift spread of the disease, has influenced people’s choices regarding visiting crowded locations such as hospitals or facilities offering medical and dental services [8, 9].
Dental procedures are recognized as potential avenues for disease transmission due to contaminated equipment, as suspended particles generated by dental instruments can land on various surfaces and facilitate virus transmission [10]. Dentists and other members of dental teams involved in procedures that generate aerosols can directly transmit the virus to individuals who are not infected [11].
At the onset of the COVID-19 pandemic, dentists worldwide were recommended to limit their professional activities to emergencies only and postpone non-emergency dental treatments until there was a relative decrease in the prevalence of the disease [9]. However, this practice can lead to health consequences such as a significant increase in oral and dental infections [8, 12]. For example, the results of a study in China showed that demand for dental services dramatically declined at the onset of the COVID-19 pandemic [9]. Another study has also indicated a sharp decline in visits to emergency departments in the US during the initial month after the beginning of the COVID-19 pandemic [13].
Since the first case of COVID-19 in Iran was reported in Qom in February 2020 [14], Iran has recorded over 7 million cases of COVID-19 and more than 146,000 deaths attributed to the disease [4]. Community health centers (CHCs) within the Iran healthcare system play a crucial role in providing primary dental care services, especially for vulnerable groups, such as children, pregnant women, and the elderly [15-17]. Therefore, a significant decrease in dental visits is concerning as it can lead to adverse outcomes Due to the restrictions on private dental care centers during the COVID-19 pandemic in Iran, it is unlikely that private dental care facilities will be able to offset the decrease in dental services provided by CHCs. Moreover, given the high costs associated with dental care services provided by private centers in Iran, the increase in out-of-pocket expenses for dental care services has become a serious concern [18].
The recommendations for dentists to prioritize emergency cases and the public’s fear of contracting COVID-19 in dental settings have significantly decreased the frequency of dental visits. This reduction in visits can lead to health implications, including a shift towards more invasive procedures. Several studies in Iran have explored the decline in dental appointments following the COVID-19 pandemic [19]. Therefore, this study aims to compare dental visit frequencies before and during the pandemic and examine the effects of COVID-19 on dental care utilization patterns in the Gonabad community health centers.
Methods
This cross-sectional study was conducted on clients receiving dental services at public CHCs in Gonabad, Iran, whose information is registered in the integrated health system of Iran’s Ministry of Health and Medical Education (SIB). The COVID-19 pandemic (before and during COVID-19) was regarded as an independent variable and dental visits and services were regarded as a dependent variable (outcome variable).
The main purpose of this study was to investigate the effects of the COVID-19 pandemic on dental visits and services. Some factors that could potentially skew the results include variations in the number of operational centers during the two periods being compared, along with factors influencing the volume of visitors to these centers (such as the saffron harvest season). Therefore, in order to reduce potential biases, we tried to choose the time frames where these factors were similar. Also, we made efforts to minimize the influence of confounding variables (like the type of services offered) to enhance the comparability between the two periods. Therefore, participants across all age groups were selected from among those who visited these centers between December 2019 and January and February 2020 (pre-COVID-19 period) and between December 2020 and January and February 2021 (during the COVID-19 pandemic period).
The first case of COVID-19 in Iran was confirmed in February 2020. Due to the closure of dental centers at the onset of the pandemic, specifically from March 10, 2020, to May 30, 2020, and again from July 4, 2020, to August 22, 2020, with only elective services available to clients in specific centers (Shahid Fayyazbakhsh and Shahid Aghaei centers), the period from February to November 2020 was not considered as part of the COVID-19 pandemic period. Moreover, the timeframe from October to November was also excluded because the decrease in dental visits in this period could partly be attributed to the involvement of some individuals from Gonabad in the harvest of saffron (a significant activity in this region).
Since some health centers are less visited by people and some others are visited more and also the qualities and performance of dentists and dental healthcare professionals may vary from center to center, the required data were equally obtained from all 16 health centers affiliated with the Gonabad University of Medical Sciences.
Inclusion and exclusion criterion
The checklist used in this study included items, such as the number of clients and the number of dental care services, such as check-ups, tooth extractions, tooth restorations, and scaling, all of which are routinely documented in the SIB system. Therefore, the only inclusion criterion was receiving dental care services at the centers affiliated with the Gonabad University of Medical Sciences during the two studied periods with registered information in the SIB. The incompleteness of the information recorded in the SIB system was also regarded as an exclusion criterion.
The data were extracted from the SIB, recorded on a checklist, and inputted into SPSS software, version 22. Both descriptive and analytical statistics were used to analyze the data at a significance level of <0.05. Initially, the normality of the quantitative data was assessed, and independent-sample t-test applied to normal variables and the Mann-Whitney test used for other variables. The figures were drawn by the SigmaPlot software, version 11.
Results
In this study, the data related to 8,533 clients (5,687 clients in the first period and 2,846 clients in the second period) and 11,850 dental care services (8,482 cases in the first period and 3,368 in the second period) were investigated over a three-month period before and during the COVID-19 pandemic (Figure 1).
The results showed that dental visits during the COVID-19 pandemic substantially reduced compared to the period preceding it. As shown in Table 1, the mean dental visits (44.3±15.9) in the second period (during the COVID-19 pandemic) significantly reduced compared to the first period (before the COVID-19 pandemic) (113.0±27.0) (P<0.001). The mean daily cases of tooth extraction were 52.3±18.4 before the COVID-19 pandemic and 28.9±11.4 during the COVID-19 pandemic, indicating a significant reduction in the second period (P<0.001). In addition, the mean daily cases of dental restorations during the COVID-19 pandemic (1.9±2.8) significantly reduced compared to those before the COVID-19 pandemic (36.9±9.7).
The daily ratio of tooth extraction cases to total dental visits was 0.45 in the first period and 0.64 in the second period. Before the COVID-19 pandemic, 45% of daily visits were for tooth extractions, a figure that significantly rose to 64% during the pandemic (P<0.001). On the other hand, the daily ratio of tooth restoration cases to total dental visits was 0.33 before the COVID-19 pandemic and 0.03 during the pandemic. In the initial period, 33% of daily visits were for tooth restorations, a percentage that notably dropped to 3% (Table 2).
The rate of each of the studied dental care services in the two periods before and after the COVID-19 pandemic (Figure 2).
Discussion
This study showed that the frequency of visits to CHCs for dental care services substantially reduced during the COVID-19 pandemic. The notable reduction can be attributed to factors such as mandatory physical distancing measures, lockdowns implemented post-pandemic onset, and guidance from officials and health experts advocating for home quarantine and the deferral of non-emergency visits to medical facilities [20]. This finding is consistent with that of Guo et al. who reported a 38% reduction in the total number of visits for emergency dental services in China during the COVID-19 pandemic [9]. Similarly, a study in Pakistan indicated that the number of visits for dental care services significantly reduced among people aged over 50 years during the COVID-19 pandemic. This trend seems to be due to media reports emphasizing the heightened vulnerability of older individuals or those with underlying health conditions to COVID-19 [12].
Therefore, it is imperative to educate the public, particularly vulnerable populations and at-risk patients, on self-care practices and tele-dentistry approaches to uphold community oral health standards during such challenging times.
In this study, the highest frequency of dental visits during the COVID-19 pandemic was related to tooth extractions. One of the reasons why people avoid or postpone visiting CHCs is the fear of virus transmission. Existing literature also supports the trend of postponed dental appointments during the COVID-19 pandemic [21], which likely contributes to the increased demand for emergency dental services like tooth extractions. Ali et al. recommended the suspension of elective dental care services during the COVID-19 pandemic, advocating for dental care services to be limited to emergencies only with necessary precautions [22].
This study also demonstrated a significant reduction in dental visits for tooth restoration during the COVID-19 pandemic, suggesting that tooth restoration was not among the main priorities of people visiting dental care centers during this period. Consistent adherence to good oral hygiene practices can help prevent dental emergencies stemming from bacterial infections. Regular oral hygiene practices, such as tooth brushing, using mouthwash with special solutions, flossing, and reducing consumption of sticky and sweet foods, can effectively reduce the risk of dental and oral infections during the COVID-19 pandemic [23, 24].
The results also revealed a shift in treatment needs during the COVID-19 pandemic; the proportion of tooth extractions as part of total dental services significantly increased during the COVID-19 pandemic, while the proportions of check-ups, tooth restoration, and scaling decreased during the same period. One of the reasons for this issue is the delay in people’s visits due to the concerns about contracting the coronavirus and the restrictions placed on healthcare facilities during the pandemic. In other words, people have minimized visits to healthcare centers unless in emergencies, and as a result, leading to a rise in the possibility of tooth extractions. Since dental health is one of the basics of the general health of humans, the reduced proportion of consulting and restorative services and the increased proportion of more invasive services, e.g. tooth extractions raises concerns about potential long-term negative impacts on public health. Previous studies have also reported the need for changes in pediatric dental treatment needs at a specialized hospital in India [25] and changes in the spectrum of dental issues at a dental emergency service center in China [9].
Considering the uniformity of dental service packages provided by Iranian CHCs, the continuation of the existing pattern of dental visits for primary dental services can affect the oral health indicators at the regional and national levels and even reduce public health outcomes in the long term. To address this challenge, it is essential to ensure the continuous delivery of dental care services through dental professionals, mobile clinics, or teledentistry systems. Adjusting the affordability of dental services, particularly in private centers, and promoting dental self-care practices are crucial steps in mitigating the potential negative effects. Future studies are recommended to identify the age and gender patterns of dental visits and investigate the oral health status of clients to determine the priority levels for dental services. Moreover, with a potential surge in demand for dental care services post-COVID-19 pandemic, health officials and policymakers are advised to anticipate and develop programs to meet the forthcoming dental treatment needs effectively.
One of the limitations of our study was the periods selected for comparison. Due to the closure of health centers in some periods during the COVID-19 pandemic, it was not possible to select all the months before and during the COVID-19 pandemic. However, the number of active centers and dentists providing dental care services was almost the same in the two studied periods. The number of active centers before and during the pandemic was equal to 16. Moreover, the number of dentists providing dental care services was almost the same in these two periods (30 dentists before and 33 dentists during the pandemic).
As the prevalence of COVID-19 decreases, the number of dental visits may rise. Therefore, future studies are recommended to conduct surveys of Iranian families to understand the challenges faced in accessing dental care during the COVID-19 pandemic or similar crises from their perspectives.
Conclusion
With the proportion of tooth restoration decreasing and extraction increasing, it seems that the COVID-19 pandemic has caused people to postpone their visits to dental care centers, resulting in a shift in demand from restorative to more invasive services like tooth extraction. In other words, people have been avoiding non-emergency visits to healthcare facilities as much as possible. Therefore, it is necessary to take measures and develop programs to reduce unnecessary cases of tooth extraction and prevent similar cases in the future.
Ethical Considerations
Compliance with ethical guidelines
As data collection did not involve direct interaction with individuals, there was no requirement for completing informed consent forms. It is important to note that access to the data was anonymous, and information was reported in an aggregated manner, not individually. This study was approved by the Ethics Committee of Gonabad University of Medical Sciences (Code: IR.GMU.REC.1400.101).
Funding
This work was supported by Gonabad University of Medical Sciences (Grant No.: 741).
Authors' contributions
Conceptualization, methodology, data analysis, funding acquisition, resources and supervision: Roya Zamani, Reza Esmaeili and Ali Mohammad Mokhtari; Data collection: Elahe Moghimi Shahri, and Roya Zamani; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate the collaboration of the Research and Technology Deputy of Gonabad University of Medical Sciences.
References
- Chhikara BS, Rathi B, Singh J, Poonam FN. Corona virus SARS-CoV-2 disease COVID-19: Infection, prevention and clinical advances of the prospective chemical drug therapeutics. Chemical Biology Letters. 2020; 7(1):63-72. [Link]
- Mokhtari AM, Susan Dewey R, Mirahmadizadeh A. The global challenges of controlling coronavirus disease 2019: A review study. Journal of Health Sciences & Surveillance System. 2021; 9(3):142-8. [DOI:10.30476/jhsss.2021.90136.1179]
- Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Bio-Medica. 2020; 91(1):157-60. [DOI:10.23750/abm.v91i1.9397] [PMID] [PMCID]
- World Health Organization (WHO).WHO COVID-19 dashboard [Internet]. 2023 [Updated 2023 June 21]. Available from: [Link]
- Morawska L, Tang JW, Bahnfleth W, Bluyssen PM, Boerstra A, Buonanno G, et al. How can airborne transmission of COVID-19 indoors be minimised? Environment International. 2020; 142:105832. [DOI:10.1016/j.envint.2020.105832] [PMID] [PMCID]
- Bi Q, Wu Y, Mei S, Ye C, Zou X, Zhang Z, et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: A retrospective cohort study. The Lancet. Infectious Diseases. 2020; 20(8):911-9. [DOI:10.1016/S1473-3099(20)30287-5] [PMID]
- Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. The New England Journal of Medicine. 2020; 382(12):1177-9. [DOI:10.1056/NEJMc2001737] [PMID] [PMCID]
- Kumar AK, Aluru S, Sravanthi G, Narahari S, Shaik MI, Reddy NRR. Implications of covid-19 pandemic outbreak on dental emergencies. Journal of Critical Reviews. 2020; 7(10):358-61. [DOI:10.31838/jcr.07.10.75]
- Guo H, Zhou Y, Liu X, Tan J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. Journal of Dental Sciences. 2020; 15(4):564-7. [DOI:10.1016/j.jds.2020.02.002] [PMID] [PMCID]
- Harrel SK, Molinari J. Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. Journal of the American Dental Association. 2004; 135(4):429-37. [DOI:10.14219/jada.archive.2004.0207] [PMID] [PMCID]
- Sabino-Silva R, Jardim ACG, Siqueira WL. Coronavirus COVID-19 impacts to dentistry and potential salivary diagnosis. Clinical oral Investigations. 2020; 24(4):1619-21. [DOI:10.1007/s00784-020-03248-x] [PMID] [PMCID]
- Akhtar Q, Mahmood K, Qayyum U, Rana NA, Sajjad HQ, Naeem A. Impact of COVID-19 on utilization of dental services by patients visiting tertiary care dental centre Lahore. Pakistan Armed Forces Medical Journal. 2020; 70(2):S560-64. [Link]
- Hartnett KP, Kite-Powell A, DeVies J, Coletta MA, Boehmer TK, Adjemian J, et al. Impact of the COVID-19 pandemic on emergency department visits -United States, January 1, 2019-May 30, 2020. MMWR. Morbidity and Mortality Weekly Report. 2020; 69(23):699-704. [DOI:10.15585/mmwr.mm6923e1] [PMID] [PMCID]
- Abdi M. Coronavirus disease 2019 (COVID-19) outbreak in Iran: Actions and problems. Infection Control and Hospital Epidemiology. 2020; 41(6):754-5. [DOI:10.1017/ice.2020.86] [PMID] [PMCID]
- Bayat F. A model of basic dental care service for Iran. Journal of Dental School, Shahid Beheshti University of Medical Sciences. 2018; 36(1):1-6. [Link]
- Khoshnevisan M, Ghasemianpour M, Samadzadeh H, Baez RJ. Oral health status and healthcare system in IR Iran. Journal of Contemporary Medical Sciences. 2018; 4(3):107-18. [Link]
- Pakshir HR. Oral health in Iran. International Dental Journal. 2004; 54(6 Suppl 1):367-72. [DOI:10.1111/j.1875-595X.2004.tb00013.x] [PMID]
- Rezaei S, Pulok MH, Zahirian Moghadam T, Zandian H. Socioeconomic-related inequalities in dental care utilization in northwestern Iran. Clinical, Cosmetic and Investigational Dentistry. 2020; 12:181-9. [DOI:10.2147/CCIDE.S253242] [PMID] [PMCID]
- Khami MR, Gholamhossein Zadeh A, Rahi D. A cross-sectional study on COVID-19-related changes in self-medication with antibiotics. Plos One. 2022; 17(6):e0269782. [DOI:10.1371/journal.pone.0269782] [PMID] [PMCID]
- Abdi M, Mirzaei R. Iran without mandatory quarantine and with social distancing strategy against coronavirus disease (COVID-19). Health Security. 2020; 18(3):257-9. [DOI:10.1089/hs.2020.0041] [PMID]
- Shamsoddin E, DeTora LM, Tovani-Palone MR, Bierer BE. Dental care in times of the COVID-19 pandemic: A review. Medical Sciences. 2021; 9(1):13. [DOI:10.3390/medsci9010013] [PMID] [PMCID]
- Ali S, Zeb U, Khan M, Muhammad A. Transmission routes and infection control of novel Coronavirus-2019 in dental clinics-a review. Journal of Islamabad Medical & Dental College. 2020; 9(1):65-72. [DOI:10.35787/jimdc.v9i1.517]
- Ashok N, Rodrigues JC, Azouni K, Darwish S, Abuderman A, Alkaabba AA, et al. Knowledge and apprehension of dental patients about MERS-A questionnaire survey. Journal of Clinical and Diagnostic Research. 2016; 10(5):ZC58-62. [DOI:10.7860/JCDR/2016/17519.7790] [PMID] [PMCID]
- Tramini P, Al Qadi Nassar B, Valcarcel J, Gibert P. Factors associated with the use of emergency dental care facilities in a French public hospital. Special Care in Dentistry. 2010; 30(2):66-71. [DOI:10.1111/j.1754-4505.2009.00125.x] [PMID]
- Nandlal B, Singh B, Gopi A. Impact on utilization and shift in treatment needs post-COVID lockdown of pediatric dentistry in a tertiary care hospital. Frontiers in Dental Medicine. 2021; 2:722292. [Link]
Type of Study: Orginal Article |
Subject:
● Health Systems
Received: 2023/11/22 | Accepted: 2024/04/21 | Published: 2024/09/1
Received: 2023/11/22 | Accepted: 2024/04/21 | Published: 2024/09/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
