

Volume 14, Issue 5 (Sep & Oct 2024)
J Research Health 2024, 14(5): 405-416 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Basuki R, Latief H, Bashori K, Sagiran S, Suud F M, Pranata S. The Scientific and Islamic Perspectives to Prevent the Incidence of Dementia Among Elderly. J Research Health 2024; 14 (5) :405-416
URL: http://jrh.gmu.ac.ir/article-1-2499-en.html
URL: http://jrh.gmu.ac.ir/article-1-2499-en.html
Rochman Basuki1 

 , Hilman Latief2 , Khoiruddin Bashori3 , Sagiran Sagiran4 , Fitriah M. Suud2 , Satriya Pranata5
, Hilman Latief2 , Khoiruddin Bashori3 , Sagiran Sagiran4 , Fitriah M. Suud2 , Satriya Pranata5
, Hilman Latief2 , Khoiruddin Bashori3 , Sagiran Sagiran4 , Fitriah M. Suud2 , Satriya Pranata5
1- Department of Islamic Education Psychology, Universitas Muhammadiyah Yogyakarta, Yogyakarta, Indonesia. , rochmanbasuki79@gmail.com
2- Department of Islamic Education Psychology, Universitas Muhammadiyah Yogyakarta, Yogyakarta, Indonesia.
3- Department of Psychology Professional Education, Universitas Ahmad Dahlan, Yogyakarta, Indonesia.
4- Department of Medicine, Faculty of Medical, Universitas Muhammadiyah Semarang, Semarang, Indonesia.
5- Department of Nursing, Faculty of Nursing and Health Sciences, Universitas Muhammadiyah Semarang, Semarang, Indonesia.
2- Department of Islamic Education Psychology, Universitas Muhammadiyah Yogyakarta, Yogyakarta, Indonesia.
3- Department of Psychology Professional Education, Universitas Ahmad Dahlan, Yogyakarta, Indonesia.
4- Department of Medicine, Faculty of Medical, Universitas Muhammadiyah Semarang, Semarang, Indonesia.
5- Department of Nursing, Faculty of Nursing and Health Sciences, Universitas Muhammadiyah Semarang, Semarang, Indonesia.
Full-Text [PDF 764 kb]
(1077 Downloads)
| Abstract (HTML) (4008 Views)
Full-Text: (1538 Views)
Introduction
Dementia is a common health problem in society. It is characterized by multiple and progressive cognitive impairments, including memory impairment that interferes with independence, and social or occupational functioning that interferes with daily activities. This leads to disability and dependency in the elderly and is, most importantly, a source of distress for affected individuals, their families, and caregivers [1]. With the projected growth trend of the aging population, the number of people with dementia is expected to increase. Worldwide, at least 57.4 million people live with dementia and 1.6 million people die each year from the condition. Although the proportion of the global population aged ≥65 years will double between 2019 and 2050, the prevalence of dementia and Alzheimer's disease (AD), which account for 60–70% of dementia, is expected to reach 152.8 million and 106.4 million people, respectively [2].
In the Qur'an, older age is called the lowest stage of life, because it is accompanied by forgetting past knowledge and experiences. "And among you, is he who is returned to the most elderly so that he does not know anything, after (once having) knowledge," (Qs. Al-Hajj/22: 5). Science refers to this condition as “dementia,” which results from the progressive degeneration of the nerve cell network related to cognitive function [3]. Moreover, the elderly population in the future may face various obstacles in their basic needs and health problems due to dementia. This is the reason why dementia should be a very important concern given by health professionals and the government of countries. These health problems and basic needs include environmental and sociocultural factors and nutritional intake. More attention is needed to address the conditions faced by the elderly population due to dementia; both the general public and health professionals must have a solid understanding of modifiable factors to prevent these conditions. This is the first step toward changing behavior. Unfortunately, public knowledge about risk factors for dementia remains poor and lags behind their knowledge about the risk factors for other common diseases, such as cardiovascular disease (CVD). Understanding the risk factors for its early prevention and treatment [4].
Prevention is a key strategy in combating dementia. A 2020 Lancet commission estimated that 40% of dementia cases could be prevented by addressing medical and lifestyle risk mediators. With increasing evidence of the efficacy of risk reduction, there has been a global policy shift, led by the World Health Organization (WHO) and others, toward the prevention of dementia through risk factor modification [5].
Recently, findings by Hosseini et al. indicated that religious and spiritual involvement is important in protecting middle-aged and elderly groups against cognitive decline. Most of the literature supports a positive relationship between religious and spiritual involvement and cognitive functioning. This can be explained by various aspects of religious activities that involve continuous stimulation of the brain, such as reciting the Qur’an, focusing during prayers, and engaging in motor functions through a series of repetitive activities [6].
Based on the information above, this research reviewed what are the risk factors for dementia as a basis for integrating dementia prevention from scientific and Islamic perspectives. Information about factors that can contribute to preventing dementia can provide valuable insights for health professionals in combining scientific and Islamic approaches simultaneously.
Methods
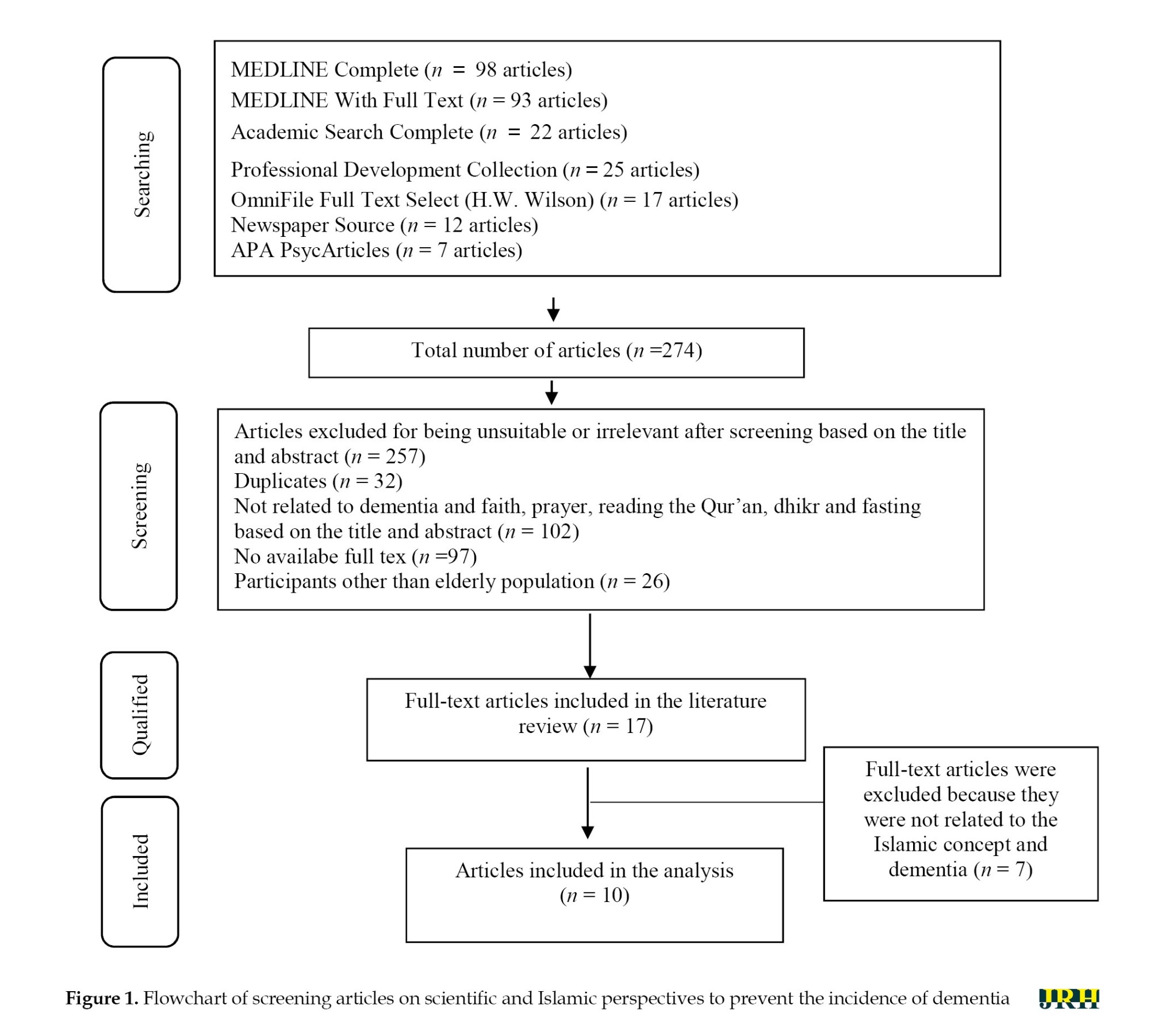
This research employed a comprehensive literature review strategy, which included searching for articles in research journal databases, conducting Internet searches, and reviewing relevant articles. Databases, including MEDLINE Complete, MEDLINE With Full Text, Academic Search Complete, Professional Development Collection, OmniFile Full Text Select (H.W. Wilson), Newspaper Source, and APA PsycArticles were searched using the keywords, namely“dementia,” “faith,” “prayer,” “reading the Qur’an,” “dhikr,” and “fasting” in the title. Additionally, the Qur’an and books related to dementia were included as supplementary literature.
The following inclusion criteria were applied: Publication dates from 2019 to 2023 (the last 5 years), original research types, accessible full texts, and studies related to factors in preventing dementia among the elderly population through Islamic and scientific approaches. The authors coded, extracted, and combined the data separately, and then, established a final consensus following discussion. All authors who reviewed the papers were experts in the study field. A total of 274 articles were obtained, but only 17 qualified. After a detailed review, 10 articles were included in the analysis. The articles used as samples were then identified and summarized based on the themes that emerged, as presented in Figure 1.
Results
Based on the results of the literature study (Table 1), the risk factors for dementia from a scientific perspective included non-modifiable risk factors (age, gender, and genetics) and modifiable risk factors (cardiovascular disease, hypertension, diabetics, smoking habit, alcohol consumption, head injury, stress, education, physical activity, obesity, and sleep disorder).
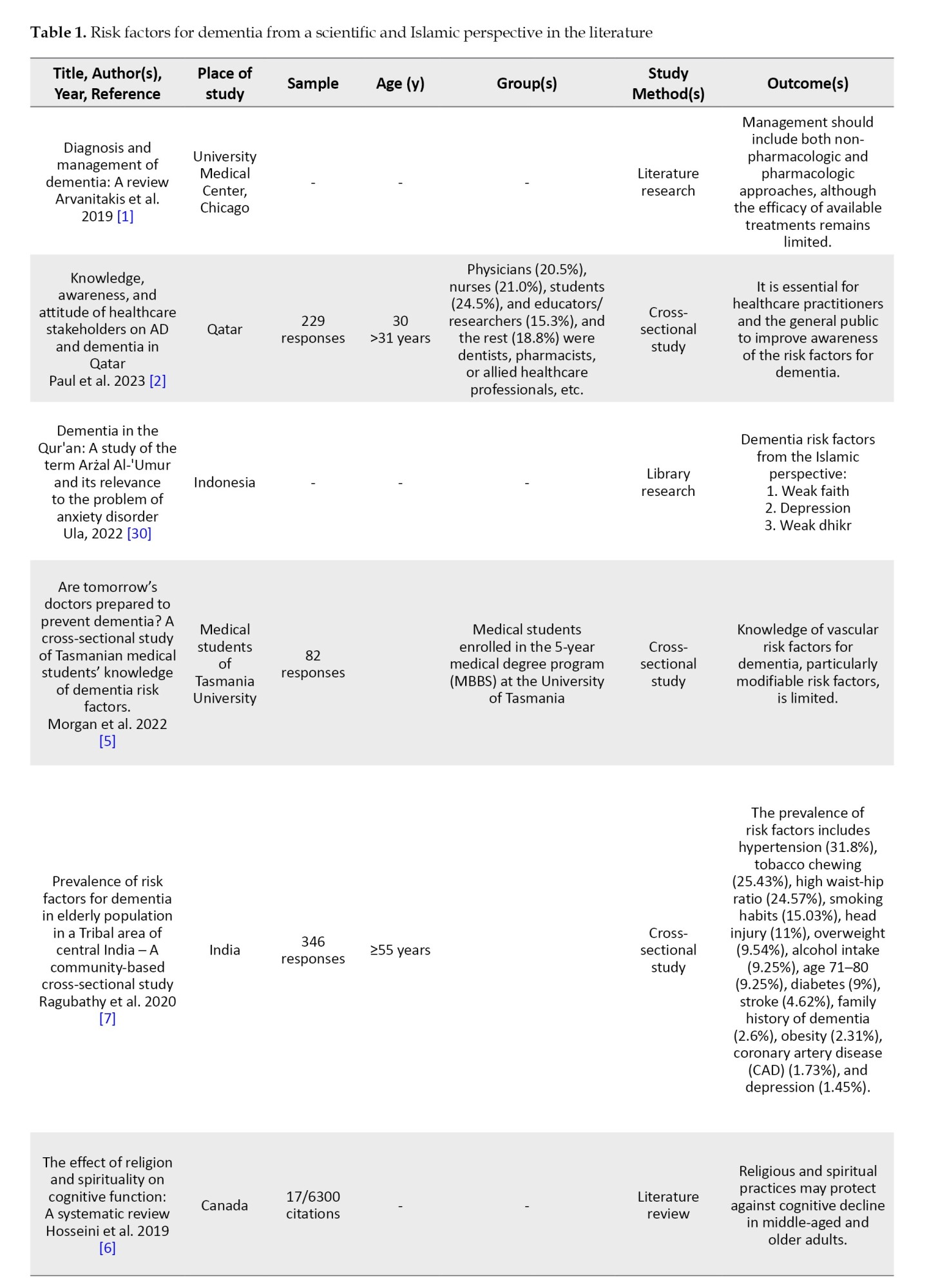
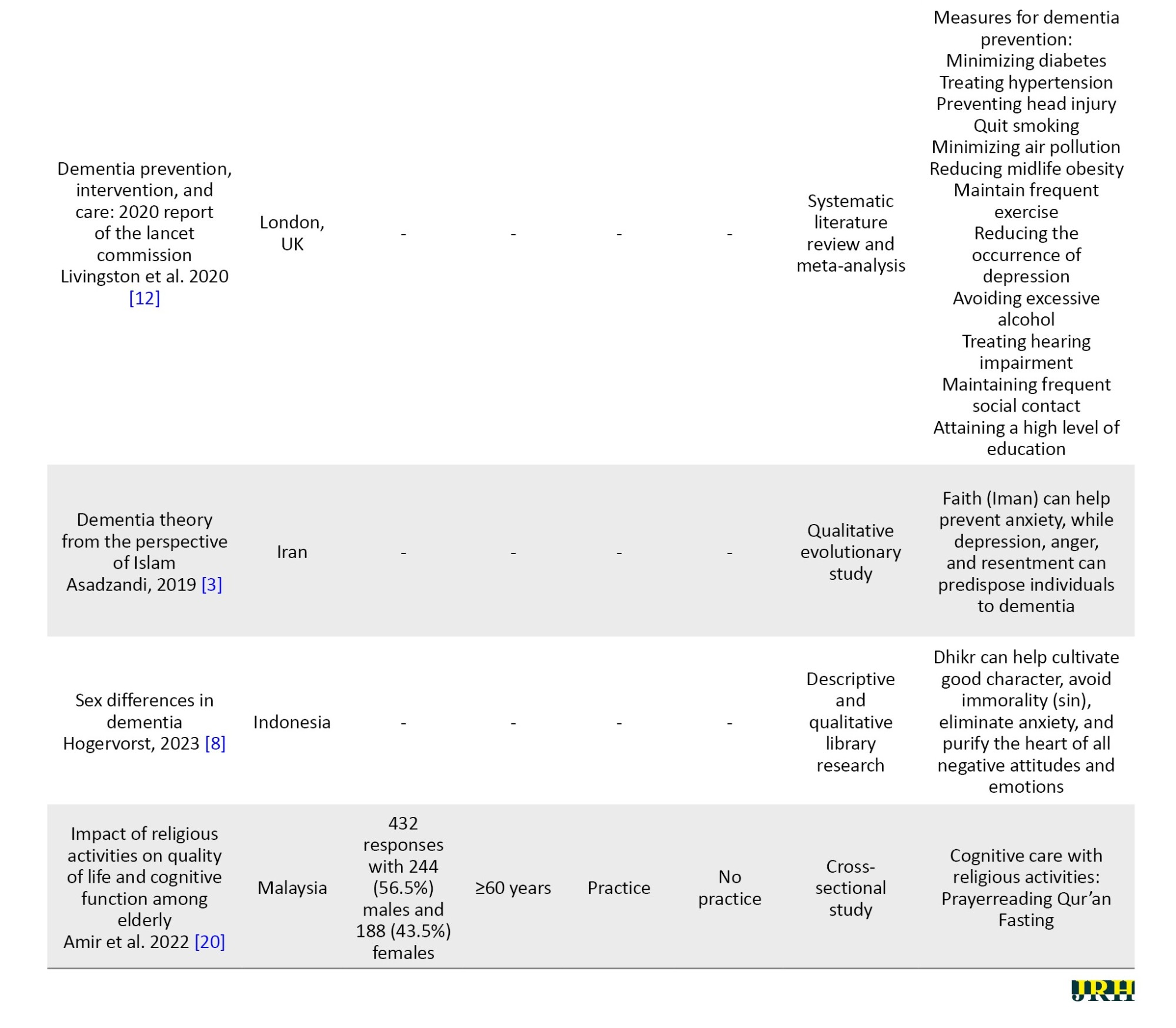
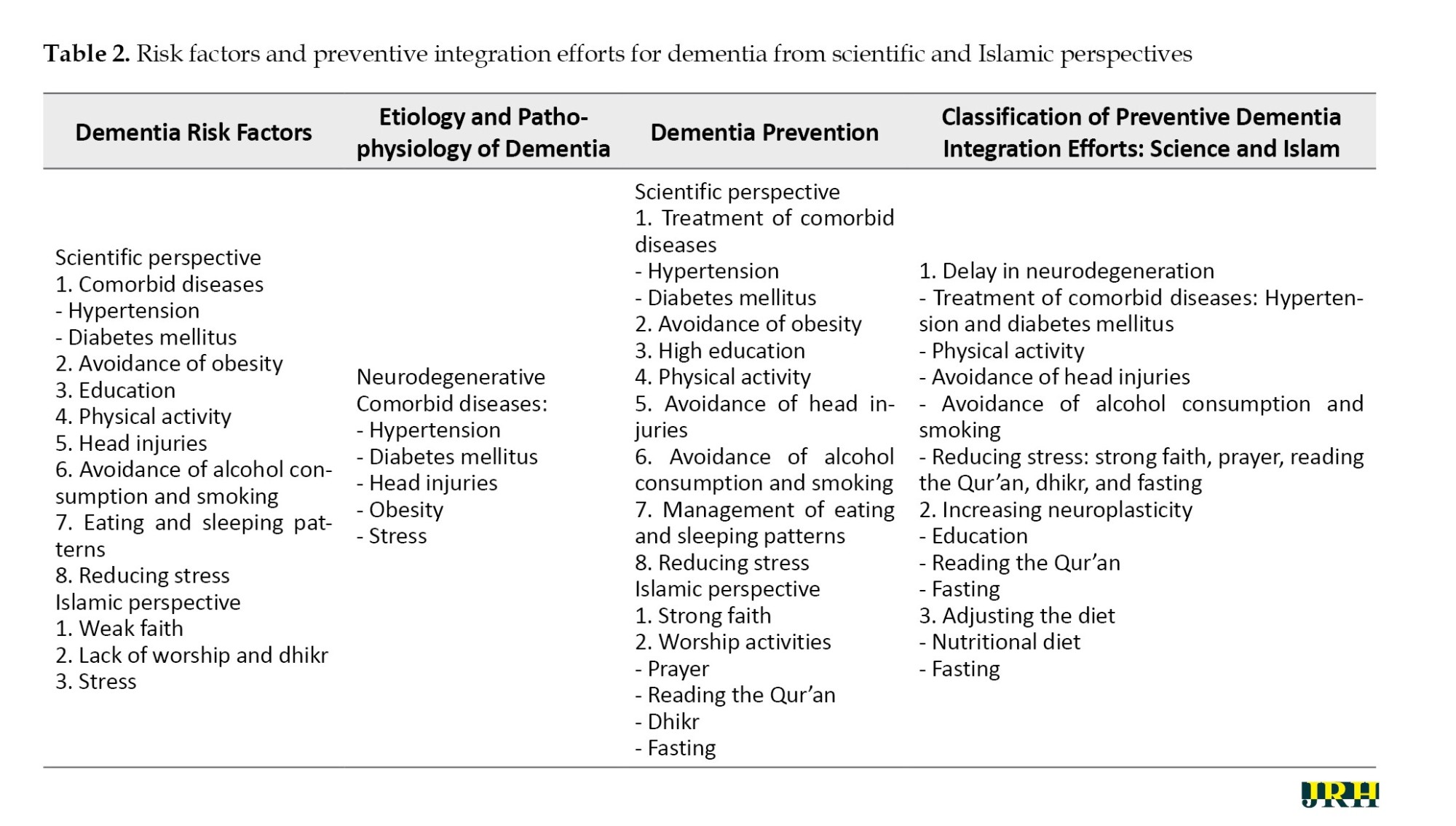
Moreover, the risk factors for dementia from an Islamic perspective were faith/belief, practicing religious activities, reading the Al-Qur’an, performing prayer, dhikr, and fasting. Moreover, the integration of risk factors and preventive efforts for dementia from both scientific and Islamic perspectives is presented in Table 2.
From Table 2, it can be seen that the efforts to prevent dementia from both scientific and Islamic perspectives focus on delaying neurodegeneration through the treatment of comorbid diseases (hypertension and diabetes mellitus), promoting physical activity, avoiding head injuries, refraining from alcohol and tobacco consumption, and reducing stress through strong faith, prayer, reading the Qur’an, dhikr, and fasting.
Discussion
Research on scientific and Islamic perspectives as an effort to prevent the incidence of dementia among the elderly population has been frequent; however, the two approaches tend to be treated separately. This research demonstrates that the two approaches are interconnected. In the following paragraph, we will separate these factors into scientific and Islamic categories, and then combine the results for discussion to highlight the novelty of the study. The relationship between the two approaches is illustrated below.
Dementia risk factors from the scientific perspective
Risk factors for dementia can be divided into two categories: Modifiable and non-modifiable risk factors. Non-modifiable risk factors include age, gender, and genetics. The prevalence of dementia increases with age, as observed in clinical settings and population studies. Some declines in bodily functions due to aging are linked to the incidence of dementia [7]. Research conducted by Hogervorst et al. found no relationship between gender and the incidence of dementia, although some studies indicate that women are more likely to have detectable dementia [8]. The most important genetic risk factor is apolipoprotein E (APOE) in late-onset AD, which is consistently identified as the greatest contributor in AD association studies. The APOE e4 allele is associated with an increased risk of late-onset AD, while the APOE e2 allele with a reduced risk. However, the APOE e4 allele does not always cause dementia [9].
Modifiable risk factors include chronic disease, health behavior, head injury, stress, and education. Heart disease is an increasing problem, resulting in vascular insufficiency that has the potential to disrupt the function of other organs, including the brain. A growing body of literature implicates heart disease as a risk factor for dementia. Additionally, several studies have shown that cardiovascular risk factors are independently associated with the development of dementia [10]. Hypertension in middle age and old age is a significant risk factor for the development of vascular dementia in later life. Damage to brain matter, along with cognitive impairment, is associated with long-term hypertensive status. Hypertension is significantly associated with an increased incidence of dementia among men [11]. Both middle-aged hypertension and late-life hypertension are significant risk factors for the development of vascular dementia in older adults. Thus, tight blood pressure control, including during sleep, can have a neuroprotective effect on the brain, and the administration of antihypertensive drugs can prevent the onset of dementia [12]. The development of chronic complications of diabetes mellitus is the excess production of superoxide anion. Intracellular hyperglycemia activates all the main pathways of chronic complications: The polyol pathway, increased hexosamine activity, activation of protein kinase C, formation of advanced glycosylation end products, oxidative stress, apoptosis, inflammation, and the expression and action of hormones, growth factors, cytokines, and inflammatory mediators. In general, diabetes mellitus has been associated with cognitive decline, especially in the elderly, leading to the emergence of cognitive impairment, and an increased risk of developing dementia, including AD and vascular dementia [13]. Diabetes is a risk factor for dementia. Untreated diabetes is a risk factor for dementia. One meta-analysis of diabetes cohort studies reported that, cross-sectionally, people with diabetes who took anti-diabetic drugs had a lower prevalence of cognitive impairment and a reduced incidence of dementia [14].
A meta-analysis of more than 37 studies was conducted to assess the correlation between smoking and dementia. It is established that smokers show an increased risk of dementia, and quitting smoking can reduce this risk. The habit of smoking in middle age has a much stronger impact on the risk of cognitive impairment in old age. Additionally, smoking in old age further increases the occurrence of dementia [15]. Heavy alcohol consumption may be associated with an increased risk of dementia in patients with mild cognitive impairment or in men carrying the APOE e4 allele. In contrast, light-moderate alcohol consumption may be associated with a reduced risk of dementia in elderly patients with mild cognitive impairment. Heavy drinkers have a higher risk of dementia than abstainers and light drinkers [7]. Regular drinking in midlife has a much stronger impact than individual factors on the risk of cognitive impairment in late life [16].
A meta-analysis of more than 37 studies was conducted to assess the correlation between smoking and dementia. It was determined that smokers showed an increased risk of dementia, and quitting smoking reduced the risk of smoking cessation. The increased risk of AD from smoking is more pronounced in APOE e4 noncarriers. Habitual smoking and regular alcohol consumption in middle age have a much stronger impact than individual factors on the risk of cognitive impairment in late life [12]. Heavy alcohol consumption may be associated with an increased risk of dementia in patients with mild cognitive impairment or men carrying the APOE e4 allele. In contrast, light to moderate alcohol consumption may be associated with a reduced risk of dementia in elderly patients with mild cognitive impairment. Heavy drinkers have a higher risk of dementia than abstainers and light drinkers [11].
This is a difficult time for people with concerns about the long-term neurological effects of head injuries. Increasing evidence links traumatic brain injuries (TBIs) to neurodegenerative diseases and dementia [17]. Many high-profile diagnoses of chronic traumatic encephalopathy (CTE), specifically post-traumatic dementia, have been made post-mortem, contributing to general anxiety about the long-term effects of even mild injuries [18]. The international classification of disease (ICD) defines mild TBI as a concussion, and severe TBI as a skull fracture, edema, brain injury, or hemorrhage. TBI is associated with a higher risk of increased incidence of dementia after six months compared to individuals who did not experience a TBI [12].
Depression is a key comorbid risk factor for dementia. Experiencing period-specific psychological distress throughout life can influence cognitive health. When the physiological stress response is triggered, the activity of the hypothalamic-pituitary-adrenal axis fosters excessive cortisol production, potentially leading to hippocampal damage. Thus, the stress response may influence cognitive function and the risk of dementia [19].
The negative impact of chronic stress on cognition can be significant, and interventions controlling stress levels provide benefits for dementia prevention. Supporting this idea, regular religious activities can improve the cognitive function of healthy individuals. Faith has been shown to delay age-related declines in cognitive function and improve some neuropsychological outcomes in subjects with mild cognitive impairment [20].
Psychological distress, such as feelings of anxiety, depression, irritability, and reactions to external stressors in a person's daily life, is associated with an increased risk of dementia. Stress can have severe and dangerous consequences not only for our brain health but also for our health in general. We can go further in dementia prevention by addressing psychological risk factors for dementia [19].
Bahiroh et al. indicated that people with lower education levels have a higher chance of having undetected dementia. This finding is supported by many studies showing that people with more education tend to perform better, making early signs of dementia more difficult to detect on standard tests because they do not reach the threshold required for detectable dementia [21]. Low education is a risk factor for accelerating memory decline and the occurrence of dementia, with the impact being more pronounced as one age. A child’s higher education level and greater lifetime educational attainment reduce the risk of dementia. New jobs can improve overall cognitive abilities, and education during late adolescence when the brain reaches its greatest plasticity. This suggests that cognitive stimulation is more important during youth [12].
Najar et al. showed that physical activity in midlife was independently associated with a reduced risk of dementia and its subtypes. They showed that these midlife activities play a role in maintaining cognitive health in old age [22]. Regular physical exercise seems to be one of the effective methods to reduce the risk of dementia among all lifestyle changes that have been studied. Several studies on the effects of aerobic exercise (exercise that increases heart rate) in middle-aged or older adults have found improvements in thinking and memory, as well as reduced rates of dementia [23].
The study of physical activity is complex. Physical activity patterns are influenced by age, generation, morbidity and gender, and social and cultural factors. Research shows an association between physical activity and a potential reduction in the risk of dementia. Individuals who do not enjoy exercising may experience one of the consequences or causes of dementia prodromes and may be at greater risk of cardiovascular morbidity. Therefore, exercise is essential for preventing and reducing risk factors for dementia [24].
Obesity has been associated with cognitive deficits, impaired long-term potentiation, and synaptic plasticity, as well as smaller brain volume, increasing the likelihood of developing AD and other dementias. Therefore, obesity is established as a risk factor for dementia [25]. Obesity has been associated with cognitive deficits, impaired long-term potentiation, and synaptic plasticity, as well as smaller brain volume, increasing the likelihood of developing AD and other dementias. Therefore, obesity is established as a risk factor for dementia [25]. Obese people had a 74% increased risk of dementia, while overweight people had a 35% greater risk of dementia compared to normal-weight people. Higher rates of overweight were observed in women suffering from AD aged 70-79 years compared to women who did not suffer from dementia. For every 1.0 increase in BMI at age 70, the risk of AD increases by 36% [26].
Sleep disorders are very common in the elderly, and these changes in sleep patterns are known to be a risk factor for the future development of mild cognitive impairment and dementia. Research suggests an interaction between worsening sleep-wake cycles and dementia. Observing such sleep-wake rhythms can provide important information about the onset of cognitive decline, even years before the clinical onset of dementia [11].
Nutrition and food components remain a challenge for research, with controversy still raging regarding the contribution of micronutrients to the incidence of dementia. Observational studies have focused on individual components ranging from folate and B vitamin content to vitamins C, D, and E, and selenium, which are potential protective factors. In the last five years, there has been a movement to consider entire diets, especially those with high plant intakes, such as the Mediterranean diet (characterized by a high intake of vegetables, legumes, fruits, nuts, cereals, and olive oil, and a low intake of saturated fats and meat) or similar Nordic diets, rather than individual nutrients, as a means to minimize cognitive decline and dementia. One example is a longitudinal cohort study of 960 participants, aged 58–99 years, in which those reporting high vegetable intake experienced less cognitive decline than those with low intake [12].
Sleep disorders are very common in the elderly, and these changes in sleep patterns are known to be a risk factor for the future development of mild cognitive impairment and dementia. Research suggests an interaction between worsening sleep-wake cycles and dementia. Observing such sleep-wake rhythms can provide important information about the onset of cognitive decline, even years before the clinical onset of dementia [27].
Risk factors for dementia from the Islamic perspective
Religion has an important influence on human health and behavior, and people often use religion to cope with illness and stressors in life. Religion and spirituality also shape the way society views neurocognitive disorders, such as the symptoms of dementia. Some of these beliefs can cause delays in seeking treatment from formal health services [28]. Among the results of the literature review regarding efforts to prevent Islamic perspectives. Based on literature studies, several risk factors for dementia from an Islamic perspective, several risk factors were identified, which are explained below [29].
Defects of spiritual stress (resentment, hatred, envy, and vengeance) can negatively impact brain function and increase the frequency of dementia. A lack of faith may weaken individuals in carrying out daily religious activities, leading to increased restlessness and anxiety, which can contribute to the onset of the dementia process [3]. Faith is the basis for carrying out daily individual religious activities, and religious activity has been positively associated with the preservation of cognitive function. Thus, it can be concluded that faith has an important role in preventing the onset of dementia [20].
Faith regarding psychological health is not just a theory; it is about how this faith can be applied in life. With faith, it will be easier for a person to find peace of mind, as faith always directs people to think positively. Therefore treating psychological illnesses with faith is considered one of the most effective approaches [30].
To ensure that one’s faith remains strong, a person should continually fortify themselves by engaging in dhikr, praying, seeking forgiveness, reminding one another, regularly evaluating themselves, and avoiding things that may harm them. This practice is important because it helps individuals recognize Allah SWT [30].
Several religious practices state that reading and listening to the Qur’an can protect against a decline in cognitive function [11]. The relationship between the frequency of reading the Qur’an and the incidence of dementia, based on a study of 75 respondents, indicated that the majority who reported not reading the Qur’an included half who experienced severe dementia (60%), while a small proportion had normal dementia (6.7%). In contrast, only a small minority who read the Qur’an experienced severe dementia (8.9%), and almost half experienced normal dementia (42.2%). Reading the Qur’an can maximize brain function. When someone reads the Qur’an, the sounds produced are received by the ears and then transmitted to the brain, which processes them and generates a response in the form of an electronic field in the cells to compensate for the vibrations produced [31, 32].
Prayer is a form of worship that includes spoken words and special bodily movements, beginning with takbir and ending with greetings. The essence of prayer is remembering Allah SWT. With a heart that consistently remembers Allah, the Most Perfect God, a person gains inner strength when facing the challenges in their life.
Medical circles have widely explored the health benefits of prayer. They have found that the rhythmic movements involved in prayer are one of the best ways for the body to relax. Additionally, they demonstrate that every movement contains certain "benefits" for human health (prayers). The results of this research showed that routine obligatory prayers have a significant relationship with better cognitive function than those who do not pray regularly. Prayer can also improve the quality of life (QoL) for the elderly [20].
Religious activities play an important role in maintaining a better QoL and cognitive function compared to the elderly who are less involved or do not engage in religious activities. A good QoL requires a holistic approach in terms of mental health and physical health leading to happiness [21]. This awareness can foster public understanding of the importance of practicing and participating in religious activities to achieve healthy aging. However, it is recommended that further research be conducted to explore other religious activities and their relationship with QoL and cognitive function [22].
Religious and spiritual practices have the potential to improve mental and physical health and reduce the risk of cognitive impairment. In a 12-month longitudinal study in Italy, it was reported that older adults with AD-related dementia (n=64) reported higher religiosity (i.e. frequency of praying, attending religious events, and reading religious material) and decreased spirituality, along with slower behavior and cognition compared to those with lower levels of religiosity. religiosity and spirituality [32].
Dhikr is a method of therapy in psychology, which can relax a person and make the heart calm. Dhikr can foster positive character traits, alleviate anxiety, purify the heart from negative attitudes and emotions, and, most importantly, is significantly influenced by the presence of the heart [33].
Allah SWT says in the Qur'an surah Ar-Ra'd verse 28
This means: This means: “(Namely) those who believe and whose hearts find peace in the remembrance of Allah. Remember, that only by remembering Allah will your heart find peace” (Ar-Ra'd/13:28). Allah SWT says in the Qur’an, Surah Ar-Ra’d, verse 28:
Dhikr, in a specific sense, refers to speech, or more practically, to mentioning the name of Allah. Through dhikr, a person remembers Allah, and their soul feels calm. When someone repeats phrases of Allah SWT, such as “Subhanallah,” several areas of the brain become active. This activity causes a bioelectric flow in the brain's nerve regions. If dhikr is said repeatedly, this nervous activity becomes pronounced and contributes to an increase in bio-electrical energy. Over time, this active group of nerves influences other nerve groups to become equally active, resulting in overall brain activation. Consequently, this can enhance cognitive abilities [34, 35].
Fasting is a spiritual practice that provides peace of mind and can also prevent and treat disease. Additionally, fasting improves cognitive function in dementia sufferers by enhancing memory. Fasting has been shown to increase the formation of new neurons, which strengthens the link between cognition and neuroplasticity. Neurogenesis in the adult hippocampus and its connections to the prefrontal cortex are related to learning and memory [36]. The underlying mechanisms contributing to the effects of fasting may include reduced oxidative stress and increased neurotrophic and bioenergetic signaling. A reduction in food intake and a lack of available energy lead to cellular stress perceived by neurons, which in turn results in increased production of stress-resistant response proteins [37]. Fasting also causes the production of ketones in large quantities, which the brain uses for energy. The presence of ketones increases the expression of neurotrophic factor derivative genes from the brain, which have a significant effect on dementia and cognition [38].
Conclusion
The healthy lifestyle described in the Qur’an encompasses both a physically healthy lifestyle and a spiritually healthy lifestyle. This aligns with the scientific approach, which emphasizes that the elderly should pay attention not only to physical health but also to spiritual health, as both aspects are closely related and influence each other. To maintain health in the elderly and prevent dementia from a physical perspective, the scientific approach includes preventing disease by avoiding risk factors, treating comorbid conditions, establishing healthy eating and sleeping patterns, avoiding obesity, engaging in physical activity, refraining from alcohol and cigarette consumption, and reducing stress. From a spiritual perspective, Islam teaches humans to obtain peace of mind through strong faith and to engage in acts of worship, such as prayer, reading the Qur’an, dhikr, and fasting.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This study was financially supported by the Universitas Muhammadiyah Semarang (Grant No.: 178/UNIMUS/2024).
Authors' contributions
All authors equally contribute to preparing all parts of the research.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank Universitas Muhammadiyah Semarang for funding this study.
References
Dementia is a common health problem in society. It is characterized by multiple and progressive cognitive impairments, including memory impairment that interferes with independence, and social or occupational functioning that interferes with daily activities. This leads to disability and dependency in the elderly and is, most importantly, a source of distress for affected individuals, their families, and caregivers [1]. With the projected growth trend of the aging population, the number of people with dementia is expected to increase. Worldwide, at least 57.4 million people live with dementia and 1.6 million people die each year from the condition. Although the proportion of the global population aged ≥65 years will double between 2019 and 2050, the prevalence of dementia and Alzheimer's disease (AD), which account for 60–70% of dementia, is expected to reach 152.8 million and 106.4 million people, respectively [2].
In the Qur'an, older age is called the lowest stage of life, because it is accompanied by forgetting past knowledge and experiences. "And among you, is he who is returned to the most elderly so that he does not know anything, after (once having) knowledge," (Qs. Al-Hajj/22: 5). Science refers to this condition as “dementia,” which results from the progressive degeneration of the nerve cell network related to cognitive function [3]. Moreover, the elderly population in the future may face various obstacles in their basic needs and health problems due to dementia. This is the reason why dementia should be a very important concern given by health professionals and the government of countries. These health problems and basic needs include environmental and sociocultural factors and nutritional intake. More attention is needed to address the conditions faced by the elderly population due to dementia; both the general public and health professionals must have a solid understanding of modifiable factors to prevent these conditions. This is the first step toward changing behavior. Unfortunately, public knowledge about risk factors for dementia remains poor and lags behind their knowledge about the risk factors for other common diseases, such as cardiovascular disease (CVD). Understanding the risk factors for its early prevention and treatment [4].
Prevention is a key strategy in combating dementia. A 2020 Lancet commission estimated that 40% of dementia cases could be prevented by addressing medical and lifestyle risk mediators. With increasing evidence of the efficacy of risk reduction, there has been a global policy shift, led by the World Health Organization (WHO) and others, toward the prevention of dementia through risk factor modification [5].
Recently, findings by Hosseini et al. indicated that religious and spiritual involvement is important in protecting middle-aged and elderly groups against cognitive decline. Most of the literature supports a positive relationship between religious and spiritual involvement and cognitive functioning. This can be explained by various aspects of religious activities that involve continuous stimulation of the brain, such as reciting the Qur’an, focusing during prayers, and engaging in motor functions through a series of repetitive activities [6].
Based on the information above, this research reviewed what are the risk factors for dementia as a basis for integrating dementia prevention from scientific and Islamic perspectives. Information about factors that can contribute to preventing dementia can provide valuable insights for health professionals in combining scientific and Islamic approaches simultaneously.
Methods
This research employed a comprehensive literature review strategy, which included searching for articles in research journal databases, conducting Internet searches, and reviewing relevant articles. Databases, including MEDLINE Complete, MEDLINE With Full Text, Academic Search Complete, Professional Development Collection, OmniFile Full Text Select (H.W. Wilson), Newspaper Source, and APA PsycArticles were searched using the keywords, namely“dementia,” “faith,” “prayer,” “reading the Qur’an,” “dhikr,” and “fasting” in the title. Additionally, the Qur’an and books related to dementia were included as supplementary literature.
The following inclusion criteria were applied: Publication dates from 2019 to 2023 (the last 5 years), original research types, accessible full texts, and studies related to factors in preventing dementia among the elderly population through Islamic and scientific approaches. The authors coded, extracted, and combined the data separately, and then, established a final consensus following discussion. All authors who reviewed the papers were experts in the study field. A total of 274 articles were obtained, but only 17 qualified. After a detailed review, 10 articles were included in the analysis. The articles used as samples were then identified and summarized based on the themes that emerged, as presented in Figure 1.
Results
Based on the results of the literature study (Table 1), the risk factors for dementia from a scientific perspective included non-modifiable risk factors (age, gender, and genetics) and modifiable risk factors (cardiovascular disease, hypertension, diabetics, smoking habit, alcohol consumption, head injury, stress, education, physical activity, obesity, and sleep disorder).
Moreover, the risk factors for dementia from an Islamic perspective were faith/belief, practicing religious activities, reading the Al-Qur’an, performing prayer, dhikr, and fasting. Moreover, the integration of risk factors and preventive efforts for dementia from both scientific and Islamic perspectives is presented in Table 2.
From Table 2, it can be seen that the efforts to prevent dementia from both scientific and Islamic perspectives focus on delaying neurodegeneration through the treatment of comorbid diseases (hypertension and diabetes mellitus), promoting physical activity, avoiding head injuries, refraining from alcohol and tobacco consumption, and reducing stress through strong faith, prayer, reading the Qur’an, dhikr, and fasting.
Discussion
Research on scientific and Islamic perspectives as an effort to prevent the incidence of dementia among the elderly population has been frequent; however, the two approaches tend to be treated separately. This research demonstrates that the two approaches are interconnected. In the following paragraph, we will separate these factors into scientific and Islamic categories, and then combine the results for discussion to highlight the novelty of the study. The relationship between the two approaches is illustrated below.
Dementia risk factors from the scientific perspective
Risk factors for dementia can be divided into two categories: Modifiable and non-modifiable risk factors. Non-modifiable risk factors include age, gender, and genetics. The prevalence of dementia increases with age, as observed in clinical settings and population studies. Some declines in bodily functions due to aging are linked to the incidence of dementia [7]. Research conducted by Hogervorst et al. found no relationship between gender and the incidence of dementia, although some studies indicate that women are more likely to have detectable dementia [8]. The most important genetic risk factor is apolipoprotein E (APOE) in late-onset AD, which is consistently identified as the greatest contributor in AD association studies. The APOE e4 allele is associated with an increased risk of late-onset AD, while the APOE e2 allele with a reduced risk. However, the APOE e4 allele does not always cause dementia [9].
Modifiable risk factors include chronic disease, health behavior, head injury, stress, and education. Heart disease is an increasing problem, resulting in vascular insufficiency that has the potential to disrupt the function of other organs, including the brain. A growing body of literature implicates heart disease as a risk factor for dementia. Additionally, several studies have shown that cardiovascular risk factors are independently associated with the development of dementia [10]. Hypertension in middle age and old age is a significant risk factor for the development of vascular dementia in later life. Damage to brain matter, along with cognitive impairment, is associated with long-term hypertensive status. Hypertension is significantly associated with an increased incidence of dementia among men [11]. Both middle-aged hypertension and late-life hypertension are significant risk factors for the development of vascular dementia in older adults. Thus, tight blood pressure control, including during sleep, can have a neuroprotective effect on the brain, and the administration of antihypertensive drugs can prevent the onset of dementia [12]. The development of chronic complications of diabetes mellitus is the excess production of superoxide anion. Intracellular hyperglycemia activates all the main pathways of chronic complications: The polyol pathway, increased hexosamine activity, activation of protein kinase C, formation of advanced glycosylation end products, oxidative stress, apoptosis, inflammation, and the expression and action of hormones, growth factors, cytokines, and inflammatory mediators. In general, diabetes mellitus has been associated with cognitive decline, especially in the elderly, leading to the emergence of cognitive impairment, and an increased risk of developing dementia, including AD and vascular dementia [13]. Diabetes is a risk factor for dementia. Untreated diabetes is a risk factor for dementia. One meta-analysis of diabetes cohort studies reported that, cross-sectionally, people with diabetes who took anti-diabetic drugs had a lower prevalence of cognitive impairment and a reduced incidence of dementia [14].
A meta-analysis of more than 37 studies was conducted to assess the correlation between smoking and dementia. It is established that smokers show an increased risk of dementia, and quitting smoking can reduce this risk. The habit of smoking in middle age has a much stronger impact on the risk of cognitive impairment in old age. Additionally, smoking in old age further increases the occurrence of dementia [15]. Heavy alcohol consumption may be associated with an increased risk of dementia in patients with mild cognitive impairment or in men carrying the APOE e4 allele. In contrast, light-moderate alcohol consumption may be associated with a reduced risk of dementia in elderly patients with mild cognitive impairment. Heavy drinkers have a higher risk of dementia than abstainers and light drinkers [7]. Regular drinking in midlife has a much stronger impact than individual factors on the risk of cognitive impairment in late life [16].
A meta-analysis of more than 37 studies was conducted to assess the correlation between smoking and dementia. It was determined that smokers showed an increased risk of dementia, and quitting smoking reduced the risk of smoking cessation. The increased risk of AD from smoking is more pronounced in APOE e4 noncarriers. Habitual smoking and regular alcohol consumption in middle age have a much stronger impact than individual factors on the risk of cognitive impairment in late life [12]. Heavy alcohol consumption may be associated with an increased risk of dementia in patients with mild cognitive impairment or men carrying the APOE e4 allele. In contrast, light to moderate alcohol consumption may be associated with a reduced risk of dementia in elderly patients with mild cognitive impairment. Heavy drinkers have a higher risk of dementia than abstainers and light drinkers [11].
This is a difficult time for people with concerns about the long-term neurological effects of head injuries. Increasing evidence links traumatic brain injuries (TBIs) to neurodegenerative diseases and dementia [17]. Many high-profile diagnoses of chronic traumatic encephalopathy (CTE), specifically post-traumatic dementia, have been made post-mortem, contributing to general anxiety about the long-term effects of even mild injuries [18]. The international classification of disease (ICD) defines mild TBI as a concussion, and severe TBI as a skull fracture, edema, brain injury, or hemorrhage. TBI is associated with a higher risk of increased incidence of dementia after six months compared to individuals who did not experience a TBI [12].
Depression is a key comorbid risk factor for dementia. Experiencing period-specific psychological distress throughout life can influence cognitive health. When the physiological stress response is triggered, the activity of the hypothalamic-pituitary-adrenal axis fosters excessive cortisol production, potentially leading to hippocampal damage. Thus, the stress response may influence cognitive function and the risk of dementia [19].
The negative impact of chronic stress on cognition can be significant, and interventions controlling stress levels provide benefits for dementia prevention. Supporting this idea, regular religious activities can improve the cognitive function of healthy individuals. Faith has been shown to delay age-related declines in cognitive function and improve some neuropsychological outcomes in subjects with mild cognitive impairment [20].
Psychological distress, such as feelings of anxiety, depression, irritability, and reactions to external stressors in a person's daily life, is associated with an increased risk of dementia. Stress can have severe and dangerous consequences not only for our brain health but also for our health in general. We can go further in dementia prevention by addressing psychological risk factors for dementia [19].
Bahiroh et al. indicated that people with lower education levels have a higher chance of having undetected dementia. This finding is supported by many studies showing that people with more education tend to perform better, making early signs of dementia more difficult to detect on standard tests because they do not reach the threshold required for detectable dementia [21]. Low education is a risk factor for accelerating memory decline and the occurrence of dementia, with the impact being more pronounced as one age. A child’s higher education level and greater lifetime educational attainment reduce the risk of dementia. New jobs can improve overall cognitive abilities, and education during late adolescence when the brain reaches its greatest plasticity. This suggests that cognitive stimulation is more important during youth [12].
Najar et al. showed that physical activity in midlife was independently associated with a reduced risk of dementia and its subtypes. They showed that these midlife activities play a role in maintaining cognitive health in old age [22]. Regular physical exercise seems to be one of the effective methods to reduce the risk of dementia among all lifestyle changes that have been studied. Several studies on the effects of aerobic exercise (exercise that increases heart rate) in middle-aged or older adults have found improvements in thinking and memory, as well as reduced rates of dementia [23].
The study of physical activity is complex. Physical activity patterns are influenced by age, generation, morbidity and gender, and social and cultural factors. Research shows an association between physical activity and a potential reduction in the risk of dementia. Individuals who do not enjoy exercising may experience one of the consequences or causes of dementia prodromes and may be at greater risk of cardiovascular morbidity. Therefore, exercise is essential for preventing and reducing risk factors for dementia [24].
Obesity has been associated with cognitive deficits, impaired long-term potentiation, and synaptic plasticity, as well as smaller brain volume, increasing the likelihood of developing AD and other dementias. Therefore, obesity is established as a risk factor for dementia [25]. Obesity has been associated with cognitive deficits, impaired long-term potentiation, and synaptic plasticity, as well as smaller brain volume, increasing the likelihood of developing AD and other dementias. Therefore, obesity is established as a risk factor for dementia [25]. Obese people had a 74% increased risk of dementia, while overweight people had a 35% greater risk of dementia compared to normal-weight people. Higher rates of overweight were observed in women suffering from AD aged 70-79 years compared to women who did not suffer from dementia. For every 1.0 increase in BMI at age 70, the risk of AD increases by 36% [26].
Sleep disorders are very common in the elderly, and these changes in sleep patterns are known to be a risk factor for the future development of mild cognitive impairment and dementia. Research suggests an interaction between worsening sleep-wake cycles and dementia. Observing such sleep-wake rhythms can provide important information about the onset of cognitive decline, even years before the clinical onset of dementia [11].
Nutrition and food components remain a challenge for research, with controversy still raging regarding the contribution of micronutrients to the incidence of dementia. Observational studies have focused on individual components ranging from folate and B vitamin content to vitamins C, D, and E, and selenium, which are potential protective factors. In the last five years, there has been a movement to consider entire diets, especially those with high plant intakes, such as the Mediterranean diet (characterized by a high intake of vegetables, legumes, fruits, nuts, cereals, and olive oil, and a low intake of saturated fats and meat) or similar Nordic diets, rather than individual nutrients, as a means to minimize cognitive decline and dementia. One example is a longitudinal cohort study of 960 participants, aged 58–99 years, in which those reporting high vegetable intake experienced less cognitive decline than those with low intake [12].
Sleep disorders are very common in the elderly, and these changes in sleep patterns are known to be a risk factor for the future development of mild cognitive impairment and dementia. Research suggests an interaction between worsening sleep-wake cycles and dementia. Observing such sleep-wake rhythms can provide important information about the onset of cognitive decline, even years before the clinical onset of dementia [27].
Risk factors for dementia from the Islamic perspective
Religion has an important influence on human health and behavior, and people often use religion to cope with illness and stressors in life. Religion and spirituality also shape the way society views neurocognitive disorders, such as the symptoms of dementia. Some of these beliefs can cause delays in seeking treatment from formal health services [28]. Among the results of the literature review regarding efforts to prevent Islamic perspectives. Based on literature studies, several risk factors for dementia from an Islamic perspective, several risk factors were identified, which are explained below [29].
Defects of spiritual stress (resentment, hatred, envy, and vengeance) can negatively impact brain function and increase the frequency of dementia. A lack of faith may weaken individuals in carrying out daily religious activities, leading to increased restlessness and anxiety, which can contribute to the onset of the dementia process [3]. Faith is the basis for carrying out daily individual religious activities, and religious activity has been positively associated with the preservation of cognitive function. Thus, it can be concluded that faith has an important role in preventing the onset of dementia [20].
Faith regarding psychological health is not just a theory; it is about how this faith can be applied in life. With faith, it will be easier for a person to find peace of mind, as faith always directs people to think positively. Therefore treating psychological illnesses with faith is considered one of the most effective approaches [30].
To ensure that one’s faith remains strong, a person should continually fortify themselves by engaging in dhikr, praying, seeking forgiveness, reminding one another, regularly evaluating themselves, and avoiding things that may harm them. This practice is important because it helps individuals recognize Allah SWT [30].
Several religious practices state that reading and listening to the Qur’an can protect against a decline in cognitive function [11]. The relationship between the frequency of reading the Qur’an and the incidence of dementia, based on a study of 75 respondents, indicated that the majority who reported not reading the Qur’an included half who experienced severe dementia (60%), while a small proportion had normal dementia (6.7%). In contrast, only a small minority who read the Qur’an experienced severe dementia (8.9%), and almost half experienced normal dementia (42.2%). Reading the Qur’an can maximize brain function. When someone reads the Qur’an, the sounds produced are received by the ears and then transmitted to the brain, which processes them and generates a response in the form of an electronic field in the cells to compensate for the vibrations produced [31, 32].
Prayer is a form of worship that includes spoken words and special bodily movements, beginning with takbir and ending with greetings. The essence of prayer is remembering Allah SWT. With a heart that consistently remembers Allah, the Most Perfect God, a person gains inner strength when facing the challenges in their life.
Medical circles have widely explored the health benefits of prayer. They have found that the rhythmic movements involved in prayer are one of the best ways for the body to relax. Additionally, they demonstrate that every movement contains certain "benefits" for human health (prayers). The results of this research showed that routine obligatory prayers have a significant relationship with better cognitive function than those who do not pray regularly. Prayer can also improve the quality of life (QoL) for the elderly [20].
Religious activities play an important role in maintaining a better QoL and cognitive function compared to the elderly who are less involved or do not engage in religious activities. A good QoL requires a holistic approach in terms of mental health and physical health leading to happiness [21]. This awareness can foster public understanding of the importance of practicing and participating in religious activities to achieve healthy aging. However, it is recommended that further research be conducted to explore other religious activities and their relationship with QoL and cognitive function [22].
Religious and spiritual practices have the potential to improve mental and physical health and reduce the risk of cognitive impairment. In a 12-month longitudinal study in Italy, it was reported that older adults with AD-related dementia (n=64) reported higher religiosity (i.e. frequency of praying, attending religious events, and reading religious material) and decreased spirituality, along with slower behavior and cognition compared to those with lower levels of religiosity. religiosity and spirituality [32].
Dhikr is a method of therapy in psychology, which can relax a person and make the heart calm. Dhikr can foster positive character traits, alleviate anxiety, purify the heart from negative attitudes and emotions, and, most importantly, is significantly influenced by the presence of the heart [33].
Allah SWT says in the Qur'an surah Ar-Ra'd verse 28
This means: This means: “(Namely) those who believe and whose hearts find peace in the remembrance of Allah. Remember, that only by remembering Allah will your heart find peace” (Ar-Ra'd/13:28). Allah SWT says in the Qur’an, Surah Ar-Ra’d, verse 28:
Dhikr, in a specific sense, refers to speech, or more practically, to mentioning the name of Allah. Through dhikr, a person remembers Allah, and their soul feels calm. When someone repeats phrases of Allah SWT, such as “Subhanallah,” several areas of the brain become active. This activity causes a bioelectric flow in the brain's nerve regions. If dhikr is said repeatedly, this nervous activity becomes pronounced and contributes to an increase in bio-electrical energy. Over time, this active group of nerves influences other nerve groups to become equally active, resulting in overall brain activation. Consequently, this can enhance cognitive abilities [34, 35].
Fasting is a spiritual practice that provides peace of mind and can also prevent and treat disease. Additionally, fasting improves cognitive function in dementia sufferers by enhancing memory. Fasting has been shown to increase the formation of new neurons, which strengthens the link between cognition and neuroplasticity. Neurogenesis in the adult hippocampus and its connections to the prefrontal cortex are related to learning and memory [36]. The underlying mechanisms contributing to the effects of fasting may include reduced oxidative stress and increased neurotrophic and bioenergetic signaling. A reduction in food intake and a lack of available energy lead to cellular stress perceived by neurons, which in turn results in increased production of stress-resistant response proteins [37]. Fasting also causes the production of ketones in large quantities, which the brain uses for energy. The presence of ketones increases the expression of neurotrophic factor derivative genes from the brain, which have a significant effect on dementia and cognition [38].
Conclusion
The healthy lifestyle described in the Qur’an encompasses both a physically healthy lifestyle and a spiritually healthy lifestyle. This aligns with the scientific approach, which emphasizes that the elderly should pay attention not only to physical health but also to spiritual health, as both aspects are closely related and influence each other. To maintain health in the elderly and prevent dementia from a physical perspective, the scientific approach includes preventing disease by avoiding risk factors, treating comorbid conditions, establishing healthy eating and sleeping patterns, avoiding obesity, engaging in physical activity, refraining from alcohol and cigarette consumption, and reducing stress. From a spiritual perspective, Islam teaches humans to obtain peace of mind through strong faith and to engage in acts of worship, such as prayer, reading the Qur’an, dhikr, and fasting.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This study was financially supported by the Universitas Muhammadiyah Semarang (Grant No.: 178/UNIMUS/2024).
Authors' contributions
All authors equally contribute to preparing all parts of the research.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank Universitas Muhammadiyah Semarang for funding this study.
References
- Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: Review. JAMA. 2019; 322(16):1589-99. [DOI:10.1001/jama.2019.4782] [PMID] [PMCID]
- Paul P, Mahfoud ZR, Malik RA, Kaul R, Muffuh Navti P, Al-Sheikhly D, et al. Knowledge, awareness, and attitude of healthcare stakeholders on alzheimer's disease and dementia in Qatar. International Journal of Environmental Research and Public Health. 2023; 20(5):4535. [DOI:10.3390/ijerph20054535] [PMID] [PMCID]
- Asadzandi M. Dementia theory from the perspective of Islam. Journal of Religion and Theology. 2019; 3(1):17-22. [DOI:10.22259/2637-5907.0301010]
- Nichols E, Vos T. The estimation of the global prevalence of dementia from 1990-2019 and forecasted prevalence through 2050: An analysis for the global burden of disease (GBD) study 2019. The Journal of The Alzheimer and Dementia. 2022; 7(S10):e051496. [DOI:10.1002/alz.051496]
- Morgan J, Bindoff A, Doherty K, Vickers J, Alty J. Are tomorrow's doctors prepared to prevent dementia? A cross-sectional study of Tasmanian medical students' knowledge of dementia risk factors. Journal of Clinical Neuroscience. 2022; 96:133-7.[DOI:10.1016/j.jocn.2021.11.005] [PMID]
- Hosseini S, Chaurasia A, Oremus M. The effect of religion and spirituality on cognitive function: A systematic review. The Gerontologist. 2019; 59(2):e76-85. [DOI:10.1093/geront/gnx024] [PMID]
- Ragubathy PK, Adikane H. Prevalence of risk factors for dementia in elderly population in a tribal area of central India-A community-based cross-sectional study. Journal of Medical Sciences and Health. 2020; 5(3):19-30. [DOI:10.46347/JMSH.2019.v05i03.004]
- Hogervorst E, Temple S, O'Donnell E. Sex differences in dementia. Current Topics in Behavioral Neurosciences. 2023; 62:309-31.[DOI:10.1007/7854_2022_408] [PMID]
- Jiao B, Liu H, Guo L, Xiao X, Liao X, Zhou Y, et al. The role of genetics in neurodegenerative dementia: A large cohort study in South China. NPJ Genomic Medicine. 2021; 6(1):69. [DOI:10.1038/s41525-021-00235-3] [PMID] [PMCID]
- Denisenko D, Ekong G, Spotts H. Dementia risk in patients with heart disease and depression. Dementia & Neuropsychologia. 2023; 17:e20230024. [DOI:10.1590/1980-5764-dn-2023-0024] [PMID] [PMCID]
- Priastana IKA, Nurmalisyah FF. Faktor risiko kejadian demensia berdasarkan studi literatur. Jurnal Ilmiah. 2020; 15(2):279-82. [DOI:10.36911/pannmed.v15i2.745]
- Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020; 396(10248):413-46. [DOI:10.1016/S0140-6736(20)30367-6] [PMID]
- Albai O, Frandes M, Timar R, Roman D, Timar B. Risk factors for developing dementia in type 2 diabetes mellitus patients with mild cognitive impairment. Neuropsychiatric Disease and Treatment. 2019; 15:167-75. [DOI:10.2147/NDT.S189905] [PMID] [PMCID]
- Sabia S, Fayosse A, Dumurgier J, Schnitzler A, Empana JP, Ebmeier KP, et al. Association of ideal cardiovascular health at age 50 with incidence of dementia: 25 year follow-up of Whitehall II cohort study. BMJ. 2019; 366:l4414. [DOI:10.1136/bmj.l4414] [PMID] [PMCID]
- Jeong SM, Park J, Han K, Yoo J, Yoo JE, Lee CM, et al. Association of changes in smoking intensity with risk of dementia in Korea. JAMa Network Open. 2023; 6(1):e2251506. [DOI:10.1001/jamanetworkopen.2022.51506] [PMID] [PMCID]
- Wu J, Dong W, Pan XF, Feng L, Yuan JM, Pan A, et al. Relation of cigarette smoking and alcohol drinking in midlife with risk of cognitive impairment in late life: The Singapore Chinese health study. Age and Ageing. 2019; 48(1):101-7. [DOI:10.1093/ageing/afy166] [PMID] [PMCID]
- Wiegmann C, Mick I, Brandl EJ, Heinz A, Gutwinski S. Alcohol and dementia - what is the link? A systematic review. Neuropsychiatric Disease and Treatment. 2020; 16:87-99. [DOI:10.2147/NDT.S198772] [PMID] [PMCID]
- Graham NS, Sharp DJ. Dementia after traumatic brain injury. BMJ. 2023; 383:2065. [DOI:10.1136/bmj.p2065] [PMID]
- Islamoska S, Ishtiak-Ahmed K, Hansen ÅM, Grynderup MB, Mortensen EL, Garde AH, et al. Vital exhaustion and incidence of dementia: Results from the copenhagen city heart study. Journal of Alzheimer's Disease. 2019; 67(1):369-79. [DOI:10.3233/JAD-180478] [PMID] [PMCID]
- Amir SN, Juliana N, Azmani S, Abu IF, Talib AHQA, Abdullah F, et al. Impact of religious activities on quality of life and cognitive function among elderly. Journal of Religion and Health. 2022; 61(2):1564-84. [DOI:10.1007/s10943-021-01408-1] [PMID] [PMCID]
- Bahiroh S, Pratiwi SA, Suud FM. Improving student happiness through the snowball throwing method in the implementation of student conceling groups of state vocational schools 2 depok yogyakarta. Journal of Critical Reviews. 2020; 7(5):563-8. [DOI:10.31838/jcr.07.05.117]
- Gamble LD, Matthews FE, Jones IR, Hillman AE, Woods B, Macleod CA, et al. Characteristics of people living with undiagnosed dementia: Findings from the CFAS Wales study. BMC Geriatrics. 2022; 22(1):409. [DOI:10.1186/s12877-022-03086-4] [PMID] [PMCID]
- Najar J, Östling S, Gudmundsson P, Sundh V, Johansson L, Kern S, et al. Cognitive and physical activity and dementia: A 44-year longitudinal population study of women. Neurology. 2019; 92(12):e1322-30. [DOI:10.1212/WNL.0000000000007021] [PMID] [PMCID]
- Wang S, Liu HY, Cheng YC, Su CH. Exercise dosage in reducing the risk of dementia development: mode, duration, and intensity-A narrative review. International Journal of Environmental Research and Public Health. 2021; 18(24):13331. [DOI:10.3390/ijerph182413331] [PMID] [PMCID]
- Saint-Maurice PF, Coughlan D, Kelly SP, Keadle SK, Cook MB, Carlson SA, et al. Association of leisure-time physical activity across the adult life course with all-cause and cause-specific mortality. JAMA Network Open. 2019; 2(3):e190355. [DOI:10.1001/jamanetworkopen.2019.0355] [PMID] [PMCID]
- Flores-Cordero JA, Pérez-Pérez A, Jiménez-Cortegana C, Alba G, Flores-Barragán A, Sánchez-Margalet V. Obesity as a risk factor for dementia and alzheimer's disease: The role of leptin. International Journal of Molecular Sciences. 2022; 23(9):5202. [DOI:10.3390/ijms23095202] [PMID] [PMCID]
- Bowman K, Thambisetty M, Kuchel GA, Ferrucci L, Melzer D. Obesity and longer term risks of dementia in 65-74 year olds. Age and Ageing. 2019; 48(3):367-73. [DOI:10.1093/ageing/afz002] [PMID] [PMCID]
- Bubbico G, Di Iorio A, Lauriola M, Sepede G, Salice S, Spina E, et al. Subjective cognitive decline and nighttime sleep alterations, A longitudinal analysis. Frontiers in Aging Neuroscience. 2019; 11:142. [DOI:10.3389/fnagi.2019.00142] [PMID] [PMCID]
- Daher-Nashif S, Hammad SH, Kane T, Al-Wattary N. Islam and mental disorders of the older adults: Religious text, belief system and caregiving practices. Journal of Religion and Health. 2021; 60(3):2051-65. [DOI:10.1007/s10943-020-01094-5] [PMID] [PMCID]
- Ula AF. [Pikun dalam al-qur’an: Kajian term arżal al-’umur dan relevansinya dengan problem anxiety disorder (Indonesian) (Undergraduate thesis)]. Java: IAIN Kediri, 2022. [Link]
- Arroisi J. [Iman dan kesehatan psikis perspektif said nursi (Kajian Psikoterapi dalam Risale-i Nur) (Indonesian)]. kalimah. 2020; 18(1):1-6. [Link]
- Rahmawati Ramli WL. [Factors Related to the Incidence of dementia at the jumpandang baru health center, tallo district, Makassar City (Indonesian). J Med Hutama; 01. [Link]
- Khafidah W, Wildanizar W, Tabrani ZA, Nurhayati N, Raden Z. The application of wahdah method in memorizing the qur’an for students of SMPN 1 unggul sukamakmur. International Journal of Islamic Educational Psychology. 2020; 1(1):37-49. [DOI:10.18196/ijiep.1104]
- Britt KC, Richards KC, Acton G, Hamilton J, Radhakrishnan K. Association of religious service attendance and neuropsychiatric symptoms, cognitive function, and sleep disturbances in all-cause dementia. International Journal of Environmental Research and Public Health. 2023; 20(5):4300. [DOI:10.3390/ijerph20054300] [PMID] [PMCID]
- Aliasan A. [Pengaruh dzikir terhadap psikolgis muslim (Indonesian)]. Yonetim. 2019; 2(1):79-93. [Link]
- Rahmat CA. Terapi religi dzikir pada odd terhadap peningkatan kognitif di instalasi psikogeriatri rsj lawang (Doctoral dissertation)]. Islamabad: International Islamic University; 2020. [Link]
- Muhandis J, Yamin MN, Nurjan S. Jamuro religious factors: Perspective of islamic education psychology. International Journal of Islamic Educational Psychology. 2020; 1(1):64-74. [DOI:10.18196/ijiep.1106]
- Portero-Tresserra M, Galofré-López N, Pallares E, Gimenez-Montes C, Barcia C, Granero R, et al. Effects of caloric restriction on spatial object recognition memory, hippocampal neuron loss and neuroinflammation in aged rats. Nutrients. 2023; 15(7):1572. [DOI:10.3390/nu15071572] [PMID] [PMCID]
- Kanwar D, Wasay M. Effects of intermittent fasting on cognition and neurodegeneration. Pakistan Journal of Neurological Sciences; 16(3):35-7. [Link]
Type of Study: Review Article |
Subject:
● Disease Control
Received: 2024/01/22 | Accepted: 2024/04/21 | Published: 2024/09/1
Received: 2024/01/22 | Accepted: 2024/04/21 | Published: 2024/09/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
