

Volume 14, Issue 6 (Nov & Dec 2024)
J Research Health 2024, 14(6): 567-574 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Akhondi R, Ghomi M, Nasimi A, Seyedhosseini S R, Pouraidi A, Akbary A et al . Effectiveness of the National Blood Pressure Measurement Campaign in the East and Southeast of Iran. J Research Health 2024; 14 (6) :567-574
URL: http://jrh.gmu.ac.ir/article-1-2507-en.html
URL: http://jrh.gmu.ac.ir/article-1-2507-en.html
Reza Akhondi1 

 , Mahsa Ghomi2 , Ali Nasimi1 , Seyed Reza Seyedhosseini3 , Arefeh Pouraidi1 , Ali Akbary4 , Ali Alami5
, Mahsa Ghomi2 , Ali Nasimi1 , Seyed Reza Seyedhosseini3 , Arefeh Pouraidi1 , Ali Akbary4 , Ali Alami5
, Mahsa Ghomi2 , Ali Nasimi1 , Seyed Reza Seyedhosseini3 , Arefeh Pouraidi1 , Ali Akbary4 , Ali Alami5
1- Student Research Committee, Gonabad University of Medical Sciences, Gonabad, Iran.
2- Student Research Committee, Zabol University of Medical Sciences, Zabol, Iran.
3- Student Research Committee, Jiroft University of Medical Sciences, Jiroft, Iran.
4- Department of Psychiatry, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
5- Department of Epidemiology and Biostatistics, School of Public Health; Social Determinants of Health Research Center, Gonabad University of Medical Sciences, Gonabad, Iran. ,alialami65@hotmail.com
2- Student Research Committee, Zabol University of Medical Sciences, Zabol, Iran.
3- Student Research Committee, Jiroft University of Medical Sciences, Jiroft, Iran.
4- Department of Psychiatry, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
5- Department of Epidemiology and Biostatistics, School of Public Health; Social Determinants of Health Research Center, Gonabad University of Medical Sciences, Gonabad, Iran. ,
Full-Text [PDF 685 kb]
(725 Downloads)
| Abstract (HTML) (3220 Views)
Full-Text: (826 Views)
Introduction
Hypertension (HTN) or high blood pressure (BP), defined by systolic BP≥140 mm Hg or diastolic BP≥90 mm Hg, is one of the major contributors to morbidity and mortality around the world [1]. It is estimated to be the leading cause of death in approximately 10 million individuals annually across the globe [2]. Together with diabetes mellitus, low-density lipoprotein cholesterol levels, body mass index, and smoking, HTN is considered a modifiable risk factor for cardiovascular diseases [3]. Furthermore, evidence supports that having pathological high BP can elevate the risk of sudden death and mortality, particularly due to chronic disorders in other systems, such as chronic renal failure [4].
HTN affects 33% of adults aged between 30 and 79 years worldwide [5], with a slightly higher prevalence in men (34%) compared to women (32%) [4]. Although there were declines in developed countries, the total number of adults with HTN increased from 650 million in 1990 to 1.3 billion in 2019, with most of them living in undeveloped and developing countries [6]. Despite this increase, the overall global prevalence of HTN remained relatively constant from 1990 to 2019 [6]. Over the years, numerous studies have sought to unravel the prevalence and patterns of HTN in Iran, providing valuable insights into the dynamics of this health condition within the country [7-21]. However, these findings show disparities in some cases. For example, according to a systematic review, the mean prevalence of HTN among the Iranian population is about 25% [16, 17, 22]. In comparison, another study that analyzed the information from the Fasa region of this cohort study reported a total prevalence of 34%, %, which is more consistent with global statistics [18]. Furthermore, the most recent study in this regard suggests that 26.6% of Iranian adults have high BP [12].
The timely identification of individuals in the prehypertensive stage or those with undiagnosed HTN, coupled with the effective restoration of BP within the normative range through pharmacological or non-pharmacological interventions, constitutes key determinants in the prognosis of the disease. Unfortunately, the national program for identifying non-communicable diseases (NCDs) is not effective enough [23].
Given the relatively high prevalence in the population, the burden of the disease, and the availability of effective treatment, it is recommended that screening programs be conducted on a large scale to identify undiagnosed patients and high-risk individuals to minimize the aforementioned complications and costs.
In this study, we aimed to estimate the prevalence of HTN by conducting an organized screening program in the eastern and southeastern regions of Iran. The effectiveness of this study is assessed by identifying the percentage of patients with HTN who were unaware of their condition prior to the implementation of the program.
Methods
In this analytical cross-sectional study conducted in 2019, we included 936 individuals from those who participated in the Iranian National BP measurement campaign (INBPMC). Using a probability proportional to size cluster sampling, the participants were selected from Gonabad, Birjand, Jiroft, and Zabol, four cities located in the Eastern and Southeast regions of Iran. The dependent variable was HTN (the outcome of this study is the percentage of newly identified hypertensive cases), while the independent variables were age, sex, place of residence, and previous history of HTN.
Based on previous research [5] indicating a prevalence of HTN of 45.1%, a sample size of 777 individuals was calculated for the study, with a significance level of 95% and a test power of 80%. In order to increase the accuracy and control potential concerns during the data collection process, an additional 20% was added to the calculated sample size. Equation 1 was used to determine the sample size.
Using a multi-stage sampling method, we selected the participants. First, we determined the required sample size in cities based on their populations. Then, we randomly selected some urban and rural sites that were active in the campaign. We included participants who enrolled in the INBPMC and met the eligibility criteria (inclusion and exclusion criteria). Informed written consent was obtained from the participants before collecting the required data.
Inclusion criteria encompassed individuals who sought services from diverse healthcare facilities, including community health centers, hospitals, and designated stations, within the eastern and southeast regions of the country. Individuals over the age of 30, without diagnosed neuropsychiatric or sensorimotor disorders, and with a minimum of 4 years of education were included in this study. After presenting pertinent information about the research plan and objectives, eligible participants meeting the inclusion criteria were recruited. Then, written informed consent was obtained from the participants, and they completed a checklist that included information, such as age, sex, place of residence, and previous medical history. The BP of the participants was recorded on this checklist. If a participant refused to participate in the study during the data collection process, he/she was excluded from the study. The sampling process continued until the predetermined sample size was reached for each site.
BP measurements were conducted by trained survey personnel using standard methods. BP was assessed using a precisely calibrated sphygmomanometer equipped with a suitably sized cuff, and the readings were recorded to the nearest whole number. The systolic BP (SBP) and diastolic BP (DBP) values were identified based on the first and 5th Korotkoff sounds, respectively. BP was assessed twice in the sitting position for each participant, using the right arm after a 10-minute resting period. The stage of HTN was determined by calculating the average of these two records. Then, the values were recorded on the appropriate checklist that included information regarding age, sex, past medical and drug history, marital status, educational level, place of residence, and measured BP of each person. The participants who had an SBP of <40 mm Hg, a DBP <90 mm Hg, and were not under treatment with any antihypertensive agents were considered normal; otherwise, they were classified as affected by HTN. To control for potential biases, the interviewers in the study received necessary training on the data collection methods during a training session.
Statistical analysis of the collected data was performed using SPSS software, version 20. Descriptive statistics, such as frequency distribution tables and related charts, were employed for qualitative data. Also, quantitative data were characterized using measures of central tendency and dispersion, such as Mean±SD.
Results
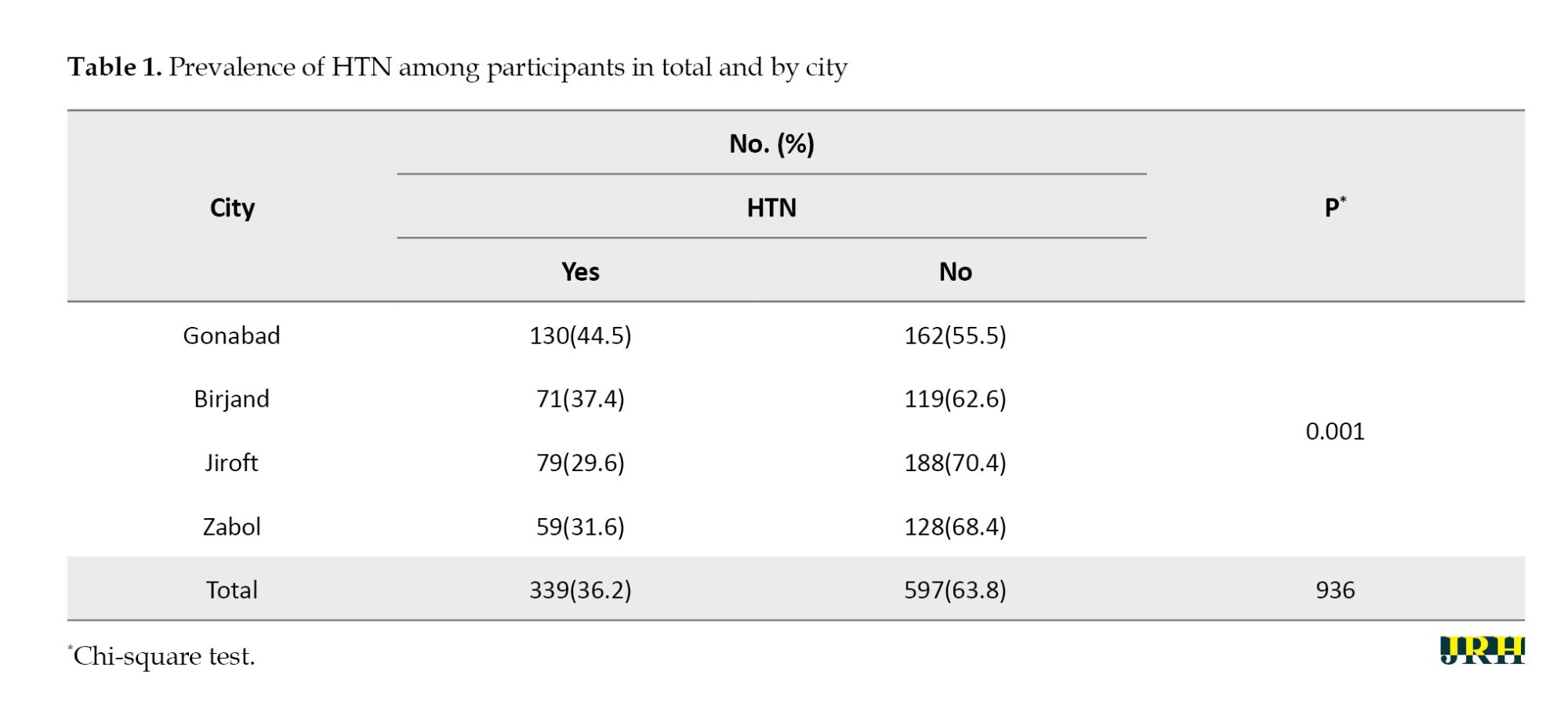
We analyzed the data of 936 participants (male: 581, female: 335; M/F ratio=1.73). The Mean±SD age of the participants was 45.48±12.774 years. The mean age of participants in Gonabad (52.32) was significantly higher than in other cities (P=0.001). The prevalence of HTN among the participants was 36.2%.
Table 1 shows that the highest prevalence of HTN was in Gonabad.
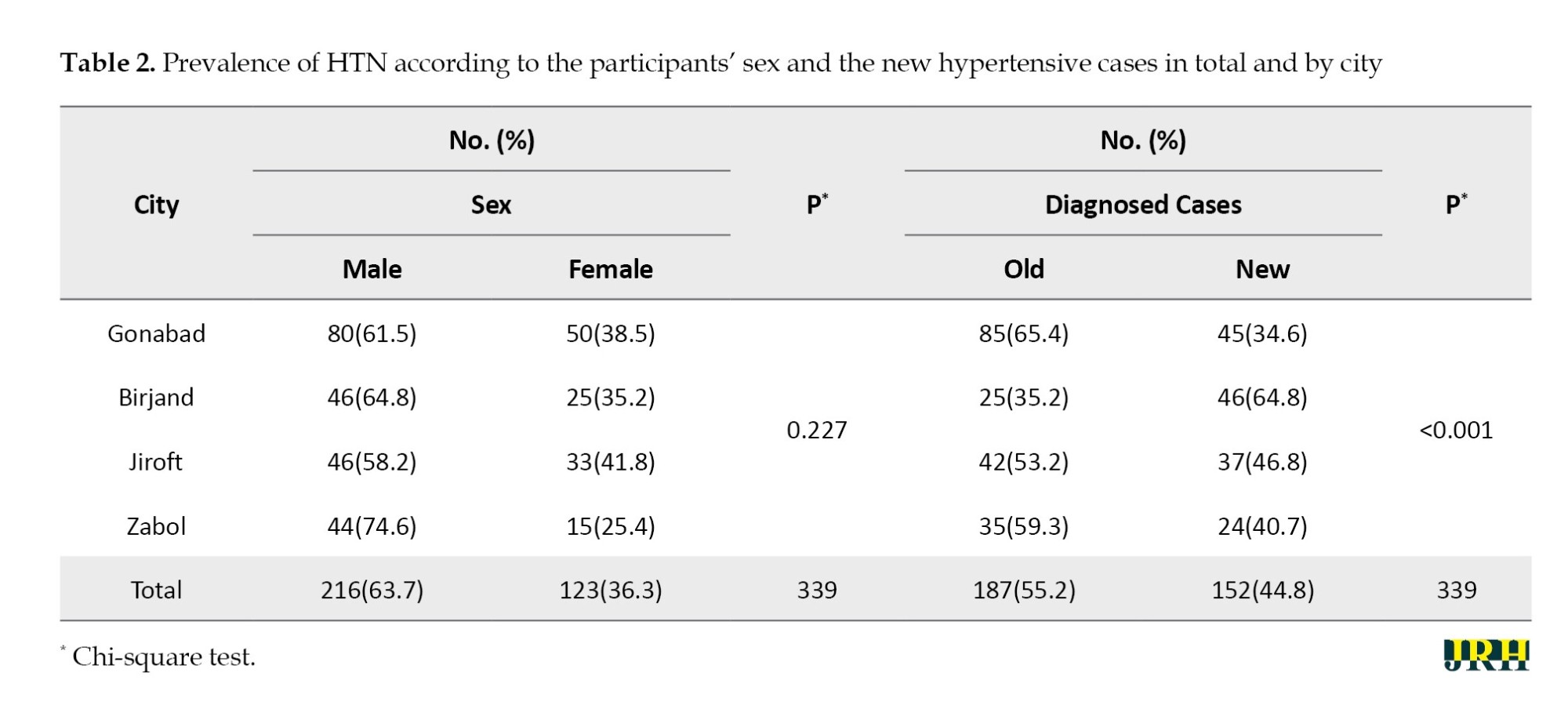
The prevalence of HTN by sex is shown in Table 2. Table 2 also shows the old and new cases of HTN, both overall and in each city. It indicates that the percentage of new hypertensive cases in this study was 16.2% (152/936). Besides, 44.8% of the patients with HTN were new hypertensive cases, and the identification of the new hypertensive cases was significantly different among the participants from different cities (Table 2). The Mean±SD age of all hypertensive cases was 50.59±13.480, while the Mean±SD age of newly and previously diagnosed cases was 45.39±11.246 and 54.82±13.088, respectively, with a statistically significant difference found (P<0.001). Among newly diagnosed hypertensive cases, 118 were men and 34 were women. There was no statistically significant difference in the sex distribution of newly diagnosed hypertensive cases across different cities (P=0.509).
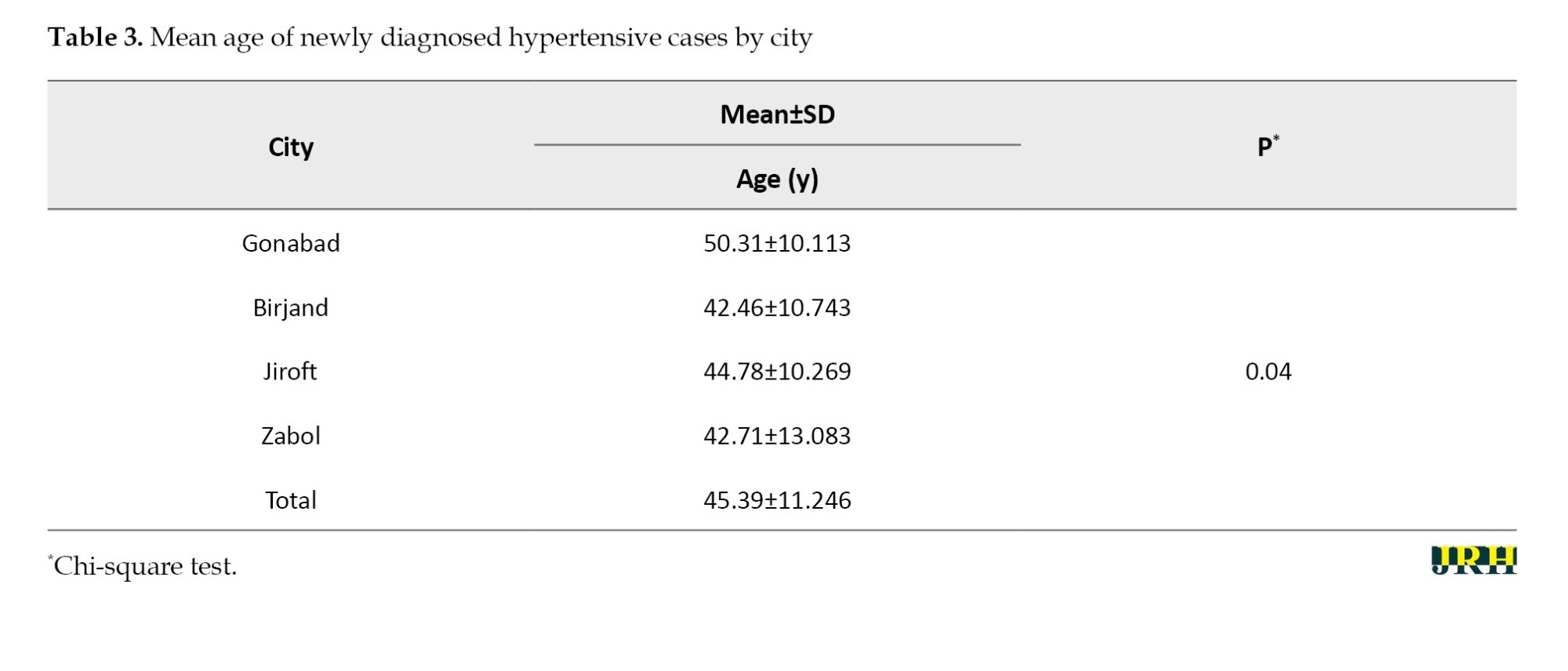
As Table 3 demonstrates, there was a significant difference between the mean age of newly diagnosed hypertensive cases and the city of the participants (P=0.04), with the mean age of new cases in Birjand being lower than in other cities.
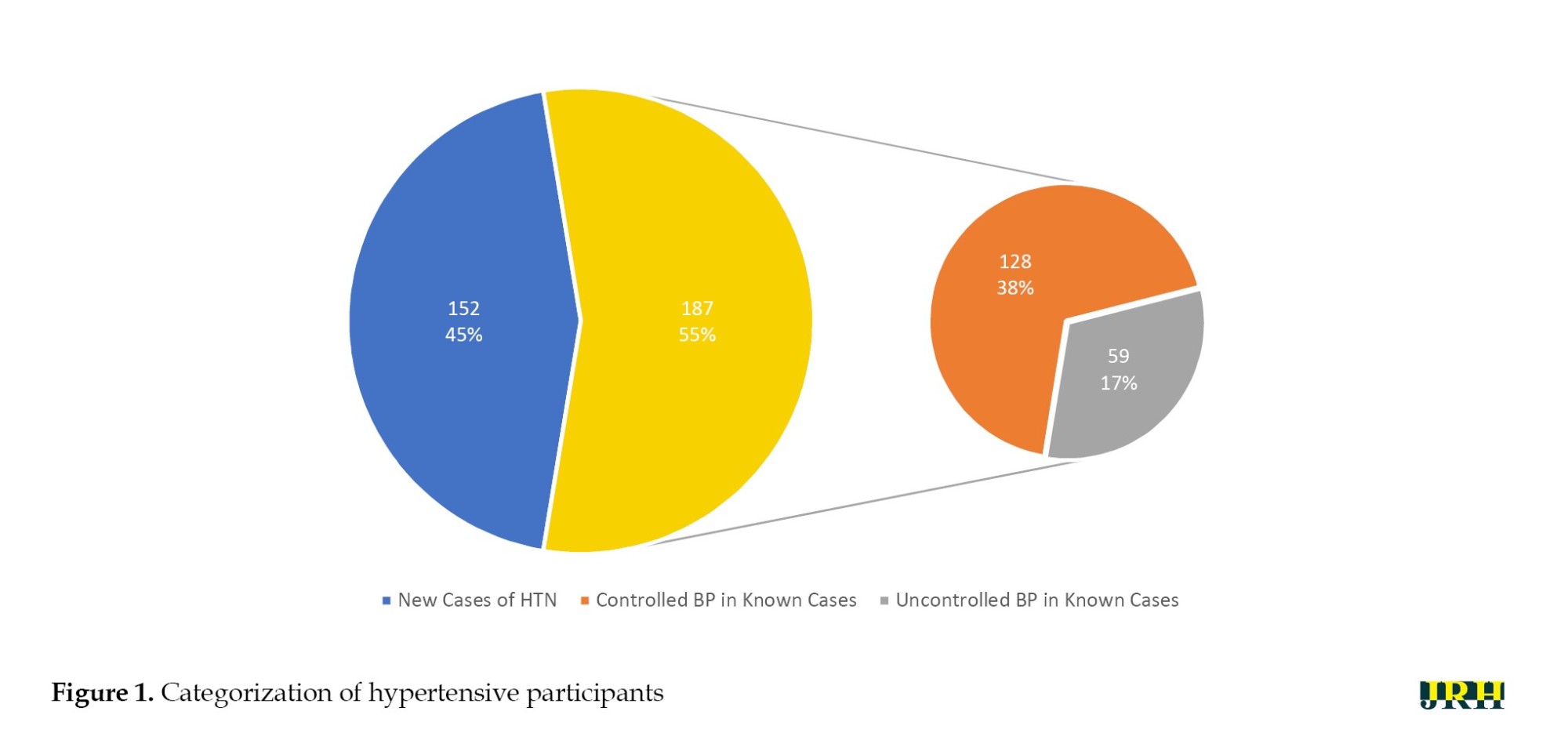
Additionally, as demonstrated in Figure 1, among the 187 old hypertensive cases (Table 2), only 128 managed to maintain controlled BP, while the remaining 59 were detected with uncontrolled BP.
Discussion
This study was conducted to determine the proportion of new hypertensive cases diagnosed during the INBPMC in the East and Southeast of Iran in 2019-20. The prevalence of HTN in this study was reported as 36.2%, which was significantly higher in Gonabad than in other cities. Among the reported cases, 44.8% were new patients, and the overall percentage of new hypertensive cases in this study was 16.2%. There was a significant association between the prevalence of HTN and residency location. Besides, a statistically significant difference was observed between the identification of new hypertensive cases and the city of residence of the participants. We did not find a significant relationship between sex and the prevalence of HTN, as well as the identification of new hypertensive cases.
In this study, 36.2% of the population was found to have hypertensive conditions, and among them, 44.8% (16.2% of the total participants) were identified with HTN for the first time. We also found significant differences in the overall prevalence of HTN, the total age average of the participants across the four cities, and the mean age of the hypertensive group compared to non-hypertensive participants. Notably, we observed a meaningful disparity between the prevalence of newly and previously diagnosed hypertensive patients across the four cities. Furthermore, no substantial association was found between the disease prevalence in men and women in either site-specific or overall analysis.
Prevalence of HTN
Previous studies concerning the prevalence of NCDs, especially HTN, have reported different results in some cases. In a cross-sectional study, “the survey of risk factors of noncommunicable diseases”, conducted in 2005 in Iran, high BP was detected in about 25% of the participants [20]. In another study in 2014, which was a part of the Shahroud eye cohort study, high BP was found in 38.2% of the subjects. Furthermore, the prevalence of hypertensive conditions in their data collection was 37.1% for men and 39.0% for women [15]. Kazemi et al. reported a 20.1% prevalence of HTN in a study conducted in Birjand, which was one of the main sites of the current research [13]. Moreover, Bijani et al. stated a 34% prevalence of HTN prevalence in their study based on the PERSIAN cohort study [18]. Also, a prevalence of 18.47% was reported by Zare et al. based on the Zahedan adult cohort study (ZACS) [19]. Additionally, an overall HTN prevalence rate of 26.2% was proposed by Aghaei Meybodi et al. based on the data gathered from 5724 individuals enrolled in Iranian multi-centric osteoporosis studies (IMOS) [21].
The prevalence measured in the current study was higher than that of most of the other studies but lower compared to that reported by Khosravi et al. [15]. Additionally, our results were more closely aligned with those reported by Bijani et al. [18].
Prevalence of the new hypertensive cases
In comparison to Esteghamati et al.’s study in 2005 [20], in which only 34% of hypertensive cases were initially aware of their disease, our study had a 21% reduction in the rate of new HTN recognitions during the screening program. This decline may be attributed to an increasing level of public awareness and early disease diagnosis in medical settings. Moreover, a higher percentage of participants with a history of HTN successfully controlled their BP in our study compared to the referenced paper (68% versus 25%). Additionally, in a more recent investigation, the authors reported that only 27.6% of the individuals with high BP became aware of their hypertensive condition for the first time during the study [8], which also highlights the increasing awareness among people.
Differences between men and women
It is noteworthy that the data were further examined to extract the potential associations and relationships concerning the study population across the cities under investigation. Despite the predominance of men in the study population, we observed no significant difference in both overall and site-specific prevalence of HTN between the sex groups, suggesting that this disease affected both male and female individuals almost equally. This finding deviates from the prevailing global pattern of male sex prevalence [13, 14, 21, 24]. However, Esteghamati et al. reported a relatively equal prevalence of the disease among men and women in their study [20]. Oori et al. also reported no substantial difference between males and females in this regard [16]. On the other hand, the results from the Shahroud eye cohort study showed even higher rates of HTN occurrence in female participants [15].
In comparison to Esteghamati et al.’s study in 2005 [20], which indicated that men were less aware of their hypertensive state than women (22.5% vs 33.1%), we did not find a significant difference between the sex groups and the identification of a new case of HTN.
Differences across the cities under study
Additionally, we observed a higher prevalence of HTN (44.5%) in Gonabad compared to the other three cities. To elucidate this discrepancy in prevalence, a focused examination of the demographic characteristics within the scope of this study is warranted. As discerned from the findings, the highest average age among participants was observed in Gonabad, surpassing the overall population average by approximately seven years. Concerning the association between increasing age and the probability of HTN incidence, as established in various studies [13-15, 18, 20, 21, 25] and reiterated in the present investigation, a direct correlation has been consistently demonstrated. Therefore, it can be postulated that the elevated prevalence of the disease in Gonabad may partially be attributed to this factor. Additionally, although the mean age of new cases is the lowest in Birjand, the detection of new cases is significantly higher than in other cities. Previous studies also show that the detection of new hypertensive cases increases with a reduction in age up to 35 years [20].
Moreover, the disparity observed between the prevalence of newly and previously diagnosed hypertensive cases across the cities under investigation may suggest variations in mean age, level of awareness, and BP monitoring among the residents of these areas.
Conclusion
The discovery of a considerable number of new cases of HTN underscores the necessity for public health awareness initiatives targeting HTN. Policymakers and healthcare professionals should prioritize educating individuals on HTN risks and advocating regular BP monitoring, especially in older populations. Also, in regions with higher HTN prevalence, interventions should include improved healthcare access and targeted awareness campaigns that address unique factors contributing to HTN in the population.
Strengths and limitations
In evaluating the strengths of our study, our inclusion in a larger, well-established cohort provided valuable context and diversity to our study population. The use of clinical assessment data ensured a high level of precision in our findings. However, it is essential to acknowledge certain limitations. The relatively smaller number of participants, compared to similar studies, while offering a focused analysis, may impact the generalizability of our findings. Additionally, it is noteworthy that studies employing the ACC/AHA guidelines for HTN may report a substantially higher prevalence compared to the present study, given that those guidelines define HTN with a lower threshold. Therefore, caution should be exercised when comparing our results with studies using different diagnostic criteria. Our suggestions for potential future research include the examination of the influence of socioeconomic factors on HTN prevalence and the investigation of the prevalence of the disease based on ACC/AHA guidelines.
Ethical Considerations
Compliance with ethical guidelines
The current study was approved by the Ethics Committee of Gonabad University of Medical Sciences (Code: IR.GMU.REC.1398.038). The participants provided written informed consent to take part in this study and were assured that their information would remain confidential.
Funding
This study was funded by the Student Research Committee of Gonabad University of Medical Sciences (Grant No.: 123/F/T/S/810).
Authors' contributions
Study design, statistical analysis, intervention and initial draft preparation: Ali Alami, Reza Akhondi, and Ali Nasimi; Data collection: Reza Akhondi, Ali Nasimi, Mahsa Ghomi, Seyed Reza Seyedhosseini, and Arefeh Pouraidi; Review and editing: Ali Alami, and Reza Akhondi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude and appreciation to all those who played a role in the implementation of this research and facilitated its process.
References
Hypertension (HTN) or high blood pressure (BP), defined by systolic BP≥140 mm Hg or diastolic BP≥90 mm Hg, is one of the major contributors to morbidity and mortality around the world [1]. It is estimated to be the leading cause of death in approximately 10 million individuals annually across the globe [2]. Together with diabetes mellitus, low-density lipoprotein cholesterol levels, body mass index, and smoking, HTN is considered a modifiable risk factor for cardiovascular diseases [3]. Furthermore, evidence supports that having pathological high BP can elevate the risk of sudden death and mortality, particularly due to chronic disorders in other systems, such as chronic renal failure [4].
HTN affects 33% of adults aged between 30 and 79 years worldwide [5], with a slightly higher prevalence in men (34%) compared to women (32%) [4]. Although there were declines in developed countries, the total number of adults with HTN increased from 650 million in 1990 to 1.3 billion in 2019, with most of them living in undeveloped and developing countries [6]. Despite this increase, the overall global prevalence of HTN remained relatively constant from 1990 to 2019 [6]. Over the years, numerous studies have sought to unravel the prevalence and patterns of HTN in Iran, providing valuable insights into the dynamics of this health condition within the country [7-21]. However, these findings show disparities in some cases. For example, according to a systematic review, the mean prevalence of HTN among the Iranian population is about 25% [16, 17, 22]. In comparison, another study that analyzed the information from the Fasa region of this cohort study reported a total prevalence of 34%, %, which is more consistent with global statistics [18]. Furthermore, the most recent study in this regard suggests that 26.6% of Iranian adults have high BP [12].
The timely identification of individuals in the prehypertensive stage or those with undiagnosed HTN, coupled with the effective restoration of BP within the normative range through pharmacological or non-pharmacological interventions, constitutes key determinants in the prognosis of the disease. Unfortunately, the national program for identifying non-communicable diseases (NCDs) is not effective enough [23].
Given the relatively high prevalence in the population, the burden of the disease, and the availability of effective treatment, it is recommended that screening programs be conducted on a large scale to identify undiagnosed patients and high-risk individuals to minimize the aforementioned complications and costs.
In this study, we aimed to estimate the prevalence of HTN by conducting an organized screening program in the eastern and southeastern regions of Iran. The effectiveness of this study is assessed by identifying the percentage of patients with HTN who were unaware of their condition prior to the implementation of the program.
Methods
In this analytical cross-sectional study conducted in 2019, we included 936 individuals from those who participated in the Iranian National BP measurement campaign (INBPMC). Using a probability proportional to size cluster sampling, the participants were selected from Gonabad, Birjand, Jiroft, and Zabol, four cities located in the Eastern and Southeast regions of Iran. The dependent variable was HTN (the outcome of this study is the percentage of newly identified hypertensive cases), while the independent variables were age, sex, place of residence, and previous history of HTN.
Based on previous research [5] indicating a prevalence of HTN of 45.1%, a sample size of 777 individuals was calculated for the study, with a significance level of 95% and a test power of 80%. In order to increase the accuracy and control potential concerns during the data collection process, an additional 20% was added to the calculated sample size. Equation 1 was used to determine the sample size.
Using a multi-stage sampling method, we selected the participants. First, we determined the required sample size in cities based on their populations. Then, we randomly selected some urban and rural sites that were active in the campaign. We included participants who enrolled in the INBPMC and met the eligibility criteria (inclusion and exclusion criteria). Informed written consent was obtained from the participants before collecting the required data.
Inclusion criteria encompassed individuals who sought services from diverse healthcare facilities, including community health centers, hospitals, and designated stations, within the eastern and southeast regions of the country. Individuals over the age of 30, without diagnosed neuropsychiatric or sensorimotor disorders, and with a minimum of 4 years of education were included in this study. After presenting pertinent information about the research plan and objectives, eligible participants meeting the inclusion criteria were recruited. Then, written informed consent was obtained from the participants, and they completed a checklist that included information, such as age, sex, place of residence, and previous medical history. The BP of the participants was recorded on this checklist. If a participant refused to participate in the study during the data collection process, he/she was excluded from the study. The sampling process continued until the predetermined sample size was reached for each site.
BP measurements were conducted by trained survey personnel using standard methods. BP was assessed using a precisely calibrated sphygmomanometer equipped with a suitably sized cuff, and the readings were recorded to the nearest whole number. The systolic BP (SBP) and diastolic BP (DBP) values were identified based on the first and 5th Korotkoff sounds, respectively. BP was assessed twice in the sitting position for each participant, using the right arm after a 10-minute resting period. The stage of HTN was determined by calculating the average of these two records. Then, the values were recorded on the appropriate checklist that included information regarding age, sex, past medical and drug history, marital status, educational level, place of residence, and measured BP of each person. The participants who had an SBP of <40 mm Hg, a DBP <90 mm Hg, and were not under treatment with any antihypertensive agents were considered normal; otherwise, they were classified as affected by HTN. To control for potential biases, the interviewers in the study received necessary training on the data collection methods during a training session.
Statistical analysis of the collected data was performed using SPSS software, version 20. Descriptive statistics, such as frequency distribution tables and related charts, were employed for qualitative data. Also, quantitative data were characterized using measures of central tendency and dispersion, such as Mean±SD.
Results
We analyzed the data of 936 participants (male: 581, female: 335; M/F ratio=1.73). The Mean±SD age of the participants was 45.48±12.774 years. The mean age of participants in Gonabad (52.32) was significantly higher than in other cities (P=0.001). The prevalence of HTN among the participants was 36.2%.
Table 1 shows that the highest prevalence of HTN was in Gonabad.
The prevalence of HTN by sex is shown in Table 2. Table 2 also shows the old and new cases of HTN, both overall and in each city. It indicates that the percentage of new hypertensive cases in this study was 16.2% (152/936). Besides, 44.8% of the patients with HTN were new hypertensive cases, and the identification of the new hypertensive cases was significantly different among the participants from different cities (Table 2). The Mean±SD age of all hypertensive cases was 50.59±13.480, while the Mean±SD age of newly and previously diagnosed cases was 45.39±11.246 and 54.82±13.088, respectively, with a statistically significant difference found (P<0.001). Among newly diagnosed hypertensive cases, 118 were men and 34 were women. There was no statistically significant difference in the sex distribution of newly diagnosed hypertensive cases across different cities (P=0.509).
As Table 3 demonstrates, there was a significant difference between the mean age of newly diagnosed hypertensive cases and the city of the participants (P=0.04), with the mean age of new cases in Birjand being lower than in other cities.
Additionally, as demonstrated in Figure 1, among the 187 old hypertensive cases (Table 2), only 128 managed to maintain controlled BP, while the remaining 59 were detected with uncontrolled BP.
Discussion
This study was conducted to determine the proportion of new hypertensive cases diagnosed during the INBPMC in the East and Southeast of Iran in 2019-20. The prevalence of HTN in this study was reported as 36.2%, which was significantly higher in Gonabad than in other cities. Among the reported cases, 44.8% were new patients, and the overall percentage of new hypertensive cases in this study was 16.2%. There was a significant association between the prevalence of HTN and residency location. Besides, a statistically significant difference was observed between the identification of new hypertensive cases and the city of residence of the participants. We did not find a significant relationship between sex and the prevalence of HTN, as well as the identification of new hypertensive cases.
In this study, 36.2% of the population was found to have hypertensive conditions, and among them, 44.8% (16.2% of the total participants) were identified with HTN for the first time. We also found significant differences in the overall prevalence of HTN, the total age average of the participants across the four cities, and the mean age of the hypertensive group compared to non-hypertensive participants. Notably, we observed a meaningful disparity between the prevalence of newly and previously diagnosed hypertensive patients across the four cities. Furthermore, no substantial association was found between the disease prevalence in men and women in either site-specific or overall analysis.
Prevalence of HTN
Previous studies concerning the prevalence of NCDs, especially HTN, have reported different results in some cases. In a cross-sectional study, “the survey of risk factors of noncommunicable diseases”, conducted in 2005 in Iran, high BP was detected in about 25% of the participants [20]. In another study in 2014, which was a part of the Shahroud eye cohort study, high BP was found in 38.2% of the subjects. Furthermore, the prevalence of hypertensive conditions in their data collection was 37.1% for men and 39.0% for women [15]. Kazemi et al. reported a 20.1% prevalence of HTN in a study conducted in Birjand, which was one of the main sites of the current research [13]. Moreover, Bijani et al. stated a 34% prevalence of HTN prevalence in their study based on the PERSIAN cohort study [18]. Also, a prevalence of 18.47% was reported by Zare et al. based on the Zahedan adult cohort study (ZACS) [19]. Additionally, an overall HTN prevalence rate of 26.2% was proposed by Aghaei Meybodi et al. based on the data gathered from 5724 individuals enrolled in Iranian multi-centric osteoporosis studies (IMOS) [21].
The prevalence measured in the current study was higher than that of most of the other studies but lower compared to that reported by Khosravi et al. [15]. Additionally, our results were more closely aligned with those reported by Bijani et al. [18].
Prevalence of the new hypertensive cases
In comparison to Esteghamati et al.’s study in 2005 [20], in which only 34% of hypertensive cases were initially aware of their disease, our study had a 21% reduction in the rate of new HTN recognitions during the screening program. This decline may be attributed to an increasing level of public awareness and early disease diagnosis in medical settings. Moreover, a higher percentage of participants with a history of HTN successfully controlled their BP in our study compared to the referenced paper (68% versus 25%). Additionally, in a more recent investigation, the authors reported that only 27.6% of the individuals with high BP became aware of their hypertensive condition for the first time during the study [8], which also highlights the increasing awareness among people.
Differences between men and women
It is noteworthy that the data were further examined to extract the potential associations and relationships concerning the study population across the cities under investigation. Despite the predominance of men in the study population, we observed no significant difference in both overall and site-specific prevalence of HTN between the sex groups, suggesting that this disease affected both male and female individuals almost equally. This finding deviates from the prevailing global pattern of male sex prevalence [13, 14, 21, 24]. However, Esteghamati et al. reported a relatively equal prevalence of the disease among men and women in their study [20]. Oori et al. also reported no substantial difference between males and females in this regard [16]. On the other hand, the results from the Shahroud eye cohort study showed even higher rates of HTN occurrence in female participants [15].
In comparison to Esteghamati et al.’s study in 2005 [20], which indicated that men were less aware of their hypertensive state than women (22.5% vs 33.1%), we did not find a significant difference between the sex groups and the identification of a new case of HTN.
Differences across the cities under study
Additionally, we observed a higher prevalence of HTN (44.5%) in Gonabad compared to the other three cities. To elucidate this discrepancy in prevalence, a focused examination of the demographic characteristics within the scope of this study is warranted. As discerned from the findings, the highest average age among participants was observed in Gonabad, surpassing the overall population average by approximately seven years. Concerning the association between increasing age and the probability of HTN incidence, as established in various studies [13-15, 18, 20, 21, 25] and reiterated in the present investigation, a direct correlation has been consistently demonstrated. Therefore, it can be postulated that the elevated prevalence of the disease in Gonabad may partially be attributed to this factor. Additionally, although the mean age of new cases is the lowest in Birjand, the detection of new cases is significantly higher than in other cities. Previous studies also show that the detection of new hypertensive cases increases with a reduction in age up to 35 years [20].
Moreover, the disparity observed between the prevalence of newly and previously diagnosed hypertensive cases across the cities under investigation may suggest variations in mean age, level of awareness, and BP monitoring among the residents of these areas.
Conclusion
The discovery of a considerable number of new cases of HTN underscores the necessity for public health awareness initiatives targeting HTN. Policymakers and healthcare professionals should prioritize educating individuals on HTN risks and advocating regular BP monitoring, especially in older populations. Also, in regions with higher HTN prevalence, interventions should include improved healthcare access and targeted awareness campaigns that address unique factors contributing to HTN in the population.
Strengths and limitations
In evaluating the strengths of our study, our inclusion in a larger, well-established cohort provided valuable context and diversity to our study population. The use of clinical assessment data ensured a high level of precision in our findings. However, it is essential to acknowledge certain limitations. The relatively smaller number of participants, compared to similar studies, while offering a focused analysis, may impact the generalizability of our findings. Additionally, it is noteworthy that studies employing the ACC/AHA guidelines for HTN may report a substantially higher prevalence compared to the present study, given that those guidelines define HTN with a lower threshold. Therefore, caution should be exercised when comparing our results with studies using different diagnostic criteria. Our suggestions for potential future research include the examination of the influence of socioeconomic factors on HTN prevalence and the investigation of the prevalence of the disease based on ACC/AHA guidelines.
Ethical Considerations
Compliance with ethical guidelines
The current study was approved by the Ethics Committee of Gonabad University of Medical Sciences (Code: IR.GMU.REC.1398.038). The participants provided written informed consent to take part in this study and were assured that their information would remain confidential.
Funding
This study was funded by the Student Research Committee of Gonabad University of Medical Sciences (Grant No.: 123/F/T/S/810).
Authors' contributions
Study design, statistical analysis, intervention and initial draft preparation: Ali Alami, Reza Akhondi, and Ali Nasimi; Data collection: Reza Akhondi, Ali Nasimi, Mahsa Ghomi, Seyed Reza Seyedhosseini, and Arefeh Pouraidi; Review and editing: Ali Alami, and Reza Akhondi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude and appreciation to all those who played a role in the implementation of this research and facilitated its process.
References
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003; 42(6):1206-52. [DOI:10.1161/01.HYP.0000107251.49515.c2]
- Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: A systematic analysis for the global burden of disease study 2019. Lancet. 2020; 396(10258):1223-49. [DOI:10.1161/01.HYP.0000107251.49515.c2]
- Magnussen C, Ojeda FM, Leong DP, Alegre-Diaz J, Amouyel P, Aviles-Santa L, et al. Global effect of modifiable risk factors on cardiovascular disease and mortality. The New England Journal of Medicine. 2023; 389(14):1273-85. [DOI:10.1056/NEJMoa2206916]
- Zhou B, Perel P, Mensah GA, Ezzati M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nature Reviews Cardiology. 2021; 18(11):785-802. [DOI:10.1038/s41569-021-00559-8]
- World Health Organization (WHO). Prevalence of hypertension among adults aged 30-79 years. 2023 [Updated 2023 December 28]. Available from: [Link]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021; 398(10304):957-80. [DOI:10.1016/S0140-6736(21)01330-1] [PMID]
- Aleali AM, Latifi SM, Rashidi H, Payami SP, Sabet A. Prevalence of hypertension and prehypertension in adolescence in Ahvaz, Iran. Diabetes & Metabolic Syndrome. 2017; 11(Suppl 2):S547-50. [DOI:10.1016/j.dsx.2017.04.002]
- Najafipour H, Nasri HR, Rostamzadeh F, Amirzadeh R, Shadkam M, Mirzazadeh A. Prevalence and incidence of pre-hypertension and hypertension (awareness/control) in Iran: findings from Kerman coronary artery diseases risk factors study 2 (KERCADRS). Journal of Human Hypertension. 2022; 36(5):461-72. [DOI:10.1038/s41371-020-00392-5]
- Mahdavi M, Parsaeian M, Farzadfar F, Mohamadi E, Olyaeemanesh A, Takian A. Inequality in prevalence, awareness, treatment, and control of hypertension in Iran: The analysis of national households’ data. BMC Public Health. 202; 22(1):2349. [DOI:10.1186/s12889-022-14768-4]
- Allameh M, Ghanei Gheshlagh R, Rahmani K. Prevalence and associated risk factors of hypertension for the middle-aged population (30-59 years) in Iran: A national cross-sectional study. High Blood Pressure & Cardiovascular Prevention. 2022; 29(1):75-80. [DOI:10.1007/s40292-021-00490-6]
- Eghbali M, Khosravi A, Feizi A, Mansouri A, Mahaki B, Sarrafzadegan N. Prevalence, awareness, treatment, control, and risk factors of hypertension among adults: A cross-sectional study in Iran. Epidemiol Health. 2018; 40:e2018020. [DOI:10.4178/epih.e2018020]
- Mohammadi S, Hassanipour S, Delam H, Nikbakht HA, Far ZG, Firoozi D, et al. Prevalence of hypertension in Iran: An updated systematic review and meta-analysis of community-based studies. Caspian Journal of Internal Medicine. 2023; 14(4):607-17. [DOI:10.22088/cjim.14.43.607] [PMID]
- Kazemi T, Hajihosseini M, Mashreghimoghadam H, Azdaki N, Ziaee M. Prevalence and determinants of hypertension among Iranian Adults, Birjand, Iran. International Journal of Preventive Medicine. 2017; 8(1):36. [DOI:10.4103/ijpvm.IJPVM_103_16]
- Hosseini M, Yaseri M, Asady H, Eleojo Musa A, Koohpayehzadeh J, Rafei A, et al. Prevalence of high blood pressure in Iranian adults based on the 2017 ACC/AHA guideline. Medical Journal of The Islamic Republic of Iran. 2019; 33:26. [DOI:10.47176/mjiri.33.26]
- Khosravi A, Emamian MH, Shariati M, Hashemi H, Fotouhi A. The prevalence of pre-hypertension and hypertension in an Iranian urban population. High Blood Pressure & Cardiovascular Prevention. 2014; 21(2):127-35. [DOI:10.1007/s40292-013-0035-y]
- Oori MJ, Mohammadi F, Norozi K, Fallahi-Khoshknab M, Ebadi A, Gheshlagh RG. Prevalence of HTN in Iran: Meta-analysis of published studies in 2004-2018. Current Hypertension Reviews. 2019; 15(2):113-22. [DOI:10.2174/1573402115666190118142818]
- Sepanlou S, Najafi F, Poustchi H, Parsaeian M, Ahmadi A, Somi M, et al. Prevalence, awareness, treatment, and control of hypertension based on ACC/AHA versus JNC7 guidelines in the Persian cohort study. Scientific Reports. 2022; 12(1):4057. [DOI:10.1038/s41598-022-07896-9]
- Bijani M, Parvizi S, Dehghan A, Sedigh-Rahimabadi M, Rostami-chijan M, Kazemi M, et al. Investigating the prevalence of hypertension and its associated risk factors in a population-based study: Fasa PERSIAN COHORT data. BMC Cardiovascular Disorders. 2020; 20(1):503. [DOI:10.1186/s12872-020-01797-3]
- Zare MG, Okati-Aliaba H, Ansari-Moghadda A, Mohammadi M, Shahraki-Sanav F. Prevalence and risk factors of pre-hypertension and hypertension among adults in Southeastern Iran: Findings from the baseline survey of the Zahedan adult cohort study. Plos One. 2023; 18(12):e0295270. [DOI:10.1371/journal.pone.0295270]
- Esteghamati A, Abbasi M, Alikhani S, Gouya MM, Delavari A, Shishehbor MH, et al. Prevalence, awareness, treatment, and risk factors associated with hypertension in the Iranian population: The national survey of risk factors for noncommunicable diseases of Iran. American Journal of Hypertension. 2008; 21(6):620-6. [DOI:10.1038/ajh.2008.154] [PMID]
- Aghaei Meybodi HR, Khashayar P, Rezai Homami M, Heshmat R, Larijani B. Prevalence of hypertension in an Iranian population. Renal Failure. 2014; 36(1):87-91. [DOI:10.3109/0886022X.2013.832315]
- Poustchi H, Eghtesad S, Kamangar F, Etemadi A, Keshtkar AA, Hekmatdoost A, et al. Prospective epidemiological research studies in Iran (the PERSIAN cohort study): Rationale, objectives, and design. Am J Epidemiol. 2018; 187(4):647-55. [DOI:10.1093/aje/kwx314] [PMID]
- Shams M, Pariani A, Raeisi A, Maleki M, Shariatinia S, Jamalizadeh A, et al. The Iranian national blood pressure measurement campaign: What do the process and output evaluation say? Archives of Iranian medicine. 2022; 25(11):718. [DOI:10.34172/aim.2022.113]
- Di Giosia P, Giorgini P, Stamerra CA, Petrarca M, Ferri C, Sahebkar A. Gender differences in epidemiology, pathophysiology, and treatment of hypertension. Current Atherosclerosis Reports. 2018; 20:1-7. [DOI:10.1007/s11883-018-0716-z]
- Buford TW. Hypertension and aging. Ageing Research Reviews. 2016; 26:96-111. [DOI:10.1016/j.arr.2016.01.007]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2024/02/14 | Accepted: 2024/05/15 | Published: 2024/10/28
Received: 2024/02/14 | Accepted: 2024/05/15 | Published: 2024/10/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
