

Volume 14, Issue 6 (Nov & Dec 2024)
J Research Health 2024, 14(6): 515-526 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Parihar P, Mishra R, Khare S, Tiwari G K. Demographic Factors and Self-compassion as Predictors of Positive Mental Health in Married Hindu Couples. J Research Health 2024; 14 (6) :515-526
URL: http://jrh.gmu.ac.ir/article-1-2519-en.html
URL: http://jrh.gmu.ac.ir/article-1-2519-en.html



1- Department of Psychology, School of Humanities, Starex University, Gurugram, India.
2- Department of Psychology, School of Humanities & Social Sciences, Doctor Harisingh Gour Vishwavidyalaya, Sagar, India.
3- Department of Psychology, School of Humanities & Social Sciences, Doctor Harisingh Gour Vishwavidyalaya, Sagar, India. ,gyaneshpsychology@gmail.com
2- Department of Psychology, School of Humanities & Social Sciences, Doctor Harisingh Gour Vishwavidyalaya, Sagar, India.
3- Department of Psychology, School of Humanities & Social Sciences, Doctor Harisingh Gour Vishwavidyalaya, Sagar, India. ,
Keywords: Correlation study, Demographic factors, Married persons, Psychological well-being, Regression analyses, Self-compassion
Full-Text [PDF 693 kb]
(737 Downloads)
| Abstract (HTML) (6635 Views)
Full-Text: (1472 Views)
Introduction
In recent years, there has been a growing interest in exploring the concept of self-compassion, derived from Buddhism. Studies indicate that this construct is pertinent in comprehending various life outcomes across diverse age groups, regardless of cultural affiliations [1-3]. Self-compassion involves displaying warmth and understanding toward oneself when confronted with failure, adversity, or feelings of inadequacy [4-6]. It is characterized by three contrasting dimensions: Self-kindness versus self-judgment, recognizing common humanity versus experiencing isolation, and practicing mindfulness versus over-identification [4]. Studies indicate that individuals who cultivate self-compassion are less prone to developing mental health issues, more inclined to report heightened life satisfaction, and exhibit effective coping skills and enhanced emotional intelligence [3, 7]. The cultivation of self-compassion contributes to mental health and overall well-being, facilitating the management of challenging life circumstances and the regulation of emotions. The positive equilibrium resulting from self-compassion fosters increased flourishing) [8, 9]. Consequently, self-compassion exerts favorable effects on mental health and well-being [5, 10].
Dreisoerner et al. highlighted essential aspects of self-compassion, such as the inclination toward kindness and empathy, the capacity to be touched by one’s distress, and the ability to endure and make sense of this stress [11]. Various theoretical frameworks have been put forward to elucidate the relationship between self-compassion and personal well-being [12, 13]. Self-compassion is instrumental in achieving life objectives by mitigating the adverse emotional impacts of perceived shortcomings and failures [3]. According to goal theories, the achievement of goals is directly linked to well-being. In contrast, the cognitive perspective posits that self-compassion does not directly lead to well-being but rather aids in balancing positive and negative experiences [13]. Additionally, adaptation theory, also known as set-point theory or the hedonic treadmill, uses historical comparisons to assess well-being, suggesting that an individual’s well-being temporarily fluctuates with changes in life circumstances [13, 14].
Studies indicate the importance of self-compassion in understanding mental health and the dynamics of relationships [3]. Creating a nurturing, healing environment can enhance self-compassion and acknowledging the role of family and social contexts in healing is crucial. While most research has traditionally examined self-compassion from an individual standpoint, there has been limited investigation into its effects on the well-being of married couples [15, 16]. Furthermore, research shows that compassion development is either encouraged or greatly hindered by various social and cultural norms [17]. Possessing self-compassion has been linked to better psychological health. Those with higher levels of self-compassion often experience less stress, anxiety, and depressive symptoms [18]. Additionally, self-compassion is correlated with positive emotional states, including increased happiness, optimism, and life satisfaction [4, 19]. Interestingly, people who are more compassionate toward others tend to extend the same compassion toward themselves [20, 21]. Recent research points out that the positive (self-kindness, common humanity, mindfulness) and negative (self-judgment, isolation, over-identification) aspects of Neff’’s (2003) model of self-compassion represent distinct concepts [1]. It is more effective to use them as separate measures for self-compassion and self-coldness [7, 8, 22].
Distinct from other religious traditions, Hindu marriage is regarded not just as a contractual :union: but as a sacred rite, serving both earthly and spiritual objectives. Investigating how self-compassion affects well-being in Hindu couples who are married could unveil fresh insights into how self-compassion interacts with emotional dynamics and the achievement of goals [23, 24]. Additionally, the impact of social class on the nexus between self-compassion and well-being in these couples is noteworthy. Those from lower social classes, typically marked by reduced financial means (lesser income, lower educational attainment) and a diminished social standing, often encounter tougher living conditions than individuals from higher social strata [25]. This disparity in resources and social status is thought to significantly influence the emotional experiences of those in the lower social class.
Research indicates that individuals from lower socioeconomic backgrounds exhibit heightened emotional responses to uncertain and negative social scenarios [26, 27]. Social class, as a hierarchical construct, is determined by an individual’s accumulation of material resources [28]. Those belonging to the lower socioeconomic stratum often find themselves in challenging environments characterized by increased threats and barriers, such as less secure neighborhoods and underfunded educational systems. These individuals typically face difficulties in leveraging their limited resources to surmount these challenges [27]. Consequently, there is a pressing need for further studies to explore this subject in greater depth, particularly focusing on how demographic and personal factors influence the interplay between self-compassion and well-being among married couples [12].
Given the importance of self-compassion in promoting resilience, adaptive coping strategies, and emotional well-being, this study aimed to examine its influence on well-being among married Hindu couples. While previous research has largely focused on individual perspectives, there is little research on the effects of self-compassion on the well-being of couples [9, 29]. This gap is particularly noteworthy given the sacred, multidimensional nature of Hindu marriage, which extends beyond contractual bonds. Moreover, the role of demographic factors (education, domicile, employment status, length of marriage, number of children, nature of family, family size and socioeconomic status) in this relationship remains understudied, particularly in light of potential disparities in resources and emotional experiences. This research aimed to address these gaps and advance our understanding of the role of self-compassion in improving the well-being of married Hindu couples across diverse demographics. Research findings on self-compassion and marital well-being among Hindu couples will enrich existing models of self-compassion by examining its impact in a specific cultural context and offering insights into its role in married life. Practitioners can use these findings to develop culturally sensitive interventions aimed at enhancing self-compassion in couples, improving relationship satisfaction and addressing the unique challenges faced by Hindu couples during rehabilitation and therapy. Policymakers can leverage this research to create supportive community programs that promote self-compassion, mental health, and well-being, particularly for lower social classes that face greater challenges and disparities.
Against this context, the current research aimed to investigate the relationship between self-compassion and well-being in married Hindu couples, assessing both the nature and extent of this association. Furthermore, the study sought to determine the proportion of variance in different well-being metrics that could be attributed to self-compassion within this demographic. Drawing from existing literature, our hypotheses posit that the positive aspects of self-compassion are much more likely to be positively correlated with and significantly contribute to, the variance observed in various well-being indices. Conversely, the negative aspects of self-compassion are expected to either have low positive or negative correlations, resulting in limited or adverse effects on the variability observed in well-being measurements.
Methods
Study design
A correlational design was employed for data collection, processing, and analysis. This design helps identify patterns and relationships and predict behaviors and outcomes.
Sample
Participants were chosen using the snowball sampling method, in which existing participants provided referrals to other potential participants for the study. This sampling method helped in finding and choosing the participants with ease. The study chose 300 Hindu couples (age range=26-50 years, Mean±SD, 38.42±7.89) in 2022. The participants were chosen from Sagar City and adjoining areas, in Madhya Pradesh, India. The majority of these participants were from lower-middle-class Hindu families, residing in both rural and urban areas. Based on Cohen’s (1988) guidelines for correlational design, a medium effect size of 0.30 was selected with a significance level of 0.05 and a power of 0.80 [30, 31]. The estimated sample size required to detect this effect size was 67 cases, calculated using G*Power software, version 3 [32]. We selected a sample size of 300 participants, which was sufficient to achieve the study objectives.
Inclusion and exclusion criteria
The research included participants who had a minimum of five years of experience in marriage and exhibited no evident physical or mental health issues. Participation was limited to Hindu couples who were 26 years old or older. The inclusion criterion was passing at least five years of married life to ensure sufficient experience with the basic issues and dynamics of married life. Couples who belonged to other religious communities, had health problems, were married for less than five years, or did not fall within the required age range were excluded from the study. The demographic details are given in Table 1.

Study measures
The following measures were used to collect the data:
Self-compassion scale
The couples’ self-compassion was assessed using the self-compassion scale [4]. This instrument evaluates the thoughts, feelings, and behaviors integral to the various elements of self-compassion. It encompasses a total of 26 items that gauge the frequency with which individuals experience feelings of inadequacy or self-criticism through aspects such as self-kindness, self-judgment, common humanity, isolation, mindfulness and over-identification. The scale is divided into six subcategories: Self-kindness (five items), self-judgment (five items), common humanity (four items), isolation (four items), mindfulness (four items) and over-identification (four items), each rated on a five-point scale ranging from ‘almost never’ to ‘almost always’. The items on the self-kindness, common humanity, and mindfulness subscales are assigned 1, 2, 3, 4 and 5 points for responses ranging from almost never to almost always. Reverse scoring was applied to responses on the self-judgment, isolation, and over-identification subscales. A total score from these subscales indicates participants’ overall self-compassion; the higher the scores on the measure, the greater the self-compassion. The minimum and maximum range of scores on the scale is from 26 to 130. The Cronbach’s α for the scale in the present sample was 0.571. The reliability and validity of the scale have been well-documented in previous research [3, 7]. Studies with diverse participant groups have consistently reported the scale’s internal reliability as satisfactory [7, 20].
Mental health continuum-short form (MHC-SF)
The MHC-SF [33] was utilized to assess the well-being of couples. This scale is rooted in research on emotional well-being [34], including both hedonic (subjective or emotional) and psychological well-being [35], as well as social well-being [36]. It comprises 14 items, asking participants to reflect on their experiences over the previous month and respond using a six-point scale ranging from ‘never’ to ‘every day, scored from one to six.’ The minimum and maximum scores on the scale are from 14 to 84. The amalgamation of psychological and social well-being scores provides a measure of eudaimonic well-being. The overall score obtained from this scale is indicative of human flourishing. The scale’s internal consistency reliability in the present sample was notably high, exceeding 0.80 [33].
Socioeconomic status scale
The socioeconomic status scale [37] served as the instrument for gauging the economic and social standing of the couples involved in the study. This particular scale is comprised of 22 items, each offering a selection of multiple-choice responses. Based on their scores, individuals and families were categorized into one of six distinct groups: Upper high (>76), high (61-75), upper middle (46-60), lower middle (31-45), poor (16-30), and very poor or below poverty line (<15). The scoring thresholds set by this scale–below 45, between 45 and 60 and above 61–correspond to low, medium and high socioeconomic statuses, respectively [37]. This scale has been frequently utilized by researchers in the field of behavioral science [9, 29].
Data analysis plan
The acquired raw values were organized based on the study’s design. Once the data collection process concluded, they underwent analysis using SPSS software, version 26. The analysis encompassed the computation of Mean±SD, Pearson product moment correlation coefficients, and stepwise regression analyses to analyze the relationships between variables and test the study hypotheses. The significance level was ≤0.05.
Results
The findings are presented in three sections. The first section is devoted to the demographic attributes of the participants. The second section to the analysis of correlation coefficients, while the third section is devoted to the discussion of hierarchical regression analyses.
Demographic attributes
There were 178 non-graduates (29.70%) and 422 graduates (70.30%). The number of male and female participants was equal, namely 300. Their age ranged from 26 to 50 years and belonged to both rural (103) and urban (497) areas. Forty percent (360) were employed while 240 were unemployed (40%). Their married life ranged from 6 to 29 years and they had 0 to 6 children. The majority of them belonged to joint families (63.80%) and the remaining 36.20% belonged to nuclear families. On average, each couple lived in a family with 2 to 31 members. Participants varied in their socioeconomic status. They belonged to upper-high (>76) (n=89, percent=15.10), high (61-67) (n=132, percent=21.90), upper-middle (46-60) (n=283, percent=47.20), lower-middle (31-45) (n=81, percent=13.6) and poor (16-30) (n=15, percent=2.50) levels of socioeconomic status. There were 178 non-graduates (29.70%) and 422 graduates (70.30%). The number of male and female participants was equal, with each group comprising 300 individuals. Their ages ranged from 26 to 50 years, and they belonged to both rural (103) and urban (497) areas. Forty percent (360) were employed, while 240 were unemployed (40%). Their married lives ranged from 6 to 29 years and they had between 0 and 6 children. The majority of participants belonged to joint families (63.80%), while the remaining 36.20% belonged to nuclear families. On average, each couple lived in a family with 2 to 31 members. Participants varied in their socioeconomic status, belonging to upper-high (>76) (n=89, percent=15.10), high (61-75) (n=132, percent=21.90), upper-middle (46-60) (n=283, percent=47.20), lower-middle (31-45) (n=81, percent=13.6) and poor (16-30) (n=15, percent=2.50) levels of socioeconomic status.
Correlation analysis
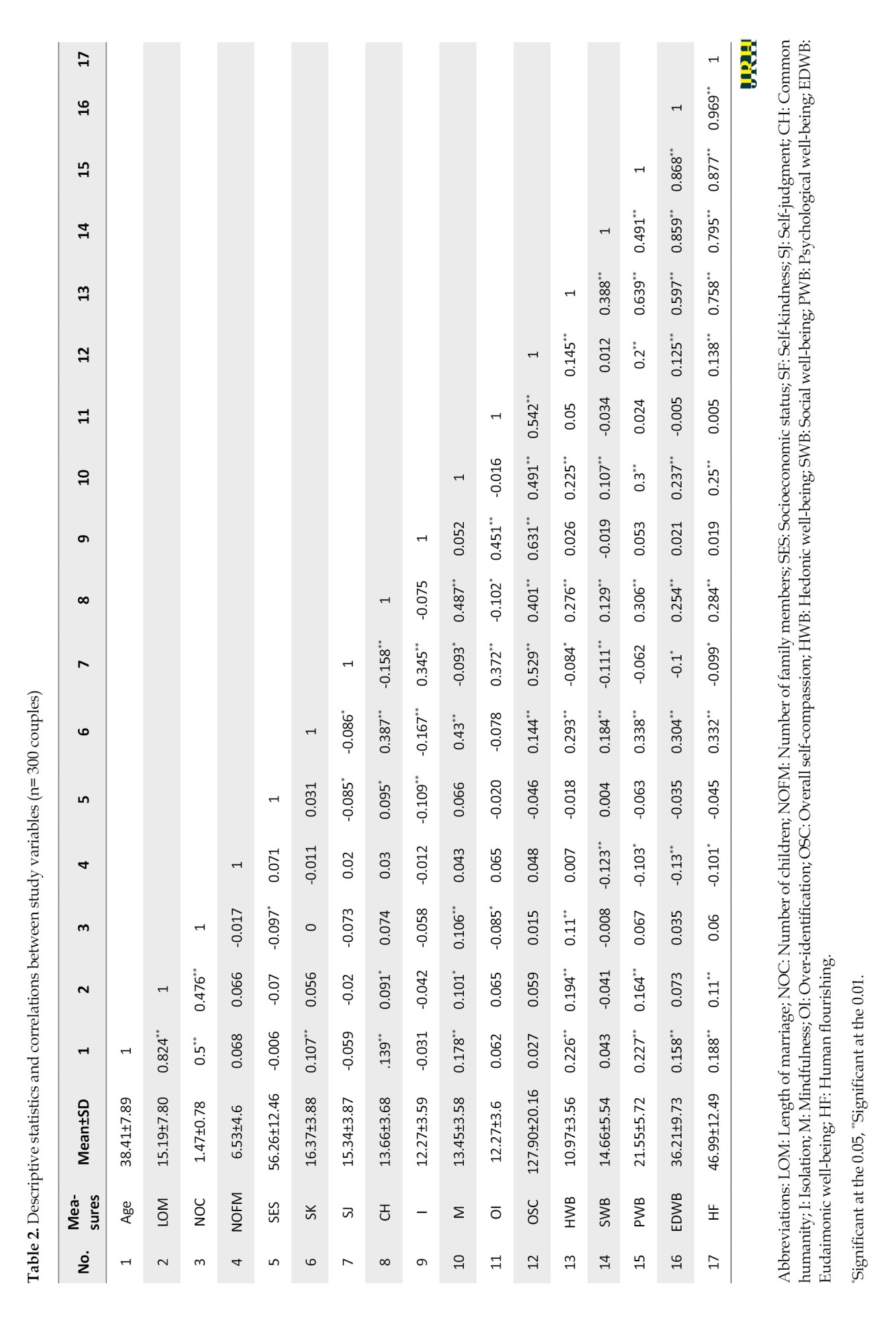
Table 2 illustrates significant positive correlations between age and hedonic well-being (r=0.226, P>0.01), psychological well-being (r=0.227, P>0.01), eudaimonic well-being (r=0.158, P>0.01) and human flourishing (r=0.188, P>0.01). The number of children had a positive correlation with hedonic well-being (r=0.110, P>0.01). The number of family members had negative correlations with social well-being (r=-0.123, P>0.01), psychological well-being (r=-0.103, P>0.01), eudaimonic well-being (r=-0.130, P>0.01) and human flourishing (r=-0.101, P>0.01). Self-kindness showed positive correlations with hedonic well-being (r=0.293, P>0.01), social well-being (r=0.184, P>0.01), psychological well-being (r=0.338, P>0.01), eudaimonic well-being (r=0.304, P>0.01) and human flourishing (r=0.332, P>0.01). Similarly, common humanity exhibited positive significant correlations with hedonic well-being (r=0.276, P>0.01), social well-being (r=0.129, P>0.01), psychological well-being (r=0.306, P>0.01), eudaimonic well-being (r=0.254, P>0.01) and human flourishing (r=0.284, P>0.01). Mindfulness indicated positive correlations with hedonic well-being (r=0.225, P>0.01), social well-being (r=0.107, P>0.01), psychological well-being (r=0.300, P>0.01), eudaimonic well-being (r=0.237, P>0.01) and human flourishing (r=0.250, P>0.01). Thus, positive aspects of self-compassion had positive correlations with different components of well-being. Conversely, self-judgment showed negative correlations with hedonic well-being (r=-0.084, P>0.05), social well-being (r=-0.111, P>0.01), eudaimonic well-being (r=-0.100, P>0.05), and human flourishing (r=-0.099, P>0.05). Isolation and over-identification exhibited non-significant, very weak negative or positive correlations with the well-being indices (Table 2).
Hierarchical regression analysis
Analysis of the standard residuals revealed no outliers in the data (min=-1.9, max=1.7). The data also met the independent error requirement, as indicated by a Durbin-Watson value of 1.63. Further tests for collinearity showed that multicollinearity was not a problem (tolerance=0.94). Furthermore, the scatter plot of standardized predicted values confirmed that the data met the assumptions of homogeneity of variance and linearity.
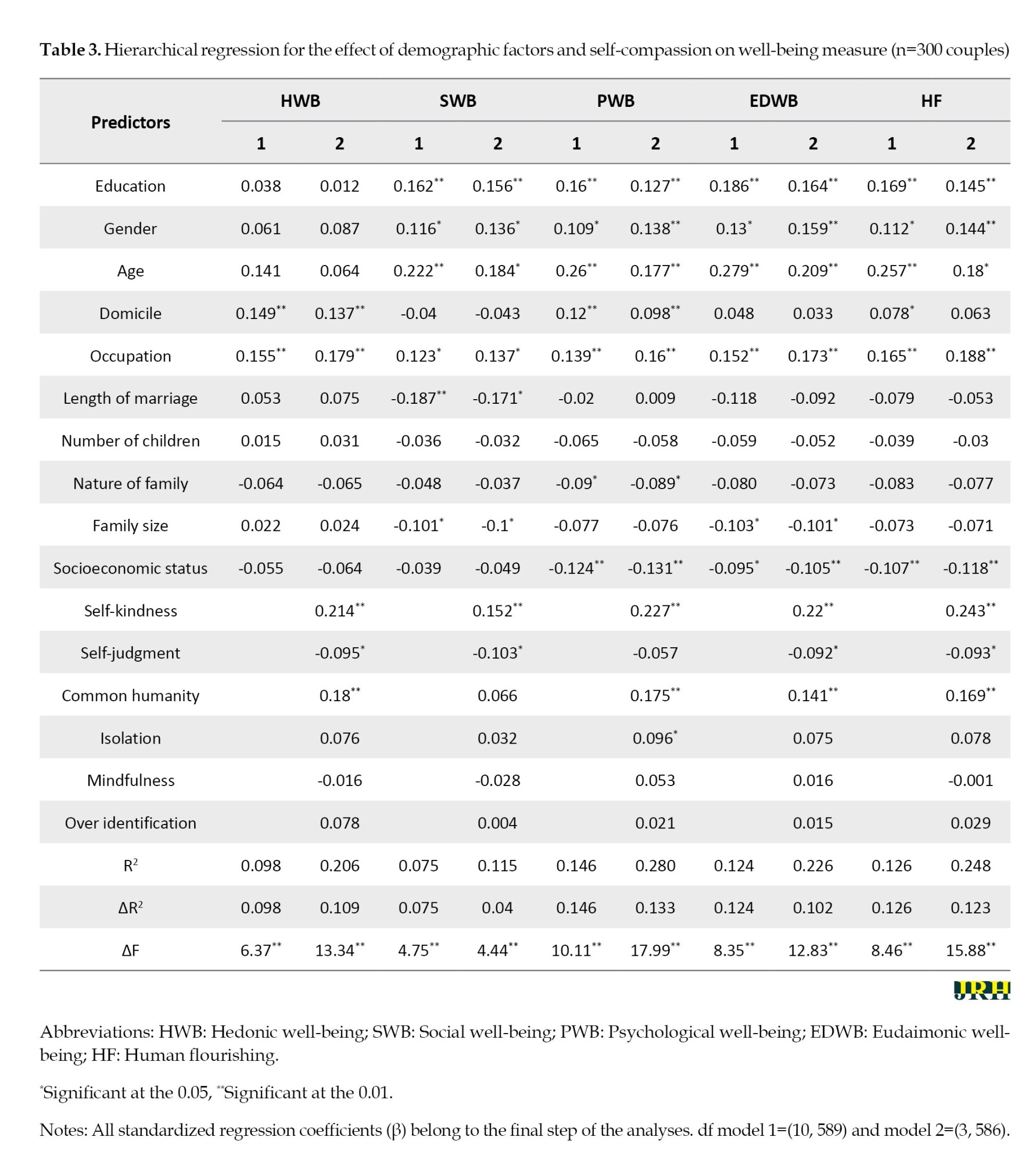
In the initial stage of the analysis, a range of demographic factors (including education level, gender, age, place of residence, occupation, marriage duration, number of children, family type, family size and socioeconomic status) were considered, as detailed in step 1. This was followed by the incorporation of variables, such as self-kindness, self-judgment, feelings of common humanity versus isolation, mindfulness, and the tendency for over-identification in step 2 (Table 3). The findings revealed that these demographic factors significantly influenced the outcomes, explaining 9.8% of the variance in hedonic well-being (R2=0.098, F(10, 589)=6.37, P<0.001). In addition, these demographic factors collectively contributed 7.5% to social well-being (R2=0.075, F(10, 589)=4.75, P<0.001), 14.6% to psychological well-being (R2=0.146, F(10, 589)=10.11, P<0.001), 12.4% to eudaimonic well-being (R2=0.124, F(10, 589)=8.35, P<0.001), and 12.6% to human flourishing (R2=0.126, F(10, 589)=8.46, P<0.001), as demonstrated in model 1 for each facet of human well-being.
The findings revealed that factors, such as self-kindness, self-judgment, a sense of shared humanity, feelings of isolation, mindfulness and tendencies toward over-identification contributed variably to different aspects of well-being. Specifically, these factors were responsible for 20.6% of hedonic well-being (R2=0.206, F(3, 586) =13.34, P<0.001), 11.5% of social well-being (R2=0.115, F(3, 586)=4.44, P<0.001), 28.0% of psychological well-being (R2=0.280, F(3, 586)=17.99, P<0.001), 22.6% of eudaimonic well-being (R2=0.226, F(3, 586)=12.83, P<0.001), and 24.8% of flourishing (R2=0.248, F(3, 586)=15.88, P<0.001), as indicated in Table 3. Additionally, integrating these factors at step 2 in the model for hedonic well-being led to a significant alteration, with a 0.109 unit (β) increase in hedonic well-being.
In the realm of social well-being, integrating factors, such as self-kindness, self-judgment, a sense of shared humanity, feelings of isolation, mindfulness, and tendencies toward over-identification at the second level resulted in a noteworthy enhancement of 0.040 units (β). Similarly, incorporating these same factors in the second phase led to a substantial improvement of 0.133 units (β) in psychological well-being. Additionally, the inclusion of these components in the second step was responsible for a significant increase of 0.102 units (β) in eudaimonic well-being. Moreover, this integration at the same stage also accounted for an important enhancement of 0.123 units (β) in the measure of flourishing, as detailed in Table 3.
Discussion
This study investigated the relationship between self-compassion and well-being in married Hindu couples. It examined how different aspects of well-being were influenced by self-compassion and other demographics. Positive aspects of self-compassion, like self-kindness, common humanity, and mindfulness were found to correlate positively with well-being. In contrast, negative aspects, such as self-judgment, isolation and over-identification showed weaker positive or negative correlations with well-being. Additionally, biographical factors, such as education, age, domicile, occupation, length of marriage, and family size also played a significant role in shaping well-being in various ways. Positive variability in various dimensions of well-being was observed with self-kindness and common humanity, while self-judgment led to negative variability.
Positive aspects of self-compassion (self-kindness, common humanity, and mindfulness) can boost the well-being of married couples by nurturing a supportive and understanding relationship. By approaching their own and their partner’s imperfections with kindness and acceptance, individuals foster greater positive mental health. This mindset enables empathetic and patient responses during conflicts and facilitates open and effective communication that strengthens emotional bonds and mutual support. Positive aspects of self-compassion also reduce stress and prevent resentment, promote a harmonious and loving relationship, and ultimately improve emotional intimacy and marital longevity [38-40]. The study hypothesized that positive aspects of self-compassion (self-kindness, common humanity, and mindfulness) would be positively correlated with various well-being indices, while negative aspects would yield poorer positive or negative correlations. The results largely support these hypotheses, with many demographic findings proving to be novel because these demographic variables have not been empirically examined previously.
Research has shown that education, gender, age, domicile and employment status significantly influence couples’ well-being. Higher education was associated with greater understanding, knowledge, career prospects, attributions, coping skills, and resilience to life events [38, 39], which likely boosted well-being. Gender disparities in access to resources and opportunities continue to exist in India [40].
Gender differences in well-being, which often favor men, may result from disparities in access to socio-cultural norms and socialization processes, as well as positive personal traits, such as self-forgiveness, self-compassion, and self-esteem [7, 10, 41, 42]. Over time, spouses adapt to each other’s life experiences during marriage, potentially leading to improved well-being over a longer marriage duration [40, 43]. Factors, such as family type (nuclear vs. joint family), family size, and socioeconomic status also play roles in well-being by introducing various experiences and opportunities. These factors highlight the influence of demographic factors on the well-being of married Hindu couples.
Research suggests that women typically demonstrate higher self-compassion than men, which leads to better well-being in marital relationships [7, 8]. Self-compassion involves treating oneself kindly, acknowledging one’s humanity and maintaining a positive perspective during challenging times. Social and cultural influences may account for this difference, as women often prioritize relationships and emotional expression, fostering self-awareness and empathy. These qualities help women deal with marital problems with patience and understanding, resulting in more positive relationship dynamics. By embracing self-compassion, women experience reduced stress and anxiety, thereby enhancing overall well-being.
Research suggests that couples’ well-being is affected by their self-compassionate characteristics. Positive aspects of self-compassion, such as self-kindness, common humanity, and mindfulness, have a positive influence on couples’ well-being. In contrast, negative aspects, like harsh self-judgment, isolation and over-identification with personal flaws harm well-being. The study highlights that beneficial components of self-compassion include self-kindness, common humanity, mindfulness, self-acceptance, patience with negative traits, and acknowledgment of shared challenges. These qualities of self-compassion contribute to emotional stability, clear perception, analytical reflection on failures, and openness to challenging experiences [4, 5, 7].
Conversely, negative aspects of self-compassion involve self-judgment, isolation, and over-identification, including harsh self-judgment, difficulty accepting mistakes, self-deprecation, and loneliness. These behaviors can lead to unfavorable comparisons with others, heightened feelings of solitude during personal failures, and an overemphasis on certain events [7, 8]. The nurturing aspects of self-compassion contribute significantly to its predictive power on various indicators of well-being. Research suggests that demographic attributes and personal resources play a crucial role in the well-being of couples. In Hindu marriages, secular and spiritual life goals are interlinked, and the growing influence of postmodern lifestyles emphasizes the importance of socioeconomic factors in couple dynamics [29].
A meta-analysis showed a close link between self-compassion and well-being [12, 24]. The review found that women had higher self-compassion levels and greater well-being than men, and the association between self-compassion and psychological well-being was particularly stronger in women. Factors, such as domicile, age, education, and family dynamics have been found to impact the relationship between self-compassion and positive mental health [12, 24], which is consistent with the findings of the current study.
In essence, this study delves into the connection between self-compassion and well-being in married Hindu couples while incorporating demographic factors influencing well-being. The research is consistent with previous studies and shows that self-compassion has a positive impact on well-being through attributes, like self-kindness, mindfulness, and common humanity [3, 5, 6]. The study advances existing research by illustrating how factors, such as education, age, occupation, and marriage length interact with self-compassion and affect well-being. Past research has pointed to gender differences in self-compassion and well-being, often in favor of women [6-8], which this study supports by exploring the cultural and socioeconomic aspects of Hindu marriages. While confirming the adverse effects of negative self-compassion traits, like self-judgment and isolation on well-being, the study also highlights the demographic intricacies of the Hindu marital context and advances understanding of the role of self-compassion in marital well-being in the Indian cultural context.
Conclusion
The findings of the research affirm the significance of self-compassion in influencing the overall well-being of Hindu couples in marital relationships. Furthermore, the study highlights the substantial impact of demographic variables, including education, gender, age, geographical location, occupation, length of marriage, family size and socioeconomic status, on the well-being of the individuals involved.
Implications, future directions and limitations
The study’s findings are significant for researchers, policymakers, and practitioners in the field. Practical applications include offering self-compassion workshops to help individuals build self-compassion. Policies that give men and women equal access to resources can balance well-being across genders. Open, honest discussions between partners can enhance mutual understanding and improve marital adjustment. Encouraging couples to practice self-acceptance and patience can create a supportive environment and reduce self-criticism. Offering training and resources can help improve couples’ resilience and coping strategies to overcome challenges. Helping couples make informed family decisions can improve their well-being. Incorporating mindfulness exercises and promoting social engagement can improve emotional stability and strengthen social support networks. Professional advice can help you overcome difficulties and strengthen relationships, especially in challenging times. Practitioners can use these insights to develop interventions that target self-compassion and demographic factors to improve marital well-being and mental health. The study can also guide policies to promote educational and socioeconomic equality to improve well-being. The small sample size, the inclusion of only Hindu married couples, and a limited number of variables are some limitations of the study. Future studies could address these limitations by using larger and more diverse samples, incorporating qualitative methods, and examining additional variables related to marital well-being. The current findings can be used to deepen our understanding of the complex factors that influence marital well-being.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by Ethics Committee of Doctor Harisingh Gour Vishwavidyalaya (Code: DHSGV/IEC/2021/10). Written consent was taken from each participant, and their confidentiality and privacy were maintained by anonymizing their details.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the support and contributions of the participants who generously devoted their valuable time to the study.
References
In recent years, there has been a growing interest in exploring the concept of self-compassion, derived from Buddhism. Studies indicate that this construct is pertinent in comprehending various life outcomes across diverse age groups, regardless of cultural affiliations [1-3]. Self-compassion involves displaying warmth and understanding toward oneself when confronted with failure, adversity, or feelings of inadequacy [4-6]. It is characterized by three contrasting dimensions: Self-kindness versus self-judgment, recognizing common humanity versus experiencing isolation, and practicing mindfulness versus over-identification [4]. Studies indicate that individuals who cultivate self-compassion are less prone to developing mental health issues, more inclined to report heightened life satisfaction, and exhibit effective coping skills and enhanced emotional intelligence [3, 7]. The cultivation of self-compassion contributes to mental health and overall well-being, facilitating the management of challenging life circumstances and the regulation of emotions. The positive equilibrium resulting from self-compassion fosters increased flourishing) [8, 9]. Consequently, self-compassion exerts favorable effects on mental health and well-being [5, 10].
Dreisoerner et al. highlighted essential aspects of self-compassion, such as the inclination toward kindness and empathy, the capacity to be touched by one’s distress, and the ability to endure and make sense of this stress [11]. Various theoretical frameworks have been put forward to elucidate the relationship between self-compassion and personal well-being [12, 13]. Self-compassion is instrumental in achieving life objectives by mitigating the adverse emotional impacts of perceived shortcomings and failures [3]. According to goal theories, the achievement of goals is directly linked to well-being. In contrast, the cognitive perspective posits that self-compassion does not directly lead to well-being but rather aids in balancing positive and negative experiences [13]. Additionally, adaptation theory, also known as set-point theory or the hedonic treadmill, uses historical comparisons to assess well-being, suggesting that an individual’s well-being temporarily fluctuates with changes in life circumstances [13, 14].
Studies indicate the importance of self-compassion in understanding mental health and the dynamics of relationships [3]. Creating a nurturing, healing environment can enhance self-compassion and acknowledging the role of family and social contexts in healing is crucial. While most research has traditionally examined self-compassion from an individual standpoint, there has been limited investigation into its effects on the well-being of married couples [15, 16]. Furthermore, research shows that compassion development is either encouraged or greatly hindered by various social and cultural norms [17]. Possessing self-compassion has been linked to better psychological health. Those with higher levels of self-compassion often experience less stress, anxiety, and depressive symptoms [18]. Additionally, self-compassion is correlated with positive emotional states, including increased happiness, optimism, and life satisfaction [4, 19]. Interestingly, people who are more compassionate toward others tend to extend the same compassion toward themselves [20, 21]. Recent research points out that the positive (self-kindness, common humanity, mindfulness) and negative (self-judgment, isolation, over-identification) aspects of Neff’’s (2003) model of self-compassion represent distinct concepts [1]. It is more effective to use them as separate measures for self-compassion and self-coldness [7, 8, 22].
Distinct from other religious traditions, Hindu marriage is regarded not just as a contractual :union: but as a sacred rite, serving both earthly and spiritual objectives. Investigating how self-compassion affects well-being in Hindu couples who are married could unveil fresh insights into how self-compassion interacts with emotional dynamics and the achievement of goals [23, 24]. Additionally, the impact of social class on the nexus between self-compassion and well-being in these couples is noteworthy. Those from lower social classes, typically marked by reduced financial means (lesser income, lower educational attainment) and a diminished social standing, often encounter tougher living conditions than individuals from higher social strata [25]. This disparity in resources and social status is thought to significantly influence the emotional experiences of those in the lower social class.
Research indicates that individuals from lower socioeconomic backgrounds exhibit heightened emotional responses to uncertain and negative social scenarios [26, 27]. Social class, as a hierarchical construct, is determined by an individual’s accumulation of material resources [28]. Those belonging to the lower socioeconomic stratum often find themselves in challenging environments characterized by increased threats and barriers, such as less secure neighborhoods and underfunded educational systems. These individuals typically face difficulties in leveraging their limited resources to surmount these challenges [27]. Consequently, there is a pressing need for further studies to explore this subject in greater depth, particularly focusing on how demographic and personal factors influence the interplay between self-compassion and well-being among married couples [12].
Given the importance of self-compassion in promoting resilience, adaptive coping strategies, and emotional well-being, this study aimed to examine its influence on well-being among married Hindu couples. While previous research has largely focused on individual perspectives, there is little research on the effects of self-compassion on the well-being of couples [9, 29]. This gap is particularly noteworthy given the sacred, multidimensional nature of Hindu marriage, which extends beyond contractual bonds. Moreover, the role of demographic factors (education, domicile, employment status, length of marriage, number of children, nature of family, family size and socioeconomic status) in this relationship remains understudied, particularly in light of potential disparities in resources and emotional experiences. This research aimed to address these gaps and advance our understanding of the role of self-compassion in improving the well-being of married Hindu couples across diverse demographics. Research findings on self-compassion and marital well-being among Hindu couples will enrich existing models of self-compassion by examining its impact in a specific cultural context and offering insights into its role in married life. Practitioners can use these findings to develop culturally sensitive interventions aimed at enhancing self-compassion in couples, improving relationship satisfaction and addressing the unique challenges faced by Hindu couples during rehabilitation and therapy. Policymakers can leverage this research to create supportive community programs that promote self-compassion, mental health, and well-being, particularly for lower social classes that face greater challenges and disparities.
Against this context, the current research aimed to investigate the relationship between self-compassion and well-being in married Hindu couples, assessing both the nature and extent of this association. Furthermore, the study sought to determine the proportion of variance in different well-being metrics that could be attributed to self-compassion within this demographic. Drawing from existing literature, our hypotheses posit that the positive aspects of self-compassion are much more likely to be positively correlated with and significantly contribute to, the variance observed in various well-being indices. Conversely, the negative aspects of self-compassion are expected to either have low positive or negative correlations, resulting in limited or adverse effects on the variability observed in well-being measurements.
Methods
Study design
A correlational design was employed for data collection, processing, and analysis. This design helps identify patterns and relationships and predict behaviors and outcomes.
Sample
Participants were chosen using the snowball sampling method, in which existing participants provided referrals to other potential participants for the study. This sampling method helped in finding and choosing the participants with ease. The study chose 300 Hindu couples (age range=26-50 years, Mean±SD, 38.42±7.89) in 2022. The participants were chosen from Sagar City and adjoining areas, in Madhya Pradesh, India. The majority of these participants were from lower-middle-class Hindu families, residing in both rural and urban areas. Based on Cohen’s (1988) guidelines for correlational design, a medium effect size of 0.30 was selected with a significance level of 0.05 and a power of 0.80 [30, 31]. The estimated sample size required to detect this effect size was 67 cases, calculated using G*Power software, version 3 [32]. We selected a sample size of 300 participants, which was sufficient to achieve the study objectives.
Inclusion and exclusion criteria
The research included participants who had a minimum of five years of experience in marriage and exhibited no evident physical or mental health issues. Participation was limited to Hindu couples who were 26 years old or older. The inclusion criterion was passing at least five years of married life to ensure sufficient experience with the basic issues and dynamics of married life. Couples who belonged to other religious communities, had health problems, were married for less than five years, or did not fall within the required age range were excluded from the study. The demographic details are given in Table 1.
Study measures
The following measures were used to collect the data:
Self-compassion scale
The couples’ self-compassion was assessed using the self-compassion scale [4]. This instrument evaluates the thoughts, feelings, and behaviors integral to the various elements of self-compassion. It encompasses a total of 26 items that gauge the frequency with which individuals experience feelings of inadequacy or self-criticism through aspects such as self-kindness, self-judgment, common humanity, isolation, mindfulness and over-identification. The scale is divided into six subcategories: Self-kindness (five items), self-judgment (five items), common humanity (four items), isolation (four items), mindfulness (four items) and over-identification (four items), each rated on a five-point scale ranging from ‘almost never’ to ‘almost always’. The items on the self-kindness, common humanity, and mindfulness subscales are assigned 1, 2, 3, 4 and 5 points for responses ranging from almost never to almost always. Reverse scoring was applied to responses on the self-judgment, isolation, and over-identification subscales. A total score from these subscales indicates participants’ overall self-compassion; the higher the scores on the measure, the greater the self-compassion. The minimum and maximum range of scores on the scale is from 26 to 130. The Cronbach’s α for the scale in the present sample was 0.571. The reliability and validity of the scale have been well-documented in previous research [3, 7]. Studies with diverse participant groups have consistently reported the scale’s internal reliability as satisfactory [7, 20].
Mental health continuum-short form (MHC-SF)
The MHC-SF [33] was utilized to assess the well-being of couples. This scale is rooted in research on emotional well-being [34], including both hedonic (subjective or emotional) and psychological well-being [35], as well as social well-being [36]. It comprises 14 items, asking participants to reflect on their experiences over the previous month and respond using a six-point scale ranging from ‘never’ to ‘every day, scored from one to six.’ The minimum and maximum scores on the scale are from 14 to 84. The amalgamation of psychological and social well-being scores provides a measure of eudaimonic well-being. The overall score obtained from this scale is indicative of human flourishing. The scale’s internal consistency reliability in the present sample was notably high, exceeding 0.80 [33].
Socioeconomic status scale
The socioeconomic status scale [37] served as the instrument for gauging the economic and social standing of the couples involved in the study. This particular scale is comprised of 22 items, each offering a selection of multiple-choice responses. Based on their scores, individuals and families were categorized into one of six distinct groups: Upper high (>76), high (61-75), upper middle (46-60), lower middle (31-45), poor (16-30), and very poor or below poverty line (<15). The scoring thresholds set by this scale–below 45, between 45 and 60 and above 61–correspond to low, medium and high socioeconomic statuses, respectively [37]. This scale has been frequently utilized by researchers in the field of behavioral science [9, 29].
Data analysis plan
The acquired raw values were organized based on the study’s design. Once the data collection process concluded, they underwent analysis using SPSS software, version 26. The analysis encompassed the computation of Mean±SD, Pearson product moment correlation coefficients, and stepwise regression analyses to analyze the relationships between variables and test the study hypotheses. The significance level was ≤0.05.
Results
The findings are presented in three sections. The first section is devoted to the demographic attributes of the participants. The second section to the analysis of correlation coefficients, while the third section is devoted to the discussion of hierarchical regression analyses.
Demographic attributes
There were 178 non-graduates (29.70%) and 422 graduates (70.30%). The number of male and female participants was equal, namely 300. Their age ranged from 26 to 50 years and belonged to both rural (103) and urban (497) areas. Forty percent (360) were employed while 240 were unemployed (40%). Their married life ranged from 6 to 29 years and they had 0 to 6 children. The majority of them belonged to joint families (63.80%) and the remaining 36.20% belonged to nuclear families. On average, each couple lived in a family with 2 to 31 members. Participants varied in their socioeconomic status. They belonged to upper-high (>76) (n=89, percent=15.10), high (61-67) (n=132, percent=21.90), upper-middle (46-60) (n=283, percent=47.20), lower-middle (31-45) (n=81, percent=13.6) and poor (16-30) (n=15, percent=2.50) levels of socioeconomic status. There were 178 non-graduates (29.70%) and 422 graduates (70.30%). The number of male and female participants was equal, with each group comprising 300 individuals. Their ages ranged from 26 to 50 years, and they belonged to both rural (103) and urban (497) areas. Forty percent (360) were employed, while 240 were unemployed (40%). Their married lives ranged from 6 to 29 years and they had between 0 and 6 children. The majority of participants belonged to joint families (63.80%), while the remaining 36.20% belonged to nuclear families. On average, each couple lived in a family with 2 to 31 members. Participants varied in their socioeconomic status, belonging to upper-high (>76) (n=89, percent=15.10), high (61-75) (n=132, percent=21.90), upper-middle (46-60) (n=283, percent=47.20), lower-middle (31-45) (n=81, percent=13.6) and poor (16-30) (n=15, percent=2.50) levels of socioeconomic status.
Correlation analysis
Table 2 illustrates significant positive correlations between age and hedonic well-being (r=0.226, P>0.01), psychological well-being (r=0.227, P>0.01), eudaimonic well-being (r=0.158, P>0.01) and human flourishing (r=0.188, P>0.01). The number of children had a positive correlation with hedonic well-being (r=0.110, P>0.01). The number of family members had negative correlations with social well-being (r=-0.123, P>0.01), psychological well-being (r=-0.103, P>0.01), eudaimonic well-being (r=-0.130, P>0.01) and human flourishing (r=-0.101, P>0.01). Self-kindness showed positive correlations with hedonic well-being (r=0.293, P>0.01), social well-being (r=0.184, P>0.01), psychological well-being (r=0.338, P>0.01), eudaimonic well-being (r=0.304, P>0.01) and human flourishing (r=0.332, P>0.01). Similarly, common humanity exhibited positive significant correlations with hedonic well-being (r=0.276, P>0.01), social well-being (r=0.129, P>0.01), psychological well-being (r=0.306, P>0.01), eudaimonic well-being (r=0.254, P>0.01) and human flourishing (r=0.284, P>0.01). Mindfulness indicated positive correlations with hedonic well-being (r=0.225, P>0.01), social well-being (r=0.107, P>0.01), psychological well-being (r=0.300, P>0.01), eudaimonic well-being (r=0.237, P>0.01) and human flourishing (r=0.250, P>0.01). Thus, positive aspects of self-compassion had positive correlations with different components of well-being. Conversely, self-judgment showed negative correlations with hedonic well-being (r=-0.084, P>0.05), social well-being (r=-0.111, P>0.01), eudaimonic well-being (r=-0.100, P>0.05), and human flourishing (r=-0.099, P>0.05). Isolation and over-identification exhibited non-significant, very weak negative or positive correlations with the well-being indices (Table 2).
Hierarchical regression analysis
Analysis of the standard residuals revealed no outliers in the data (min=-1.9, max=1.7). The data also met the independent error requirement, as indicated by a Durbin-Watson value of 1.63. Further tests for collinearity showed that multicollinearity was not a problem (tolerance=0.94). Furthermore, the scatter plot of standardized predicted values confirmed that the data met the assumptions of homogeneity of variance and linearity.
In the initial stage of the analysis, a range of demographic factors (including education level, gender, age, place of residence, occupation, marriage duration, number of children, family type, family size and socioeconomic status) were considered, as detailed in step 1. This was followed by the incorporation of variables, such as self-kindness, self-judgment, feelings of common humanity versus isolation, mindfulness, and the tendency for over-identification in step 2 (Table 3). The findings revealed that these demographic factors significantly influenced the outcomes, explaining 9.8% of the variance in hedonic well-being (R2=0.098, F(10, 589)=6.37, P<0.001). In addition, these demographic factors collectively contributed 7.5% to social well-being (R2=0.075, F(10, 589)=4.75, P<0.001), 14.6% to psychological well-being (R2=0.146, F(10, 589)=10.11, P<0.001), 12.4% to eudaimonic well-being (R2=0.124, F(10, 589)=8.35, P<0.001), and 12.6% to human flourishing (R2=0.126, F(10, 589)=8.46, P<0.001), as demonstrated in model 1 for each facet of human well-being.
The findings revealed that factors, such as self-kindness, self-judgment, a sense of shared humanity, feelings of isolation, mindfulness and tendencies toward over-identification contributed variably to different aspects of well-being. Specifically, these factors were responsible for 20.6% of hedonic well-being (R2=0.206, F(3, 586) =13.34, P<0.001), 11.5% of social well-being (R2=0.115, F(3, 586)=4.44, P<0.001), 28.0% of psychological well-being (R2=0.280, F(3, 586)=17.99, P<0.001), 22.6% of eudaimonic well-being (R2=0.226, F(3, 586)=12.83, P<0.001), and 24.8% of flourishing (R2=0.248, F(3, 586)=15.88, P<0.001), as indicated in Table 3. Additionally, integrating these factors at step 2 in the model for hedonic well-being led to a significant alteration, with a 0.109 unit (β) increase in hedonic well-being.
In the realm of social well-being, integrating factors, such as self-kindness, self-judgment, a sense of shared humanity, feelings of isolation, mindfulness, and tendencies toward over-identification at the second level resulted in a noteworthy enhancement of 0.040 units (β). Similarly, incorporating these same factors in the second phase led to a substantial improvement of 0.133 units (β) in psychological well-being. Additionally, the inclusion of these components in the second step was responsible for a significant increase of 0.102 units (β) in eudaimonic well-being. Moreover, this integration at the same stage also accounted for an important enhancement of 0.123 units (β) in the measure of flourishing, as detailed in Table 3.
Discussion
This study investigated the relationship between self-compassion and well-being in married Hindu couples. It examined how different aspects of well-being were influenced by self-compassion and other demographics. Positive aspects of self-compassion, like self-kindness, common humanity, and mindfulness were found to correlate positively with well-being. In contrast, negative aspects, such as self-judgment, isolation and over-identification showed weaker positive or negative correlations with well-being. Additionally, biographical factors, such as education, age, domicile, occupation, length of marriage, and family size also played a significant role in shaping well-being in various ways. Positive variability in various dimensions of well-being was observed with self-kindness and common humanity, while self-judgment led to negative variability.
Positive aspects of self-compassion (self-kindness, common humanity, and mindfulness) can boost the well-being of married couples by nurturing a supportive and understanding relationship. By approaching their own and their partner’s imperfections with kindness and acceptance, individuals foster greater positive mental health. This mindset enables empathetic and patient responses during conflicts and facilitates open and effective communication that strengthens emotional bonds and mutual support. Positive aspects of self-compassion also reduce stress and prevent resentment, promote a harmonious and loving relationship, and ultimately improve emotional intimacy and marital longevity [38-40]. The study hypothesized that positive aspects of self-compassion (self-kindness, common humanity, and mindfulness) would be positively correlated with various well-being indices, while negative aspects would yield poorer positive or negative correlations. The results largely support these hypotheses, with many demographic findings proving to be novel because these demographic variables have not been empirically examined previously.
Research has shown that education, gender, age, domicile and employment status significantly influence couples’ well-being. Higher education was associated with greater understanding, knowledge, career prospects, attributions, coping skills, and resilience to life events [38, 39], which likely boosted well-being. Gender disparities in access to resources and opportunities continue to exist in India [40].
Gender differences in well-being, which often favor men, may result from disparities in access to socio-cultural norms and socialization processes, as well as positive personal traits, such as self-forgiveness, self-compassion, and self-esteem [7, 10, 41, 42]. Over time, spouses adapt to each other’s life experiences during marriage, potentially leading to improved well-being over a longer marriage duration [40, 43]. Factors, such as family type (nuclear vs. joint family), family size, and socioeconomic status also play roles in well-being by introducing various experiences and opportunities. These factors highlight the influence of demographic factors on the well-being of married Hindu couples.
Research suggests that women typically demonstrate higher self-compassion than men, which leads to better well-being in marital relationships [7, 8]. Self-compassion involves treating oneself kindly, acknowledging one’s humanity and maintaining a positive perspective during challenging times. Social and cultural influences may account for this difference, as women often prioritize relationships and emotional expression, fostering self-awareness and empathy. These qualities help women deal with marital problems with patience and understanding, resulting in more positive relationship dynamics. By embracing self-compassion, women experience reduced stress and anxiety, thereby enhancing overall well-being.
Research suggests that couples’ well-being is affected by their self-compassionate characteristics. Positive aspects of self-compassion, such as self-kindness, common humanity, and mindfulness, have a positive influence on couples’ well-being. In contrast, negative aspects, like harsh self-judgment, isolation and over-identification with personal flaws harm well-being. The study highlights that beneficial components of self-compassion include self-kindness, common humanity, mindfulness, self-acceptance, patience with negative traits, and acknowledgment of shared challenges. These qualities of self-compassion contribute to emotional stability, clear perception, analytical reflection on failures, and openness to challenging experiences [4, 5, 7].
Conversely, negative aspects of self-compassion involve self-judgment, isolation, and over-identification, including harsh self-judgment, difficulty accepting mistakes, self-deprecation, and loneliness. These behaviors can lead to unfavorable comparisons with others, heightened feelings of solitude during personal failures, and an overemphasis on certain events [7, 8]. The nurturing aspects of self-compassion contribute significantly to its predictive power on various indicators of well-being. Research suggests that demographic attributes and personal resources play a crucial role in the well-being of couples. In Hindu marriages, secular and spiritual life goals are interlinked, and the growing influence of postmodern lifestyles emphasizes the importance of socioeconomic factors in couple dynamics [29].
A meta-analysis showed a close link between self-compassion and well-being [12, 24]. The review found that women had higher self-compassion levels and greater well-being than men, and the association between self-compassion and psychological well-being was particularly stronger in women. Factors, such as domicile, age, education, and family dynamics have been found to impact the relationship between self-compassion and positive mental health [12, 24], which is consistent with the findings of the current study.
In essence, this study delves into the connection between self-compassion and well-being in married Hindu couples while incorporating demographic factors influencing well-being. The research is consistent with previous studies and shows that self-compassion has a positive impact on well-being through attributes, like self-kindness, mindfulness, and common humanity [3, 5, 6]. The study advances existing research by illustrating how factors, such as education, age, occupation, and marriage length interact with self-compassion and affect well-being. Past research has pointed to gender differences in self-compassion and well-being, often in favor of women [6-8], which this study supports by exploring the cultural and socioeconomic aspects of Hindu marriages. While confirming the adverse effects of negative self-compassion traits, like self-judgment and isolation on well-being, the study also highlights the demographic intricacies of the Hindu marital context and advances understanding of the role of self-compassion in marital well-being in the Indian cultural context.
Conclusion
The findings of the research affirm the significance of self-compassion in influencing the overall well-being of Hindu couples in marital relationships. Furthermore, the study highlights the substantial impact of demographic variables, including education, gender, age, geographical location, occupation, length of marriage, family size and socioeconomic status, on the well-being of the individuals involved.
Implications, future directions and limitations
The study’s findings are significant for researchers, policymakers, and practitioners in the field. Practical applications include offering self-compassion workshops to help individuals build self-compassion. Policies that give men and women equal access to resources can balance well-being across genders. Open, honest discussions between partners can enhance mutual understanding and improve marital adjustment. Encouraging couples to practice self-acceptance and patience can create a supportive environment and reduce self-criticism. Offering training and resources can help improve couples’ resilience and coping strategies to overcome challenges. Helping couples make informed family decisions can improve their well-being. Incorporating mindfulness exercises and promoting social engagement can improve emotional stability and strengthen social support networks. Professional advice can help you overcome difficulties and strengthen relationships, especially in challenging times. Practitioners can use these insights to develop interventions that target self-compassion and demographic factors to improve marital well-being and mental health. The study can also guide policies to promote educational and socioeconomic equality to improve well-being. The small sample size, the inclusion of only Hindu married couples, and a limited number of variables are some limitations of the study. Future studies could address these limitations by using larger and more diverse samples, incorporating qualitative methods, and examining additional variables related to marital well-being. The current findings can be used to deepen our understanding of the complex factors that influence marital well-being.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by Ethics Committee of Doctor Harisingh Gour Vishwavidyalaya (Code: DHSGV/IEC/2021/10). Written consent was taken from each participant, and their confidentiality and privacy were maintained by anonymizing their details.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the support and contributions of the participants who generously devoted their valuable time to the study.
References
- Neff KD. Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity. 2003; 2(2):85-101. [DOI:10.1080/15298860309032]
- Semenchuk BN, Kullman SM, Neilson CJ, Ceccarelli L, Boreskie K, Kehler DS, et al. Self-compassion, health behaviors, self-regulation, and affective states among individuals at risk of or diagnosed with a chronic disease: A scoping review. Mindfulness. 2022; 13(5):1085-111. [DOI:10.1007/s12671-021-01821-3]
- Neff KD. Self-Compassion: Theory, method, research, and intervention. Annual Review of Psychology. 2023; 74(1):193-218. [DOI:10.1146/annurev-psych-032420-031047]
- Neff KD. The development and validation of a scale to measure self-compassion. Self and Identity. 2003; 2(3):223-50. [DOI:10.1080/15298860309027]
- Tiwari GK, Pandey R, Rai PK, Pandey R, Verma Y, Parihar P, et al. Self-compassion as an intrapersonal resource of perceived positive mental health outcomes: A thematic analysis. Mental Health, Religion & Culture. 2020;23(7):550-69. [DOI:10.1080/13674676.2020.1774524]
- Verma Y, Tiwari GK, Pandey A, Pandey R. Triguna (three qualities) personality model and two-factor conceptualization of self-compassion: A new insight to understand achievement goal orientations. Current Issues in Personality Psychology. 2020;8(3):211-28. [DOI:10.5114/cipp.2020.100096]
- Pandey R, Tiwari GK, Parihar P, Rai PK. Positive, not negative, self-compassion mediates the relationship between self-esteem and well-being. Psychology and Psychotherapy. 2021; 94(1):1-15. [DOI:10.1111/papt.12259]
- Pandey R, Tiwari GK, Pandey R, Mandal SP, Mudgal S, Parihar P, et al. The relationship between self-esteem and self-forgiveness: Understanding the mediating role of positive and negative self-compassion. Psychological Thought. 2023; 16(2):230-60. [DOI:10.37708/psyct.v16i2.571]
- Parihar P, Tiwari GK, Rai PK. Understanding the relationship between self-compassion and interdependent happiness of the married hindu couples. Polish Psychological Bulletin. 2020; 51(4):260-72. [DOI:10.24425/ppb.2020.135458]
- Pandey R, Tiwari GK, Parihar P, Rai PK. The relationship between self-forgiveness and human flourishing: Inferring the underlying psychological mechanisms. Polish Psychological Bulletin. 2020; 51(1):23-36. [DOI:10.24425/ppb.2020.132649]
- Dreisoerner A, Junker NM, Van Dick R. The relationship among the components of self-compassion: A pilot study using a compassionate writing intervention to enhance self-kindness, common humanity, and mindfulness. Journal of Happiness Studies. 2021; 22(1):21-47. [DOI:10.1007/s10902-019-00217-4]
- Zessin U, Dickhäuser O, Garbade S. The relationship between self-compassion and well-being: A meta-analysis. Applied Psychology: Health and Well-Being. 2015; 7(3):340-64. [DOI:10.1111/aphw.12051]
- Cruz S, Sousa M, Peixoto M, Meireles A, Marques S, Faria S, et al. The interplay between emotional well-being, self-compassion, and basic psychological needs in adolescents. International Journal of Adolescence and Youth. 2024; 29(1):2318340. [DOI:10.1080/02673843.2024.2318340]
- Buecker S, Luhmann M, Haehner P, Bühler JL, Dapp LC, Luciano EC, et al. The development of subjective well-being across the life span: A meta-analytic review of longitudinal studies. Psychological Bulletin. 2023; 149(7-8):418-46. [DOI:10.1037/bul0000401]
- Körner R, Tandler N, Petersen L, Schütz A. Is caring for oneself relevant to happy relationship functioning? Exploring associations between self-compassion and romantic relationship satisfaction in actors and partners. Personal Relationships. 2024; 31(2):333-57. [DOI:10.1111/pere.12535]
- Birni G, Eryilmaz A. Enhancing well-being of the married: Investigating marital satisfaction, self-compassion and happiness increasing strategies. Turkish Psychological Counseling and Guidance Journal. 2022; 12(67):650-69. [DOI:10.17066/tpdrd.12061408]
- Gilbert P. Creating a compassionate world: Addressing the conflicts between sharing and caring versus controlling and holding evolved strategies. Frontiers in Psychology. 2021; 11:582090. [DOI:10.3389/fpsyg.2020.582090]
- Muris P, Fernández-Martínez I, Otgaar H. On the edge of psychopathology: Strong relations between reversed self-compassion and symptoms of anxiety and depression in young people. Clinical Child and Family Psychology Review. 2024; 27:407-23. [DOI:10.1007/s10567-024-00471-w]
- Förster K, Kanske P. Upregulating positive affect through compassion: Psychological and physiological evidence. International Journal of Psychophysiology. 2022; 176:100-7. [DOI:10.1016/j.ijpsycho.2022.03.009]
- García-Campayo J, Barceló-Soler A, Martínez-Rubio D, Navarrete J, Pérez-Aranda A, Feliu-Soler A, et al. Exploring the relationship between self-compassion and compassion for others: The role of psychological distress and wellbeing. Assessment. 2023; 31(5):10731911231203966. [DOI:10.1177/10731911231203966]
- Cha JE, Serlachius AS, Cavadino A, Kirby JN, Consedine NS. Self-compassion and compassion for others: A multiple mediation study of personal values. Mindfulness. 2023; 14(10):2417-29. [DOI:10.1007/s12671-023-02202-8]
- Muris P, van den Broek M, Otgaar H, Oudenhoven I, Lennartz J. Good and bad sides of self-compassion: A face validity check of the self-compassion scale and an investigation of its relations to coping and emotional symptoms in non-clinical adolescents. Journal of Child and Family Studies. 2018; 27(8):2411-21. [DOI:10.1007/s10826-018-1099-z]
- Mongrain M. Compassion, happiness, and self-esteem. In: Maggino F, editor. Encyclopedia of quality of life and well-being research. Berlin: Springer International Publishing; 2022. [DOI:10.1007/978-3-319-69909-7_3896-2]
- Muris P, Otgaar H. Self-esteem and self-compassion: a narrative review and meta-analysis on their links to psychological problems and well-being. Psychology Research and Behavior Management. 2023; 16:2961-75. [DOI:10.2147/PRBM.S402455]
- Wilson S, Worsley A. Unequal childhoods: A case study application of Lareau’s ‘accomplishment of natural growth’in British working-class and poor families. British Educational Research Journal. 2021; 47(3):770-86. [DOI:10.1002/berj.3707]
- Navarro-Carrillo G, Alonso-Ferres M, Moya M, Valor-Segura I. Socioeconomic status and psychological well-being: Revisiting the role of subjective socioeconomic status. Frontiers in Psychology. 2020; 11:1303. [DOI:10.3389/fpsyg.2020.01303]
- Zhang Y, Su D, Chen Y, Tan M, Chen X. Effect of socioeconomic status on the physical and mental health of the elderly: The mediating effect of social participation. BMC Public Health. 2022;22(1):605. [DOI:10.1186/s12889-022-13062-7]
- Redhead D, Power EA. Social hierarchies and social networks in humans. Philosophical Transactions of the Royal Society B. 2022; 377(1845):20200440. [DOI:10.1098/rstb.2020.0440]
- Parihar P, Tiwari GK, Rai PK. Understanding the role of forgiveness in shaping the flourishing of Hindu married couples. Jurnal of Education and Buddhist Studies. 2023; 3(1):46-60. [DOI:10.53417/sjebs.v3i1.99]
- Cohen J. Statistical power analysis for the behavioral sciences. New York: Routledge; 1988. [DOI:10.4324/9780203771587]
- Cohen J. Statistical power analysis. Current Directions in Psychological Science. 1992; 1(3):98-101. [DOI:10.1111/1467-8721.ep10768783]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods. 2007; 39(2):175-91. [DOI:10.3758/BF03193146]
- Keyes CLM. Mental illness and/or mental health? investigating axioms of the complete state model of health. Journal of Consulting and Clinical Psychology. 2005; 73(3):539-48. [DOI:10.1037/0022-006X.73.3.539]
- Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: Three decades of progress. Psychological Bulletin. 1999; 125(2):276-302. [DOI:10.1037/0033-2909.125.2.276]
- Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology. 1989; 57(6):1069-81. [DOI:10.1037/0022-3514.57.6.1069]
- Keyes CLM. Social well-being. Social Psychology Quarterly. 1998; 61(2):121. [DOI:10.2307/2787065]
- Aggarwal OP, Bhasin SK, Sharma AK, Chhabra P, Aggarwal K, Rajoura OP. A new instrument (scale) for measuring the socioeconomic status of a family: Preliminary study. Indian Journal of Community Medicine. 2005; 30(4):111. [Link]
- Darling-Hammond L, Flook L, Cook-Harvey C, Barron B, Osher D. Implications for educational practice of the science of learning and development. Applied Developmental Science. 2019; 24(2):97-140. [DOI:10.1080/10888691.2018.1537791]
- Black M, Barnes A, Strong M, Brook A, Ray A, Holden B, et al. Relationships between child development at school entry and adolescent health-A participatory systematic review. International Journal of Environmental Research and Public Health. 2021; 18(21):11613. [DOI:10.3390/ijerph182111613]
- Diener E, Gohm CL, Suh E, Oishi S. Similarity of the relations between marital status and subjective well-being across cultures. Journal of Cross-Cultural Psychology. 2000; 31(4):419-36. [DOI:10.1177/0022022100031004001]
- Tiwari GK, Pandey R, Parihar P, Rai PK. Self-forgiveness and human flourishing: Understanding the mediating role of self-esteem. Mental Health, Religion & Culture. 2023; 26(5):418-30. [DOI:10.1080/13674676.2023.2238642]
- Tiwari GK, Pandey R, Rai PK, Shukla M, Jain R, Budhwani P, et al. Understanding the nature and consequences of transgressions and forgiveness in the workplace in India. Interpersona. 2023; 17(1):45-68. [DOI:10.5964/ijpr.4625]
- Perkins JM, Lee HY, James KS, Oh J, Krishna A, Heo J, et al. Marital status, widowhood duration, gender and health outcomes: A cross-sectional study among older adults in India. BMC Public Health. 2016; 16(1):1032. [DOI:10.1186/s12889-016-3682-9]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2024/03/8 | Accepted: 2024/05/14 | Published: 2024/10/28
Received: 2024/03/8 | Accepted: 2024/05/14 | Published: 2024/10/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
