

Volume 14, Issue 5 (Sep & Oct 2024)
J Research Health 2024, 14(5): 417-426 |
Back to browse issues page



Ethics code: Ref. No. 079-84
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Pradhan N, Karki R, Kaphle M. Dengue Fever Knowledge and Attitudes in Hetauda, Bagmati Province, Nepal: A Cross-sectional Study. J Research Health 2024; 14 (5) :417-426
URL: http://jrh.gmu.ac.ir/article-1-2551-en.html
URL: http://jrh.gmu.ac.ir/article-1-2551-en.html



1- Department of Public Health, Yeti Health Science Academy, Purbanchal University, Kathmandu, Nepal.
2- Central Department of Public Health, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal. ,karkirajesh2022@gmail.com
3- Department of Public Health, Peoples Dental College and Hospital, Tribhuvan University, Kathmandu, Nepal.
2- Central Department of Public Health, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal. ,
3- Department of Public Health, Peoples Dental College and Hospital, Tribhuvan University, Kathmandu, Nepal.
Full-Text [PDF 636 kb]
(556 Downloads)
| Abstract (HTML) (3341 Views)
Full-Text: (1164 Views)
Introduction
Dengue fever (DF) remains a significant global public health concern and is recognized as a key arthropod-borne disease agent [1]. It is an infectious illness caused by any of the four dengue virus serotypes: DENVs 1-4, which are primarily transmitted by mosquitoes, particularly the female Aedes mosquito [2]. The World Health Organization (WHO) reports a substantial increase in global dengue cases, impacting about half the world’s population, with 100-400 million infections annually. Many cases, often mild or asymptomatic, go unreported or are misdiagnosed as other febrile illnesses [3]. DF is associated with substantial morbidity, mortality, and economic burden, particularly in developing countries [4].
Nepal is prone to outbreaks of numerous infectious diseases [5], with the DF emerging as a significant health concern. Its prevalence is observed year-round across all 77 districts [6]. The first recorded instance of dengue in Nepal occurred in 2005, involving a foreigner in Chitwan district. Since then, dengue cases have progressively risen in Nepal, predominantly in the tropical lowlands and subtropical hilly regions, including Kathmandu. Between 2006 and 2022, Nepal experienced several dengue outbreaks [6]. According to the Epidemiology and Disease Control Division (EDCD) of Nepal in 2023, there were 51,243 reported dengue cases from all 77 districts, with 20 confirmed deaths. Bagmati Province reported 7,704 cases, constituting 15.0% of the national burden, while Makwanpur district reported 143 cases [7]. In 2022, Nepal experienced its largest-ever dengue outbreak, with the majority of cases reported in the Bagmati Province. The Kathmandu district was the most severely affected, with 14,376 cases, and the Makwanpur district, with 5,837 cases, ranked fourth after Lalitpur and Bhaktapur districts [8].
To effectively control and prevent DF, a comprehensive approach is needed. This includes combining conventional methods, like larvicides and insecticides, with community-based strategies. Integrated vector management (IVM) optimizes resource use and promotes sustainable interventions. Community engagement, with local leaders mobilizing efforts and sharing information, is crucial. Tailoring strategies to local needs and fostering community ownership are essential for sustained behavior change and improved prevention. Active community participation and cross-sector collaboration are key to effectively combatting DF [9]. In addition to factors, such as low socioeconomic status, inadequate sanitation, and substandard public health facilities, a lack of awareness among the population fosters conditions conducive to the emergence of this disease and significantly contributes to the socioeconomic burden in Nepal [5]. While numerous studies have focused on dengue-infected individuals, there is limited research on the knowledge and attitudes of the general population regarding dengue [10]. To design effective public health interventions for dengue in various altitudinal regions of Nepal, it is crucial to understand the community’s knowledge, attitudes, and practices (KAP) related to the dengue virus and its vectors [11]. Therefore, this study aimed to measure knowledge and attitudes among household members toward DF. Although this study focused on Bagmati Province, Nepal, its findings on community KAP regarding DF can inform interventions beyond this region. Understanding KAP can benefit similar areas in Nepal with comparable demographics and socioeconomic conditions and may hold value for other dengue-endemic countries facing similar contexts.
Locally, the research offers valuable data for policymakers in Bagmati Province, informing culturally appropriate prevention campaigns, resource allocation, and improved public health strategies. Publishing in an international journal allows for broader knowledge dissemination, contributing to a global understanding of KAP and informing more effective prevention strategies across dengue-endemic regions.
Methods
A cross-sectional study was carried out in Hetauda Sub-metropolitan City, located in the Makwanpur district of the Bagmati Province in central Nepal, serving as the capital of the Bagmati Province. Hetauda was selected for its status as a dengue-prone area. Specifically, out of the 19 wards in Hetauda, we focused on wards 4, 5, and 7. The selection of these wards was based on raw data obtained from the ward offices, revealing a higher prevalence of dengue during the study period. Additionally, resource constraints influenced the decision to limit the selection to these three wards.
The study population comprised household heads in the selected wards. In cases where the head of the household was unavailable or unable to participate, the next senior member was included. Participants were required to be 18 years or older. The sample size was determined using the Taro Yamane formula (Equation 1):
, where N represents the total number of households in the selected wards (N=30806), e is the margin of error (0.05), and a reliability level of 95%. Incorporating a 10% non-response rate yielded a final sample size of 434. A proportionate stratified random sampling method was used to select the required households. A list of households in the selected wards was prepared, and a cumulative total was calculated. The sampling interval (k) was then estimated as 30806/434=71. Starting from Ward No. 4, the first household was randomly selected, and every 71st interval thereafter was chosen until the required sample size was met. Local health workers and community members assisted in identifying households. Any respondents who did not give their consent to participate were excluded, and the next household in line was included.
A self-constructed structured questionnaire, developed based on two previous studies [12, 13], was utilized. The questionnaire covered socio-demographic information and included questions to assess knowledge and practices related to dengue. The questionnaire underwent validation by two public health experts, and its reliability was assessed using Cronbach’s α, yielding values of 0.91 for knowledge and 0.88 for attitude. Pretesting involved 10% of the sample population, which was excluded from the final analysis. Face-to-face interviews were conducted from March 1, 2023, to June 25, 2023. Data collection was carried out in the local Nepali language, with researchers directly involved in the process.
The questions covered the symptoms of DF, modes of transmission, and preventive measures. The knowledge level was dichotomized using an 80% cutoff point (score: ≤18 as low knowledge, score: ≥19 as good knowledge) [11]. The attitude was evaluated using a four-point Likert scale (strongly agree=four, agree=three, neutral=two, and disagree=one) with six positively phrased questions. Attitude scores ranged from 6 to 24, and a cutoff point of 50% was established (scores of 12 or less were considered a negative attitude, while scores higher than 12 were considered a positive attitude) [14].
Data were processed through editing, coding, and entry into SPSS software, version 26, and analysis was conducted as appropriate. Descriptive statistics, including frequency, percentage, and mean, were employed to analyze categorical variables. Similarly, the chi-square test was used to measure associations between socio-demographic variables and other selected variables with knowledge and attitude levels. Pearson correlation was also utilized to examine the relationship between knowledge and attitude. The significance level was set at a P<0.05.
Results
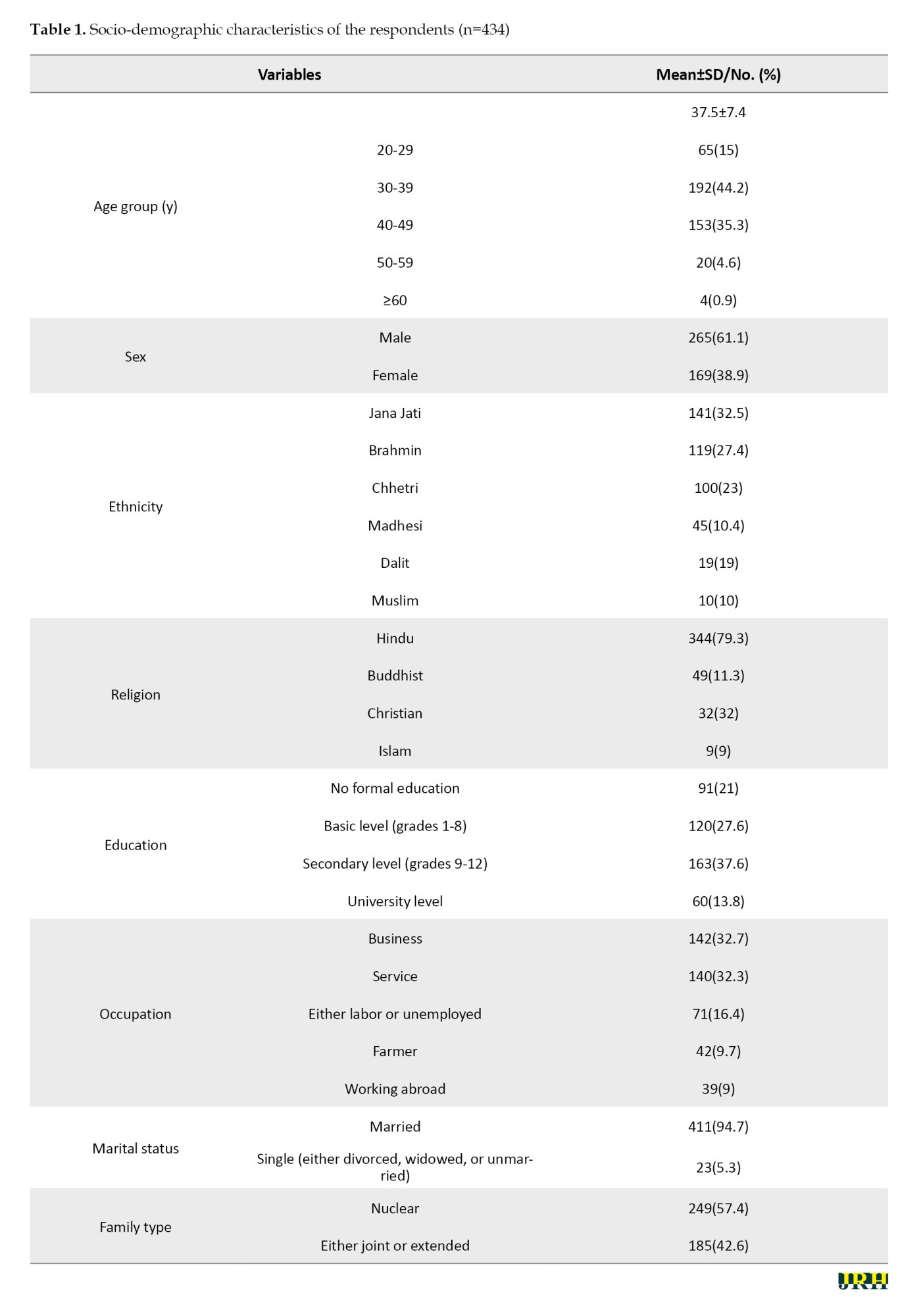
Out of 434 respondents, the majority (44.2%) belonged to the age group of 30-39, with a mean age of 37.50±7.40 years. Similarly, the majority were male (61.1%), belonged to the Jana Jati ethnicity (32.5%), practiced Hinduism (79.3%), had a secondary level education (37.6%), were employed in business (32.7%) or service (32.3%), were married (94.7%), and lived in a nuclear family setup (57.4%) (Table 1).
The majority (65.4%) mentioned health professionals as their source of information on DF, while 91.2% cited friends or neighbors. Similarly, regarding types of media, the primary source was television (85.3%), followed by the internet (81.3%) and radio (76.0%).
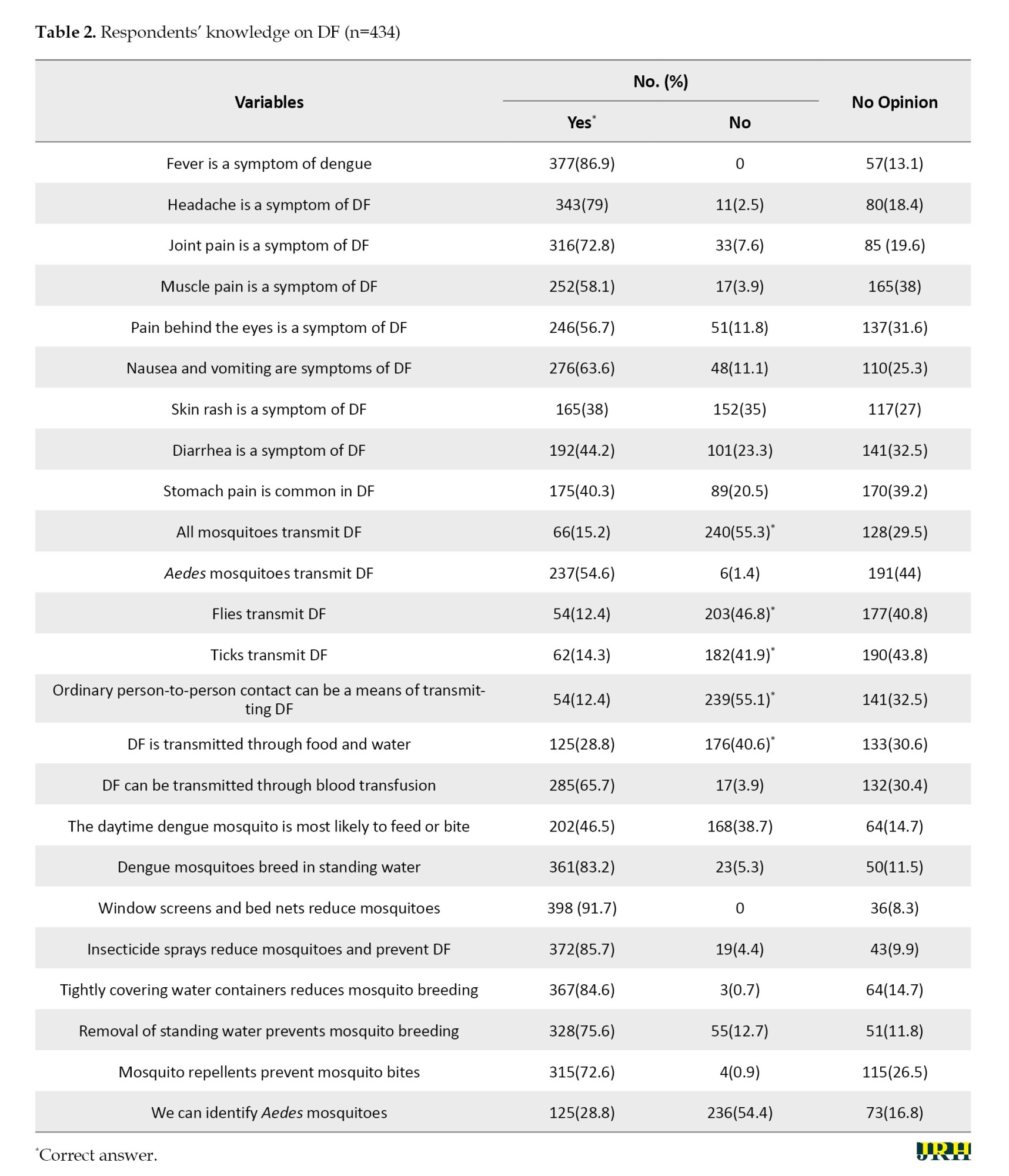
Out of the total of 24 questions assessing knowledge, 61.2% of respondents provided correct answers to all questions. Further analysis revealed that 60% of respondents correctly identified the signs and symptoms of DF, with the majority (86.9%) stating that fever is the major symptom. Regarding modes of transmission, 51.4% provided correct answers, and just over half (54.6%) correctly identified Aedes mosquitoes as the vectors of transmission. In terms of preventive measures, 77.1% provided correct answers, and among them, 91.7% believed that window screens and bed nets can prevent DF. However, only 28.8% mentioned the ability to identify Aedes mosquitoes (Table 2). Based on the total score obtained, the mean score was 14.7±6.45. When classified by level, the majority (77.2%) exhibited low knowledge, while only 22.8% demonstrated high knowledge.
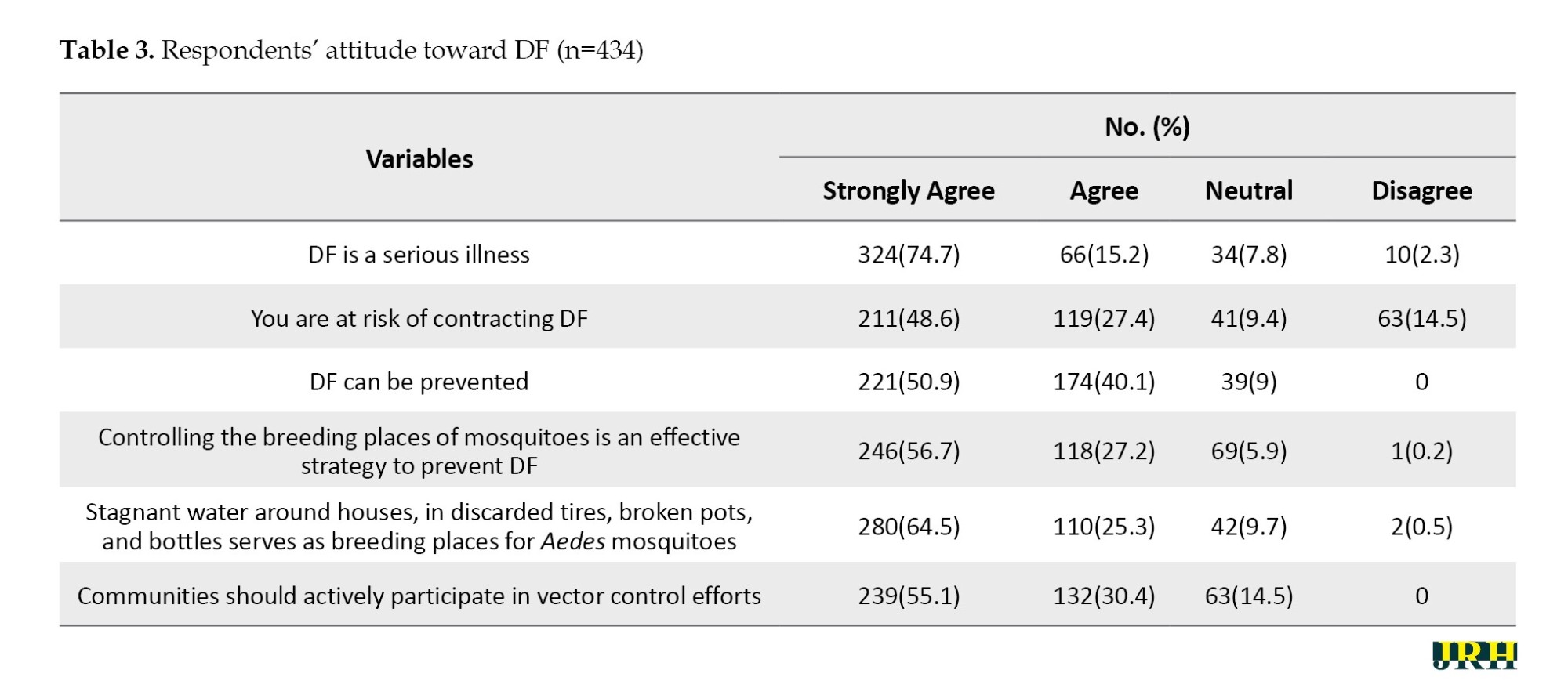
Similarly, a total of 58.4% strongly agreed with all six statements used to assess attitudes, with the majority (mean score: 20.5±3.71; 74.7%) strongly agree with the statement that fever is a symptom of dengue (Table 3). When categorized by level, the majority (93.8%) displayed a positive attitude, while only 6.2% held a negative attitude toward DF.
Pearson correlation analysis was conducted, and the results indicated a moderate positive significant correlation (r=0.429) between the knowledge score and attitude score toward DF (P<0.001).
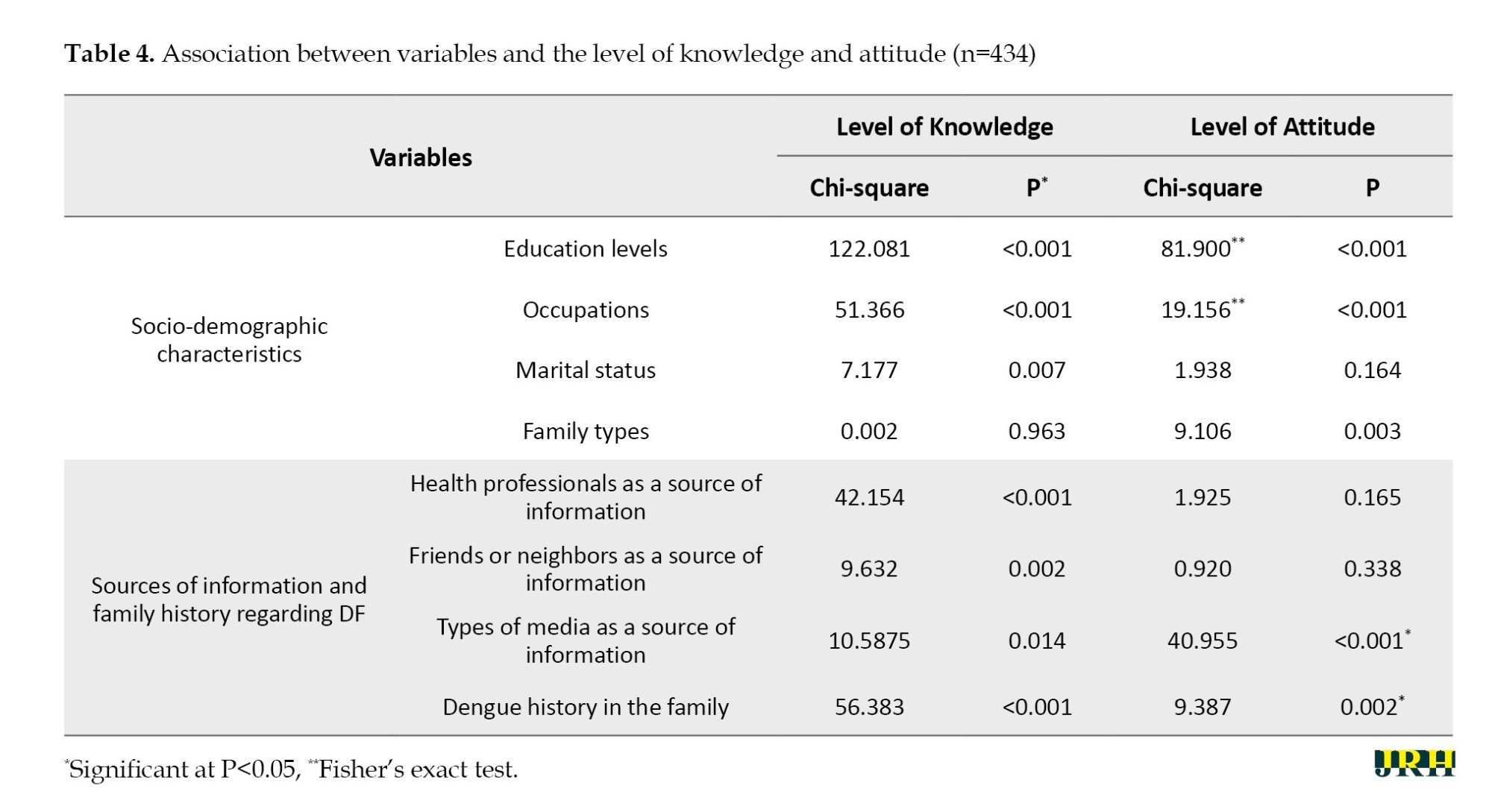
Our analysis revealed significant associations between knowledge levels and several factors (Table 4). Regarding knowledge levels, we identified significant associations with factors such as education levels, occupations, marital status, sources of information (health professionals, friends or neighbors, and types of media), and family history of dengue (all P<0.05). Notably, family types showed no significant association (P=0.963).
Similarly, significant associations were observed between respondents’ attitudes and their educational levels, occupations, family types, types of media as a source of information, and family history of DF (all P<0.05). In contrast, marital status, and health professionals, friends, or neighbors as sources of information did not show significant associations with respondents’ attitudes (P>0.05).
Discussion
In our investigation, the demographic profile of the respondents revealed a predominant representation of males who were married, possessed a secondary level of education and were actively engaged in economic activities. This aligns with the demographic characteristics observed in a prior study [15] and underscores demographic trends pertinent to DF awareness and prevention in Nepal. Additionally, our findings regarding the primary source of information on DF indicated that television was the most prominent medium, consistent with the results reported in previous studies [11, 16]. This underscores the influential role of mass media in disseminating public health messages and suggests avenues for targeted communication strategies.
Regarding the respondents’ knowledge of DF symptoms, transmission modes, and preventive measures, our study revealed that a significant portion believed fever to be a symptom and that transmission occurs through blood. Moreover, the majority recognized the preventive role of window screens and bed nets, while only a minority indicated that Aedes mosquitoes can be identified. A similar observation was made in a study conducted among community members of Kanchan Rural Municipality in the Rupandehi district of Nepal [12]. These insights indicate a need for tailored educational interventions that address specific misconceptions and promote accurate knowledge dissemination. Despite low overall knowledge levels, a positive attitude toward the seriousness of DF was prevalent among respondents. This sentiment aligns with findings from neighboring countries, like Bangladesh [17], and Pakistan [18], highlighting regional awareness of the disease’s severity. However, as noted in previous studies [12], translating positive attitudes into effective preventive behaviors requires comprehensive knowledge.
When evaluating knowledge levels, our study revealed a prevalent low knowledge base among respondents concerning DF. However, a positive attitude toward the illness was predominant. This aligns with a study conducted in Nepal [19], where despite low knowledge levels, a substantial percentage of the population exhibited a positive attitude. Similar trends were observed in studies conducted in Bangladesh [17], and India [20]. Studies conducted in Budhabhumi Municipality [21], and Madhyabindu Municipality [22] in Nepal also reported that the majority had low knowledge about DF. Interestingly, our findings diverged from some previous studies [23, 24], which reported higher knowledge levels. We attribute this discrepancy to variations in sample size, population characteristics, measurement methods, and study locations. Moreover, our study identified a positive correlation between knowledge and attitude, corroborating results from cross-sectional studies in Indonesia [4], Rawalpindi, Pakistan [25], and Nepal [19]. This underscores the importance of enhancing knowledge to foster more effective preventive behaviors.
In terms of sociodemographic factors, our study demonstrated statistically significant associations between education level, occupation, and marital status with the knowledge level of mothers, consistent with prior research [26, 27]. These findings suggest that educational attainment and professional background play crucial roles in shaping knowledge acquisition and attitudes toward DF prevention.
Similarly, the education level was found to be associated with attitude, echoing findings from previous studies [28]. Furthermore, our investigation revealed statistically significant associations between various sources of information and family history of DF with the knowledge and attitudes of respondents toward DF, consistent with findings from a previous study [29]. These insights underscore the multifaceted influences on DF awareness and highlight the importance of targeted public health interventions that leverage diverse communication channels and consider familial health histories.
Conclusion
In conclusion, our comprehensive investigation in Hetauda Sub-metropolitan City, Nepal, sheds light on the existing knowledge and attitudes towards DF within the community. The positive attitudes among the majority of respondents provide a promising foundation for community engagement and educational initiatives. The positive attitudes among the majority of respondents provide a promising foundation for community engagement and education initiatives. The findings also underscore the pivotal role of social networks, television, and the internet as primary sources of dengue information, highlighting the significance of utilizing these platforms for effective health communication strategies. The moderate positive correlation between knowledge and attitude scores suggests the potential for interventions that simultaneously enhance knowledge and foster positive attitudes. Furthermore, significant associations between respondents’ education, occupation, media usage, and family history of dengue with their knowledge and attitudes emphasize the nuanced nature of these factors. This information is crucial for tailoring interventions to specific demographic groups and optimizing the impact of public health campaigns.
In summary, this study offers valuable insights into the current state of knowledge and attitudes regarding DF in the community. It lays the groundwork for targeted interventions aimed at enhancing awareness, fostering positive attitudes, and contributing to the mitigation of dengue-related risks in Nepal.
Limitations
This community-based cross-sectional study was conducted exclusively in three wards of Hetauda Sub-Metropolitan City, which may limit the generalizability of findings to the broader population and introduce selection bias. Furthermore, the study focused solely on exploring knowledge and attitudes, lacking an assessment of practices related to DF within the community. Therefore, our understanding of current practices among community members regarding DF is constrained.
Methodologically, our study employed the Chi-square test for analysis, which is suitable for identifying associations between variables but is incapable of establishing causal relationships. Future research could employ longitudinal studies or intervention trials to explore causal relationships between factors identified in this study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Review Committee of Yeti Health Science Academy (Code: 079-84), and formal permission was granted from the Ward Office. Informed consent was obtained from the respondents before data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Nilisha Pradhan; Methodology: Rajesh Karki and Nilisha Pradhan; Investigation: All authors; Data curation: Nilisha Pradhan and Maheshor Kaphle; Formal analysis: Rajesh Karki; Writing of the original draft: Nilisha Pradhan; Review and editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all the respondents for dedicating their valuable time and participating in this study.
References
Dengue fever (DF) remains a significant global public health concern and is recognized as a key arthropod-borne disease agent [1]. It is an infectious illness caused by any of the four dengue virus serotypes: DENVs 1-4, which are primarily transmitted by mosquitoes, particularly the female Aedes mosquito [2]. The World Health Organization (WHO) reports a substantial increase in global dengue cases, impacting about half the world’s population, with 100-400 million infections annually. Many cases, often mild or asymptomatic, go unreported or are misdiagnosed as other febrile illnesses [3]. DF is associated with substantial morbidity, mortality, and economic burden, particularly in developing countries [4].
Nepal is prone to outbreaks of numerous infectious diseases [5], with the DF emerging as a significant health concern. Its prevalence is observed year-round across all 77 districts [6]. The first recorded instance of dengue in Nepal occurred in 2005, involving a foreigner in Chitwan district. Since then, dengue cases have progressively risen in Nepal, predominantly in the tropical lowlands and subtropical hilly regions, including Kathmandu. Between 2006 and 2022, Nepal experienced several dengue outbreaks [6]. According to the Epidemiology and Disease Control Division (EDCD) of Nepal in 2023, there were 51,243 reported dengue cases from all 77 districts, with 20 confirmed deaths. Bagmati Province reported 7,704 cases, constituting 15.0% of the national burden, while Makwanpur district reported 143 cases [7]. In 2022, Nepal experienced its largest-ever dengue outbreak, with the majority of cases reported in the Bagmati Province. The Kathmandu district was the most severely affected, with 14,376 cases, and the Makwanpur district, with 5,837 cases, ranked fourth after Lalitpur and Bhaktapur districts [8].
To effectively control and prevent DF, a comprehensive approach is needed. This includes combining conventional methods, like larvicides and insecticides, with community-based strategies. Integrated vector management (IVM) optimizes resource use and promotes sustainable interventions. Community engagement, with local leaders mobilizing efforts and sharing information, is crucial. Tailoring strategies to local needs and fostering community ownership are essential for sustained behavior change and improved prevention. Active community participation and cross-sector collaboration are key to effectively combatting DF [9]. In addition to factors, such as low socioeconomic status, inadequate sanitation, and substandard public health facilities, a lack of awareness among the population fosters conditions conducive to the emergence of this disease and significantly contributes to the socioeconomic burden in Nepal [5]. While numerous studies have focused on dengue-infected individuals, there is limited research on the knowledge and attitudes of the general population regarding dengue [10]. To design effective public health interventions for dengue in various altitudinal regions of Nepal, it is crucial to understand the community’s knowledge, attitudes, and practices (KAP) related to the dengue virus and its vectors [11]. Therefore, this study aimed to measure knowledge and attitudes among household members toward DF. Although this study focused on Bagmati Province, Nepal, its findings on community KAP regarding DF can inform interventions beyond this region. Understanding KAP can benefit similar areas in Nepal with comparable demographics and socioeconomic conditions and may hold value for other dengue-endemic countries facing similar contexts.
Locally, the research offers valuable data for policymakers in Bagmati Province, informing culturally appropriate prevention campaigns, resource allocation, and improved public health strategies. Publishing in an international journal allows for broader knowledge dissemination, contributing to a global understanding of KAP and informing more effective prevention strategies across dengue-endemic regions.
Methods
A cross-sectional study was carried out in Hetauda Sub-metropolitan City, located in the Makwanpur district of the Bagmati Province in central Nepal, serving as the capital of the Bagmati Province. Hetauda was selected for its status as a dengue-prone area. Specifically, out of the 19 wards in Hetauda, we focused on wards 4, 5, and 7. The selection of these wards was based on raw data obtained from the ward offices, revealing a higher prevalence of dengue during the study period. Additionally, resource constraints influenced the decision to limit the selection to these three wards.
The study population comprised household heads in the selected wards. In cases where the head of the household was unavailable or unable to participate, the next senior member was included. Participants were required to be 18 years or older. The sample size was determined using the Taro Yamane formula (Equation 1):
, where N represents the total number of households in the selected wards (N=30806), e is the margin of error (0.05), and a reliability level of 95%. Incorporating a 10% non-response rate yielded a final sample size of 434. A proportionate stratified random sampling method was used to select the required households. A list of households in the selected wards was prepared, and a cumulative total was calculated. The sampling interval (k) was then estimated as 30806/434=71. Starting from Ward No. 4, the first household was randomly selected, and every 71st interval thereafter was chosen until the required sample size was met. Local health workers and community members assisted in identifying households. Any respondents who did not give their consent to participate were excluded, and the next household in line was included.
A self-constructed structured questionnaire, developed based on two previous studies [12, 13], was utilized. The questionnaire covered socio-demographic information and included questions to assess knowledge and practices related to dengue. The questionnaire underwent validation by two public health experts, and its reliability was assessed using Cronbach’s α, yielding values of 0.91 for knowledge and 0.88 for attitude. Pretesting involved 10% of the sample population, which was excluded from the final analysis. Face-to-face interviews were conducted from March 1, 2023, to June 25, 2023. Data collection was carried out in the local Nepali language, with researchers directly involved in the process.
The questions covered the symptoms of DF, modes of transmission, and preventive measures. The knowledge level was dichotomized using an 80% cutoff point (score: ≤18 as low knowledge, score: ≥19 as good knowledge) [11]. The attitude was evaluated using a four-point Likert scale (strongly agree=four, agree=three, neutral=two, and disagree=one) with six positively phrased questions. Attitude scores ranged from 6 to 24, and a cutoff point of 50% was established (scores of 12 or less were considered a negative attitude, while scores higher than 12 were considered a positive attitude) [14].
Data were processed through editing, coding, and entry into SPSS software, version 26, and analysis was conducted as appropriate. Descriptive statistics, including frequency, percentage, and mean, were employed to analyze categorical variables. Similarly, the chi-square test was used to measure associations between socio-demographic variables and other selected variables with knowledge and attitude levels. Pearson correlation was also utilized to examine the relationship between knowledge and attitude. The significance level was set at a P<0.05.
Results
Out of 434 respondents, the majority (44.2%) belonged to the age group of 30-39, with a mean age of 37.50±7.40 years. Similarly, the majority were male (61.1%), belonged to the Jana Jati ethnicity (32.5%), practiced Hinduism (79.3%), had a secondary level education (37.6%), were employed in business (32.7%) or service (32.3%), were married (94.7%), and lived in a nuclear family setup (57.4%) (Table 1).
The majority (65.4%) mentioned health professionals as their source of information on DF, while 91.2% cited friends or neighbors. Similarly, regarding types of media, the primary source was television (85.3%), followed by the internet (81.3%) and radio (76.0%).
Out of the total of 24 questions assessing knowledge, 61.2% of respondents provided correct answers to all questions. Further analysis revealed that 60% of respondents correctly identified the signs and symptoms of DF, with the majority (86.9%) stating that fever is the major symptom. Regarding modes of transmission, 51.4% provided correct answers, and just over half (54.6%) correctly identified Aedes mosquitoes as the vectors of transmission. In terms of preventive measures, 77.1% provided correct answers, and among them, 91.7% believed that window screens and bed nets can prevent DF. However, only 28.8% mentioned the ability to identify Aedes mosquitoes (Table 2). Based on the total score obtained, the mean score was 14.7±6.45. When classified by level, the majority (77.2%) exhibited low knowledge, while only 22.8% demonstrated high knowledge.
Similarly, a total of 58.4% strongly agreed with all six statements used to assess attitudes, with the majority (mean score: 20.5±3.71; 74.7%) strongly agree with the statement that fever is a symptom of dengue (Table 3). When categorized by level, the majority (93.8%) displayed a positive attitude, while only 6.2% held a negative attitude toward DF.
Pearson correlation analysis was conducted, and the results indicated a moderate positive significant correlation (r=0.429) between the knowledge score and attitude score toward DF (P<0.001).
Our analysis revealed significant associations between knowledge levels and several factors (Table 4). Regarding knowledge levels, we identified significant associations with factors such as education levels, occupations, marital status, sources of information (health professionals, friends or neighbors, and types of media), and family history of dengue (all P<0.05). Notably, family types showed no significant association (P=0.963).
Similarly, significant associations were observed between respondents’ attitudes and their educational levels, occupations, family types, types of media as a source of information, and family history of DF (all P<0.05). In contrast, marital status, and health professionals, friends, or neighbors as sources of information did not show significant associations with respondents’ attitudes (P>0.05).
Discussion
In our investigation, the demographic profile of the respondents revealed a predominant representation of males who were married, possessed a secondary level of education and were actively engaged in economic activities. This aligns with the demographic characteristics observed in a prior study [15] and underscores demographic trends pertinent to DF awareness and prevention in Nepal. Additionally, our findings regarding the primary source of information on DF indicated that television was the most prominent medium, consistent with the results reported in previous studies [11, 16]. This underscores the influential role of mass media in disseminating public health messages and suggests avenues for targeted communication strategies.
Regarding the respondents’ knowledge of DF symptoms, transmission modes, and preventive measures, our study revealed that a significant portion believed fever to be a symptom and that transmission occurs through blood. Moreover, the majority recognized the preventive role of window screens and bed nets, while only a minority indicated that Aedes mosquitoes can be identified. A similar observation was made in a study conducted among community members of Kanchan Rural Municipality in the Rupandehi district of Nepal [12]. These insights indicate a need for tailored educational interventions that address specific misconceptions and promote accurate knowledge dissemination. Despite low overall knowledge levels, a positive attitude toward the seriousness of DF was prevalent among respondents. This sentiment aligns with findings from neighboring countries, like Bangladesh [17], and Pakistan [18], highlighting regional awareness of the disease’s severity. However, as noted in previous studies [12], translating positive attitudes into effective preventive behaviors requires comprehensive knowledge.
When evaluating knowledge levels, our study revealed a prevalent low knowledge base among respondents concerning DF. However, a positive attitude toward the illness was predominant. This aligns with a study conducted in Nepal [19], where despite low knowledge levels, a substantial percentage of the population exhibited a positive attitude. Similar trends were observed in studies conducted in Bangladesh [17], and India [20]. Studies conducted in Budhabhumi Municipality [21], and Madhyabindu Municipality [22] in Nepal also reported that the majority had low knowledge about DF. Interestingly, our findings diverged from some previous studies [23, 24], which reported higher knowledge levels. We attribute this discrepancy to variations in sample size, population characteristics, measurement methods, and study locations. Moreover, our study identified a positive correlation between knowledge and attitude, corroborating results from cross-sectional studies in Indonesia [4], Rawalpindi, Pakistan [25], and Nepal [19]. This underscores the importance of enhancing knowledge to foster more effective preventive behaviors.
In terms of sociodemographic factors, our study demonstrated statistically significant associations between education level, occupation, and marital status with the knowledge level of mothers, consistent with prior research [26, 27]. These findings suggest that educational attainment and professional background play crucial roles in shaping knowledge acquisition and attitudes toward DF prevention.
Similarly, the education level was found to be associated with attitude, echoing findings from previous studies [28]. Furthermore, our investigation revealed statistically significant associations between various sources of information and family history of DF with the knowledge and attitudes of respondents toward DF, consistent with findings from a previous study [29]. These insights underscore the multifaceted influences on DF awareness and highlight the importance of targeted public health interventions that leverage diverse communication channels and consider familial health histories.
Conclusion
In conclusion, our comprehensive investigation in Hetauda Sub-metropolitan City, Nepal, sheds light on the existing knowledge and attitudes towards DF within the community. The positive attitudes among the majority of respondents provide a promising foundation for community engagement and educational initiatives. The positive attitudes among the majority of respondents provide a promising foundation for community engagement and education initiatives. The findings also underscore the pivotal role of social networks, television, and the internet as primary sources of dengue information, highlighting the significance of utilizing these platforms for effective health communication strategies. The moderate positive correlation between knowledge and attitude scores suggests the potential for interventions that simultaneously enhance knowledge and foster positive attitudes. Furthermore, significant associations between respondents’ education, occupation, media usage, and family history of dengue with their knowledge and attitudes emphasize the nuanced nature of these factors. This information is crucial for tailoring interventions to specific demographic groups and optimizing the impact of public health campaigns.
In summary, this study offers valuable insights into the current state of knowledge and attitudes regarding DF in the community. It lays the groundwork for targeted interventions aimed at enhancing awareness, fostering positive attitudes, and contributing to the mitigation of dengue-related risks in Nepal.
Limitations
This community-based cross-sectional study was conducted exclusively in three wards of Hetauda Sub-Metropolitan City, which may limit the generalizability of findings to the broader population and introduce selection bias. Furthermore, the study focused solely on exploring knowledge and attitudes, lacking an assessment of practices related to DF within the community. Therefore, our understanding of current practices among community members regarding DF is constrained.
Methodologically, our study employed the Chi-square test for analysis, which is suitable for identifying associations between variables but is incapable of establishing causal relationships. Future research could employ longitudinal studies or intervention trials to explore causal relationships between factors identified in this study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Review Committee of Yeti Health Science Academy (Code: 079-84), and formal permission was granted from the Ward Office. Informed consent was obtained from the respondents before data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Nilisha Pradhan; Methodology: Rajesh Karki and Nilisha Pradhan; Investigation: All authors; Data curation: Nilisha Pradhan and Maheshor Kaphle; Formal analysis: Rajesh Karki; Writing of the original draft: Nilisha Pradhan; Review and editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all the respondents for dedicating their valuable time and participating in this study.
References
- Gupta BP, Lamsal M, Chaulagain S, Rauniyar R, Malla R, Shrestha S, et al. Emergence of dengue in Nepal. Virusdisease. 2018; 29(2):129-33. [DOI:10.1007/s13337-018-0439-3] [PMID] [PMCID]
- Khetarpal N, Khanna I. Dengue fever: Causes, complications, and vaccine strategies. Journal of Immunology Research. 2016; 2016:6803098. [DOI:10.1155/2016/6803098] [PMID] [PMCID]
- World Health Organization (WHO). Dengue and severe dengue [Internet]. 2024 [Updated 2024 April 23]. Available from: [Link]
- Harapan H, Rajamoorthy Y, Anwar S, Bustamam A, Radiansyah A, Angraini P, et al. Knowledge, attitude and practice regarding dengue virus infection among inhabitants of Aceh, Indonesia: A cross-sectional study. BMC Infectious Diseases. 2018; 18(1):96. [DOI:10.1186/s12879-018-3006-z] [PMID] [PMCID]
- Acharya KP, Chaulagain B, Acharya N, Shrestha K, Subramanya SH. Establishment and recent surge in spatio-temporal spread of dengue in Nepal. Emerging Microbes & Infections. 2020; 9(1):676-9. [DOI:10.1080/22221751.2020.1740062] [PMID] [PMCID]
- Department of Health Services. Annual report. Kathmandu: Department of Health Services; 2022. [Link]
- Epidemiology and Disease Control Division. Situation report on dengue in Nepal-2023. Kathmandu: Epidemiology and Disease Control Division; 2023. [Link]
- Pokharel P, Khanal S, Ghimire S, Pokhrel KM, Shrestha AB. Frequent outbreaks of dengue in Nepal–causes and solutions: A narrative review. IJS Global Health. 2023; 6(5):e0351. [DOI:10.1097/GH9.0000000000000351]
- Samsudin NA, Othman H, Siau CS, Zaini ZI. Exploring community needs in combating aedes mosquitoes and dengue fever: A study with urban community in the recurrent hotspot area. BMC Public Health. 2024; 24(1):1651. [DOI:10.1186/s12889-024-18965-1] [PMID] [PMCID]
- Paudel D, Kakchapati S, Lageju N, Karki S, Dhungana J, Regmi S, et al. Factors influencing the knowledge, attitude, and practices of police personnel toward dengue fever in Kathmandu, Nepal. Journal of Occupational Health. 2023; 65(1):e12421. [DOI:10.1002/1348-9585.12421] [PMID] [PMCID]
- Phuyal P, Kramer IM, Kuch U, Magdeburg A, Groneberg DA, Lamichhane Dhimal M, et al. The knowledge, attitude and practice of community people on dengue fever in central Nepal: A cross-sectional study. BMC Infectious Diseases. 2022; 22(1):454. [DOI:10.1186/s12879-022-07404-4] [PMID] [PMCID]
- Khanal R, Thapa R, Khanal M. Knowledge and preventive practices regarding dengue fever in Nepal. American Journal of Health Research. 2021; 9(6):218-28. [DOI:10.11648/j.ajhr.20210906.12]
- Manzoor S, Afzal M, Hussain M, Gilani S. Knowledge attitude and practice towards dengue fever prevention among adult population of rural area of Lahore Pakistan. International Journal of Scientific & Engineering Research. 2018; 9(5):1665-73. [Link]
- Saghir MA, Ahmed WAM, Dhaiban MMA, Osman ME, Abduljabbar NI. Knowledge, attitude, and practices of the community toward dengue fever in Shabwah Governorate, Yemen: A descriptive study. The Journal of the Egyptian Public Health Association. 2022; 97(1):27. [DOI:10.1186/s42506-022-00121-5] [PMID] [PMCID]
- Sajjad S, Ishfaq K, Bibi Z. Knowledge, attitudes and practices regarding dengue fever among people in district multan, Pakistan. Annals of Social Sciences and Perspective. 2023; 4(2):563-79. [DOI:10.52700/assap.v4i2.338]
- Adhikari S, Adhikari G. Knowledge, attitude and preventive practices regarding dengue fever among the community people of Baratpur. The BSMC Journal of Local Development. 2016; 1(1):10-20. [Link]
- Sharmila N, Habib SE, Health C. Knowledge, attitude, and practice towards dengue: A study among the inhabitants of malibagh of Dhaka city, Bangladesh. Journal of Social Behavior and Community Health. 2021; 5(1):630-40. [DOI:10.18502/jsbch.v5i1.6733]
- Shafique M, Muhammad Mukhtar M, Areesantichai C, Perngparn U. Knowledge, attitude and practices towards dengue fever among the communities living in slums of Islamabad, Pakistan; A cross-sectional survey. International Journal of Multidisciplinary Research and Publications. 4(1):85-90. [Link]
- Dhimal M, Aryal KK, Dhimal ML, Gautam I, Singh SP, Bhusal CL, Kuch U. Knowledge, attitude and practice regarding dengue fever among the healthy population of highland and lowland communities in central Nepal. Plos One. 2014; 9(7):e102028. [DOI:10.1371/journal.pone.0102028] [PMID] [PMCID]
- Basra GK, Rohilla S, Singh S. Knowledge, attitude and practice regarding dengue fever among residents of Indira Colony, Ghaziabad. Journal of Communicable Diseases. 2019; 51(3):22-7. [DOI:10.24321/0019.5138.201922]
- Paudel AK, Chhetri MR, Devkota N, Maharjan PL, Pokhrel S, Kaphle M. Knowledge and practices on dengue prevention among the people of Buddhabhumi Municipality of Nepal: a cross-sectional study. Nepal Medical College Journal. 2023; 25(1):42-8. [DOI:10.3126/nmcj.v25i1.53375]
- Mahato N, Khanal N, Luitel N, Chaudhary Y, Marasini R. Knowledge and practice of people regarding prevention of dengue in Madhyabindu Municipality, Nawalparasi, Nepal. One Health Journal of Nepal. 2022; 2(4):38-40. [Link]
- Neupane B, Rijal KR, Banjara MR, Pandey BD. Knowledge and prevention measures against dengue in southern Nepal. Journal of Coastal Life Medicine. 2014; 2(12):998-1001. [DOI:10.12980/JCLM.2.2014APJTD-2014-0084]
- Yadav K, Yadav N, Prakash S, Yadav BK. Knowledge, attitude and preventive practices of dengue in local community people of Janakpurdham. Janaki Medical College Journal of Medical Science. 2022; 10(03):51-63. [DOI:10.3126/jmcjms.v10i03.55554]
- Khan KA, Qureshi Z, Anwar S, Ashraf S, Fatima S, Fawad F. Knowledge, attitude, and practice about dengue transmission among residents of dengue prevalent zones of Rawalpindi. Pakistan Journal of Public Health. 2022; 12(2):72-6. [DOI:10.32413/pjph.v12i2.1002]
- Sah NK. Knowledge and practice on prevention and control of dengue fever among people at Mangalpur VDC, Chitwan district of Nepal. Journal of Chitwan Medical College. 2021; 11(2):92-7. [DOI:10.54530/jcmc.285]
- Alhoot MA, Abdalqader M, Mohammed MF, Alwan MR, Eltariki FEM, Aziz FM, et al. Assessment of knowledge, attitudes and practice toward dengue fever among University Students in Malaysia. Global Journal of Public Health Medicine. 2021; 3(1):289-300. [DOI:10.37557/gjphm.v3i1.76]
- Fernandez-Guzman D, Caira-Chuquineyra B, Calderon-Ramirez PM, Cisneros-Alcca S, Benito-Vargas RM. Sociodemographic factors associated to knowledge and attitudes towards dengue prevention among the Peruvian population: Findings from a national survey. BMJ Open. 2023; 13(3):e071236. [DOI:10.1136/bmjopen-2022-071236] [PMID] [PMCID]
- Ghebrehiwot L, Huda B. Factors associated with knowledge and attitude on prevention of dengue fever among international postgraduate students in a Malaysian university. International Journal of Public Health and Clinical Sciences. 2018; 5(4):123-32. [Link]
Type of Study: Orginal Article |
Subject:
● Disease Control
Received: 2024/05/17 | Accepted: 2024/07/9 | Published: 2024/09/1
Received: 2024/05/17 | Accepted: 2024/07/9 | Published: 2024/09/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
