

Volume 16, Issue 3 (May & June 2026)
J Research Health 2026, 16(3): 305-314 |
Back to browse issues page

Ethics code: IR.KHOY.REC.1402.044
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sodeify R, Habibpour Z, Mokhtari M, Omiya M. Association Between Cultural Intelligence and Professional Socialization in Nursing Students: A Cross-sectional Study. J Research Health 2026; 16 (3) :305-314
URL: http://jrh.gmu.ac.ir/article-1-2699-en.html
URL: http://jrh.gmu.ac.ir/article-1-2699-en.html



1- Department of Medical-Surgical Nursing, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran.
2- Department of Psychiatric Nursing, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran. ,habibpoor_z@khoyums.ac.ir
3- Department of Epidemiology, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran.
4- Department of Medical-Surgical Nursing, Student Research Committee, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran.
2- Department of Psychiatric Nursing, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran. ,
3- Department of Epidemiology, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran.
4- Department of Medical-Surgical Nursing, Student Research Committee, School of Nursing, Khoy University of Medical Sciences, Khoy, Iran.
Full-Text [PDF 644 kb]
(133 Downloads)
| Abstract (HTML) (393 Views)
Full-Text: (19 Views)
Introduction
Socialization is a lifelong process that begins with the internalization of familial norms and subcultural values, fundamentally shaping an individual’s self-concept [1]. As individuals mature and assume roles within new social groups, they progressively acquire new norms and, in doing so, refine their self-identity [2]. Professional socialization—a specialized dimension of this broader process—is inherently complex, encompassing learning, interaction, transformation, and adaptation. It is marked by characteristics, such as unpredictability, nonlinearity, and involuntariness, as well as its inevitable, dynamic, and continuous nature [3]. A substantial portion of professional competence is cultivated through interpersonal relationships, collaboration, and teamwork within various social and organizational settings [4]. Throughout the lifespan, individuals engage in personal, situational, and institutional interactions influenced by a range of variables—including social status, religious affiliation, gender, and ethnicity [5]—all of which are shaped by the cultural context [6]. The competencies necessary for engagement within professional cultures and effective functioning in social organizations are developed progressively over time through exposure and experience [7, 8]. Cultural intelligence (CQ) refers to an individual’s capability to function and communicate effectively in culturally diverse situations. Unlike other forms of intelligence, CQ enables individuals to display adaptive behaviors and respond appropriately across cultural boundaries [7]. In intercultural contexts—where traditional forms of cognitive, emotional, or social intelligence may be insufficient—CQ acts as a bridge, facilitating both conceptual understanding and behavioral alignment across different cultural frameworks [9]. Importantly, individuals possessing high levels of general intelligence or well-developed social skills may still encounter challenges in intercultural settings if their CQ is underdeveloped [10, 11]. Emotional and social cues, while meaningful in familiar contexts, often fail to translate across divergent cultural systems [12].
In contrast, individuals with elevated CQ can accurately interpret behaviors rooted in unfamiliar cultural norms and adapt accordingly [10, 11]. A substantial body of research has documented significant relationships between CQ and various outcomes, including enhanced social tolerance [13, 14], improved interpersonal interactions [12], career development and mobility [15, 16], and heightened professional competence in nursing and healthcare contexts. Several studies underscore the predictive value of CQ for specific professional behaviors and competencies [16, 17]. In the nursing profession, CQ is increasingly regarded as a critical determinant of healthcare quality, directly contributing to the efficiency and inclusivity of health systems [12]. Attaining global professional competence requires the ability to navigate and manage cultural diversity—one of the key advantages afforded by high CQ [18].
CQ not only helps individuals clarify their career goals and professional paths but also fosters meaningful, effective relationships with people from diverse cultural backgrounds [19]. As nurses enter the workforce as global citizens in increasingly diverse ethnic, cultural, and linguistic environments, adopting new professional identities becomes essential to fostering inclusive, respectful, and high-performing clinical and academic settings [20]. Institutions and organizations operating internationally or within culturally pluralistic societies must regard ethnic, cultural, and social expectations as integral to professional practice [21].
In Iran—a country characterized by considerable cultural diversity, including various ethnicities, climates, religions, dialects, values, and belief systems—such distinctions can significantly affect interpersonal communication and professional performance in healthcare delivery. To address these complex dynamics, this study investigates the relationship between CQ and professional socialization among nursing students at Khoy University of Medical Sciences, Iran.
Methods
Study design
This cross-sectional study was conducted among nursing students at Khoy University of Medical Sciences in April 2024.
Sampling
Questionnaires were distributed to students who met the predefined inclusion criteria. The inclusion criteria included willingness to participate, enrollment as a nursing student, and completion of at least one semester of clinical internship. The exclusion criteria included concurrent employment during academic study, prior academic experience or graduation in another field, participation in CQ or professional socialization training programs, presence of apparent psychiatric disorders, history of psychotropic medication use, and transfer or guest student status during the current semester. Statistical analyses were conducted on 143 fully completed questionnaires that met the inclusion criteria.
Measures and procedures
The sample size was calculated using Cochran’s formula for finite populations. Assuming a 95% confidence level, a 5% margin of error, and maximum variability (P=0.5), the minimum required sample size was estimated at 125. To account for potential non-responses, this number was increased by 20%, resulting in a target sample size of 150 students. Using convenience sampling, the researcher invited 178 eligible students to participate. After obtaining ethical approval and permission to access classes, the researcher attended scheduled class sessions. At the start of each class, the study was briefly introduced to all students, and the study’s purpose, confidentiality, and voluntary nature were clearly explained. Students who met the inclusion criteria and expressed interest in participating were then provided with the questionnaires during the last 15 minutes of the class session. Questionnaires were collected immediately upon completion. Data were collected using a demographic checklist, the CQ questionnaire (CIQ), and the professional socialization questionnaire. A total of 143 fully completed questionnaires were received, exceeding the minimum required sample size and ensuring sufficient statistical power for analysis.
CIQ
The 20-item CIQ was developed by Ang et al. in 2004 and assesses four distinct dimensions of CQ. Items 1–4 evaluate the metacognitive (strategic) component; items 5–11 assess the cognitive (knowledge-based) dimension; items 12–15 measure the motivational aspect; and items 16–20 pertain to the behavioral component. It uses a seven-point Likert scale ranging from “totally disagree” (1) to “totally agree” (7), yielding total score between 20 and 140, with higher scores indicating greater CQ. Scores are calculated by summing all item responses. The CIQ evaluates an individual’s capacity to communicate and function effectively across diverse cultural contexts [22]. The Persian version of this questionnaire was adapted and validated by Ahanchian et al. in 2011. Reliability coefficients (Cronbach’s α) for the subscales were 0.83 (metacognitive), 0.86 (cognitive), 0.85 (motivational), and 0.76 (behavioral) [23]. The instrument’s reliability and validity have also been confirmed in subsequent studies conducted by Ghadampour et al. and Ghaderpanah et al. [24, 25].
Professional socialization questionnaire
The professional socialization questionnaire was developed by Bishive et al. [19] in 2016 and comprises 48 items categorized into four dimensions: professional valuation and recognition (items 1–11), professional skills (items 12–35), management and organizational policies (items 36–45), and interpersonal communication (items 46–48). Respondents rate each item on a five-point Likert scale, where 1 indicates “very little agreement” and 5 indicates “very much agreement”. Total scores range from 48 to 240, with higher values indicating greater professional socialization.
Interpretation of the mean scores in each dimension is as follows: Scores between 0% and 33% are considered low, scores between 34% and 66% are moderate, and scores between 67% and 100% are classified as high. Content validity was established using both quantitative and qualitative methods. The instrument demonstrated strong internal consistency, with a Cronbach’s α coefficient of 0.92 and an intraclass correlation coefficient of 0.94 [19]. The reliability and validity of this questionnaire were further confirmed in a study by Barkhordari et al. [26].
Variables and definitions
The primary outcome variable in this study was professional socialization, assessed using the professional socialization questionnaire. It was developed by Bishive et al. [19]. This instrument consists of 48 items distributed across four dimensions: professional valuation and recognition, professional skills, management and organizational policies, and interpersonal communication.
The primary predictor variable was CQ, measured using the CI scale, which includes four components: Cognitive, metacognitive, motivational, and behavioral.
Potential confounders included age, gender, marital status, and residential status (boarding vs non-boarding); however, no multivariable adjustments were made due to the study’s cross-sectional and correlational design. Effect modification was not evaluated. Since the study did not involve clinical diagnosis, diagnostic criteria were not applicable.
Data analysis
Data analysis was performed using descriptive statistics (including frequency distributions, Mean±SD, independent t-tests to compare two groups (male and female), and one-way analysis of variance (ANOVA) for comparing more than two groups, assuming normal distribution of the data. The Pearson correlation coefficient and linear regression analysis were applied to examine associations between variables. All analyses were conducted using SPSS software, version 20, with statistical significance set at P<0.05.
Results
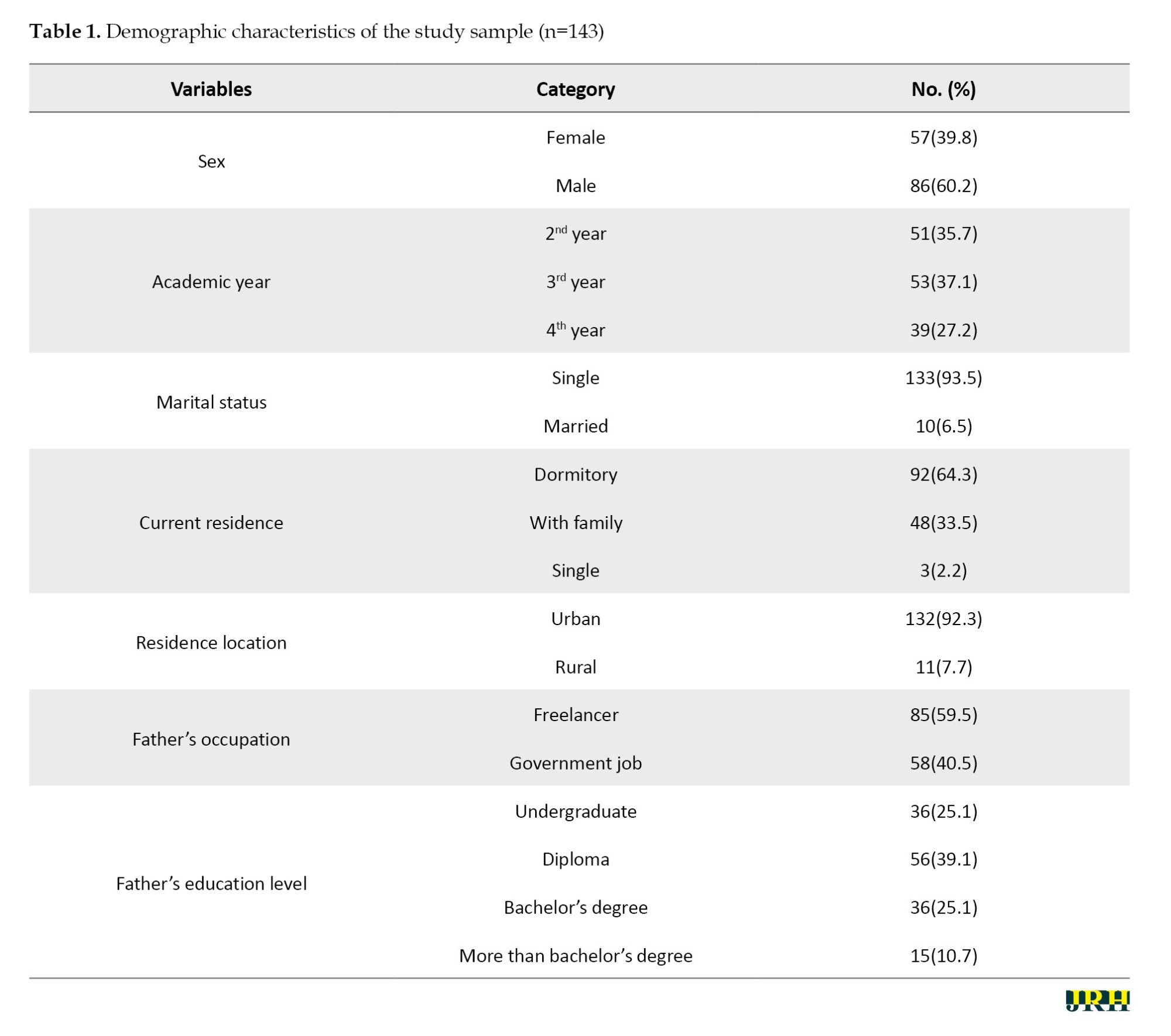
The results indicated that the mean age of participants was 22.62±1.85 years. Among the 143 participants, 59.5% (n=91) were male, 93.5% (n=134) were single, 63.4% (n=91) lived in urban areas, and 92.2% (n=132) lived in university dormitories (Table 1).
The mean CQ score among nursing students at Khoy University of Medical Sciences, Iran, was 63.88 out of a possible 140. The mean professional socialization score was 110.62 out of a possible 240, indicating a moderate level of professional socialization among the students.
Table 2 presents the results of the Pearson correlation test, which demonstrates a significant positive relationship between CQ and professional socialization among nursing students.
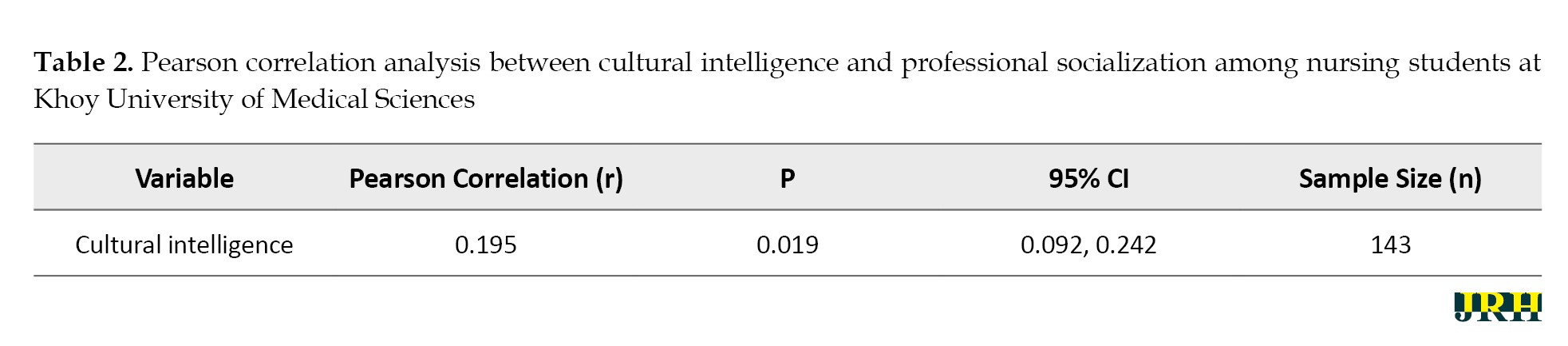
This indicates that higher CQ is associated with increased levels of professional socialization. The relationship between professional socialization and students’ demographic characteristics was examined, revealing significant associations with marital status, gender, and academic grade level Table 3.
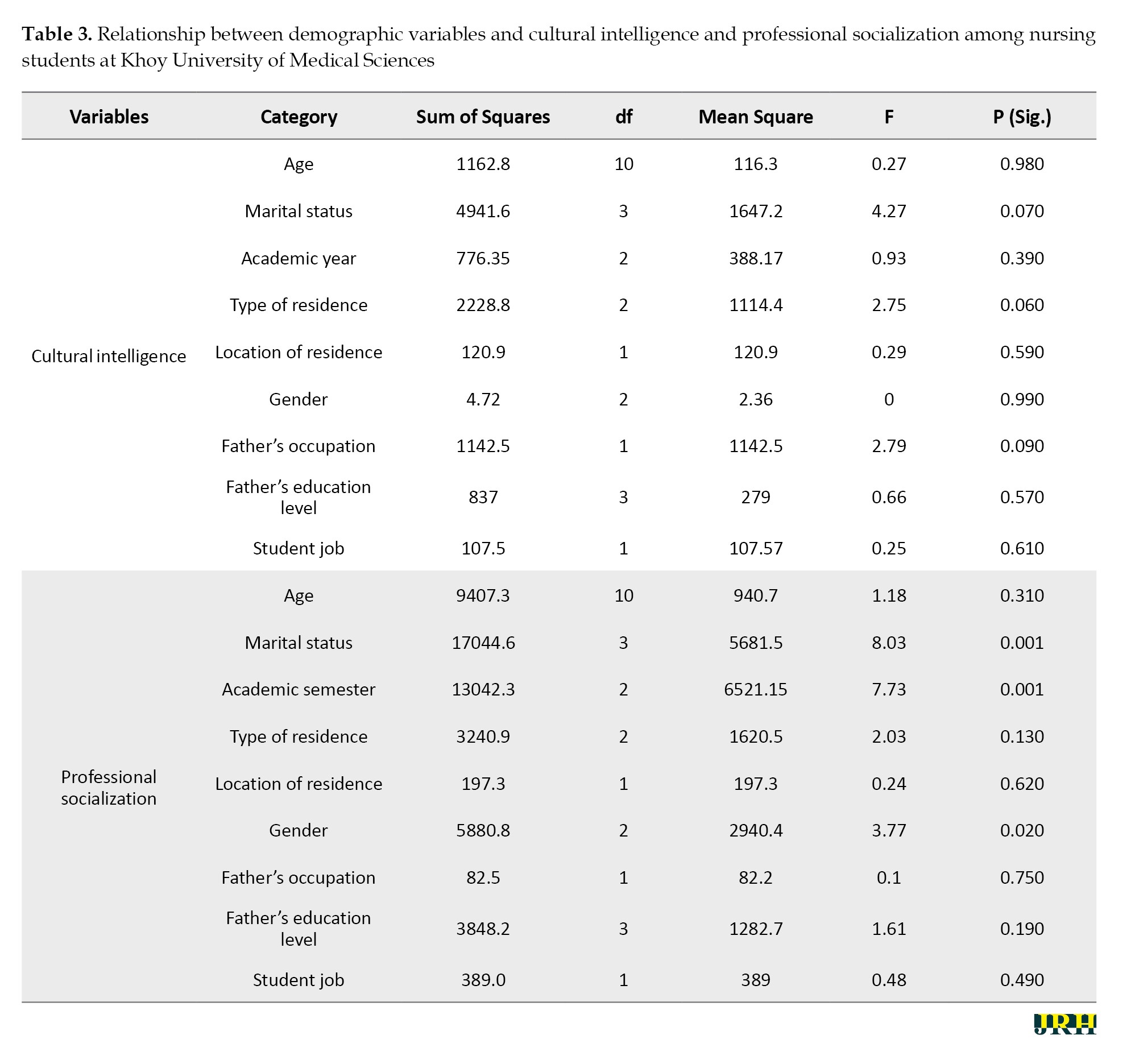
Table 4 shows that the coefficient of determination (R²) represents the proportion of variance in professional socialization explained by each dimension of CQ.
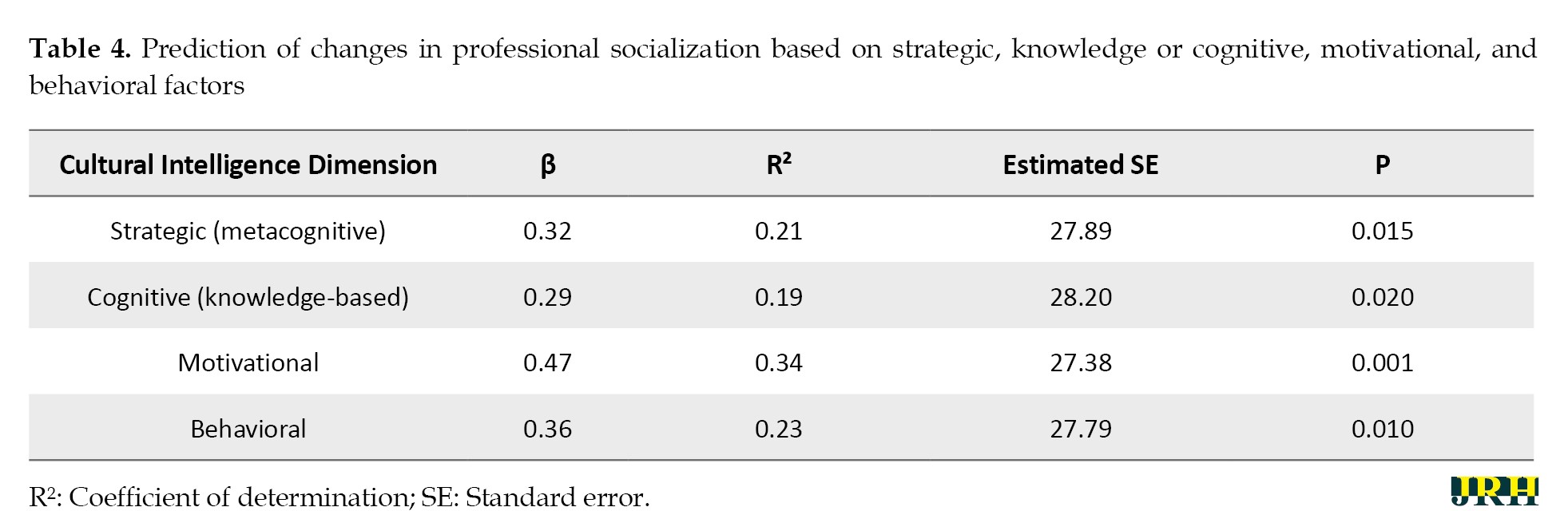
The findings indicate that the strategic (metacognitive) dimension explains 21% of the variance; the cognitive (knowledge-based) dimension explains 19%, the motivational dimension 34%, and the behavioral dimension 23%. Among these, motivational factors showed the strongest predictive power (R²=0.34, β=0.47, P=0.001), while cognitive factors had the weakest predictive effect (R²=0.19, β=0.29, P=0.020).
Discussion
This study examined the relationship between CQ and professional socialization among nursing students at Khoy University of Medical Sciences, Iran. The results indicated that the participating nursing students demonstrated a moderate level of CQ, and that CQ was not significantly associated with any of the examined demographic characteristics. In this context, Hassani and colleagues, in a study conducted in Iran, reported that the average CQ score among university students ranged from weak to moderate [27]. Ahanchian et al. [23] found that Iranian nurses demonstrated average levels of CQ. Consistent with these findings, Göl et al. in a study conducted in Turkey, reported that undergraduate nursing students exhibited an average level of CQ [28]. In contrast, Abouelenein and Mostafa Mohamed, in a study conducted in Egypt, found that 76.6% of nursing students demonstrated high levels of CQ, and no significant associations were observed between CQ and demographic characteristics [29]. Given these findings, nursing students are encouraged to enter their future professional roles with emotional composure and to communicate effectively with colleagues in a manner that avoids discomfort or misunderstanding. Therefore, implementing an appropriately designed educational program may enhance students’ capacity to recognize and respect cultural diversity.
This study revealed that the average professional socialization score among the participating nursing students was low, and professional socialization was found to be significantly associated with both gender and marital status. Most previous studies on professional socialization have reported average levels of professional socialization among nursing students. For example, a study by Ghaderpanah in Iran indicated that 93% of nursing students scored in the low to average range of professional socialization [25]. Barkhordari’s research reported average professional socialization scores among nursing students [26]. In Sanandaj, Zandi et al. found that most nurses exhibited a moderate level of professional socialization, which aligns with the findings of the present study [30]. However, findings by Noohi et al. demonstrated high levels of professional socialization among undergraduate nursing students [31]. Professional socialization during undergraduate nursing education is a critical component in training clinically competent practitioners and serves as the foundation through which novice nurses acquire essential research skills, critical thinking, and reasoning abilities [32]. When organizational and professional socialization processes are effectively implemented, they foster greater organizational commitment, which is a key factor in enhancing efficiency and performance within healthcare settings [25]. Therefore, promoting and strengthening professional socialization among nursing students is imperative to optimize their professional development and improving their future clinical competence.
The findings support the primary objective of the study, revealing a significant positive association between CQ and professional socialization among nursing students—higher levels of CQ were linked to stronger professional socialization. Among the four dimensions, the motivational component explained the largest proportion of variance (34%), followed by the behavioral (23%), strategic (21%), and cognitive (19%) dimensions. This underscores the central role of motivation in shaping professional identity and suggests that interventions aimed at enhancing professional socialization in multicultural or organizational settings should prioritize strategies that foster cultural motivation, such as promoting intercultural curiosity and self-efficacy.
Although research explicitly investigating the relationship between CQ and professional socialization within educational contexts remains limited, findings from related studies offer empirical support for these results. For example, Bahaadini et al. reported that nurses with higher levels of CQ also exhibited stronger scores in social interaction [12], while those with elevated CQ demonstrated greater professional competencies [33]. In a separate study, Beheshti et al. found that CQ accounted for approximately 12% of the variance in social tolerance among citizens [13]. A subsequent investigation by the same researcher, focusing on the Baloch population, reported that CQ explained roughly 26% of the variance in social tolerance [14]. These findings suggest that individuals who are more adept at navigating culturally diverse environments and who display a higher degree of openness toward individuals with differing characteristics are more likely to demonstrate increased tolerance and adaptability in social interactions [13, 14].
Numerous studies conducted across diverse populations have identified significant associations between CQ and various psychosocial constructs, including interpersonal communication, organizational citizenship behavior among teachers [33], organizational sociability in newly recruited industrial employees [34], auditors’ social responsibility [35], social identity among students of educational sciences [33], social perspective-taking in professional settings [36], and adaptive performance among nurses [37]. CQ endows medical students with the capacity to function effectively in multicultural clinical environments. Empirical evidence has shown that higher levels of CQ are positively associated with enhanced interpersonal interactions among healthcare professionals—an essential factor in promoting collaboration in culturally diverse healthcare teams [12, 38].
The ability to identify and appreciate cultural differences strengthens communicative competence and enables nursing students to engage more effectively with patients from various sociocultural backgrounds. This form of cultural adaptation contributes not only to individual development but also to the advancement of institutional goals by fostering a more cohesive, respectful, and inclusive workplace [27]. Furthermore, culturally intelligent managers consistently demonstrate superior interpersonal competence when interacting with individuals from dissimilar cultural backgrounds, enhancing their effectiveness in fulfilling professional roles [39].
Therefore, the integration of CQ into nursing curricula is essential for fostering effective interprofessional collaboration within healthcare teams. Given that nurses often serve as the primary point of contact for patients, their ability to communicate across cultural boundaries is fundamental to ensuring both patient safety and satisfaction [40]. Empirical studies have shown that culturally competent nurses are more adept at navigating intercultural interactions, enhancing teamwork and collaboration in clinical environments. This competency is critical in response to the increasing cultural heterogeneity of patient populations, which necessitates a healthcare workforce capable of delivering nuanced and culturally congruent care [16].
Among the dimensions of CQ, cultural sensitivity is especially influential in shaping patient satisfaction and clinical outcomes. Research has demonstrated that patients report greater satisfaction when cultural considerations are acknowledged and integrated into their individualized care plans [38, 40]. Such culturally attuned care not only improves patient satisfaction but also enhances treatment efficacy by aligning care strategies with patients’ values, preferences, and cultural norms. For instance, culturally sensitive approaches have been shown to increase adherence to medical recommendations among individuals from diverse backgrounds, contributing to better overall health outcomes [27].
Given the well-established benefits of CQ in nursing and medical education, it is essential to prioritize its integration into curriculum design. Embedding cross-cultural nursing content within educational frameworks can substantially enhance students’ cultural competence and better equip them to navigate the complexities of today’s diverse healthcare environments. Innovative pedagogical approaches that emphasize experiential learning—such as simulation-based training involving culturally varied patient scenarios—have the potential to improve students’ self-efficacy and confidence, reinforcing their ability to deliver culturally responsive and patient-centered care [16].
Conclusion
This study found that nursing students possess a moderate level of CQ, which is significantly associated with higher levels of professional socialization. This suggests that CQ plays a key role in helping students internalize professional values, behaviors, and responsibilities. As such, enhancing CQ should be a priority in nursing education. Incorporating intercultural training and reflective practice into the curriculum may effectively support this goal. Future research should explore evidence-based strategies for integrating CQ into health professions education to better prepare graduates for diverse clinical environments.
Limitations and recommendations
The cross-sectional design of this study inherently limits the ability to infer causal relationships, restricting the findings to associations between variables and precluding definitive conclusions about whether CQ influences professional socialization or vice versa. Data collection relied on self-report questionnaires, which are vulnerable to social desirability and other response biases. Although measures were taken to minimize these biases—such as guaranteeing participant confidentiality and stressing the importance of honest responses—the potential for bias remains and may have affected the results in either direction. While the study controlled for certain demographic factors by excluding participants with prior work experience, previous education in unrelated fields, or concurrent hospital employment, other influential variables were not accounted for. These include personality traits, family background, social support systems, prior experiences, and exposure to diverse ethnic groups within familial or community contexts, all of which may impact CQ or professional socialization beyond the scope of this research. The sample was limited to nursing students at Khoy University of Medical Sciences, restricting the generalizability of the findings to the broader nursing student population. Accordingly, the results should be interpreted with caution. Future studies employing longitudinal designs and larger, more heterogeneous samples are recommended to better clarify the temporal relationship and causal dynamics between CQ and professional socialization.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Khoy University of Medical Sciences, Khoy, Iran (Code: IR.KHOY.REC.1402.044).
Funding
This study was financially supported by Khoy University of Medical Sciences, Khoy, Iran.
Authors' contributions
Conceptualization, study design, and supervision: Zeinab Habibpour and Roghieh Sodeify; Data collection: Masoud Omiya; Data analysis: Mehdi Mokhtari; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank all the nursing students who participated in this study. They also express their appreciation to the Research Vice Chancellor of Khoy University of Medical Sciences for providing financial and administrative support.
Socialization is a lifelong process that begins with the internalization of familial norms and subcultural values, fundamentally shaping an individual’s self-concept [1]. As individuals mature and assume roles within new social groups, they progressively acquire new norms and, in doing so, refine their self-identity [2]. Professional socialization—a specialized dimension of this broader process—is inherently complex, encompassing learning, interaction, transformation, and adaptation. It is marked by characteristics, such as unpredictability, nonlinearity, and involuntariness, as well as its inevitable, dynamic, and continuous nature [3]. A substantial portion of professional competence is cultivated through interpersonal relationships, collaboration, and teamwork within various social and organizational settings [4]. Throughout the lifespan, individuals engage in personal, situational, and institutional interactions influenced by a range of variables—including social status, religious affiliation, gender, and ethnicity [5]—all of which are shaped by the cultural context [6]. The competencies necessary for engagement within professional cultures and effective functioning in social organizations are developed progressively over time through exposure and experience [7, 8]. Cultural intelligence (CQ) refers to an individual’s capability to function and communicate effectively in culturally diverse situations. Unlike other forms of intelligence, CQ enables individuals to display adaptive behaviors and respond appropriately across cultural boundaries [7]. In intercultural contexts—where traditional forms of cognitive, emotional, or social intelligence may be insufficient—CQ acts as a bridge, facilitating both conceptual understanding and behavioral alignment across different cultural frameworks [9]. Importantly, individuals possessing high levels of general intelligence or well-developed social skills may still encounter challenges in intercultural settings if their CQ is underdeveloped [10, 11]. Emotional and social cues, while meaningful in familiar contexts, often fail to translate across divergent cultural systems [12].
In contrast, individuals with elevated CQ can accurately interpret behaviors rooted in unfamiliar cultural norms and adapt accordingly [10, 11]. A substantial body of research has documented significant relationships between CQ and various outcomes, including enhanced social tolerance [13, 14], improved interpersonal interactions [12], career development and mobility [15, 16], and heightened professional competence in nursing and healthcare contexts. Several studies underscore the predictive value of CQ for specific professional behaviors and competencies [16, 17]. In the nursing profession, CQ is increasingly regarded as a critical determinant of healthcare quality, directly contributing to the efficiency and inclusivity of health systems [12]. Attaining global professional competence requires the ability to navigate and manage cultural diversity—one of the key advantages afforded by high CQ [18].
CQ not only helps individuals clarify their career goals and professional paths but also fosters meaningful, effective relationships with people from diverse cultural backgrounds [19]. As nurses enter the workforce as global citizens in increasingly diverse ethnic, cultural, and linguistic environments, adopting new professional identities becomes essential to fostering inclusive, respectful, and high-performing clinical and academic settings [20]. Institutions and organizations operating internationally or within culturally pluralistic societies must regard ethnic, cultural, and social expectations as integral to professional practice [21].
In Iran—a country characterized by considerable cultural diversity, including various ethnicities, climates, religions, dialects, values, and belief systems—such distinctions can significantly affect interpersonal communication and professional performance in healthcare delivery. To address these complex dynamics, this study investigates the relationship between CQ and professional socialization among nursing students at Khoy University of Medical Sciences, Iran.
Methods
Study design
This cross-sectional study was conducted among nursing students at Khoy University of Medical Sciences in April 2024.
Sampling
Questionnaires were distributed to students who met the predefined inclusion criteria. The inclusion criteria included willingness to participate, enrollment as a nursing student, and completion of at least one semester of clinical internship. The exclusion criteria included concurrent employment during academic study, prior academic experience or graduation in another field, participation in CQ or professional socialization training programs, presence of apparent psychiatric disorders, history of psychotropic medication use, and transfer or guest student status during the current semester. Statistical analyses were conducted on 143 fully completed questionnaires that met the inclusion criteria.
Measures and procedures
The sample size was calculated using Cochran’s formula for finite populations. Assuming a 95% confidence level, a 5% margin of error, and maximum variability (P=0.5), the minimum required sample size was estimated at 125. To account for potential non-responses, this number was increased by 20%, resulting in a target sample size of 150 students. Using convenience sampling, the researcher invited 178 eligible students to participate. After obtaining ethical approval and permission to access classes, the researcher attended scheduled class sessions. At the start of each class, the study was briefly introduced to all students, and the study’s purpose, confidentiality, and voluntary nature were clearly explained. Students who met the inclusion criteria and expressed interest in participating were then provided with the questionnaires during the last 15 minutes of the class session. Questionnaires were collected immediately upon completion. Data were collected using a demographic checklist, the CQ questionnaire (CIQ), and the professional socialization questionnaire. A total of 143 fully completed questionnaires were received, exceeding the minimum required sample size and ensuring sufficient statistical power for analysis.
CIQ
The 20-item CIQ was developed by Ang et al. in 2004 and assesses four distinct dimensions of CQ. Items 1–4 evaluate the metacognitive (strategic) component; items 5–11 assess the cognitive (knowledge-based) dimension; items 12–15 measure the motivational aspect; and items 16–20 pertain to the behavioral component. It uses a seven-point Likert scale ranging from “totally disagree” (1) to “totally agree” (7), yielding total score between 20 and 140, with higher scores indicating greater CQ. Scores are calculated by summing all item responses. The CIQ evaluates an individual’s capacity to communicate and function effectively across diverse cultural contexts [22]. The Persian version of this questionnaire was adapted and validated by Ahanchian et al. in 2011. Reliability coefficients (Cronbach’s α) for the subscales were 0.83 (metacognitive), 0.86 (cognitive), 0.85 (motivational), and 0.76 (behavioral) [23]. The instrument’s reliability and validity have also been confirmed in subsequent studies conducted by Ghadampour et al. and Ghaderpanah et al. [24, 25].
Professional socialization questionnaire
The professional socialization questionnaire was developed by Bishive et al. [19] in 2016 and comprises 48 items categorized into four dimensions: professional valuation and recognition (items 1–11), professional skills (items 12–35), management and organizational policies (items 36–45), and interpersonal communication (items 46–48). Respondents rate each item on a five-point Likert scale, where 1 indicates “very little agreement” and 5 indicates “very much agreement”. Total scores range from 48 to 240, with higher values indicating greater professional socialization.
Interpretation of the mean scores in each dimension is as follows: Scores between 0% and 33% are considered low, scores between 34% and 66% are moderate, and scores between 67% and 100% are classified as high. Content validity was established using both quantitative and qualitative methods. The instrument demonstrated strong internal consistency, with a Cronbach’s α coefficient of 0.92 and an intraclass correlation coefficient of 0.94 [19]. The reliability and validity of this questionnaire were further confirmed in a study by Barkhordari et al. [26].
Variables and definitions
The primary outcome variable in this study was professional socialization, assessed using the professional socialization questionnaire. It was developed by Bishive et al. [19]. This instrument consists of 48 items distributed across four dimensions: professional valuation and recognition, professional skills, management and organizational policies, and interpersonal communication.
The primary predictor variable was CQ, measured using the CI scale, which includes four components: Cognitive, metacognitive, motivational, and behavioral.
Potential confounders included age, gender, marital status, and residential status (boarding vs non-boarding); however, no multivariable adjustments were made due to the study’s cross-sectional and correlational design. Effect modification was not evaluated. Since the study did not involve clinical diagnosis, diagnostic criteria were not applicable.
Data analysis
Data analysis was performed using descriptive statistics (including frequency distributions, Mean±SD, independent t-tests to compare two groups (male and female), and one-way analysis of variance (ANOVA) for comparing more than two groups, assuming normal distribution of the data. The Pearson correlation coefficient and linear regression analysis were applied to examine associations between variables. All analyses were conducted using SPSS software, version 20, with statistical significance set at P<0.05.
Results
The results indicated that the mean age of participants was 22.62±1.85 years. Among the 143 participants, 59.5% (n=91) were male, 93.5% (n=134) were single, 63.4% (n=91) lived in urban areas, and 92.2% (n=132) lived in university dormitories (Table 1).
The mean CQ score among nursing students at Khoy University of Medical Sciences, Iran, was 63.88 out of a possible 140. The mean professional socialization score was 110.62 out of a possible 240, indicating a moderate level of professional socialization among the students.
Table 2 presents the results of the Pearson correlation test, which demonstrates a significant positive relationship between CQ and professional socialization among nursing students.
This indicates that higher CQ is associated with increased levels of professional socialization. The relationship between professional socialization and students’ demographic characteristics was examined, revealing significant associations with marital status, gender, and academic grade level Table 3.
Table 4 shows that the coefficient of determination (R²) represents the proportion of variance in professional socialization explained by each dimension of CQ.
The findings indicate that the strategic (metacognitive) dimension explains 21% of the variance; the cognitive (knowledge-based) dimension explains 19%, the motivational dimension 34%, and the behavioral dimension 23%. Among these, motivational factors showed the strongest predictive power (R²=0.34, β=0.47, P=0.001), while cognitive factors had the weakest predictive effect (R²=0.19, β=0.29, P=0.020).
Discussion
This study examined the relationship between CQ and professional socialization among nursing students at Khoy University of Medical Sciences, Iran. The results indicated that the participating nursing students demonstrated a moderate level of CQ, and that CQ was not significantly associated with any of the examined demographic characteristics. In this context, Hassani and colleagues, in a study conducted in Iran, reported that the average CQ score among university students ranged from weak to moderate [27]. Ahanchian et al. [23] found that Iranian nurses demonstrated average levels of CQ. Consistent with these findings, Göl et al. in a study conducted in Turkey, reported that undergraduate nursing students exhibited an average level of CQ [28]. In contrast, Abouelenein and Mostafa Mohamed, in a study conducted in Egypt, found that 76.6% of nursing students demonstrated high levels of CQ, and no significant associations were observed between CQ and demographic characteristics [29]. Given these findings, nursing students are encouraged to enter their future professional roles with emotional composure and to communicate effectively with colleagues in a manner that avoids discomfort or misunderstanding. Therefore, implementing an appropriately designed educational program may enhance students’ capacity to recognize and respect cultural diversity.
This study revealed that the average professional socialization score among the participating nursing students was low, and professional socialization was found to be significantly associated with both gender and marital status. Most previous studies on professional socialization have reported average levels of professional socialization among nursing students. For example, a study by Ghaderpanah in Iran indicated that 93% of nursing students scored in the low to average range of professional socialization [25]. Barkhordari’s research reported average professional socialization scores among nursing students [26]. In Sanandaj, Zandi et al. found that most nurses exhibited a moderate level of professional socialization, which aligns with the findings of the present study [30]. However, findings by Noohi et al. demonstrated high levels of professional socialization among undergraduate nursing students [31]. Professional socialization during undergraduate nursing education is a critical component in training clinically competent practitioners and serves as the foundation through which novice nurses acquire essential research skills, critical thinking, and reasoning abilities [32]. When organizational and professional socialization processes are effectively implemented, they foster greater organizational commitment, which is a key factor in enhancing efficiency and performance within healthcare settings [25]. Therefore, promoting and strengthening professional socialization among nursing students is imperative to optimize their professional development and improving their future clinical competence.
The findings support the primary objective of the study, revealing a significant positive association between CQ and professional socialization among nursing students—higher levels of CQ were linked to stronger professional socialization. Among the four dimensions, the motivational component explained the largest proportion of variance (34%), followed by the behavioral (23%), strategic (21%), and cognitive (19%) dimensions. This underscores the central role of motivation in shaping professional identity and suggests that interventions aimed at enhancing professional socialization in multicultural or organizational settings should prioritize strategies that foster cultural motivation, such as promoting intercultural curiosity and self-efficacy.
Although research explicitly investigating the relationship between CQ and professional socialization within educational contexts remains limited, findings from related studies offer empirical support for these results. For example, Bahaadini et al. reported that nurses with higher levels of CQ also exhibited stronger scores in social interaction [12], while those with elevated CQ demonstrated greater professional competencies [33]. In a separate study, Beheshti et al. found that CQ accounted for approximately 12% of the variance in social tolerance among citizens [13]. A subsequent investigation by the same researcher, focusing on the Baloch population, reported that CQ explained roughly 26% of the variance in social tolerance [14]. These findings suggest that individuals who are more adept at navigating culturally diverse environments and who display a higher degree of openness toward individuals with differing characteristics are more likely to demonstrate increased tolerance and adaptability in social interactions [13, 14].
Numerous studies conducted across diverse populations have identified significant associations between CQ and various psychosocial constructs, including interpersonal communication, organizational citizenship behavior among teachers [33], organizational sociability in newly recruited industrial employees [34], auditors’ social responsibility [35], social identity among students of educational sciences [33], social perspective-taking in professional settings [36], and adaptive performance among nurses [37]. CQ endows medical students with the capacity to function effectively in multicultural clinical environments. Empirical evidence has shown that higher levels of CQ are positively associated with enhanced interpersonal interactions among healthcare professionals—an essential factor in promoting collaboration in culturally diverse healthcare teams [12, 38].
The ability to identify and appreciate cultural differences strengthens communicative competence and enables nursing students to engage more effectively with patients from various sociocultural backgrounds. This form of cultural adaptation contributes not only to individual development but also to the advancement of institutional goals by fostering a more cohesive, respectful, and inclusive workplace [27]. Furthermore, culturally intelligent managers consistently demonstrate superior interpersonal competence when interacting with individuals from dissimilar cultural backgrounds, enhancing their effectiveness in fulfilling professional roles [39].
Therefore, the integration of CQ into nursing curricula is essential for fostering effective interprofessional collaboration within healthcare teams. Given that nurses often serve as the primary point of contact for patients, their ability to communicate across cultural boundaries is fundamental to ensuring both patient safety and satisfaction [40]. Empirical studies have shown that culturally competent nurses are more adept at navigating intercultural interactions, enhancing teamwork and collaboration in clinical environments. This competency is critical in response to the increasing cultural heterogeneity of patient populations, which necessitates a healthcare workforce capable of delivering nuanced and culturally congruent care [16].
Among the dimensions of CQ, cultural sensitivity is especially influential in shaping patient satisfaction and clinical outcomes. Research has demonstrated that patients report greater satisfaction when cultural considerations are acknowledged and integrated into their individualized care plans [38, 40]. Such culturally attuned care not only improves patient satisfaction but also enhances treatment efficacy by aligning care strategies with patients’ values, preferences, and cultural norms. For instance, culturally sensitive approaches have been shown to increase adherence to medical recommendations among individuals from diverse backgrounds, contributing to better overall health outcomes [27].
Given the well-established benefits of CQ in nursing and medical education, it is essential to prioritize its integration into curriculum design. Embedding cross-cultural nursing content within educational frameworks can substantially enhance students’ cultural competence and better equip them to navigate the complexities of today’s diverse healthcare environments. Innovative pedagogical approaches that emphasize experiential learning—such as simulation-based training involving culturally varied patient scenarios—have the potential to improve students’ self-efficacy and confidence, reinforcing their ability to deliver culturally responsive and patient-centered care [16].
Conclusion
This study found that nursing students possess a moderate level of CQ, which is significantly associated with higher levels of professional socialization. This suggests that CQ plays a key role in helping students internalize professional values, behaviors, and responsibilities. As such, enhancing CQ should be a priority in nursing education. Incorporating intercultural training and reflective practice into the curriculum may effectively support this goal. Future research should explore evidence-based strategies for integrating CQ into health professions education to better prepare graduates for diverse clinical environments.
Limitations and recommendations
The cross-sectional design of this study inherently limits the ability to infer causal relationships, restricting the findings to associations between variables and precluding definitive conclusions about whether CQ influences professional socialization or vice versa. Data collection relied on self-report questionnaires, which are vulnerable to social desirability and other response biases. Although measures were taken to minimize these biases—such as guaranteeing participant confidentiality and stressing the importance of honest responses—the potential for bias remains and may have affected the results in either direction. While the study controlled for certain demographic factors by excluding participants with prior work experience, previous education in unrelated fields, or concurrent hospital employment, other influential variables were not accounted for. These include personality traits, family background, social support systems, prior experiences, and exposure to diverse ethnic groups within familial or community contexts, all of which may impact CQ or professional socialization beyond the scope of this research. The sample was limited to nursing students at Khoy University of Medical Sciences, restricting the generalizability of the findings to the broader nursing student population. Accordingly, the results should be interpreted with caution. Future studies employing longitudinal designs and larger, more heterogeneous samples are recommended to better clarify the temporal relationship and causal dynamics between CQ and professional socialization.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Khoy University of Medical Sciences, Khoy, Iran (Code: IR.KHOY.REC.1402.044).
Funding
This study was financially supported by Khoy University of Medical Sciences, Khoy, Iran.
Authors' contributions
Conceptualization, study design, and supervision: Zeinab Habibpour and Roghieh Sodeify; Data collection: Masoud Omiya; Data analysis: Mehdi Mokhtari; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank all the nursing students who participated in this study. They also express their appreciation to the Research Vice Chancellor of Khoy University of Medical Sciences for providing financial and administrative support.
Reference
- Grusec JE, Hastings PD. Handbook of socialization: Theory and research. New York: Guilford Publications; 2014. [link]
- Dinmohammadi M, Peyrovi H, Mehrdad N. Concept analysis of professional socialization in nursing. Nursing Forum. 2013; 48(1):26-34. [DOI:10.1111/nuf.12006] [PMID]
- Shinyashiki GT, Mendes IAC, Trevizan MA, Day RA. Professional socialization: students becoming nurses. Revista Latino-Americana de Enfermagem. 2006; 14(4):601-7. [DOI: 10.1590/s0104-11692006000400019] [PMID]
- Mirzaeyan S, Tahmasebi S. Influencing factors of professional socialization of clinical nurses. Journal of Clinical Nursing and Midwifery. 2016; 5(1):76-86. [Link]
- Price SL. Becoming a nurse: A meta‐study of early professional socialization and career choice in nursing. Journal of Advanced Nursing. 2009; 65(1):11-9. [DOI:10.1111/j.1365-2648.2008.04839.x] [PMID]
- Lawson B, Petersen KJ, Cousins PD, Handfield RB. Knowledge sharing in interorganizational product development teams: The effect of formal and informal socialization mechanisms. Journal of Product Innovation Management. 2009; 26(2):156-72. [DOI:10.1111/j.1540-5885.2009.00343.x]
- Devenish A, Clark M, Fleming M. Experiences in becoming a paramedic: the professional socialization of university qualified paramedics. Creative Education. 2016; 7(6):786-801.[DOI:10.4236/ce.2016.76081]
- Van Dyne L, Ang S, Livermore D. Cultural intelligence: A pathway for leading in a rapidly globalizing world. In: Hannum K, McFeeters BB, Booysen L, editors. Leading across differences: casebook. New Jersey: John Wiley & Sons; 2010. [Link]
- Barzykowski K, Majda A, Szkup M, Przyłęcki P. The Polish version of the cultural intelligence scale: Assessment of its reliability and validity among healthcare professionals and medical faculty students. Plos One. 2019; 14(11):e0225240.[DOI:10.1371/journal.pone.0225240] [PMID]
- Bücker JJ, Furrer O, Poutsma E, Buyens D. The impact of cultural intelligence on communication effectiveness, job satisfaction and anxiety for Chinese host country managers working for foreign multinationals. The International Journal of Human Resource Management. 2014; 25(14):2068-87. [DOI:10.1080/09585192.2013.870293]
- Moshabaki A, Tizro A. Emotional and cultural intelligences factors of global leadership success. Commercial Strategies. 2020; 8(44):237-50. [Link]
- Bahaadini F, Rashidinejad M, Jahani Y, Eghbali T. Cultural intelligence in nurses: Relationship with social interaction. Iranian Journal of Culture and Health Promotion. 2021; 5(2):228-36. [Link]
- Beheshti S. R. Sociological explanation of social tolerance and its dimensions among Iranian ethnic groups. Social Issues of Iran. 2011; 2(4)35-47. [Link]
- Beheshti S, Naraghimanesh M, Naraghimanesh S. Sociological explanation of the relationship between cultural intelligence and social tolerance among Baloch people. Strategic Researches of Social Issues. 2023; 12(4):101-22. [DOI:10.22108/srspi.2024.140473.1968]
- Agili, BS. [Investigating the relationship between cultural intelligence and organizational culture with the career path of education workers in Bandar Turkmen city (Persian)]. New Developments in Psychology, Educational Sciences and Education. 2022; 49(5):411-34. [Link]
- Rahimaghaee F, Mozdbar R. Cultural intelligence and its relation with professional competency in nurses. Nursing Practice Today. 2017; 4(3):115-24. [Link]
- Atalla ADG, Elseesy NA. Cultural Intelligence and professional competencies among nurses: A cross-sectional study. Alexandria Scientific Nursing Journal. 2023; 25(1):151-64.[DOI:10.21608/asalexu.2023.300022]
- Rand I. Cultural intelligence: The essential intelligence for the 21st century. Alexandria: Shrm Foundation; 2015. [Link]
- Bishive MS, Mousavi S, Majde TZ, Ghanbzri KA, Kazemnazhad LE. [Survey of nursing students professional socialization in the Guilan university of medical sciences (Persian)]. Journal of Holistic Nursing and Midwifery. 2016; 25(80):19-28. [Link]
- Galan-Lominchar M, Roque IM, Cazallas CDC, Mcalpin R, Fernández-Ayuso D, Ribeiro AS. Nursing students' internationalization: Virtual exchange and clinical simulation impact cultural intelligence. Nursing Outlook. 2024; 72(2):102137. [DOI:10.1016/j.outlook.2024.102137] [PMID]
- Sharma N, Hussain D. Dynamics of social identity and cultural intelligence in acculturative adaptation of an ethnic minority group in India. Analyses of Social Issues and Public Policy. 2021; 21(1):453-70. [DOI:10.1111/asap.12225]
- Ang S, Van Dyne L, Koh C, Ng K. The measurement of cultural intelligence. In 2004 Academy of Management Meetings Symposium on Cultural Intelligence in the 21st Century. New Orleans. [Link]
- Ahanchian MR, Amiri R, Bakhshi M. [Correlation between cultural intelligence and social interaction of nurses (Persian)]. Journal of health promotion management. 2012; 1(2):44-53. [Link]
- Ghadampour E, Mehrdad. H, Jafari H. [Investigating the relationship between personality traits and cultural intelligence of employees of cultural heritage, handicrafts and tourism organization of Lorestan province (Persian)]. Educational Psychology. 2011; 2(1):101-81. [Link]
- Ghaderpanah A, Ajudani F, Ghasemzadeh N. [Investigating the level of socialization and professional identity of nursing students in Urmia University of Medical Sciences (Persian)]. Nursing and Midwifery Journal. 2023; 21(11):887-97. [DOI:10.61186/unmf.21.11.887]
- Barkhordari-Sharifabad M, Mortazavi A. Professional socialization of nursing students and its relationship with self-esteem. Journal of Medical Education. 2021; 20(3):e118118. [DOI:10.5812/jme.118118]
- Hassani F. Effect of cultural intelligence on self-directed learning of nursing students. Bimonthly of Education Strategies in Medical Sciences. 2015; 8(2):115-22. [Link]
- Göl İ, Erkin Ö. Association between cultural intelligence and cultural sensitivity in nursing students: A cross-sectional descriptive study. Collegian. 2019; 26(4):485-91. [DOI:10.1016/j.colegn.2018.12.007]
- Aboelenein S, Mohamed SM. Study the relationship between cultural intelligence and academic vitality with self-directed learning among nursing students. International Egyptian Journal of Nursing Sciences and Research. 2022; 2(2):133-48. [Link]
- Ghanbari# S, Zandi K, Amani S. The relationship between organizational socialization and organizational indifference in nurses. Quarterly Journal of Nursing Management. 2018; 6(3):9-16. [Link]
- Noohi E, Ildarabadi E, Fakhrbarati M. Relationship between professional confidence and professional socialization among nursing students: A cross-sectional study. La Prensa Medica Argentina. 2020; b106(5). [DOI:10.47275/0032-745X-231]
- Shin H, Sok S, Hyun KS, Kim MJ. Competency and an active learning program in undergraduate nursing education. Journal of Advanced Nursing. 2015; 71(3):591-8. [DOI: 10.1111/jan.12564] [PMID]
- Atalla ADG, Mahmoud Elseesy NA, El-Ashry AM, Sharif LS, Mahsoon A, Aljohani WF, et al. Unraveling the synergy: How organizational intelligence fuel soft skills and nurses’ thriving: A cross-sectional study. BMC Nursing. 2024; 23(1):315. [DOI:10.1186/s12912-024-01933-w] [PMID]
- Alifuddin M, Widodo W. How is cultural intelligence related to human behavior? Journal of Intelligence. 2022; 10(1):3.[DOI:10.3390/jintelligence10010003] [PMID]
- Momeni S, Poorzamani Z. [Assessing the relationship between auditors’,cultural intelligence and social responsibility: A psychological model using structural equations (Persian)]. Journal of Financial and Behavioral Researches in Accounting. 2022; 2(3):38-68. [Link]
- Faghieh Aram B, Moeadi S, Kazemi M. [The relationship between cultural intelligence and spiritual intelligence with students’ social identity (Persian)]. Journal of Islamic Perspective on Educational Science. 2019; 6(11):129-50. [Link]
- Ibrahim Mahmoud S, Ali Hassan H, Marzouk Amer S. Relation between Nurses’ cultural intelligence and adaptive performance. Egyptian Journal of Health Care. 2022; 13(4):1922-37. [DOI:10.21608/ejhc.2022.338895]
- Bakhtiari Z, Hanifi N, Varjoshani NJ. The relationship between cultural intelligence and cultural competence of students of nursing and midwifery during COVID-19: A cross-sectional study. Journal of Medical Education and Curricular Development. 2023; 10:23821205231184042. [DOI: 10.1177/23821205231184042] [PMID]
- Jyoti J, Kour S. Assessing the cultural intelligence and task performance equation: Mediating role of cultural adjustment. Cross Cultural Management. 2015; 22(2):236-58. [DOI:10.1108/CCM-04-2013-0072]
- Ličen S, Prosen M. The development of cultural competences in nursing students and their significance in shaping the future work environment: A pilot study. BMC Medical Education. 2023; 23(1):819. [DOI:10.1186/s12909-023-04800-5] [PMID]
Type of Study: Orginal Article |
Subject:
● Health Systems
Received: 2024/12/11 | Accepted: 2025/09/20 | Published: 2026/03/14
Received: 2024/12/11 | Accepted: 2025/09/20 | Published: 2026/03/14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
