

Volume 15, Issue 6 (Nov & Dec 2025)
J Research Health 2025, 15(6): 603-614 |
Back to browse issues page


Ethics code: IR.MODARES.REC.1402.001
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bagheri Sheykhangafshe F, Savabi Niri V, Azizrousta S, Allahzade M, Farahani H. The Efficacy of Acceptance and Commitment Therapy on Internalized Shame, Fear of Success, and Anxiety Sensitivity in Nursing With Imposter. J Research Health 2025; 15 (6) :603-614
URL: http://jrh.gmu.ac.ir/article-1-2716-en.html
URL: http://jrh.gmu.ac.ir/article-1-2716-en.html
Farzin Bagheri Sheykhangafshe1 

 , Vahid Savabi Niri2 , Saba Azizrousta2 , Mohadese Allahzade3 , Hojjatollah Farahani4
, Vahid Savabi Niri2 , Saba Azizrousta2 , Mohadese Allahzade3 , Hojjatollah Farahani4
, Vahid Savabi Niri2 , Saba Azizrousta2 , Mohadese Allahzade3 , Hojjatollah Farahani4
1- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran. , farzinbagheri73@gmail.com
2- Department of Clinical Psychology, Faculty of Humanities, Ardabil Branch, Islamic Azad University, Ardabil, Iran.
3- Department of Psychology, Faculty of Psychology and Education Science, Semnan University, Semnan, Iran.
4- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran.
2- Department of Clinical Psychology, Faculty of Humanities, Ardabil Branch, Islamic Azad University, Ardabil, Iran.
3- Department of Psychology, Faculty of Psychology and Education Science, Semnan University, Semnan, Iran.
4- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran.
Full-Text [PDF 679 kb]
(828 Downloads)
| Abstract (HTML) (2639 Views)
Full-Text: (713 Views)
Introduction
Becoming a nurse is often rewarding and challenging, requiring students to master complex skills, navigate demanding academic expectations, and develop the emotional resilience necessary for patient care [1]. However, for many nursing students, the pressures of these experiences can be compounded by the psychological phenomenon known as the imposter phenomenon (IP) [2]. First identified by clinical psychologists Clance and Imes in the 1970s, IP describes feelings of self-doubt, inadequacy, and the persistent belief that one’s successes are undeserved or the result of luck rather than competence [3]. Despite their accomplishments, individuals with IP often fear being exposed as frauds, leading to heightened stress, anxiety, and self-criticism. Among nursing students, the prevalence of the IP is particularly concerning [4]. These students are not only transitioning into professional roles that demand high levels of responsibility and expertise but are also navigating environments where their actions directly impact patient outcomes [5]. El-Ashry et al. [2] highlighted that a significant proportion of nursing students experienced moderate to severe levels of depression, anxiety, and stress, with 46.3% reporting moderate levels of IP. They also found a positive correlation between IP and depression, anxiety, and stress.
Internalized shame and IP are deeply interrelated constructs that can profoundly influence an individual’s sense of self and ability to thrive in personal and professional settings [6]. Internalized shame refers to the pervasive, often unconscious, belief that one is fundamentally flawed, unworthy, or inadequate [7]. This self-perception, shaped by experiences of criticism, rejection, or societal expectations, often manifests as persistent self-judgment and feelings of inferiority [8]. The interplay between internalized shame and IP is particularly significant because both reinforce cycles of self-doubt and emotional distress [9]. Internalized shame lays the groundwork for the feelings of inadequacy central to IP. At the same time, the experience of IP perpetuates shame by framing successes as unearned and failures as confirmations of inherent worthlessness [10]. Overall, these dynamics can erode self-confidence, hinder personal growth, and limit professional advancement, creating significant barriers to well-being [11].
Success is often celebrated as a desirable goal, yet for many individuals, it can also evoke complex emotions, such as fear, self-doubt, and anxiety [12]. The fear of success—a psychological phenomenon characterized by apprehension about the consequences of achievement—can manifest in behaviors that undermine personal and professional growth [13]. When coupled with IP, these fears become even more pronounced. The fear of success often stems from concerns about heightened expectations, increased visibility, or peer alienation [14]. For those with the IP, these concerns are amplified by a fundamental disbelief in their capabilities [15]. Success becomes a paradoxical experience; while it validates their achievements externally, it intensifies their internal doubts and fears of being found out [16]. This dynamic can lead to self-sabotage, hesitation to pursue opportunities, and a reluctance to acknowledge or celebrate accomplishments [17].
Anxiety sensitivity, the fear of anxiety-related sensations due to beliefs that they signal harmful physical, cognitive, or social outcomes, plays a significant role in amplifying the experience of IP [18]. For individuals with high anxiety sensitivity, the physiological and emotional responses associated with stress—such as rapid heartbeat, difficulty concentrating, or feelings of inadequacy—are not only uncomfortable but also interpreted as confirmation of their perceived incompetence [19]. The interplay between anxiety sensitivity and IP creates a feedback loop that heightens self-doubt and emotional distress [20]. Individuals who are highly sensitive to the physical and cognitive symptoms of anxiety may interpret these sensations as evidence that they are incapable of meeting expectations or unworthy of their achievements [21]. This self-perception reinforces the imposter belief system, leading to avoidance behaviors, overcompensation, or burnout, as individuals attempt to mask their internal struggles [22].
While traditional approaches to addressing IP focus on challenging distorted thoughts or boosting self-esteem, acceptance and commitment therapy (ACT) offers a novel approach that shifts the focus from thought correction to acceptance and value-driven action [23]. ACT is grounded in the principles of psychological flexibility, mindfulness, and value clarification [24]. Rather than disputing the negative thoughts and feelings that fuel IP, ACT helps individuals develop a new relationship with these experiences [25]. By fostering acceptance, individuals learn to view imposter-related thoughts as transient mental events rather than truths [26]. Through mindfulness, they become more present in the moment, reducing the grip of self-critical rumination [27]. Furthermore, ACT encourages individuals to define their core values—what truly matters to them—and to commit to actions aligned with those values, even in the presence of self-doubt or anxiety [28]. The application of ACT to the IP is especially promising because it equips individuals with tools to break free from the cycle of avoidance and self-criticism that often characterizes IP [29]. By accepting the presence of uncomfortable thoughts and emotions, individuals can redirect their energy toward meaningful goals, fostering both resilience and authenticity [30]. This introduction delves into the role of ACT in addressing IP, emphasizing its potential to promote long-term psychological well-being and a more balanced sense of self-worth [31]. Through this lens, IP is not seen as a barrier to success but as an experience that can be managed and contextualized, empowering individuals to lead values-driven lives [32].
Ong et al. [33] examined the impact of ACT on clinical perfectionism, which is characterized by a rigid adherence to excessively high standards often associated with self-doubt and IP. Their study found that ACT significantly reduced perfectionism, psychological distress, and functional impairment, suggesting that targeting core maladaptive processes—rather than focusing solely on symptom relief—can lead to meaningful improvements in self-efficacy and resilience. Wood et al. [34] conducted a case study on a competitive figure skater with autism who experienced low self-confidence and performance anxiety. Over 25 ACT-based intervention sessions, the athlete learned to accept unhelpful thoughts rather than struggle against them, leading to increased psychological flexibility, reduced self-imposed pressure, and improved self-efficacy. The intervention successfully mitigated self-doubt and perfectionistic tendencies, contributing to greater confidence in training and competition.
French et al. [35] conducted a meta-analysis on ACT self-help interventions, revealing significant reductions in anxiety, depression, and psychological inflexibility. Their findings indicate that ACT fosters psychological flexibility, which in turn decreases self-doubt and feelings of fraudulence associated with IP. Notably, greater improvements were observed when clinician guidance was provided, reinforcing ACT’s effectiveness in addressing perfectionism and enhancing self-confidence. Collectively, these studies support ACT as an effective intervention in reducing perfectionistic concerns, alleviating self-doubt, and mitigating IP. By fostering acceptance, mindfulness, and value-driven actions, ACT promotes greater psychological resilience and self-efficacy, making it a valuable approach for individuals struggling with maladaptive self-perceptions and performance-related anxiety.
This study aimed to comprehensively evaluate the effectiveness of ACT in addressing internalized shame, fear of success, and anxiety sensitivity among nursing students experiencing IP. Given the high-pressure academic and clinical environments that nursing students navigate, these psychological burdens can significantly impact their confidence, professional identity, and overall well-being. This study sought to determine whether ACT, by promoting psychological flexibility, mindfulness, and value-driven actions, can effectively mitigate these challenges and foster greater emotional resilience. Specifically, this research examined how ACT reduces the psychological distress associated with these constructs and whether its mechanisms—such as cognitive defusion, acceptance, and self-compassion—help students break free from self-doubt and self-criticism. By bridging the gap between traditional cognitive approaches and mindfulness-based interventions, this study contributes to the expanding body of research exploring ACT as a novel and evidence-based intervention for IP. Furthermore, it aimed to provide empirical support for integrating ACT into nursing education and mental health interventions, offering a structured approach to enhancing students’ coping strategies, self-efficacy, and professional confidence. If successful, the findings could inform the development of targeted interventions tailored to the specific needs of nursing students, ultimately improving their mental well-being, academic performance, and readiness for the demands of the healthcare profession. By addressing these psychological barriers early in their training, this study has the potential to contribute to long-term improvements in both personal and professional outcomes for future nursing professionals.
Methods
Study design
This study utilized a parallel-group randomized controlled trial (RCT) design with pre-test and post-test measurements, including a control group. Allocation concealment was ensured by using a computer-generated randomization sequence, which was performed by an independent researcher who was not involved in participant recruitment or intervention delivery.
Participants
The statistical population comprised nursing students residing in Districts 7 and 8 of Tehran from September to November 2023. From an initial pool of 36 eligible students, randomized block sampling was applied to ensure balanced group allocation, resulting in 18 participants in the experimental group and 18 in the control group. Randomization was conducted using a stratified approach, accounting for gender and academic performance to minimize selection bias. The sample size calculation was performed using G*Power software, version 3.1, with an effect size of 1.53, a power (1−β) of 0.97, and an alpha of 0.05, based on prior studies.
The effect size selection was informed by previous clinical trials and meta-analyses on ACT interventions for psychological distress in student populations. The practical significance of this effect size suggests a substantial reduction in imposter syndrome symptoms through ACT.
Inclusion criteria: A score greater than 45 on the IP scale; age range of 18–30 years (to ensure population homogeneity and developmental relevance); written informed consent (an ethical requirement rather than a selection criterion); absence of psychiatric medication usage (to control for pharmacological influences on psychological symptoms).
Exclusion criteria: Failure to respond to more than 10% of questionnaire items (to maintain data integrity); a significant increase in stress levels, defined as a ≥1.5 standard deviation (SD) increase in perceived stress scale scores; missing more than two ACT sessions (to ensure intervention adherence).
Tools/Instruments
Imposter syndrome scale (ISS): The ISS was originally developed by Clance and Imes [3]. The scale consists of 20 items, where participants indicate their level of agreement with each statement on a five-point Likert scale ranging from “never” to “very much.” Based on the total score, levels of imposter syndrome are categorized as follows: A score of less than 40 indicates weak imposter syndrome, 41–60 indicates moderate imposter syndrome, 61–80 indicates pathological imposter syndrome, and a score above 80 signifies severe imposter syndrome. Studies have reported high internal consistency for the ISS, with Cronbach’s α coefficients ranging from 0.85 to 0.94 [3]. Additionally, its validity and reliability were found to be satisfactory among Iranian students, with a reported Cronbach’s α of 0.86 [36]. In the present study, the reliability of the scale was also confirmed, with a Cronbach’s α coefficient of 0.82.
Internalized shame scale (ISS): The ISS was developed by Cook [37] to measure the degree of internalized shame experienced by individuals. This scale consists of 30 items, scored on a five-point Likert scale ranging from 1 (“never”) to 5 (“always”), with total scores ranging from 30 to 150. Higher scores indicate greater levels of internalized shame. The ISS assesses the respondent’s feelings of personal value, self-adequacy, and the tendency to experience shame in social and personal contexts. Cook [37] reported high reliability for the ISS, with Cronbach’s α coefficients ranging from 0.84 to 0.97, reflecting its strong psychometric properties. Additionally, Jafari et al. [38] confirmed the validity and reliability of the scale in Iran, reporting a Cronbach’s α of 0.89. In the present study, the reliability of the ISS was also confirmed, with a Cronbach’s α coefficient of 0.85, supporting its continued use in diverse populations.
Fear of success scale (FOSS): The FOSS was developed in 1979 by Zuckerman and Allison to assess the extent of an individual’s fear of achieving success [39]. This fear is conceptualized as a learned personality trait rooted in early life experiences, reflecting a stable motivation to avoid success due to negative perceptions and anticipated consequences of achievement. According to Atkinson, fear of success represents a personal inclination based on the belief that success might lead to real or predicted negative outcomes. The FOSS consists of 27 items, scored on a seven-point Likert scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”), with total scores ranging from 27 to 189. Higher scores indicate a greater fear of success. In the original study, the FOSS demonstrated strong psychometric properties, with reported reliability (Cronbach’s α) ranging between 0.82 and 0.88 and good content and construct validity, supporting its use as a reliable measure of fear of success [39]. Additionally, Ashrafifard and Mafakheri [40] reported satisfactory validity and reliability for the scale in Iran, with a Cronbach’s α coefficient of 0.83. In the present study, the reliability of the scale was also confirmed, with a Cronbach’s α coefficient of 0.84, supporting its use as a reliable measure of fear of success.
Anxiety sensitivity index-3 (ASI-3): The ASI-3 measures the level of worry related to various symptoms of anxiety [41]. Derived from the revised ASI-3, this scale comprises 18 items and evaluates anxiety sensitivity across three dimensions: physical concerns (6 items), cognitive concerns (6 items), and social concerns (6 items). It is scored on a five-point Likert scale ranging from 0 (“very little agree”) to 4 (“completely agree”), with total scores ranging from 0 to 72. The ASI-3 demonstrates strong psychometric properties, with internal consistency coefficients ranging between 0.76 and 0.86 for physical concerns, 0.79 and 0.91 for cognitive concerns, and 0.73 and 0.86 for social concerns. Additionally, the scale has shown good convergent and divergent validity [41]. In Iran, Cronbach’s α coefficients for the physical, cognitive, and social subscales were reported as 0.89, 0.84, and 0.80, respectively [42]. In the present study, the internal consistency for the subscales was also confirmed, with Cronbach’s α coefficients ranging from 0.81 to 0.85.
Data collection
Data collection involved a pre-test and post-test evaluation using validated scales, including the ISS, ISS, FOSS, and ASI-3. The experimental group underwent eight 90-minute ACT sessions over eight weeks, while the control group received no intervention. Pre-test assessments established baseline levels for all variables, and post-test evaluations measured changes following the intervention.
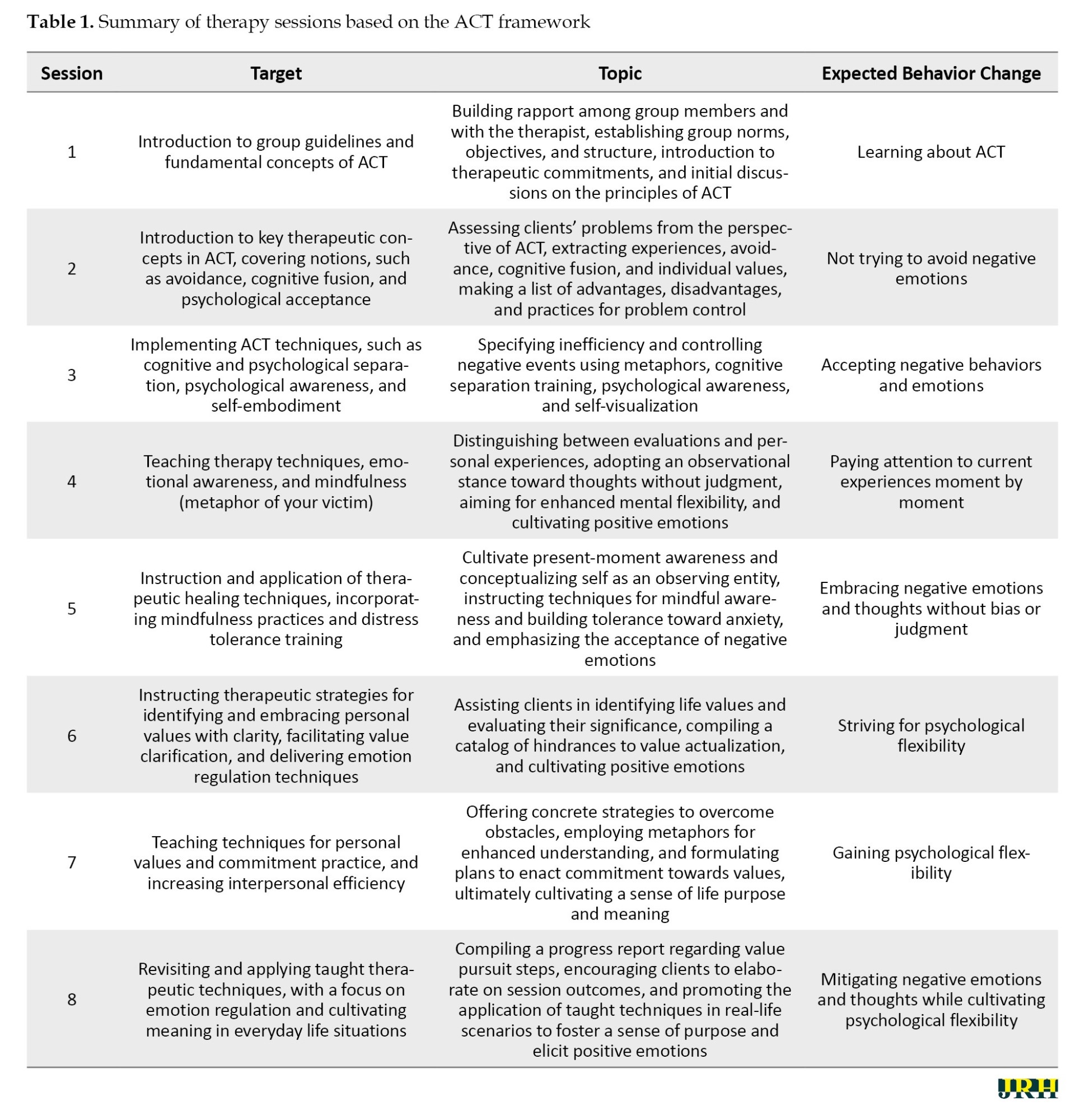
ACT sessions by a therapist in the psychology clinic were then performed in eight 90-minute weekly group sessions for the experimental group, while the control group did not receive any intervention. ACT was designed based on the ACT programs proposed by Hayes et al. [43] and also taking into account the key characteristics in the design of ACT programs (Table 1).
Data analysis
To analyze the research data, descriptive statistics (Mean±SD) and covariance analysis were used based on their assumptions using SPSS software, version 27. The significance level of these tests was considered 0.05. The Shapiro-Wilk test checked the normality of the distribution of variables in the two groups, and its result was not significant for all variables. Therefore, it can be concluded that the distribution of variables was normal (P>0.05).
Results
The mean age of participants in the intervention group was 24.38±6.07 years, while in the control group, it was 24.89±5.69 years. In terms of demographics, 65% were female, 48% were married, and 53% held a bachelor’s degree. Additionally, 66% of participants had experienced IP for two years.
A chi-square test was used to compare the intervention and control groups in terms of age, gender, marital status, educational level, and duration of IP. The results showed no significant differences between the two groups (χ²=3.24, P=0.518), indicating that the groups were statistically equivalent at baseline. This lack of significant difference suggests that any observed effects in the study are more likely attributed to the intervention rather than pre-existing demographic variations. Additionally, an independent t-test confirmed that there was no significant difference in age between the groups (t=0.72, P=0.476), supporting the assumption that the groups were well-matched. By ensuring demographic equivalence, these results strengthen the validity of subsequent analyses by minimizing the risk of confounding variables influencing the outcomes.
Table 2 presents the Mean±SD of pre-test and post-test scores for internalized shame, fear of success, and anxiety sensitivity among nursing students with IP in the experimental and control groups.
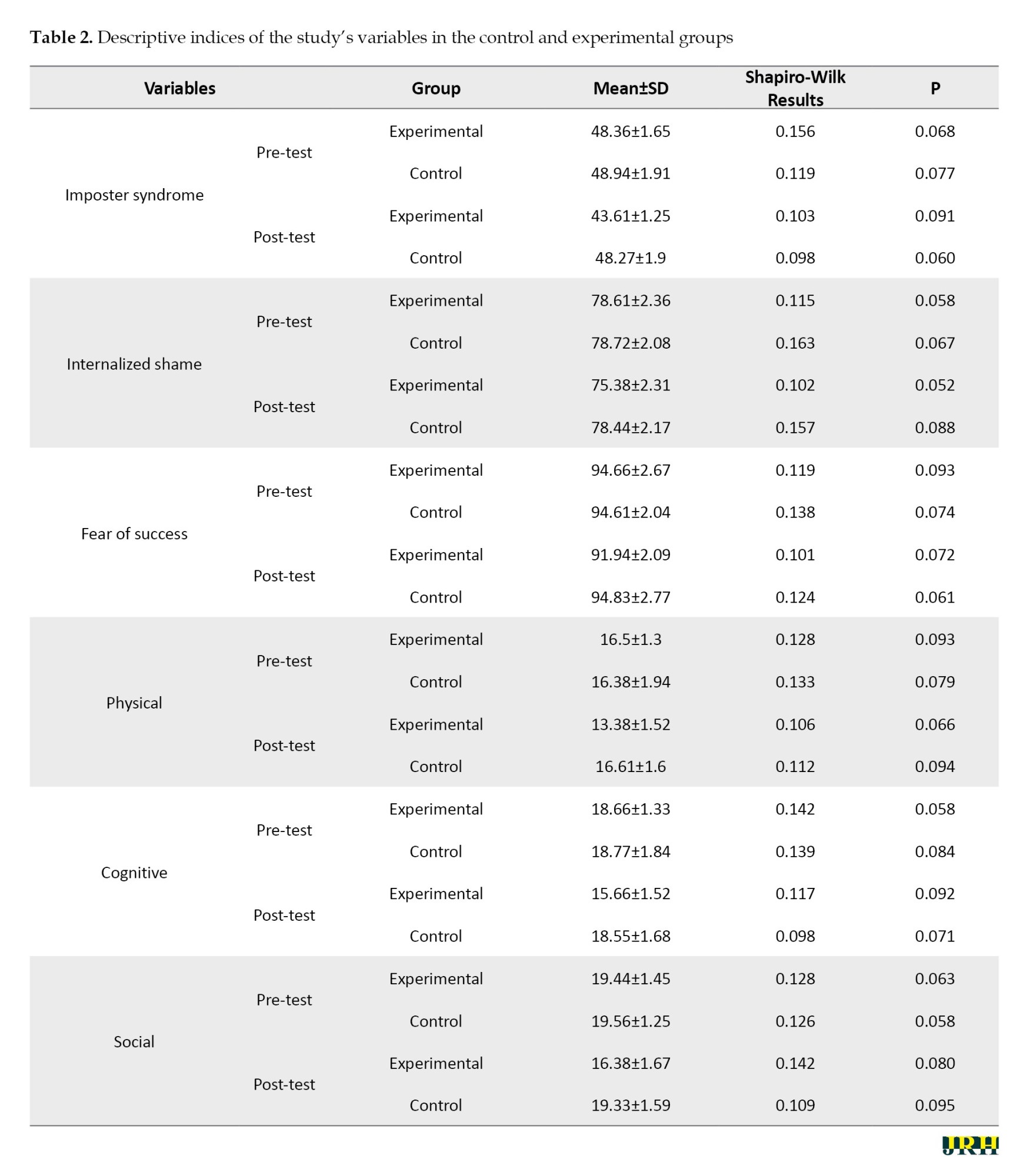
Additionally, the results of the Shapiro-Wilk test for normality are included. The table indicates that none of the variables showed significant deviations based on the Shapiro-Wilk test, suggesting that the distribution of variables in both groups is normal (Table 2).
Multivariate analysis of covariance (MANCOVA) was employed to assess the effect of ACT on internalized shame, fear of success, and anxiety sensitivity in nursing students with IP. The results of Levene’s test, used to evaluate the homogeneity of variance among the dependent variables across groups, indicated that variances were equal for internalized shame (F=4.1, P=0.051), fear of success (F=2.81, P=0.102), and anxiety sensitivity (F=1.83, P=0.187). Additionally, Box’s test, conducted to assess the equality of the covariance matrix of dependent variables between the experimental and control groups, confirmed that the covariance matrices were equal (Box M=18.89, F=1.05, P=0.391).
The chi-square Bartlett test, used to evaluate sphericity or the significance of relationships among internalized shame, fear of success, and anxiety sensitivity, revealed a significant relationship between the variables (χ2=124.77, df=14, P<0.01). Another critical assumption for conducting MANCOVA is the homogeneity of regression slopes. This was assessed by examining the interaction between the dependent variables and the independent variable (intervention method) across pre-test and post-test scores. The interaction results indicated that the regression slopes were homogeneous, as these interactions were not significant. Therefore, this assumption was also satisfied. Since all necessary assumptions for conducting MANCOVA were met, the test was deemed appropriate. Subsequently, MANCOVA was performed to identify the differences between the experimental and control groups, as summarized in Table 3.
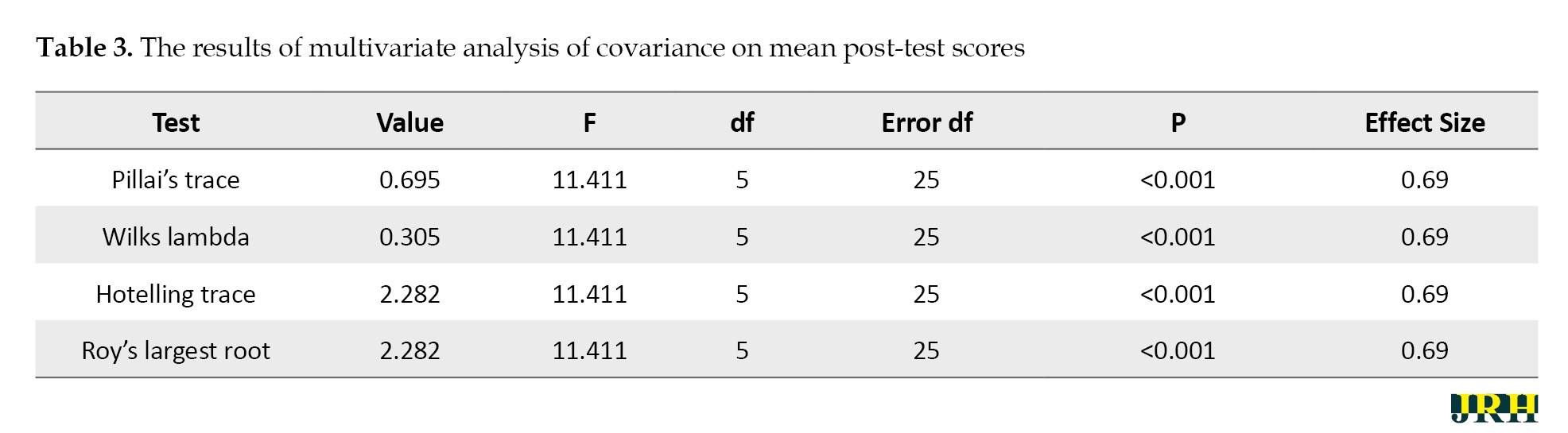
The findings indicated a significant effect of the independent variable on the dependent variables. In other words, there was a notable difference between the experimental and control groups in at least one of the measured variables: Internalized shame, fear of success, or anxiety sensitivity. The calculated effect size revealed that 69% of the total variance between the experimental and control groups was attributable to the influence of the independent variable. Additionally, the statistical power of the test was 1, confirming the adequacy of the sample size for this analysis. To pinpoint the specific variables contributing to these differences, an ANCOVA was conducted as part of the MANCOVA. The detailed results of this analysis are provided in Table 4.
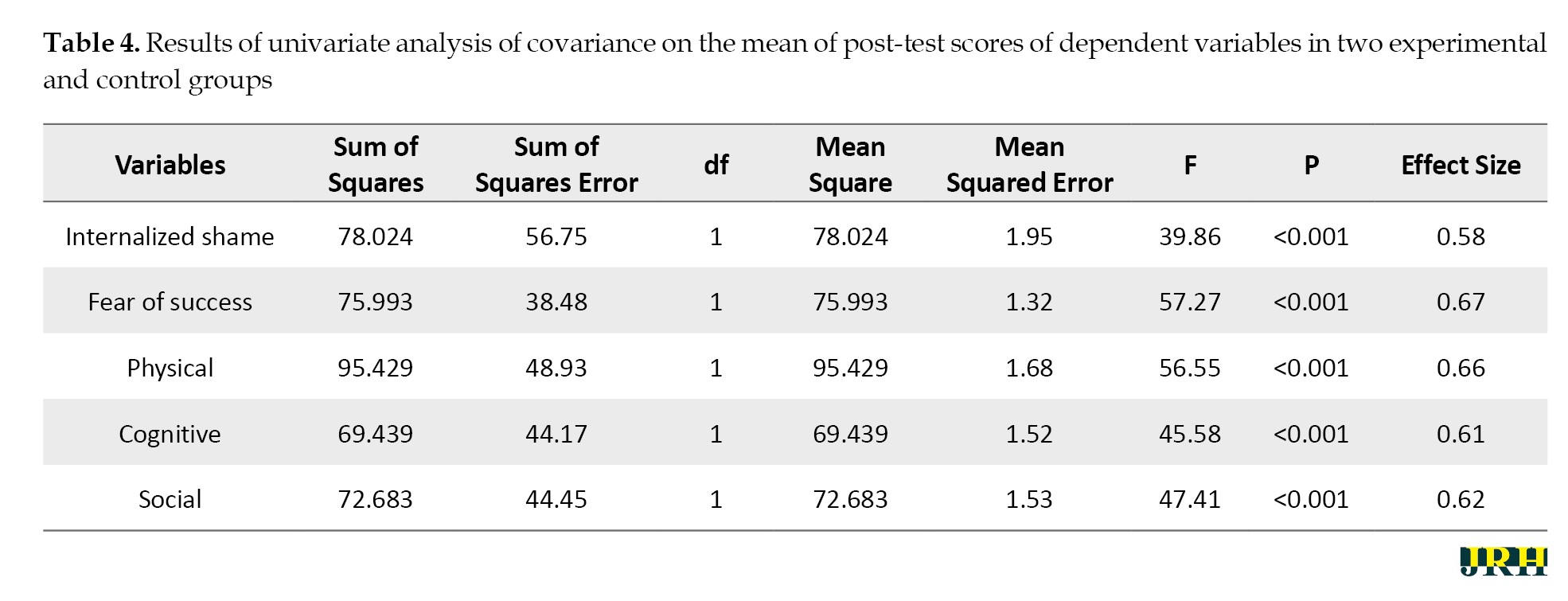
The F-statistic was significant for internalized shame (F=39.86), fear of success (F=57.27), physical (F=56.55), cognitive (F=45.58), and social (F=47.41) at the level of 0.001. These results indicated significant differences between the experimental and control groups across these variables. Moreover, the effect size calculations showed that the intervention accounted for 58% of the variance in internalized shame, 67% in fear of success, 66% in physical, 61% in cognitive, and 62% in social. These findings suggest that ACT is highly effective in significantly reducing internalized shame, fear of success, and anxiety sensitivity in nursing students experiencing IP.
Discussion
Our primary aim was to evaluate the effectiveness of ACT in addressing internalized shame, fear of success, and anxiety sensitivity among nursing students experiencing IP. Given the high expectations, critical evaluations, and intense pressures inherent in academic and clinical environments, nursing students often encounter significant psychological distress, which can reinforce feelings of inadequacy and self-doubt. By integrating ACT, this study aimed to offer a therapeutic framework that promotes acceptance, mindfulness, and value-driven action as a means of mitigating these psychological barriers. To gain a deeper understanding of ACT’s impact, the following discussion first explored its role in reducing internalized shame, examining how mindfulness and cognitive defusion techniques facilitate a shift away from self-critical thought patterns. Next, we analyzed its influence on fear of success, particularly how ACT fosters psychological flexibility to counteract avoidance behaviors [43]. Finally, we evaluated its effects on anxiety sensitivity, highlighting the mechanisms through which ACT reduces reactivity to distressing emotions. Through this structured analysis, we aimed to elucidate how ACT contributes to the overall psychological well-being of nursing students facing IP [35].
The findings of this study demonstrated that ACT is an effective intervention for reducing internalized shame among nursing students experiencing IP. ACT’s success in addressing internalized shame lies in its unique approach to managing self-critical thoughts and emotions [25]. By teaching nursing students mindfulness practices, ACT helps them observe their self-critical thoughts from a detached perspective, recognizing them as temporary mental events rather than objective truths. This shift reduces the emotional weight of these thoughts, freeing students from the cycle of self-judgment [29]. Furthermore, incorporating self-compassion into ACT allows nursing students to view themselves with greater kindness, fostering a sense of intrinsic worth that is not tied to external performance or validation [30]. A key strength of ACT is its focus on values-driven living [11]. By helping nursing students identify their core personal and professional values, ACT enables them to anchor their actions and decisions on what truly matters to them, rather than being derailed by self-doubt or societal pressures [27]. This value-based approach alleviates feelings of shame and empowers students to develop a stronger sense of purpose and resilience, which are critical for navigating the challenges of their education and future careers [29]. Internalized shame can significantly hinder a student’s ability to engage fully in their educational journey by reinforcing cycles of self-doubt and self-criticism. Addressing internalized shame is critical in medical education, where students are subjected to rigorous evaluations and high expectations. By alleviating these feelings, ACT enables students to focus more effectively on learning and practicing essential clinical and theoretical skills, enhancing their educational experiences and professional readiness [33].
This study demonstrated that ACT is a highly effective intervention for reducing the fear of success among nursing students experiencing IP. ACT addresses this fear by providing nursing students with the tools to confront and accept the emotional complexities associated with success [28]. Through mindfulness practices, ACT encourages students to remain present, helping them detach from overwhelming, future-oriented fears about what success might entail [31]. This shift in focus allows them to embrace their achievements without being consumed by anxiety regarding the potential pressures or changes that may follow [15]. Furthermore, ACT emphasizes values-driven living, which plays a critical role in reducing fear of success [29]. By helping students clarify their authentic aspirations and align their actions with their values, ACT provides a meaningful framework for navigating professional and personal growth without being constrained by fear [30]. The study also highlights ACT’s role in fostering confidence and promoting a willingness to pursue professional growth opportunities. Nursing students with IP often impose limitations on themselves, avoiding situations where their success might lead to scrutiny or higher expectations [27]. ACT helps break this cycle by encouraging students to commit to meaningful actions despite the presence of fear or self-doubt. This approach empowers them to embrace their roles fully, both academically and clinically, equipping them with the resilience to thrive in demanding environments [23].
This study revealed that ACT is a highly effective intervention for reducing anxiety sensitivity among nursing students experiencing IP. ACT addresses anxiety sensitivity by teaching cognitive diffusion techniques that help students detach from anxious thoughts and reinterpret them as transient and manageable experiences. By viewing these thoughts as mental events rather than objective truths, students are less likely to become overwhelmed by their fears. The mindfulness practices central to ACT further support this shift, encouraging students to stay present and develop a non-judgmental awareness of their emotional and physiological states [31]. Over time, this approach normalizes the experience of anxiety, reducing its perceived threat and diminishing the avoidance behaviors that often accompany anxiety sensitivity [20]. The emphasis on acceptance and psychological flexibility within ACT is particularly impactful [30]. Nursing students learn to embrace their anxiety-related symptoms as natural responses to high-pressure situations rather than indicators of failure or inadequacy. This acceptance allows them to approach stressors with greater confidence and focus, enabling them to perform effectively in their academic and clinical roles [25]. By fostering resilience and reducing the fear of anxiety itself, ACT equips nursing students with tools to navigate their challenging environments while maintaining emotional balance and clarity [24]. Anxiety sensitivity can magnify stress and impede performance in high-pressure situations, such as clinical rotations or critical exams. By teaching students to view anxiety as a natural response to these challenges, ACT enhances psychological flexibility, allowing them to manage stress more effectively. This resilience ensures that students can focus and perform optimally in demanding educational and clinical settings, facilitating the development of essential skills without being overwhelmed by anxiety [43].
This study was limited by its small sample size and focus on nursing students from specific districts in Tehran, which restricts the generalizability of the findings. Additionally, the absence of long-term follow-up prevented the assessment of ACT’s sustained effects. The reliance on self-reported measures introduces potential biases, and the lack of a comparative intervention for the control group limits the understanding of ACT’s effectiveness relative to other approaches. Moreover, cultural and contextual factors specific to the study population may affect the applicability of the results to broader or international settings. Future studies should expand the sample to include participants from diverse fields and regions to improve generalizability. Incorporating long-term follow-ups can provide insights into the sustainability of ACT’s benefits. Comparative research examining ACT alongside other interventions, such as CBT or mindfulness-based therapy, is recommended to determine the most effective approach for addressing IP. Additionally, integrating ACT principles into educational and clinical training programs could help nursing students manage IP more effectively.
Conclusion
This study highlights the significant potential of ACT as an effective intervention for addressing the multifaceted psychological challenges faced by nursing students experiencing IP. By reducing internalized shame, fear of success, and anxiety sensitivity, ACT empowers students to break free from cycles of self-doubt, self-criticism, and avoidance behaviors that undermine their personal and professional development. Through its emphasis on mindfulness, cognitive diffusion, and values-driven living, ACT equips students with practical tools to reframe negative thought patterns, embrace their emotional experiences, and anchor their actions in meaningful aspirations. This holistic approach fosters resilience, self-compassion, and psychological flexibility, enabling nursing students to navigate the demanding academic and clinical environments with confidence and clarity. These findings underscore the value of integrating ACT into nursing education to promote mental health, well-being, and long-term professional growth.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tarbiat Modares University, Tehran, Iran (Code: IR.MODARES.REC.1402.001). Informed consent was obtained from all participants before their inclusion in the study. Participants were provided with detailed information about the study’s purpose, procedures, and their right to withdraw at any time without any repercussions.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design and supervision: Farzin Bagheri Sheykhangafshe; Data intervention and data collection: Saba Azizrousta and Mohadese Allahzade; Conceptualization, methodology, investigation, data curation, data analysis and writing: Hojjatollah Farahani; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank the nursing students who participated in this study. Your dedication, openness, and commitment were invaluable to this research and greatly contributed to advancing support strategies for nursing students’ well-being and resilience.
References
Becoming a nurse is often rewarding and challenging, requiring students to master complex skills, navigate demanding academic expectations, and develop the emotional resilience necessary for patient care [1]. However, for many nursing students, the pressures of these experiences can be compounded by the psychological phenomenon known as the imposter phenomenon (IP) [2]. First identified by clinical psychologists Clance and Imes in the 1970s, IP describes feelings of self-doubt, inadequacy, and the persistent belief that one’s successes are undeserved or the result of luck rather than competence [3]. Despite their accomplishments, individuals with IP often fear being exposed as frauds, leading to heightened stress, anxiety, and self-criticism. Among nursing students, the prevalence of the IP is particularly concerning [4]. These students are not only transitioning into professional roles that demand high levels of responsibility and expertise but are also navigating environments where their actions directly impact patient outcomes [5]. El-Ashry et al. [2] highlighted that a significant proportion of nursing students experienced moderate to severe levels of depression, anxiety, and stress, with 46.3% reporting moderate levels of IP. They also found a positive correlation between IP and depression, anxiety, and stress.
Internalized shame and IP are deeply interrelated constructs that can profoundly influence an individual’s sense of self and ability to thrive in personal and professional settings [6]. Internalized shame refers to the pervasive, often unconscious, belief that one is fundamentally flawed, unworthy, or inadequate [7]. This self-perception, shaped by experiences of criticism, rejection, or societal expectations, often manifests as persistent self-judgment and feelings of inferiority [8]. The interplay between internalized shame and IP is particularly significant because both reinforce cycles of self-doubt and emotional distress [9]. Internalized shame lays the groundwork for the feelings of inadequacy central to IP. At the same time, the experience of IP perpetuates shame by framing successes as unearned and failures as confirmations of inherent worthlessness [10]. Overall, these dynamics can erode self-confidence, hinder personal growth, and limit professional advancement, creating significant barriers to well-being [11].
Success is often celebrated as a desirable goal, yet for many individuals, it can also evoke complex emotions, such as fear, self-doubt, and anxiety [12]. The fear of success—a psychological phenomenon characterized by apprehension about the consequences of achievement—can manifest in behaviors that undermine personal and professional growth [13]. When coupled with IP, these fears become even more pronounced. The fear of success often stems from concerns about heightened expectations, increased visibility, or peer alienation [14]. For those with the IP, these concerns are amplified by a fundamental disbelief in their capabilities [15]. Success becomes a paradoxical experience; while it validates their achievements externally, it intensifies their internal doubts and fears of being found out [16]. This dynamic can lead to self-sabotage, hesitation to pursue opportunities, and a reluctance to acknowledge or celebrate accomplishments [17].
Anxiety sensitivity, the fear of anxiety-related sensations due to beliefs that they signal harmful physical, cognitive, or social outcomes, plays a significant role in amplifying the experience of IP [18]. For individuals with high anxiety sensitivity, the physiological and emotional responses associated with stress—such as rapid heartbeat, difficulty concentrating, or feelings of inadequacy—are not only uncomfortable but also interpreted as confirmation of their perceived incompetence [19]. The interplay between anxiety sensitivity and IP creates a feedback loop that heightens self-doubt and emotional distress [20]. Individuals who are highly sensitive to the physical and cognitive symptoms of anxiety may interpret these sensations as evidence that they are incapable of meeting expectations or unworthy of their achievements [21]. This self-perception reinforces the imposter belief system, leading to avoidance behaviors, overcompensation, or burnout, as individuals attempt to mask their internal struggles [22].
While traditional approaches to addressing IP focus on challenging distorted thoughts or boosting self-esteem, acceptance and commitment therapy (ACT) offers a novel approach that shifts the focus from thought correction to acceptance and value-driven action [23]. ACT is grounded in the principles of psychological flexibility, mindfulness, and value clarification [24]. Rather than disputing the negative thoughts and feelings that fuel IP, ACT helps individuals develop a new relationship with these experiences [25]. By fostering acceptance, individuals learn to view imposter-related thoughts as transient mental events rather than truths [26]. Through mindfulness, they become more present in the moment, reducing the grip of self-critical rumination [27]. Furthermore, ACT encourages individuals to define their core values—what truly matters to them—and to commit to actions aligned with those values, even in the presence of self-doubt or anxiety [28]. The application of ACT to the IP is especially promising because it equips individuals with tools to break free from the cycle of avoidance and self-criticism that often characterizes IP [29]. By accepting the presence of uncomfortable thoughts and emotions, individuals can redirect their energy toward meaningful goals, fostering both resilience and authenticity [30]. This introduction delves into the role of ACT in addressing IP, emphasizing its potential to promote long-term psychological well-being and a more balanced sense of self-worth [31]. Through this lens, IP is not seen as a barrier to success but as an experience that can be managed and contextualized, empowering individuals to lead values-driven lives [32].
Ong et al. [33] examined the impact of ACT on clinical perfectionism, which is characterized by a rigid adherence to excessively high standards often associated with self-doubt and IP. Their study found that ACT significantly reduced perfectionism, psychological distress, and functional impairment, suggesting that targeting core maladaptive processes—rather than focusing solely on symptom relief—can lead to meaningful improvements in self-efficacy and resilience. Wood et al. [34] conducted a case study on a competitive figure skater with autism who experienced low self-confidence and performance anxiety. Over 25 ACT-based intervention sessions, the athlete learned to accept unhelpful thoughts rather than struggle against them, leading to increased psychological flexibility, reduced self-imposed pressure, and improved self-efficacy. The intervention successfully mitigated self-doubt and perfectionistic tendencies, contributing to greater confidence in training and competition.
French et al. [35] conducted a meta-analysis on ACT self-help interventions, revealing significant reductions in anxiety, depression, and psychological inflexibility. Their findings indicate that ACT fosters psychological flexibility, which in turn decreases self-doubt and feelings of fraudulence associated with IP. Notably, greater improvements were observed when clinician guidance was provided, reinforcing ACT’s effectiveness in addressing perfectionism and enhancing self-confidence. Collectively, these studies support ACT as an effective intervention in reducing perfectionistic concerns, alleviating self-doubt, and mitigating IP. By fostering acceptance, mindfulness, and value-driven actions, ACT promotes greater psychological resilience and self-efficacy, making it a valuable approach for individuals struggling with maladaptive self-perceptions and performance-related anxiety.
This study aimed to comprehensively evaluate the effectiveness of ACT in addressing internalized shame, fear of success, and anxiety sensitivity among nursing students experiencing IP. Given the high-pressure academic and clinical environments that nursing students navigate, these psychological burdens can significantly impact their confidence, professional identity, and overall well-being. This study sought to determine whether ACT, by promoting psychological flexibility, mindfulness, and value-driven actions, can effectively mitigate these challenges and foster greater emotional resilience. Specifically, this research examined how ACT reduces the psychological distress associated with these constructs and whether its mechanisms—such as cognitive defusion, acceptance, and self-compassion—help students break free from self-doubt and self-criticism. By bridging the gap between traditional cognitive approaches and mindfulness-based interventions, this study contributes to the expanding body of research exploring ACT as a novel and evidence-based intervention for IP. Furthermore, it aimed to provide empirical support for integrating ACT into nursing education and mental health interventions, offering a structured approach to enhancing students’ coping strategies, self-efficacy, and professional confidence. If successful, the findings could inform the development of targeted interventions tailored to the specific needs of nursing students, ultimately improving their mental well-being, academic performance, and readiness for the demands of the healthcare profession. By addressing these psychological barriers early in their training, this study has the potential to contribute to long-term improvements in both personal and professional outcomes for future nursing professionals.
Methods
Study design
This study utilized a parallel-group randomized controlled trial (RCT) design with pre-test and post-test measurements, including a control group. Allocation concealment was ensured by using a computer-generated randomization sequence, which was performed by an independent researcher who was not involved in participant recruitment or intervention delivery.
Participants
The statistical population comprised nursing students residing in Districts 7 and 8 of Tehran from September to November 2023. From an initial pool of 36 eligible students, randomized block sampling was applied to ensure balanced group allocation, resulting in 18 participants in the experimental group and 18 in the control group. Randomization was conducted using a stratified approach, accounting for gender and academic performance to minimize selection bias. The sample size calculation was performed using G*Power software, version 3.1, with an effect size of 1.53, a power (1−β) of 0.97, and an alpha of 0.05, based on prior studies.
The effect size selection was informed by previous clinical trials and meta-analyses on ACT interventions for psychological distress in student populations. The practical significance of this effect size suggests a substantial reduction in imposter syndrome symptoms through ACT.
Inclusion criteria: A score greater than 45 on the IP scale; age range of 18–30 years (to ensure population homogeneity and developmental relevance); written informed consent (an ethical requirement rather than a selection criterion); absence of psychiatric medication usage (to control for pharmacological influences on psychological symptoms).
Exclusion criteria: Failure to respond to more than 10% of questionnaire items (to maintain data integrity); a significant increase in stress levels, defined as a ≥1.5 standard deviation (SD) increase in perceived stress scale scores; missing more than two ACT sessions (to ensure intervention adherence).
Tools/Instruments
Imposter syndrome scale (ISS): The ISS was originally developed by Clance and Imes [3]. The scale consists of 20 items, where participants indicate their level of agreement with each statement on a five-point Likert scale ranging from “never” to “very much.” Based on the total score, levels of imposter syndrome are categorized as follows: A score of less than 40 indicates weak imposter syndrome, 41–60 indicates moderate imposter syndrome, 61–80 indicates pathological imposter syndrome, and a score above 80 signifies severe imposter syndrome. Studies have reported high internal consistency for the ISS, with Cronbach’s α coefficients ranging from 0.85 to 0.94 [3]. Additionally, its validity and reliability were found to be satisfactory among Iranian students, with a reported Cronbach’s α of 0.86 [36]. In the present study, the reliability of the scale was also confirmed, with a Cronbach’s α coefficient of 0.82.
Internalized shame scale (ISS): The ISS was developed by Cook [37] to measure the degree of internalized shame experienced by individuals. This scale consists of 30 items, scored on a five-point Likert scale ranging from 1 (“never”) to 5 (“always”), with total scores ranging from 30 to 150. Higher scores indicate greater levels of internalized shame. The ISS assesses the respondent’s feelings of personal value, self-adequacy, and the tendency to experience shame in social and personal contexts. Cook [37] reported high reliability for the ISS, with Cronbach’s α coefficients ranging from 0.84 to 0.97, reflecting its strong psychometric properties. Additionally, Jafari et al. [38] confirmed the validity and reliability of the scale in Iran, reporting a Cronbach’s α of 0.89. In the present study, the reliability of the ISS was also confirmed, with a Cronbach’s α coefficient of 0.85, supporting its continued use in diverse populations.
Fear of success scale (FOSS): The FOSS was developed in 1979 by Zuckerman and Allison to assess the extent of an individual’s fear of achieving success [39]. This fear is conceptualized as a learned personality trait rooted in early life experiences, reflecting a stable motivation to avoid success due to negative perceptions and anticipated consequences of achievement. According to Atkinson, fear of success represents a personal inclination based on the belief that success might lead to real or predicted negative outcomes. The FOSS consists of 27 items, scored on a seven-point Likert scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”), with total scores ranging from 27 to 189. Higher scores indicate a greater fear of success. In the original study, the FOSS demonstrated strong psychometric properties, with reported reliability (Cronbach’s α) ranging between 0.82 and 0.88 and good content and construct validity, supporting its use as a reliable measure of fear of success [39]. Additionally, Ashrafifard and Mafakheri [40] reported satisfactory validity and reliability for the scale in Iran, with a Cronbach’s α coefficient of 0.83. In the present study, the reliability of the scale was also confirmed, with a Cronbach’s α coefficient of 0.84, supporting its use as a reliable measure of fear of success.
Anxiety sensitivity index-3 (ASI-3): The ASI-3 measures the level of worry related to various symptoms of anxiety [41]. Derived from the revised ASI-3, this scale comprises 18 items and evaluates anxiety sensitivity across three dimensions: physical concerns (6 items), cognitive concerns (6 items), and social concerns (6 items). It is scored on a five-point Likert scale ranging from 0 (“very little agree”) to 4 (“completely agree”), with total scores ranging from 0 to 72. The ASI-3 demonstrates strong psychometric properties, with internal consistency coefficients ranging between 0.76 and 0.86 for physical concerns, 0.79 and 0.91 for cognitive concerns, and 0.73 and 0.86 for social concerns. Additionally, the scale has shown good convergent and divergent validity [41]. In Iran, Cronbach’s α coefficients for the physical, cognitive, and social subscales were reported as 0.89, 0.84, and 0.80, respectively [42]. In the present study, the internal consistency for the subscales was also confirmed, with Cronbach’s α coefficients ranging from 0.81 to 0.85.
Data collection
Data collection involved a pre-test and post-test evaluation using validated scales, including the ISS, ISS, FOSS, and ASI-3. The experimental group underwent eight 90-minute ACT sessions over eight weeks, while the control group received no intervention. Pre-test assessments established baseline levels for all variables, and post-test evaluations measured changes following the intervention.
ACT sessions by a therapist in the psychology clinic were then performed in eight 90-minute weekly group sessions for the experimental group, while the control group did not receive any intervention. ACT was designed based on the ACT programs proposed by Hayes et al. [43] and also taking into account the key characteristics in the design of ACT programs (Table 1).
Data analysis
To analyze the research data, descriptive statistics (Mean±SD) and covariance analysis were used based on their assumptions using SPSS software, version 27. The significance level of these tests was considered 0.05. The Shapiro-Wilk test checked the normality of the distribution of variables in the two groups, and its result was not significant for all variables. Therefore, it can be concluded that the distribution of variables was normal (P>0.05).
Results
The mean age of participants in the intervention group was 24.38±6.07 years, while in the control group, it was 24.89±5.69 years. In terms of demographics, 65% were female, 48% were married, and 53% held a bachelor’s degree. Additionally, 66% of participants had experienced IP for two years.
A chi-square test was used to compare the intervention and control groups in terms of age, gender, marital status, educational level, and duration of IP. The results showed no significant differences between the two groups (χ²=3.24, P=0.518), indicating that the groups were statistically equivalent at baseline. This lack of significant difference suggests that any observed effects in the study are more likely attributed to the intervention rather than pre-existing demographic variations. Additionally, an independent t-test confirmed that there was no significant difference in age between the groups (t=0.72, P=0.476), supporting the assumption that the groups were well-matched. By ensuring demographic equivalence, these results strengthen the validity of subsequent analyses by minimizing the risk of confounding variables influencing the outcomes.
Table 2 presents the Mean±SD of pre-test and post-test scores for internalized shame, fear of success, and anxiety sensitivity among nursing students with IP in the experimental and control groups.
Additionally, the results of the Shapiro-Wilk test for normality are included. The table indicates that none of the variables showed significant deviations based on the Shapiro-Wilk test, suggesting that the distribution of variables in both groups is normal (Table 2).
Multivariate analysis of covariance (MANCOVA) was employed to assess the effect of ACT on internalized shame, fear of success, and anxiety sensitivity in nursing students with IP. The results of Levene’s test, used to evaluate the homogeneity of variance among the dependent variables across groups, indicated that variances were equal for internalized shame (F=4.1, P=0.051), fear of success (F=2.81, P=0.102), and anxiety sensitivity (F=1.83, P=0.187). Additionally, Box’s test, conducted to assess the equality of the covariance matrix of dependent variables between the experimental and control groups, confirmed that the covariance matrices were equal (Box M=18.89, F=1.05, P=0.391).
The chi-square Bartlett test, used to evaluate sphericity or the significance of relationships among internalized shame, fear of success, and anxiety sensitivity, revealed a significant relationship between the variables (χ2=124.77, df=14, P<0.01). Another critical assumption for conducting MANCOVA is the homogeneity of regression slopes. This was assessed by examining the interaction between the dependent variables and the independent variable (intervention method) across pre-test and post-test scores. The interaction results indicated that the regression slopes were homogeneous, as these interactions were not significant. Therefore, this assumption was also satisfied. Since all necessary assumptions for conducting MANCOVA were met, the test was deemed appropriate. Subsequently, MANCOVA was performed to identify the differences between the experimental and control groups, as summarized in Table 3.
The findings indicated a significant effect of the independent variable on the dependent variables. In other words, there was a notable difference between the experimental and control groups in at least one of the measured variables: Internalized shame, fear of success, or anxiety sensitivity. The calculated effect size revealed that 69% of the total variance between the experimental and control groups was attributable to the influence of the independent variable. Additionally, the statistical power of the test was 1, confirming the adequacy of the sample size for this analysis. To pinpoint the specific variables contributing to these differences, an ANCOVA was conducted as part of the MANCOVA. The detailed results of this analysis are provided in Table 4.
The F-statistic was significant for internalized shame (F=39.86), fear of success (F=57.27), physical (F=56.55), cognitive (F=45.58), and social (F=47.41) at the level of 0.001. These results indicated significant differences between the experimental and control groups across these variables. Moreover, the effect size calculations showed that the intervention accounted for 58% of the variance in internalized shame, 67% in fear of success, 66% in physical, 61% in cognitive, and 62% in social. These findings suggest that ACT is highly effective in significantly reducing internalized shame, fear of success, and anxiety sensitivity in nursing students experiencing IP.
Discussion
Our primary aim was to evaluate the effectiveness of ACT in addressing internalized shame, fear of success, and anxiety sensitivity among nursing students experiencing IP. Given the high expectations, critical evaluations, and intense pressures inherent in academic and clinical environments, nursing students often encounter significant psychological distress, which can reinforce feelings of inadequacy and self-doubt. By integrating ACT, this study aimed to offer a therapeutic framework that promotes acceptance, mindfulness, and value-driven action as a means of mitigating these psychological barriers. To gain a deeper understanding of ACT’s impact, the following discussion first explored its role in reducing internalized shame, examining how mindfulness and cognitive defusion techniques facilitate a shift away from self-critical thought patterns. Next, we analyzed its influence on fear of success, particularly how ACT fosters psychological flexibility to counteract avoidance behaviors [43]. Finally, we evaluated its effects on anxiety sensitivity, highlighting the mechanisms through which ACT reduces reactivity to distressing emotions. Through this structured analysis, we aimed to elucidate how ACT contributes to the overall psychological well-being of nursing students facing IP [35].
The findings of this study demonstrated that ACT is an effective intervention for reducing internalized shame among nursing students experiencing IP. ACT’s success in addressing internalized shame lies in its unique approach to managing self-critical thoughts and emotions [25]. By teaching nursing students mindfulness practices, ACT helps them observe their self-critical thoughts from a detached perspective, recognizing them as temporary mental events rather than objective truths. This shift reduces the emotional weight of these thoughts, freeing students from the cycle of self-judgment [29]. Furthermore, incorporating self-compassion into ACT allows nursing students to view themselves with greater kindness, fostering a sense of intrinsic worth that is not tied to external performance or validation [30]. A key strength of ACT is its focus on values-driven living [11]. By helping nursing students identify their core personal and professional values, ACT enables them to anchor their actions and decisions on what truly matters to them, rather than being derailed by self-doubt or societal pressures [27]. This value-based approach alleviates feelings of shame and empowers students to develop a stronger sense of purpose and resilience, which are critical for navigating the challenges of their education and future careers [29]. Internalized shame can significantly hinder a student’s ability to engage fully in their educational journey by reinforcing cycles of self-doubt and self-criticism. Addressing internalized shame is critical in medical education, where students are subjected to rigorous evaluations and high expectations. By alleviating these feelings, ACT enables students to focus more effectively on learning and practicing essential clinical and theoretical skills, enhancing their educational experiences and professional readiness [33].
This study demonstrated that ACT is a highly effective intervention for reducing the fear of success among nursing students experiencing IP. ACT addresses this fear by providing nursing students with the tools to confront and accept the emotional complexities associated with success [28]. Through mindfulness practices, ACT encourages students to remain present, helping them detach from overwhelming, future-oriented fears about what success might entail [31]. This shift in focus allows them to embrace their achievements without being consumed by anxiety regarding the potential pressures or changes that may follow [15]. Furthermore, ACT emphasizes values-driven living, which plays a critical role in reducing fear of success [29]. By helping students clarify their authentic aspirations and align their actions with their values, ACT provides a meaningful framework for navigating professional and personal growth without being constrained by fear [30]. The study also highlights ACT’s role in fostering confidence and promoting a willingness to pursue professional growth opportunities. Nursing students with IP often impose limitations on themselves, avoiding situations where their success might lead to scrutiny or higher expectations [27]. ACT helps break this cycle by encouraging students to commit to meaningful actions despite the presence of fear or self-doubt. This approach empowers them to embrace their roles fully, both academically and clinically, equipping them with the resilience to thrive in demanding environments [23].
This study revealed that ACT is a highly effective intervention for reducing anxiety sensitivity among nursing students experiencing IP. ACT addresses anxiety sensitivity by teaching cognitive diffusion techniques that help students detach from anxious thoughts and reinterpret them as transient and manageable experiences. By viewing these thoughts as mental events rather than objective truths, students are less likely to become overwhelmed by their fears. The mindfulness practices central to ACT further support this shift, encouraging students to stay present and develop a non-judgmental awareness of their emotional and physiological states [31]. Over time, this approach normalizes the experience of anxiety, reducing its perceived threat and diminishing the avoidance behaviors that often accompany anxiety sensitivity [20]. The emphasis on acceptance and psychological flexibility within ACT is particularly impactful [30]. Nursing students learn to embrace their anxiety-related symptoms as natural responses to high-pressure situations rather than indicators of failure or inadequacy. This acceptance allows them to approach stressors with greater confidence and focus, enabling them to perform effectively in their academic and clinical roles [25]. By fostering resilience and reducing the fear of anxiety itself, ACT equips nursing students with tools to navigate their challenging environments while maintaining emotional balance and clarity [24]. Anxiety sensitivity can magnify stress and impede performance in high-pressure situations, such as clinical rotations or critical exams. By teaching students to view anxiety as a natural response to these challenges, ACT enhances psychological flexibility, allowing them to manage stress more effectively. This resilience ensures that students can focus and perform optimally in demanding educational and clinical settings, facilitating the development of essential skills without being overwhelmed by anxiety [43].
This study was limited by its small sample size and focus on nursing students from specific districts in Tehran, which restricts the generalizability of the findings. Additionally, the absence of long-term follow-up prevented the assessment of ACT’s sustained effects. The reliance on self-reported measures introduces potential biases, and the lack of a comparative intervention for the control group limits the understanding of ACT’s effectiveness relative to other approaches. Moreover, cultural and contextual factors specific to the study population may affect the applicability of the results to broader or international settings. Future studies should expand the sample to include participants from diverse fields and regions to improve generalizability. Incorporating long-term follow-ups can provide insights into the sustainability of ACT’s benefits. Comparative research examining ACT alongside other interventions, such as CBT or mindfulness-based therapy, is recommended to determine the most effective approach for addressing IP. Additionally, integrating ACT principles into educational and clinical training programs could help nursing students manage IP more effectively.
Conclusion
This study highlights the significant potential of ACT as an effective intervention for addressing the multifaceted psychological challenges faced by nursing students experiencing IP. By reducing internalized shame, fear of success, and anxiety sensitivity, ACT empowers students to break free from cycles of self-doubt, self-criticism, and avoidance behaviors that undermine their personal and professional development. Through its emphasis on mindfulness, cognitive diffusion, and values-driven living, ACT equips students with practical tools to reframe negative thought patterns, embrace their emotional experiences, and anchor their actions in meaningful aspirations. This holistic approach fosters resilience, self-compassion, and psychological flexibility, enabling nursing students to navigate the demanding academic and clinical environments with confidence and clarity. These findings underscore the value of integrating ACT into nursing education to promote mental health, well-being, and long-term professional growth.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tarbiat Modares University, Tehran, Iran (Code: IR.MODARES.REC.1402.001). Informed consent was obtained from all participants before their inclusion in the study. Participants were provided with detailed information about the study’s purpose, procedures, and their right to withdraw at any time without any repercussions.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design and supervision: Farzin Bagheri Sheykhangafshe; Data intervention and data collection: Saba Azizrousta and Mohadese Allahzade; Conceptualization, methodology, investigation, data curation, data analysis and writing: Hojjatollah Farahani; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank the nursing students who participated in this study. Your dedication, openness, and commitment were invaluable to this research and greatly contributed to advancing support strategies for nursing students’ well-being and resilience.
References
- Christensen M, Aubeeluck A, Fergusson D, Craft J, Knight J, Wirihana L, et al. Do student nurses experience Imposter Phenomenon? An international comparison of final year undergraduate nursing students readiness for registration. Journal of Advanced Nursing. 2016; 72(11):2784-93. [DOI:10.1111/jan.13034] [PMID]
- El-Ashry AM, Taha SM, Abd Elhay ES, Hammad HA, Khedr MA, El-Sayed MM. Prevalence of imposter syndrome and its association with depression, stress, and anxiety among nursing students: A multi-center cross-sectional study. BMC Nursing. 2024; 23(1):862. [DOI:10.1186/s12912-024-02414-w] [PMID]
- Clance PR, Imes SA. The imposter phenomenon in high achieving women: Dynamics and therapeutic intervention. Psychotherapy: Theory, Research & Practice. 1978; 15(3):241-7. [DOI:10.1037/h0086006]
- Aubeeluck A, Stacey G, Stupple EJ. Do graduate entry nursing student’s experience ‘imposter phenomenon’?: An issue for debate. Nurse Education in Practice. 2016; 19:104-6. [DOI:10.1016/j.nepr.2016.06.003] [PMID]
- Peng Y, Xiao SW, Tu H, Xiong XY, Ma ZJ, Xu WJ, et al. The impostor phenomenon among nursing students and nurses: A scoping review. Frontiers in Psychology. 2022; 13:809031. [DOI:10.3389/fpsyg.2022.809031] [PMID]
- Fimiani R, Leonardi J, Gorman B, Gazzillo F. Interpersonal guilt, impostor phenomenon, depression, and anxiety. Psychology Hub. 2021; 38(2):31-40. [Link]
- Jacobs MD, Sasser JT. Impostor phenomenon in undergraduate nursing students: A pilot study of prevalence and patterns. Journal of Nursing Education. 2021; 60(6):329-32. [DOI:10.3928/01484834-20210520-05] [PMID]
- Kamran Siddiqui Z. Navigating imposter phenomenon: A collective journey towards empowerment. The Clinical Teacher. 2024; 21(5):e13783. [DOI:10.1111/tct.13783] [PMID]
- Chrousos GP, Mentis AF, Dardiotis E. Focusing on the neuro-psycho-biological and evolutionary underpinnings of the imposter syndrome. Frontiers in Psychology. 2020; 11:1553. [DOI:10.3389/fpsyg.2020.01553] [PMID]
- Yang Y, Xu C, Karatas T, Glass TE, Maeda Y. Achievement goals, imposter syndrome, and psychological distress among female STEM students: A structural equation model. Journal of College Student Retention: Research, Theory & Practice. 2024; 15210251231219933. [DOI:10.1177/15210251231219933]
- Le L. Unpacking the imposter syndrome and mental health as a person of color first generation college student within institutions of higher education. McNair Research Journal SJSU. 2021; 17(1):10. [DOI:10.31979/mrj.2021.1710]
- Cader FA, Gupta A, Han JK, Ibrahim NE, Lundberg GP, Mohamed A, et al. How feeling like an imposter can impede your success. JACC. Case Reports. 2021; 3(2):347-9. [DOI:10.1016/j.jaccas.2021.01.003] [PMID]
- Zanchetta M, Junker S, Wolf AM, Traut-Mattausch E. “Overcoming the fear that haunts your success”-the effectiveness of interventions for reducing the impostor phenomenon. Frontiers in Psychology. 2020; 11:405. [DOI:10.3389/fpsyg.2020.00405] [PMID]
- Noskeau R, Santos A, Wang W. Connecting the dots between mindset and impostor phenomenon, via fear of failure and goal orientation, in working adults. Frontiers in Psychology. 2021; 12:588438. [DOI:10.3389/fpsyg.2021.588438] [PMID]
- Ayaz-Alkaya S, Köse-Kabakcıoğlu N, Terzi H. Fear of lacking access to mobile devices ("nomophobia"): A preliminary study of prevalence, predictors, and relationship to perceived stress in nursing students. Nursing Outlook. 2025; 73(4):102434. [DOI:10.1016/j.outlook.2025.102434] [PMID]
- Breeze M. Imposter syndrome as a public feeling. In: Taylor Y, Lahad K, editors. Feeling academic in the Neoliberal University. Palgrave Studies in Gender and Education. Cham: Palgrave Macmillan; 2018. [DOI:10.1007/978-3-319-64224-6_9]
- Pákozdy C, Askew J, Dyer J, Gately P, Martin L, Mavor KI, et al. The imposter phenomenon and its relationship with self-efficacy, perfectionism and happiness in university students. Current Psychology. 2024; 43(6):5153-62. [DOI:10.1007/s12144-023-04672-4]
- Fraenza CB. The role of social influence in anxiety and the imposter phenomenon. Online Learning. 2016; 20(2):230-43. [DOI:10.24059/olj.v20i2.618]
- Iwenofu C, Dupont R, Kaczkurkin A. Hope for the future can reduce anxiety, perfectionism, and feelings of imposter syndrome. Vanderbilt Undergraduate Research Journal. 2024; 14(1). [Link]
- Wang KT, Sheveleva MS, Permyakova TM. Imposter syndrome among Russian students: The link between perfectionism and psychological distress. Personality and Individual Differences. 2019; 143:1-6. [DOI:10.1016/j.paid.2019.02.005]
- Zulfiqar N, Abbasi T. Mediating Role of Test Anxiety in Association Between Imposter Phenomenon and Perfectionism among High-Achieving Students. Journal of Advanced Academics. 2024; 35(4):698-717. [DOI:10.1177/1932202X241281782]
- Maftei A, Dumitriu A, Holman AC. They will discover I’ma fraud! The Imposter Syndrome Among Psychology Students. Studia Psychologica. 2021; 63(4):337-51. [DOI:10.31577/sp.2021.04.831]
- Heslop G, Bonilla-Velez J, Faucett EA, Cabrera-Muffly C. Understanding and overcoming the psychological barriers to diversity: Imposter syndrome and stereotype threat. Current Otorhinolaryngology Reports. 2023; 11(2):71-2. [DOI:10.1007/s40136-023-00464-3]
- Bravata DM, Watts SA, Keefer AL, Madhusudhan DK, Taylor KT, Clark DM, et al. Prevalence, predictors, and treatment of impostor syndrome: A systematic review. Journal of General Internal Medicine. 2020; 35(4):1252-75. [DOI:10.1007/s11606-019-05364-1] [PMID]
- Watson DR, Hill AP, Madigan DJ, Donachie TC. Effectiveness of an online acceptance and commitment therapy programme for perfectionism in soccer players: A randomized control trial. Sport, Exercise, and Performance Psychology. 2024; 13(1):5-22. [DOI:10.1037/spy0000333]
- Ong CW, Hancock AS, Barrett TS, Lee EB, Wan N, Gillam RB, et al. A preliminary investigation of the effect of acceptance and commitment therapy on neural activation in clinical perfectionism. Journal of Contextual Behavioral Science. 2020; 18:152-61. [DOI:10.1016/j.jcbs.2020.09.007]
- Barrett K, Stewart I. A preliminary comparison of the efficacy of online Acceptance and Commitment Therapy (ACT) and Cognitive Behavioural Therapy (CBT) stress management interventions for social and healthcare workers. Health & Social Care in the Community. 2021; 29(1):113-26. [DOI:10.1111/hsc.13074] [PMID]
- Siraj RA, Aldhahir AM, Alzahrani YR, Alqarni AA, Alanazi TM, Alruwaili A, et al. The impact of imposter syndrome on self-esteem and intention to quit among respiratory therapy (RT) students in Saudi Arabia. SAGE Open Medicine. 2024; 12:20503121241260149. [DOI:10.1177/20503121241260149] [PMID]
- Hutchins HM, Flores J. Don’t believe everything you think: Applying a cognitive processing therapy intervention to disrupting imposter phenomenon. New Horizons in Adult Education and Human Resource Development. 2021; 33(4):33-47. [DOI:10.1002/nha3.20325]
- Sheykhangafshe FB, Nouri E, Niri VS, Choubtashani M, Farahani H. The efficacy of cognitive behavioral therapy on mental health, self-esteem and emotion regulation of medical students with imposter syndrome. Educational Research in Medical Sciences. 2024; 13(1):e147868. [DOI:10.5812/ermsj-147868]
- Siddiqui ZK, Church HR, Jayasuriya R, Boddice T, Tomlinson J. Educational interventions for imposter phenomenon in healthcare: A scoping review. BMC Medical Education. 2024; 24(1):43. [DOI:10.1186/s12909-023-04984-w] [PMID]
- Clark P, Holden C, Russell M, Downs H. The impostor phenomenon in mental health professionals: Relationships among compassion fatigue, burnout, and compassion satisfaction. Contemporary Family Therapy. 2022; 44(2):185-97. [DOI:10.1007/s10591-021-09580-y] [PMID]
- Ong CW, Lee EB, Krafft J, Terry CL, Barrett TS, Levin ME, et al. A randomized controlled trial of acceptance and commitment therapy for clinical perfectionism. Journal of Obsessive-Compulsive and Related Disorders. 2019; 22:100444. [DOI:10.1016/j.jocrd.2019.100444]
- Wood S, Turner MJ. Using acceptance and commitment therapy to develop self-confidence in a neurodivergent athlete. Case Studies in Sport and Exercise Psychology. 2024; 8(1):37-46. [Link]
- French K, Golijani-Moghaddam N, Schröder T. What is the evidence for the efficacy of self-help acceptance and commitment therapy? A systematic review and meta-analysis. Journal of Contextual Behavioral Science. 2017; 6(4):360-74. [DOI:10.1016/j.jcbs.2017.08.002]
- Bagheri Sheykhangafshe F, Tajbakhsh K, Savabi Niri V, Mikelani N, Eghbali F, Fathi-Ashtiani A. The effectiveness of schema therapy on self-efficacy, burnout, and perfectionism of employees with imposter syndrome. Health and Development Journal. 2022; 11(3):140-8. [DOI:10.34172/jhad.92349]
- Cook DR. The Internalized Shame Scale: Professional manual. Menomonie, WI: Channel Press; 1993. [Link]
- Jafari T, Zarei M, Shahraki MN, Amani O. Investigating the relationship between burnout, internalized shame and metacognitive beliefs on emotion regulation in women affected by marital infidelity. Psychology of Woman Journal. 2023; 4(1):90-8. [DOI:10.61838/kman.pwj.4.1.10]
- Zuckerman M, Allison SN. Fear of Success Scale. Journal of Personality Assessment. 1977. [DOI:10.1037/t07231-000]
- Ashrafifard S, Mafakheri A. Investigating the relationship between attribution styles and metacognitive skills with fear of success among students. Iranian Journal of Psychiatry and Behavioral Sciences. 2017; 11(2):e9461. [DOI:10.5812/ijpbs.9461]
- Taylor S, Zvolensky MJ, Cox BJ, Deacon B, Heimberg RG, Ledley DR, et al. Robust dimensions of anxiety sensitivity: Development and initial validation of the anxiety sensitivity index-3. Psychological Assessment. 2007; 19(2):176-88. [DOI:10.1037/1040-3590.19.2.176] [PMID]
- Sheykhangafshe FB, Fathi-Ashtiani A, Savabi Niri V, Otadi S, Rezaei Golezani H. The efficacy of cognitive-behavioral therapy on coping strategies and anxiety sensitivity of patients with covid-19 obsession. Journal of Research and Health. 2023; 13(1):41-50. [DOI:10.32598/JRH.13.1.1922.2]
- Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: The process and practice of mindful change. New York: Guilford Press; 2011. [Link]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2025/01/3 | Accepted: 2025/03/5 | Published: 2025/11/7
Received: 2025/01/3 | Accepted: 2025/03/5 | Published: 2025/11/7
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
