

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 181-188 |
Back to browse issues page


Ethics code: IR.MAZUMS.RIB.REC.1401.109
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
mokhtari B, Farrokhfar S, roodgar M. Impact of Parental Income, Employment, and Housing on Infant Growth in the First Year of Life in Ramsar City, Iran. J Research Health 2026; 16 (2) :181-188
URL: http://jrh.gmu.ac.ir/article-1-2727-en.html
URL: http://jrh.gmu.ac.ir/article-1-2727-en.html



1- Faculty of Medicine, Ramsar Campus, Mazandaran University of Medical Sciences, Ramsar, Iran. & Student Research Committee, Ramsar Campus, Mazandaran University of Medical Sciences, Ramsar, Iran.
2- Department of Anatomical Sciences, Faculty of Medicine, Ramsar Campus, Mazandaran University of Medical Sciences, Ramsar, Iran. ,samanefarrokhfar@gmail.com
2- Department of Anatomical Sciences, Faculty of Medicine, Ramsar Campus, Mazandaran University of Medical Sciences, Ramsar, Iran. ,
Full-Text [PDF 503 kb]
(151 Downloads)
| Abstract (HTML) (760 Views)
Full-Text: (148 Views)
Introduction
The growth patterns of children during their first year of life are crucial milestones that serve as a window into their overall health, making it essential for healthcare providers to closely monitor these changes and uncover the factors influencing them. Anthropometry is a quantitative, non-invasive, and cost-effective approach to evaluating the health and growth of infants and children. By measuring various body parts, such as weight, height, head circumference, clavicle length, and femur length, physical differences can be identified, aiding in public health and clinical decision-making [1, 2]. Growth patterns are key indicators of a child’s well-being, with poverty and food insecurity linked to higher mortality rates, delayed development, disabilities, and reduced national productivity. Traditionally associated with thinness and low weight, food insecurity is increasingly associated with obesity as a marker of poor nutrition [3, 4]. The importance of early nutrition in lifelong health underpins the Developmental Origins of Health and Disease [5]. Poverty significantly contributes to malnutrition, with socioeconomic status (SES) (income, location, and housing) directly correlating with health outcomes. Improved economic conditions enhance healthcare access and influence social determinants of health, which account for over 50% of children’s health outcomes [6-9].
Parental employment also affects children’s health, particularly maternal employment, which presents a complex dynamic. While increased household income from maternal work can improve health spending, reduced maternal availability may limit the time spent on direct childcare and nutritious meal preparation, resulting in an ambiguous overall impact on child health [10, 11].
Infant growth is affected by various factors, including parental SES, and identifying and addressing the root causes of reduced growth indicators is essential for public health, health development, and correcting social imbalances. This cross-sectional study aimed to investigate the relationship between parental SES (including home ownership, income, and employment) and anthropometric changes (height, weight, and head circumference) in the first year of life in children referred to Ramsar health centers from March 2022 to March 2023 (1401 AH Iranian calendar).
Methods
A retrospective cross-sectional study was conducted to investigate the impact of household SES on infant anthropometric indices during the first year of life among children visiting health centers in Ramsar City, Iran, from March 2022 to March 2023. The inclusion criteria were full-term birth, absence of genetic disorders, and being an only child, while those with genetic and congenital diseases were excluded. This field-based study employed a checklist as a data collection tool. The checklist included information on annual income, parental employment, and home ownership. Due to the non-normal distribution of income, household incomes were categorized into four groups using Iran’s central percentile index. Concurrently, infant anthropometric indices (height, weight, and head circumference) were measured and recorded by a trained and consistent health worker using a home-based/health center study method. Changes in these variables were evaluated according to the infants’ age range. Using the Morgan table and considering that the average number of singleton births in the 5 years prior to the study in Ramsar was below 300 per year, the sample size was determined to be 148 babies. However, due to the erosive volume and unpredictability of possible sample outflows, such as migration and mortality, 180 cases were reviewed, of which 153 were eligible for the study.
Statistical analysis was performed using SPSS software, version 26 and Prism GraphPad, and appropriate statistical tests were employed in each case. Within-subject analysis was performed using the Greenhouse-Geisser correction, and the independent t-test was used to compare the means of two independent populations. The significance level was set at 0.05 (P<0.05) in all cases.
Results
The results of the present study were obtained from a retrospective review of the records of 153 eligible infants as follows: Regarding housing status, 116 families (75.8%) were homeowners, and 37 families (24.2%) were renters. The income of 16 families (10.5%) was in the first quartile, 63 families (41.2%) in the second, 60 families (39.2%) in the third, and 14 families (9.2%) in the fourth. In terms of parental employment status, 38 cases (24.8%) had both parents employed, 102 cases (66.7%) had a father employed and a stay-at-home mother, 8 cases (5.2%) had an unemployed father and an employed mother, and five cases (3.3%) had both parents unemployed.
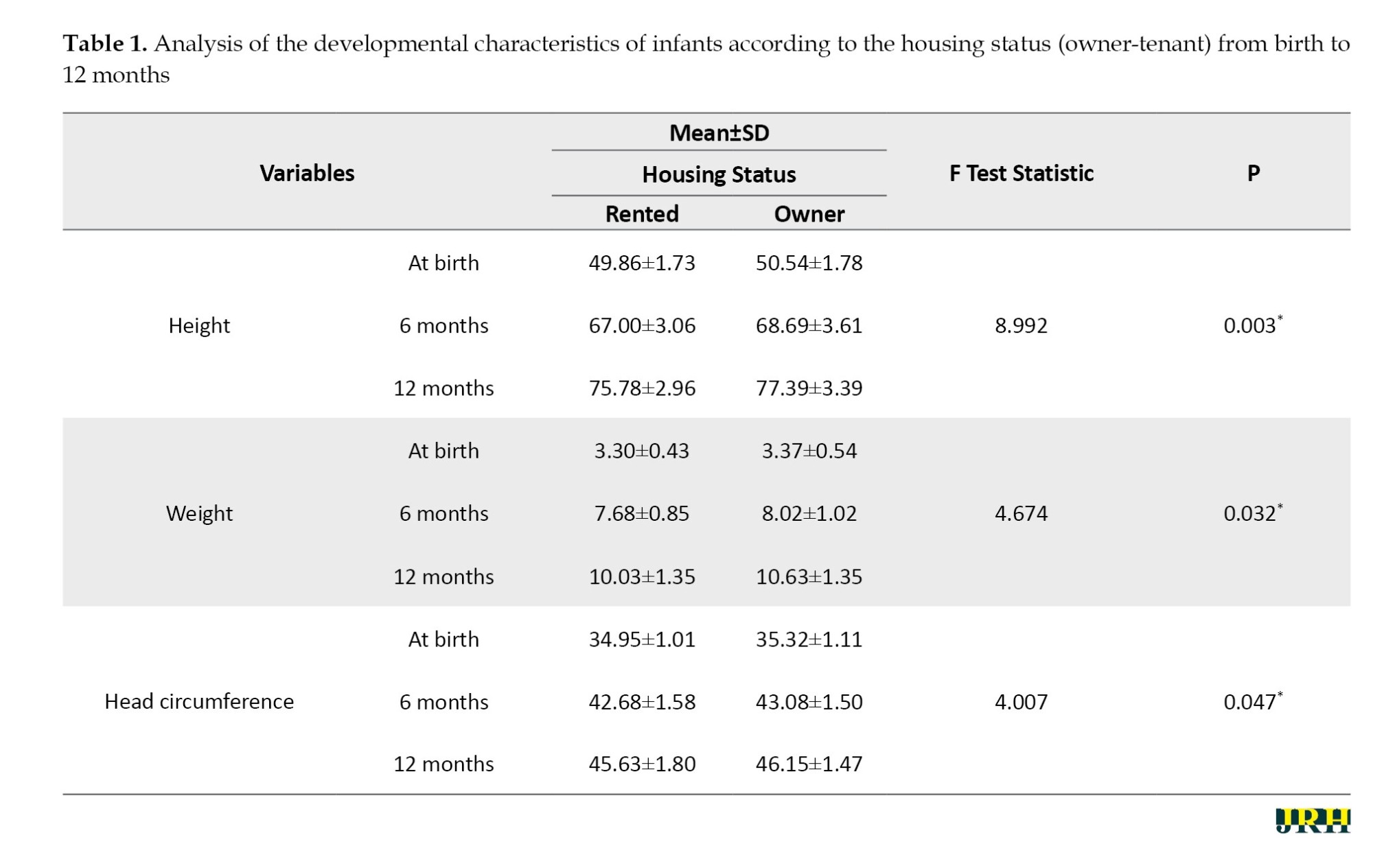
Determining the mean of anthropometric indices (height, weight, and head circumference) among children visiting Ramsar health centers from March 2022 to March 2023, categorized by housing status (owner-occupied vs rented)
A within-subjects analysis using Greenhouse-Geisser correction revealed a significant difference in the mean height, weight, and head circumference of infants at birth, 6 months, and 12 months (P<0.001). Between-groups analysis based on the results in Table 1 demonstrated the following:
Height: A significant difference was observed in the growth trajectory of mean height among infants across the three time points (birth, 6, and 12 months) based on housing status (owner-occupied vs. rented) (P=0.003).
Weight: Similarly, a significant difference was observed in the growth trajectory of mean weight among infants across the three time points based on housing status (P=0.032).
Head circumference: The trend of increasing mean head circumference across the three time points also differed significantly between owner-occupied and rented groups (P=0.047).
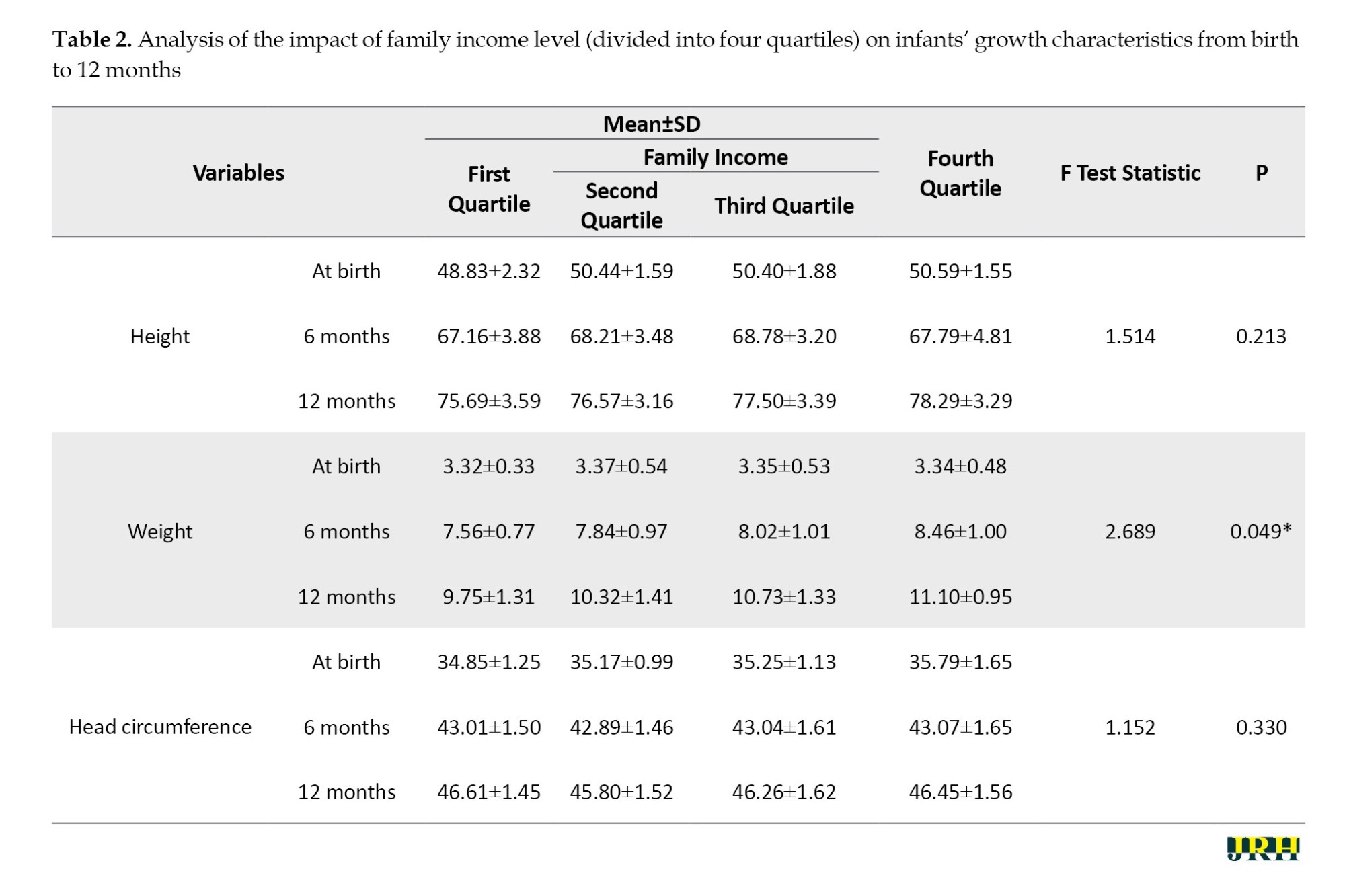
Determination of the mean anthropometric indices (height, weight, and head circumference) among children visiting health centers in Ramsar from March 2022 to March 2023, categorized by family income status
Within-group analysis: A significant difference was observed in the mean height, weight, and head circumference of infants at birth, 6 months, and 12 months based on the Greenhouse-Geisser test (P<0.001).
Between-group analysis based on Table 2:
Height: No significant difference was found in the mean height growth trend of infants across the three time points (birth, 6 months, and 12 months) based on family income quartile (P=0.213).
Weight: A significant difference was found in the mean weight growth trend of infants across the three time points (birth, 6 months, and 12 months) based on family income quartile (P=0.049).
Head circumference: No significant difference was found in the mean head circumference growth trend of infants across the three time points (birth, 6 months, and 12 months) based on family income quartile (P=0.330).
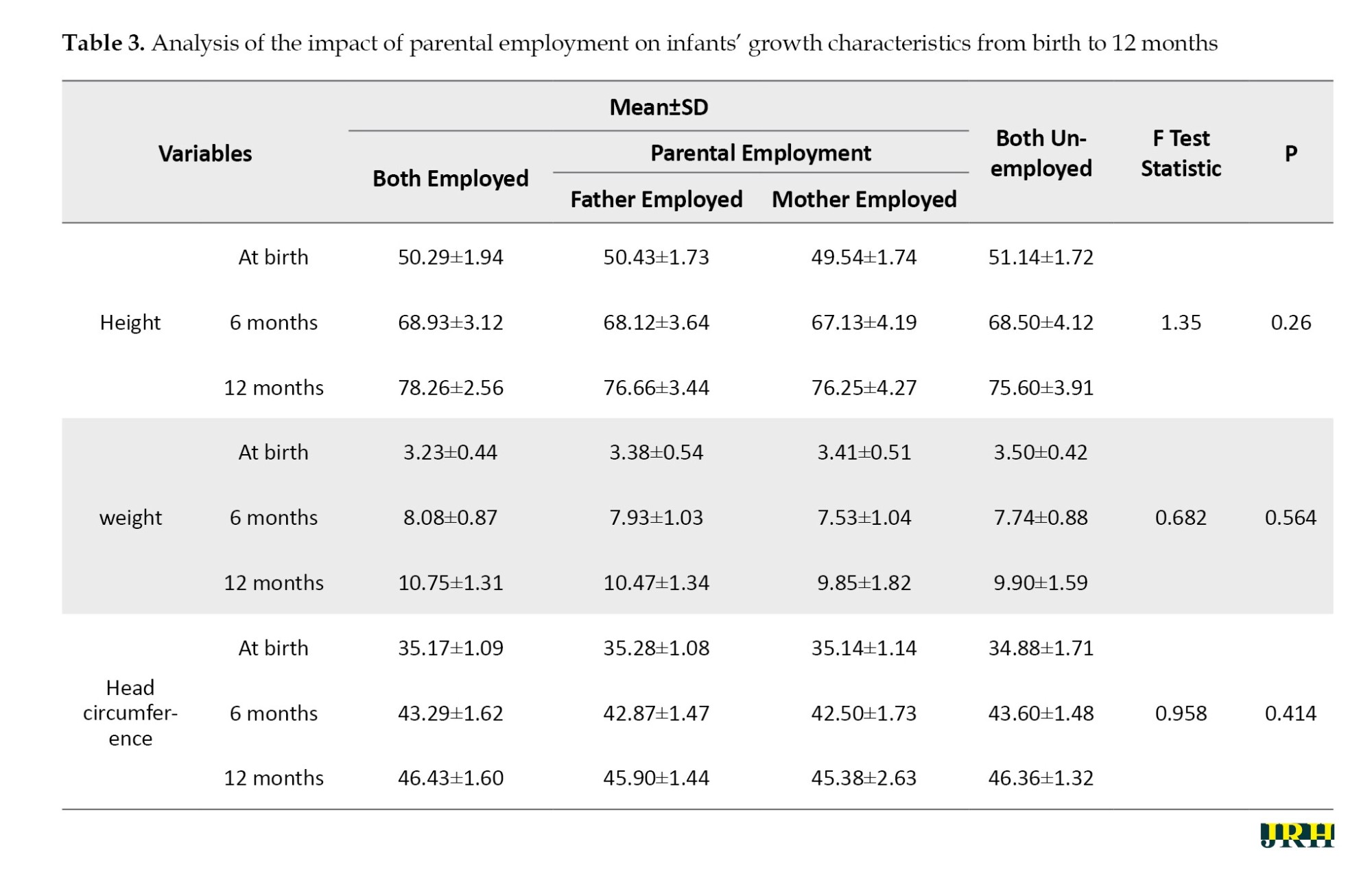
Determination of the mean anthropometric indices (height, weight, and head circumference) among children visiting health centers in Ramsar city, in March 2022 to March 2023, categorized by parental employment status
Within-group analysis: A significant difference was observed in the mean height, weight, and head circumference of infants at birth, 6 months, and 12 months based on the Greenhouse-Geisser test (P<0.001).
Between-group analysis based on Table 3:
Height: No significant difference was found in the mean height growth trend of infants across the three time points (birth, 6 months, and 12 months) based on parental employment status (both parents unemployed, father unemployed and mother employed, father employed and mother a homemaker, both parents employed) (P=0.260).
Weight: No significant difference was found in the mean weight growth trend of infants across the three time points (birth, 6 months, and 12 months) based on parental employment status (both parents unemployed, father unemployed and mother employed, father employed and mother a homemaker, both parents employed) (P=0.564).
Head circumference: No significant difference was found in the mean head circumference growth trend of infants across the three time points (birth, 6 months, and 12 months) based on parental employment status (both parents unemployed, father unemployed and mother employed, father employed and mother a homemaker, and both parents employed) (P=0.414).
Discussion
This study examined the influence of parental SES on infant growth, focusing on key anthropometric indicators—head circumference, height, and weight—measured at two intervals: birth to 6 months and 6 to 12 months. While SES variables, such as employment, housing status, and income, were analyzed, significant associations were identified only with family income and housing status. Parental employment patterns, with most fathers employed and mothers staying at home, reflected traditional family structures in Iran. Employment status did not significantly affect infant growth in this sample, aligning with mixed findings in existing research [12, 13]. Previous studies from South Asia and Africa suggest that maternal employment can negatively impact child nutrition and growth, but this often depends on factors, such as working hours, return-to-work timing, and socioeconomic conditions [14, 15]. As maternal employment rises globally, active policies, such as parental leave, can help mitigate its potential impact on early childhood development.
In the present study, significant differences were observed between children’s growth parameters and living conditions in owned and rented homes. Poor housing conditions are often associated with adverse health outcomes, and the quality, stability, and affordability of housing are directly linked to both socioemotional and physical health [16]. In a study conducted in Iran, a significant association was observed between house size and ownership and infant mortality [17]. A study in Germany showed that poor housing conditions lead to worse mental and physical health for people, including children [18].
Infants from low-income families were associated with lower birth weights, consistent with global findings [19]. Amirian et al.’s study in Iran showed health inequalities between poor and rich subgroups, which may increase the risk of morbidity and mortality among the poor [20]. Séguin et al.’s study found that inadequate household income was associated with poorer overall health and higher hospital admission rates among infants in the first 5 months of life, even after adjusting for factors affecting infant health, including maternal education level [21]. However, adequate nutrition among middle-income families may have mitigated height disparities.
Early interventions targeting low-income families are essential for promoting equitable growth and reducing health disparities. Addressing income inequality and improving access to healthcare and welfare services remain critical for fostering healthy infant development and long-term well-being [22-24].
Conclusion
The findings suggest that unfavorable parental economic status, particularly low income and housing conditions, can lead to suboptimal growth in infants during their first year of life. Improving the quality of life by improving families’ income and housing status can ultimately lead to improved general health and reduced healthcare costs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Ramsar Campus, Iran (Code: IR.MAZUMS.RIB.REC.1401.109). Throughout all stages of the research, patients’ rights were respected in accordance with ethical principles, confidentiality of their information, and adherence to the principles of the Declaration of Helsinki.
Funding
This study was financially supportedby Ramsar Campus, Mazandaran University of Medical Sciences, Iran.
Authors' contributions
study Design, managing the project, and conducting the experiments: Babak Mokhtari and Masoumeh Roodgar; Data analyzing, interpreting the results, and contributing to the final manuscript: Samaneh Farrokhfar and Babak Mokhtari; Conceptualization, methodology, formal analysis, investigation, data curation, writing the original draft, reviewing, editing, validation, supervision, and final approval: Samaneh Farrokhfar
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express ther deepest gratitude to the Ramsar Campus of Mazandaran University of Medical Science (Ramsar City, Iran). The results presented in this paper were obtained as part of a student’s dissertation.
References
The growth patterns of children during their first year of life are crucial milestones that serve as a window into their overall health, making it essential for healthcare providers to closely monitor these changes and uncover the factors influencing them. Anthropometry is a quantitative, non-invasive, and cost-effective approach to evaluating the health and growth of infants and children. By measuring various body parts, such as weight, height, head circumference, clavicle length, and femur length, physical differences can be identified, aiding in public health and clinical decision-making [1, 2]. Growth patterns are key indicators of a child’s well-being, with poverty and food insecurity linked to higher mortality rates, delayed development, disabilities, and reduced national productivity. Traditionally associated with thinness and low weight, food insecurity is increasingly associated with obesity as a marker of poor nutrition [3, 4]. The importance of early nutrition in lifelong health underpins the Developmental Origins of Health and Disease [5]. Poverty significantly contributes to malnutrition, with socioeconomic status (SES) (income, location, and housing) directly correlating with health outcomes. Improved economic conditions enhance healthcare access and influence social determinants of health, which account for over 50% of children’s health outcomes [6-9].
Parental employment also affects children’s health, particularly maternal employment, which presents a complex dynamic. While increased household income from maternal work can improve health spending, reduced maternal availability may limit the time spent on direct childcare and nutritious meal preparation, resulting in an ambiguous overall impact on child health [10, 11].
Infant growth is affected by various factors, including parental SES, and identifying and addressing the root causes of reduced growth indicators is essential for public health, health development, and correcting social imbalances. This cross-sectional study aimed to investigate the relationship between parental SES (including home ownership, income, and employment) and anthropometric changes (height, weight, and head circumference) in the first year of life in children referred to Ramsar health centers from March 2022 to March 2023 (1401 AH Iranian calendar).
Methods
A retrospective cross-sectional study was conducted to investigate the impact of household SES on infant anthropometric indices during the first year of life among children visiting health centers in Ramsar City, Iran, from March 2022 to March 2023. The inclusion criteria were full-term birth, absence of genetic disorders, and being an only child, while those with genetic and congenital diseases were excluded. This field-based study employed a checklist as a data collection tool. The checklist included information on annual income, parental employment, and home ownership. Due to the non-normal distribution of income, household incomes were categorized into four groups using Iran’s central percentile index. Concurrently, infant anthropometric indices (height, weight, and head circumference) were measured and recorded by a trained and consistent health worker using a home-based/health center study method. Changes in these variables were evaluated according to the infants’ age range. Using the Morgan table and considering that the average number of singleton births in the 5 years prior to the study in Ramsar was below 300 per year, the sample size was determined to be 148 babies. However, due to the erosive volume and unpredictability of possible sample outflows, such as migration and mortality, 180 cases were reviewed, of which 153 were eligible for the study.
Statistical analysis was performed using SPSS software, version 26 and Prism GraphPad, and appropriate statistical tests were employed in each case. Within-subject analysis was performed using the Greenhouse-Geisser correction, and the independent t-test was used to compare the means of two independent populations. The significance level was set at 0.05 (P<0.05) in all cases.
Results
The results of the present study were obtained from a retrospective review of the records of 153 eligible infants as follows: Regarding housing status, 116 families (75.8%) were homeowners, and 37 families (24.2%) were renters. The income of 16 families (10.5%) was in the first quartile, 63 families (41.2%) in the second, 60 families (39.2%) in the third, and 14 families (9.2%) in the fourth. In terms of parental employment status, 38 cases (24.8%) had both parents employed, 102 cases (66.7%) had a father employed and a stay-at-home mother, 8 cases (5.2%) had an unemployed father and an employed mother, and five cases (3.3%) had both parents unemployed.
Determining the mean of anthropometric indices (height, weight, and head circumference) among children visiting Ramsar health centers from March 2022 to March 2023, categorized by housing status (owner-occupied vs rented)
A within-subjects analysis using Greenhouse-Geisser correction revealed a significant difference in the mean height, weight, and head circumference of infants at birth, 6 months, and 12 months (P<0.001). Between-groups analysis based on the results in Table 1 demonstrated the following:
Height: A significant difference was observed in the growth trajectory of mean height among infants across the three time points (birth, 6, and 12 months) based on housing status (owner-occupied vs. rented) (P=0.003).
Weight: Similarly, a significant difference was observed in the growth trajectory of mean weight among infants across the three time points based on housing status (P=0.032).
Head circumference: The trend of increasing mean head circumference across the three time points also differed significantly between owner-occupied and rented groups (P=0.047).
Determination of the mean anthropometric indices (height, weight, and head circumference) among children visiting health centers in Ramsar from March 2022 to March 2023, categorized by family income status
Within-group analysis: A significant difference was observed in the mean height, weight, and head circumference of infants at birth, 6 months, and 12 months based on the Greenhouse-Geisser test (P<0.001).
Between-group analysis based on Table 2:
Height: No significant difference was found in the mean height growth trend of infants across the three time points (birth, 6 months, and 12 months) based on family income quartile (P=0.213).
Weight: A significant difference was found in the mean weight growth trend of infants across the three time points (birth, 6 months, and 12 months) based on family income quartile (P=0.049).
Head circumference: No significant difference was found in the mean head circumference growth trend of infants across the three time points (birth, 6 months, and 12 months) based on family income quartile (P=0.330).
Determination of the mean anthropometric indices (height, weight, and head circumference) among children visiting health centers in Ramsar city, in March 2022 to March 2023, categorized by parental employment status
Within-group analysis: A significant difference was observed in the mean height, weight, and head circumference of infants at birth, 6 months, and 12 months based on the Greenhouse-Geisser test (P<0.001).
Between-group analysis based on Table 3:
Height: No significant difference was found in the mean height growth trend of infants across the three time points (birth, 6 months, and 12 months) based on parental employment status (both parents unemployed, father unemployed and mother employed, father employed and mother a homemaker, both parents employed) (P=0.260).
Weight: No significant difference was found in the mean weight growth trend of infants across the three time points (birth, 6 months, and 12 months) based on parental employment status (both parents unemployed, father unemployed and mother employed, father employed and mother a homemaker, both parents employed) (P=0.564).
Head circumference: No significant difference was found in the mean head circumference growth trend of infants across the three time points (birth, 6 months, and 12 months) based on parental employment status (both parents unemployed, father unemployed and mother employed, father employed and mother a homemaker, and both parents employed) (P=0.414).
Discussion
This study examined the influence of parental SES on infant growth, focusing on key anthropometric indicators—head circumference, height, and weight—measured at two intervals: birth to 6 months and 6 to 12 months. While SES variables, such as employment, housing status, and income, were analyzed, significant associations were identified only with family income and housing status. Parental employment patterns, with most fathers employed and mothers staying at home, reflected traditional family structures in Iran. Employment status did not significantly affect infant growth in this sample, aligning with mixed findings in existing research [12, 13]. Previous studies from South Asia and Africa suggest that maternal employment can negatively impact child nutrition and growth, but this often depends on factors, such as working hours, return-to-work timing, and socioeconomic conditions [14, 15]. As maternal employment rises globally, active policies, such as parental leave, can help mitigate its potential impact on early childhood development.
In the present study, significant differences were observed between children’s growth parameters and living conditions in owned and rented homes. Poor housing conditions are often associated with adverse health outcomes, and the quality, stability, and affordability of housing are directly linked to both socioemotional and physical health [16]. In a study conducted in Iran, a significant association was observed between house size and ownership and infant mortality [17]. A study in Germany showed that poor housing conditions lead to worse mental and physical health for people, including children [18].
Infants from low-income families were associated with lower birth weights, consistent with global findings [19]. Amirian et al.’s study in Iran showed health inequalities between poor and rich subgroups, which may increase the risk of morbidity and mortality among the poor [20]. Séguin et al.’s study found that inadequate household income was associated with poorer overall health and higher hospital admission rates among infants in the first 5 months of life, even after adjusting for factors affecting infant health, including maternal education level [21]. However, adequate nutrition among middle-income families may have mitigated height disparities.
Early interventions targeting low-income families are essential for promoting equitable growth and reducing health disparities. Addressing income inequality and improving access to healthcare and welfare services remain critical for fostering healthy infant development and long-term well-being [22-24].
Conclusion
The findings suggest that unfavorable parental economic status, particularly low income and housing conditions, can lead to suboptimal growth in infants during their first year of life. Improving the quality of life by improving families’ income and housing status can ultimately lead to improved general health and reduced healthcare costs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Ramsar Campus, Iran (Code: IR.MAZUMS.RIB.REC.1401.109). Throughout all stages of the research, patients’ rights were respected in accordance with ethical principles, confidentiality of their information, and adherence to the principles of the Declaration of Helsinki.
Funding
This study was financially supportedby Ramsar Campus, Mazandaran University of Medical Sciences, Iran.
Authors' contributions
study Design, managing the project, and conducting the experiments: Babak Mokhtari and Masoumeh Roodgar; Data analyzing, interpreting the results, and contributing to the final manuscript: Samaneh Farrokhfar and Babak Mokhtari; Conceptualization, methodology, formal analysis, investigation, data curation, writing the original draft, reviewing, editing, validation, supervision, and final approval: Samaneh Farrokhfar
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express ther deepest gratitude to the Ramsar Campus of Mazandaran University of Medical Science (Ramsar City, Iran). The results presented in this paper were obtained as part of a student’s dissertation.
References
- Howe LD, Galobardes B, Matijasevich A, Gordon D, Johnston D, Onwujekwe O, et al. Measuring socio-economic position for epidemiological studies in low- and middle-income countries: A methods of measurement in epidemiology paper. International Journal of Epidemiology. 2012; 41(3):871-86. [DOI:10.1093/ije/dys037] [PMID]
- Casadei K, Kiel J. Anthropometric measurement. Treasure Island (FL): StatPearls Publishing; 2025. [PMID]
- O'Malley JA, Klett BM, Klein MD, Inman N, Beck AF. Revealing the prevalence and consequences of food insecurity in children with epilepsy. Journal of Community Health. 2017; 42(6):1213-9. [DOI:10.1007/s10900-017-0372-1] [PMID]
- Cook JT, Poblacion AP. Estimating the health-related costs of food insecurity and hunger. Washington: Bread for the World Institute; 2016. [Link]
- Georgieff MK. Early life nutrition and brain development: breakthroughs, challenges and new horizons. The Proceedings of the Nutrition Society. 2023; 82(2):104-12. [DOI:10.1017/S0029665122002774] [PMID]
- Cameron L, Williams J. Is the relationship between socioeconomic status and health stronger for older children in developing countries? Demography. 2009; 46(2):303-24.[DOI:10.1353/dem.0.0054] [PMID]
- Didsbury MS, Kim S, Medway MM, Tong A, McTaggart SJ, Walker AM, et al. Socio-economic status and quality of life in children with chronic disease: A systematic review. Journal of Paediatrics and Child Health. 2016; 52(12):1062-9. [DOI:10.1111/jpc.13407] [PMID]
- Siponen SM, Ahonen RS, Savolainen PH, Hämeen-Anttila KP. Children's health and parental socioeconomic factors: a population-based survey in Finland. BMC Public Health. 2011; 11:457. [DOI:10.1186/1471-2458-11-457] [PMID]
- Frasquilho D, de Matos MG, Santos T, Gaspar T, Caldas de Almeida JM. Unemployment as a source of mental distress to individuals and their family: Unemployed parents' perceptions during the economic recession. International Journal of Social Psychiatry. 2016; 62(5):477-86. [DOI:10.1177/0020764016650469] [PMID]
- Vinck J, Van Lancker W. An intersectional approach towards parental employment in families with a child with a disability: The case of Belgium. Work, Employment and Society. 2020; 34(2):228-61. [DOI:10.1177/0950017019872648]
- Milligan K, Stablie M. Child benefits, maternal employment, and children's health: Evidence from Canadian child benefit expansions. The American Economic Review. 2009; 99(2):128-32. [PMID]
- Peyman N, Oakley D. Effective contraceptive use: An exploration of theory-based influences. Health Education Research. 2009; 24(4):575-85. [DOI:10.1093/her/cyn058] [PMID]
- Pieters J, Rawlings S. Parental unemployment and child health in China. Review of Economics of the Household. 2020; 18:207-37. [DOI:10.1007/s11150-019-09457-y]
- Hosen MZ, Pulok MH, Hajizadeh M. Effects of maternal employment on child malnutrition in South Asia: An instrumental variable approach. Nutrition. 2023; 105:111851. [DOI:10.1016/j.nut.2022.111851] [PMID]
- Kopp M, Lindauer M, Garthus-Niegel S. Association between maternal employment and the child´s mental health: a systematic review with meta-analysis. European Child & Adolescent Psychiatry. 2024; 33(9):3025-42. [DOI:10.1007/s00787-023-02164-1]
- Holden KA, Lee AR, Hawcutt DB, Sinha IP. The impact of poor housing and indoor air quality on respiratory health in children. Breathe. 2023; 19(2):230058. [DOI:10.1183/20734735.0058-2023] [PMID]
- Hosseinpoor AR, Van Doorslaer E, Speybroeck N, Naghavi M, Mohammad K, Majdzadeh R, et al. Decomposing socioeconomic inequality in infant mortality in Iran. International Journal of Epidemiology. 2006; 35(5):1211-9. [DOI:10.1093/ije/dyl164] [PMID]
- Palacios J, Eichholtz P, Kok N, Aydin E. The impact of housing conditions on health outcomes. Real Estate Economics. 2021; 49(4):1172-200. [DOI:10.1111/1540-6229.12317]
- Mekonnen T, Papadopoulou E, Arah OA, Brantsæter AL, Lien N, Gebremariam MK. Socioeconomic inequalities in children's weight, height and BMI trajectories in Norway. Scientific Reports. 2021; 11(1):4979. [DOI:10.1038/s41598-021-84615-w] [PMID]
- Amirian H, Poorolajal J, Roshanaei G, Esmailnasab N, Moradi G. Analyzing socioeconomic related health inequality in mothers and children using the concentration index. Epidemiology, Biostatistics, and Public Health. 2014; 11(3):e9086. [DOI:10.2427/9086]
- Séguin L, Xu Q, Potvin L, Zunzunegui MV, Frohlich KL. Effects of low income on infant health. CMAJ: Canadian Medical Association journal. 2003; 168(12):1533-8. [PMID]
- Hagemann E, Silva DT, Davis JA, Gibson LY, Prescott SL. Developmental Origins of Health and Disease (DOHaD): The importance of life-course and transgenerational approaches. Paediatric Respiratory Reviews. 2021; 40:3-9. [DOI:10.1016/j.prrv.2021.05.005] [PMID]
- Hertzman C, Power C. Health and human development: understandings from life-course research. Developmental neuropsychology. 2003; 24(2-3):719-44. [DOI:10.4324/9781003059691-10]
- Lipkin PH, Macias MM; Council on Children With Disabilities, Section on Developmental and Behavioral Pediatrics. Promoting optimal development: identifying infants and young children with developmental disorders through developmental surveillance and screening. Pediatrics. 2020; 145(1):e20193449. [DOI:10.1542/peds.2019-3449]
Type of Study: Short Communication |
Subject:
● Service Quality
Received: 2025/01/21 | Accepted: 2025/06/25 | Published: 2026/03/1
Received: 2025/01/21 | Accepted: 2025/06/25 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
