

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 139-148 |
Back to browse issues page


Ethics code: IR.GMU.REC.1400.022
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rahmani R, Yaghoobi Moghaddam F, Mohammadzadeh F, Rostamian M. Psychometric Properties of the Persian Version of Self-care Activities Screening Scale: A Validation Study. J Research Health 2026; 16 (2) :139-148
URL: http://jrh.gmu.ac.ir/article-1-2733-en.html
URL: http://jrh.gmu.ac.ir/article-1-2733-en.html



1- Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran.
2- Department of Midwifery, Social Development and Health Promotion Research Center, Faculty of Medicine, Gonabad University of Medical Sciences, Gonabad, Iran.
3- Department of Epidemiology & Biostatistics, Social Development and Health Promotion Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran.
4- Department of English, Reproductive Health and Population Research Center, Faculty of Medicine, Gonabad University of Medical Sciences, Gonabad, Iran. ,m.rostamian.edu@gmail.com
2- Department of Midwifery, Social Development and Health Promotion Research Center, Faculty of Medicine, Gonabad University of Medical Sciences, Gonabad, Iran.
3- Department of Epidemiology & Biostatistics, Social Development and Health Promotion Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran.
4- Department of English, Reproductive Health and Population Research Center, Faculty of Medicine, Gonabad University of Medical Sciences, Gonabad, Iran. ,
Keywords: Validation, Psychometrics, Self-care activities screening scale (SASS)-14, Iran, Stressful experiences
Full-Text [PDF 827 kb]
(249 Downloads)
| Abstract (HTML) (927 Views)
Full-Text: (128 Views)
Introduction
Health is the ability to adapt and self-manage in the face of social, physical, and emotional challenges [1]. Self-care is an essential and valuable principle in today’s society because it emphasizes the active role of individuals in maintaining their health [2]. Furthermore, self-care is an emerging operational strategy for managing and preventing chronic and infectious diseases, contributing to increased energy, positive affect, stress reduction, enhanced well-being, improved self-confidence, and overall advancement of community health [3-6]. Various respiratory diseases, such as coronaviruses, threaten human health [7]. On January 30, 2020, the World Health Organization (WHO) declared an international health emergency based on information obtained from Wuhan, China, and other parts of the world [8]. Coronavirus disease (COVID-19) is a respiratory illness with symptoms ranging from mild colds to severe acute respiratory syndrome [9]. It has spread rapidly worldwide and created public health emergencies, especially in vulnerable groups [10]. The WHO considers it a global public health concern [11]. People in the community experience a wide range of symptoms of stress and mental disorders, including mood swings, insomnia, stress, anxiety, anger, irritability, emotional exhaustion, depression, and post-traumatic stress symptoms. Furthermore, low morale and irritability are particularly common [12]. However, engaging in self-care activities as part of health measures can help us control stress and prevent health problems and symptoms [13]. The self-care activities screening scale (SASS-14) was developed to assess self-care during stressful experiences, such as the COVID-19 pandemic.
The SASS-14 is a reliable and concise instrument for measuring self-care during stressful experiences, such as confinement. It can be particularly useful for rapidly assessing the promotion of health behaviors among the general population. Furthermore, it can be highly beneficial for self-care during stressful experiences, such as quarantine conditions. The SASS-14 is a short, rapidly administrable, and online-accessible questionnaire, enabling healthcare professionals to easily apply it remotely for self-care screening and the promotion of healthy behaviors [14]. By identifying individuals who could benefit most from additional physical and psychological support during complex situations like confinement, the SASS-14 can help prevent future health complications. Its brevity, rapid completion time, and online accessibility make it an ideal instrument for remote administration by healthcare professionals. This allows for convenient and widespread screening of healthy routines in both general and clinical populations, even during periods of restricted movement. This proactive approach enables more targeted interventions, optimizing resource allocation and improving public health outcomes.
Given the importance of self-care, providing self-care services can be a substantial achievement for community members. Therefore, due to the lack of an accurate and contextually relevant tool for precisely evaluating self-care behaviors, this study aimed to develop and validate the psychometric properties of the Persian version of the SASS-14.
Methods
This study was conducted in two stages: first, translating the SASS-14 from English to Persian, and second, examining its psychometric properties.
Measurements
Sociodemographic questionnaire
The checklist included several items, such as age, gender, marital status, education, occupation, place of residence, and income.
The SASS-14
The SASS-14 was originally developed by Martinez et al. (2021) [14] to screen self-care activities in the COVID-19 epidemic. This questionnaire comprises 14 items, coded on a Likert scale ranging from one (never) to six (always). The minimum and maximum possible scores of the questionnaire are 0 and 84, respectively. Higher scores indicate higher levels of self-care. The SASS-14 consists of four subscales: Health awareness (five items); nutrition and physical activity (three items); sleep quality (two items); and social support, interpersonal skills, and leisure activities (four items), encompassing personal and interpersonal coping strategies.
Satisfaction with life scale (SWLS)
This scale was developed by Diener et al. (1985) and consists of five statements that measure the cognitive component of actual well-being [15]. The psychometric properties of the Persian version of the scale were assessed by Bayani et al. (2007). Its structural validity was assessed via convergent validity using the Oxford Happiness Inventory and the Beck Depression Inventory; Cronbach’s α was 0.83, and test-re-test indicated 0.69 reliability [16].
The 36-item short-form health survey (SF-36)
This questionnaire was developed to assess the overall state of health and disability [17]. Scores range from 0 to 100, with higher scores indicating a better quality of life. The Persian version of this scale demonstrated good validity and reliability in Montazeri et al.’s 2005 study [17].
Stage 1: Translation process
The original version of SASS-14 was translated from English to Persian in several steps. In the first stage, two qualified and independent translators (a reproductive health specialist and a PhD. holder in teaching english as a foreign language [TEFL]) translated the original English version into Persian (backward translation). Next, the translations were compared and evaluated for quality, and the most appropriate phrasing was selected to achieve a single, reconciled translation. Subsequently, the final translated version was given to two other English Language Specialists, who had not observed the original English text, to perform a back-translation into English, ensuring translation accuracy. Finally, all translations and the original version were reviewed and compared by translators and authors, and the final Persian version was approved.
Stage 2: Psychometric properties
Design, participants, and sampling
Participants in this cross-sectional study were selected from the population of different towns in Iran using a convenience sampling strategy between March and November 2021. A link, including study objectives and questionnaire items, was disseminated via SMS and through relevant groups and channels on WhatsApp, Telegram, and Instagram applications. Participants completed the questionnaire if they met the inclusion criteria. They were also requested to share the questionnaire with other individuals, groups, and channels within their networks. The inclusion criteria included willingness to participate in the study, age over 18 years, literacy in reading and writing, and the absence of diagnosed mental disorders (e.g. depression, anxiety, and obsession) in recent weeks. The subject-to-item ratio method is frequently used to determine the sample size required for exploratory factor analysis (EFA) [18]. Recommendations for the subject-to-item ratio range from 2 to 20 individuals per item, with a minimum sample size of 100 to 250 suggested [18]. Moreover, literature recommendations for sample size in confirmatory factor analysis (CFA) vary from 150 to 1000 individuals [18]. In this study, based on the questionnaire’s 14 items, the minimum required sample size was 140 individuals (10 times the number of items) [19]; this was increased to 200 samples to comply with the minimum sample size recommendations. To perform EFA and CFA on separate samples, 400 samples were targeted.
Data analysis
All statistical analyses were conducted using IBM SPSS software, version 19.0 (IBM SPSS, Armonk, NY: IBM Corp.) and AMOS software, version 19.0.
Content validity
Eight health experts, one instrumentation specialist, and one clinical specialist (10 individuals in total) approved the content validity of the final Persian version. To determine the content validity ratio (CVR), a three-point Likert scale was used (necessary, useful but not necessary, not necessary). The content validity of each item was confirmed if its CVR was >0.62, according to the Lawshe Table [20]. To determine the content validity index (CVI), each expert was asked to rate the relevance, clarity, simplicity, and ambiguity of each item using a 4-point Likert scale; items with CVI>0.79 were considered appropriate.
Construct validity
The sample was randomly split into two equal subsamples (n=200 each) for cross-validation. The first subsample underwent EFA to identify the factor structure, while the second subsample was used for CFA to validate the derived structure. This approach follows established psychometric practices [21-23], serving three key purposes: mitigating overfitting, testing structural replicability, and enhancing the robustness of construct validity findings. Before performing EFA and CFA, univariate normality was assessed using the Kolmogorov–Smirnov test (with a P>0.05 indicating normality) and by examining the values of skewness and kurtosis. Multivariate normality assumptions were also tested using skewness and kurtosis values, as well as a chi-square versus Mahalanobis distance plot. Skewness and kurtosis values between -2 and +2, along with the placement of points on a straight line in the graph, indicate data normality [24]. The presence of multicollinearity was also assessed using the variance inflation factor (VIF); a VIF<3 was considered indicative of the absence of multicollinearity [25].
Data adequacy for EFA was also assessed using Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) index. Significance (P<0.05, indicating rejection of the null hypothesis) in Bartlett’s test and a KMO value above 0.7 were considered acceptable [26]. Principal component analysis and Varimax rotation were used to extract the factors. Based on the assumption that the scale is not unidimensional, four factors were extracted, consistent with the number of factors in the original version of the scale. The adequacy of the number of factors was evaluated based on eigenvalues greater than one and using scree plots.
To ensure a clear and interpretable factor structure, the EFA followed recommended guidelines regarding factor loadings. Items were considered acceptable if they had a loading of at least 0.40 on their primary factor, exhibited loadings below 0.30 on all other factors, and had at least a 0.20 difference between their highest and next highest loadings [27, 28]. CFA was conducted on the second sample based on the factors extracted from the EFA model, using maximum likelihood estimation. The model fit indices, including χ2/df, goodness-of-fit index (GFI), adjusted GFI (AGFI), comparative fit index (CFI), Tucker-Lewis Index (TLI), root mean square error of approximation (RMSEA), and normed fit index (NFI), were also evaluated.
Convergent validity
To determine convergent validity, participants completed the SASS-14, SWLS, and SF-36 concurrently. Then, the correlation coefficients between the responses of these scales were determined. Correlation coefficients were interpreted as follows: Less than 0.1, weak; between 0.1 and 0.5, moderate; between 0.5 and 0.8, strong; and greater than 0.8, very strong [29].
Reliability
The reliability of the Persian SASS-14 was assessed using Cronbach’s α coefficient and the test-re-test method, with a two-week interval, in a subsample of 30 individuals. A Cronbach’s α value between 0.6 and 0.7 indicates an acceptable level of reliability, while a value greater than or equal to 0.8 indicates good reliability [30]. Test-re-test reliability was determined using the intraclass correlation coefficient (ICC): Values greater than 0.75 were considered good reliability, between 0.5 and 0.75 moderate, and less than 0.5 poor [31].
Results
Participant characteristics
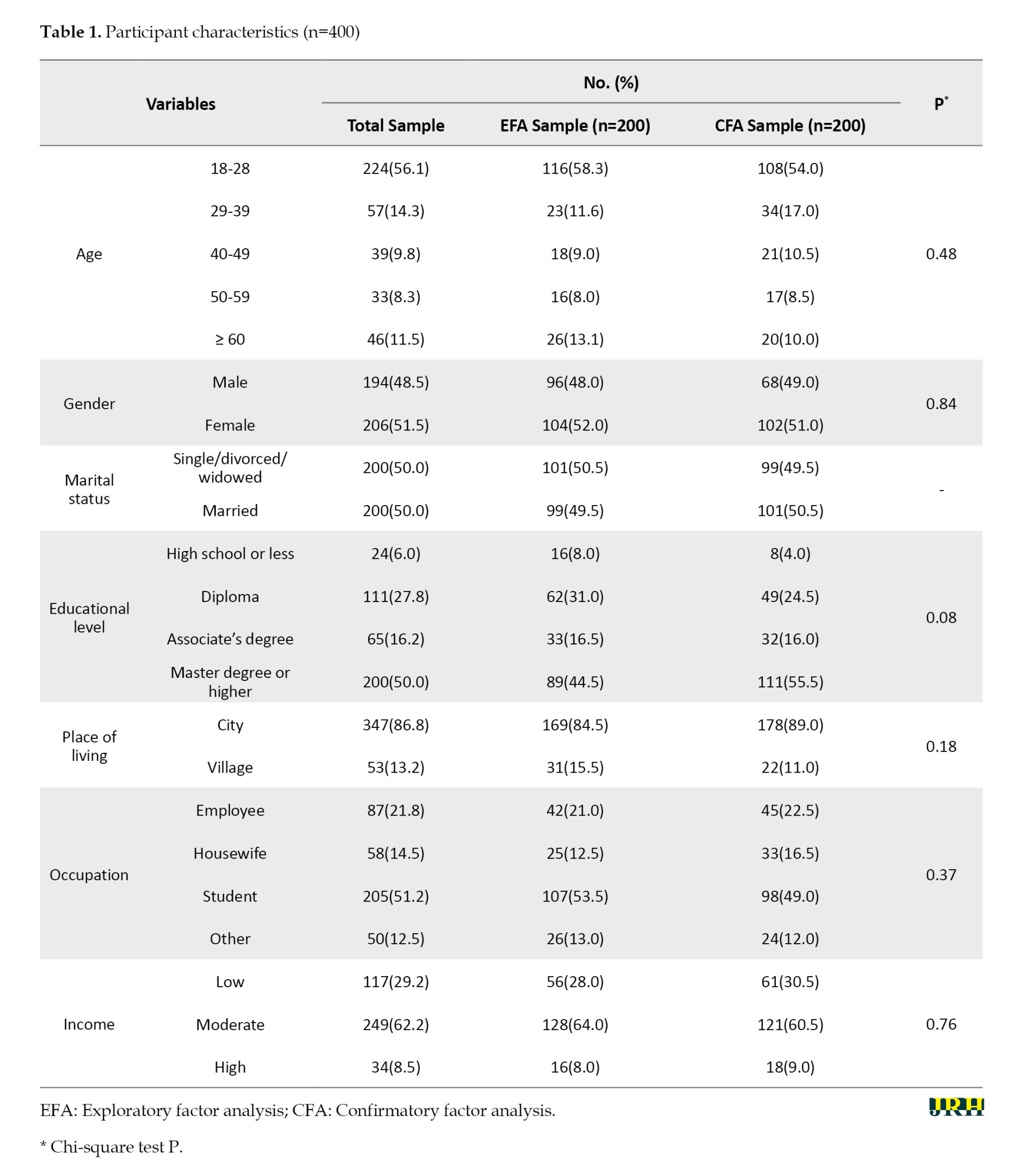
Most participants (78.2%) were from Khorasan Razavi Province, Iran, with the remaining participants representing South Khorasan (5.4%), North Khorasan (4.6%), Mazandaran (4.6%), East Azerbaijan (1.5%), Alborz (1.1%), Isfahan (1.9%), and other provinces (2.7%) in Iran. The Mean±SD age of participants was 33.18±15.76 years, with a range of 18 to 87 years; 51.5% of the participants were female. Table 1 presents participant characteristics for both EFA and CFA samples. The samples did not differ significantly in terms of individual characteristics.
Content validity
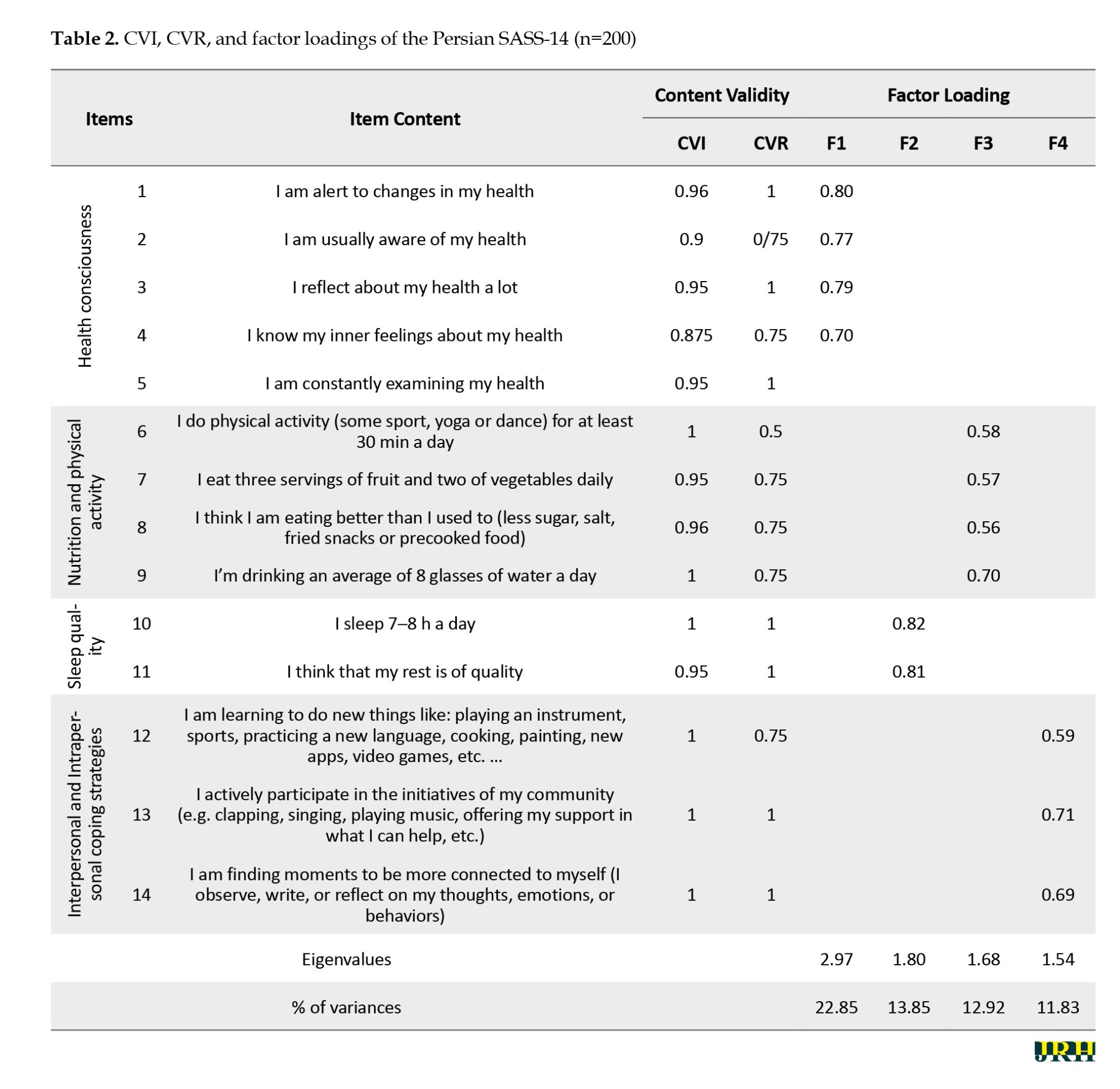
All questionnaire items obtained CVR scores greater than 0.62, based on the Lawshe Table (Table 2). The CVI value for 12 questionnaire items exceeded 0.79; only two items required revision and correction. After correction, the content validity of all 14 items was confirmed.
Construct validity
In EFA, the KMO value was 0.74, indicating sample adequacy. Bartlett’s test also yielded a significant result, indicating a relationship between items (χ2[78]=700.64, P<0.001). Thirteen items were retained in the four-factor EFA solution. Item 5 (‘I am constantly examining my health’) was removed from the analysis due to substantial cross-loading. Specifically, it loaded 0.424 on Factor 1 and 0.558 on Factor 4. Since the difference between these loadings was less than 0.20, and both loadings exceeded 0.30, the item did not meet the criteria for a simple structure and was therefore excluded to maintain the interpretability of the factor solution. The four factors with eigenvalues greater than one explained 61.45% of the variance. After Varimax rotation, the variance explained by the first through fourth factors was 22.85%, 13.85%, 12.92%, and 11.83%, respectively. Scree plots also confirmed the adequacy of the four-factor model. Factor loadings of items ranged from 0.56 to 0.82 (Table 2).
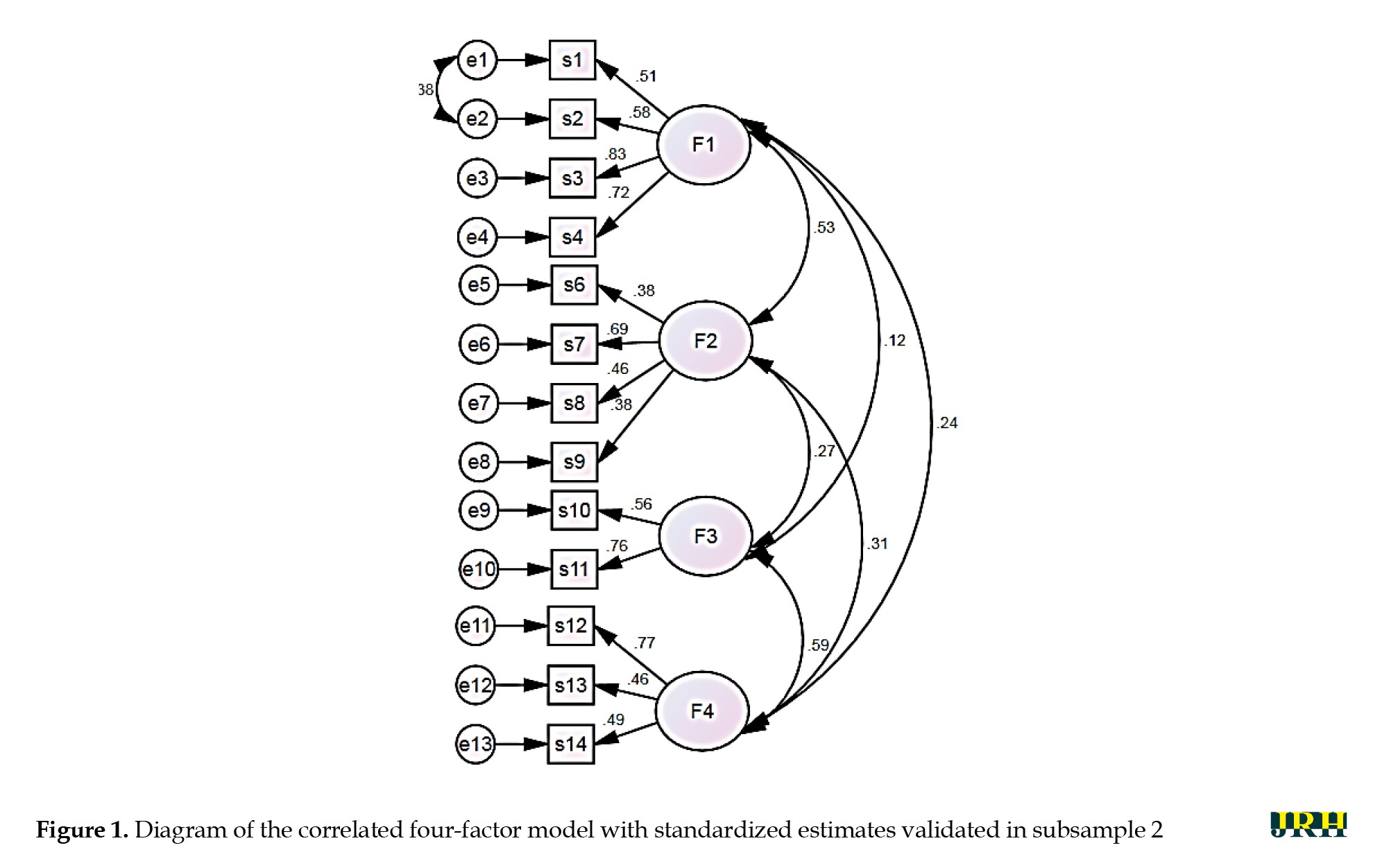
The CFA results confirmed the structure of the four-factor model with 13 items, and the model fit indices indicated that the model was sufficiently consistent with the data (Table 3).
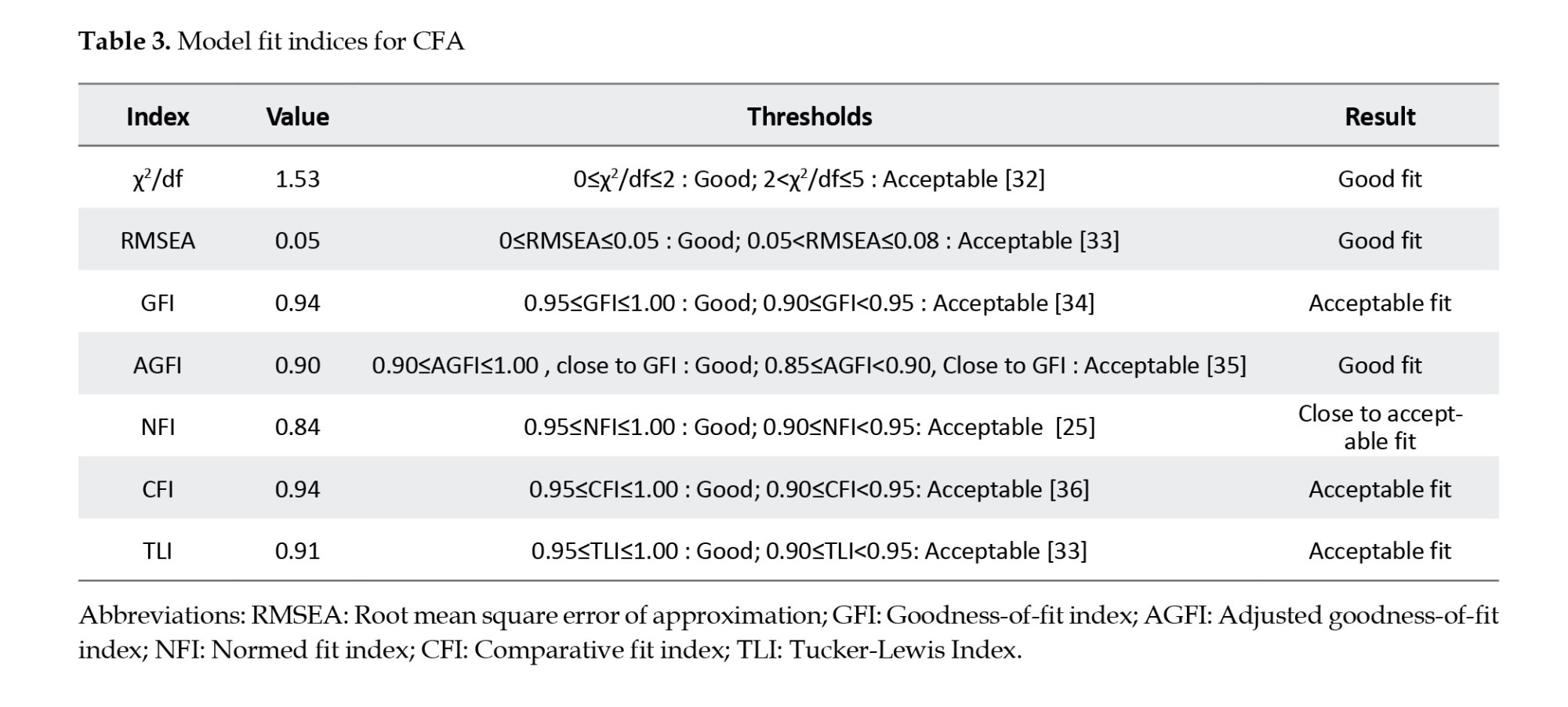
Figure 1 shows the standardized coefficients of the approved CFA model.
Convergent validity
Spearman correlation coefficients between the scores of the SASS-14 and the SF-36 (r=0.21, P<0.001), as well as the SWLS (r=0.17, P=0.001), revealed positive and significant correlations, although not strong. The ICC value in the test-re-test reliability analysis was 0.96 for the whole scale, indicating excellent stability. For the subscales, ICC values ranged from 0.60 to 0.81. Additionally, the Cronbach’s α coefficient for the whole scale was 0.70, indicating a good level of internal consistency. For the subscales, Cronbach’s α values were: Health consciousness=0.82, nutrition and physical activity=0.62, sleep quality=0.61, and interpersonal and intrapersonal coping strategies=0.61.
Discussion
Self-care is an integral part of daily life, encompassing acquired, conscious, and purposeful actions individuals take for themselves, their children, and their families to maintain health, protect mental and physical well-being, address social and psychological needs, prevent illnesses or accidents, manage chronic conditions, and protect health following acute illness or hospital discharge. Self-care clearly enhances individual efficiency and skills and is a core concept for promoting healthy behavior [37].
Self-care is especially important during an epidemic outbreak, such as the COVID-19 pandemic. Epidemics are not only a concern for physical health but also contribute to various psychological illnesses, including stress and anxiety [38]. Therefore, standardized questionnaires are needed to assess self-care behaviors in the general population, which can be particularly useful for rapidly evaluating health behaviors. Given the absence of a Persian screening questionnaire for self-care activities in the Iranian community, the present study aimed to develop and validate a Persian self-care questionnaire. The results of the present study demonstrate that the Persian version of the SASS-14 and its dimensions possess adequate validity and reliability for use in Iranian society, similar to the original scale. We did not encounter major problems in the translation and cultural adaptation process of the SASS-14, indicating that the changes made to the questionnaire were not fundamental. The CVI values for 12 items of the questionnaire exceeded 0.79, with only two items requiring revision, which were subsequently confirmed. The Cronbach’s α coefficient for the whole scale was 0.70, indicating a desirable level of internal consistency. For the subscales, Cronbach’s α values ranged from 0.61 to 0.82, also demonstrating acceptable to good reliability. Furthermore, the ICC value in the test-re-test method was 0.96, indicating good internal reliability.
It should be noted that Item 5 was deliberately removed from the factor analysis to enhance the clarity and validity of the factor structure. This item exhibited substantial loadings on two factors, with a difference of less than 0.20 between them. Such cross-loading suggests that the item does not distinctly represent a single underlying construct, thereby complicating factor interpretability. According to established guidelines, items should ideally load above 0.40 on their primary factor, below 0.30 on other factors, and exhibit at least a 0.20 difference between primary and secondary loadings to ensure a simple structure and discriminant validity [28]. Retaining items with significant cross-loadings can obscure factor distinctiveness and potentially compromise the scale’s construct validity [39]. Additionally, Items 1 (‘I am alert to changes in my health’) and 2 (‘I am usually aware of my health’) were found to be conceptually related. Both items reflect different yet closely linked aspects of health self-awareness, which is a component of health literacy and self-regulation. Specifically, Item 1 captures an individual’s vigilance and sensitivity to changes in health status (reactive monitoring), whereas Item 2 assesses a broader, more stable awareness of one’s overall health state (proactive awareness). This relationship is consistent with previous findings suggesting that health-conscious individuals are more likely to understand their health, pay close attention to personal health issues, and take proactive steps to maintain their well-being [40]. Accordingly, the decision to allow correlation of error terms between these two items was theoretically justified. In CFA, correlating residuals is warranted when items share similar content, wording, or method variance not fully explained by the latent construct [27, 32]. Since both items involve self-perception processes related to health monitoring, some residual covariance beyond the latent factor was expected. Allowing correlated errors, when supported by substantive theory rather than solely by statistical fit indices, is an accepted practice to improve model fit while preserving theoretical validity [41]. Thus, the correlation between the error terms of Items 1 and 2 reflects meaningful shared variance attributable to the close conceptual alignment of these measures, rather than a statistical artifact.
Future research should prioritize replicating these findings in more diverse international samples to ensure broader applicability. Additionally, this study did not assess the temporal stability of the SASS-14, a crucial psychometric property that warrants investigation in subsequent research. Despite the aforementioned limitations, the SASS-14 offers significant strengths and crucial clinical implications. Its utility in screening self-care activities within the general population enables proactive identification of individuals at risk of developing detrimental health behaviors and subsequent health deterioration. Secondly, its brevity, rapid completion, and online accessibility make it an exceptionally practical instrument, facilitating the prevention of future health complications and the timely identification of individuals who would most benefit from supplementary physical and psychological support during challenging circumstances. Healthcare professionals can readily administer it remotely, enabling efficient screening of healthy routines across both general and clinical populations during periods of confinement. Future research should explore the relationship between SASS-14 scores and subsequent health behaviors. Such investigations would powerfully demonstrate the tool’s predictive value, highlighting its importance as a prerequisite for fostering healthy lifestyle choices. Moreover, to achieve a comprehensive understanding of the intricate self-care process, it is imperative to evaluate the SASS-14 in conjunction with measures of interconnected self-care elements, such as self-care agency and self-care efficacy.
Conclusion
The CFA results confirmed the structure of the 13-item model, and the model fit indicators showed that the model was sufficiently consistent with the data. Likewise, Spearman correlation coefficients between the scores of the Persian SASS-14 and the SF-36 Health Survey, as well as the SWLS, revealed positive and significant results, confirming the criterion validity of the Persian questionnaire, although the correlations were not strong. Finally, EFA results demonstrated that the Persian scale corresponds to the original scale in terms of the number of items within each category, and it was not necessary to delete or replace items, which confirms the construct validity of the questionnaire. This questionnaire had not been validated in Iran previously. To validate and localize it, sampling was performed in several cities and villages across Iran, which expands the generalizability of findings to the Iranian community and reduces the need for further localization. A well-established and validated scale in a society could be used with high confidence in future studies. Measuring self-care among individuals in Iran is necessary, and the localization of this questionnaire provides an innovative solution for this purpose.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Gonabad University of Medical Sciences, Gonabad, Iran (Code: IR.GMU.REC.1400.022). The study objectives were explained to participants at the beginning of the online questionnaire, and all participants provided informed consent. Participants were also informed of their right to withdraw from the study at any point, and the confidentiality of their information was maintained. This study adhered to the ethical principles outlined in the Declaration of Helsinki.
Funding
This study was supported by a Grant-in-Aid from the Social Development and Health Promotion Research Center, affiliated with Gonabad University of Medical Sciences.
Authors' contributions
Conseptualization, drafting of the manuscript and study design: Rasol Rahmani and Fatemeh Yaghoobi Moghaddam; Statistical analysis: Fatemeh Mohammadzadeh; revising the manuscript and providing the intellectual content: Morteza Rostamian.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors are immensely grateful to the anonymous reviewers for their invaluable feedback and to the esteemed editor of the Journal of Research & Health for the expert guidance.
References
Health is the ability to adapt and self-manage in the face of social, physical, and emotional challenges [1]. Self-care is an essential and valuable principle in today’s society because it emphasizes the active role of individuals in maintaining their health [2]. Furthermore, self-care is an emerging operational strategy for managing and preventing chronic and infectious diseases, contributing to increased energy, positive affect, stress reduction, enhanced well-being, improved self-confidence, and overall advancement of community health [3-6]. Various respiratory diseases, such as coronaviruses, threaten human health [7]. On January 30, 2020, the World Health Organization (WHO) declared an international health emergency based on information obtained from Wuhan, China, and other parts of the world [8]. Coronavirus disease (COVID-19) is a respiratory illness with symptoms ranging from mild colds to severe acute respiratory syndrome [9]. It has spread rapidly worldwide and created public health emergencies, especially in vulnerable groups [10]. The WHO considers it a global public health concern [11]. People in the community experience a wide range of symptoms of stress and mental disorders, including mood swings, insomnia, stress, anxiety, anger, irritability, emotional exhaustion, depression, and post-traumatic stress symptoms. Furthermore, low morale and irritability are particularly common [12]. However, engaging in self-care activities as part of health measures can help us control stress and prevent health problems and symptoms [13]. The self-care activities screening scale (SASS-14) was developed to assess self-care during stressful experiences, such as the COVID-19 pandemic.
The SASS-14 is a reliable and concise instrument for measuring self-care during stressful experiences, such as confinement. It can be particularly useful for rapidly assessing the promotion of health behaviors among the general population. Furthermore, it can be highly beneficial for self-care during stressful experiences, such as quarantine conditions. The SASS-14 is a short, rapidly administrable, and online-accessible questionnaire, enabling healthcare professionals to easily apply it remotely for self-care screening and the promotion of healthy behaviors [14]. By identifying individuals who could benefit most from additional physical and psychological support during complex situations like confinement, the SASS-14 can help prevent future health complications. Its brevity, rapid completion time, and online accessibility make it an ideal instrument for remote administration by healthcare professionals. This allows for convenient and widespread screening of healthy routines in both general and clinical populations, even during periods of restricted movement. This proactive approach enables more targeted interventions, optimizing resource allocation and improving public health outcomes.
Given the importance of self-care, providing self-care services can be a substantial achievement for community members. Therefore, due to the lack of an accurate and contextually relevant tool for precisely evaluating self-care behaviors, this study aimed to develop and validate the psychometric properties of the Persian version of the SASS-14.
Methods
This study was conducted in two stages: first, translating the SASS-14 from English to Persian, and second, examining its psychometric properties.
Measurements
Sociodemographic questionnaire
The checklist included several items, such as age, gender, marital status, education, occupation, place of residence, and income.
The SASS-14
The SASS-14 was originally developed by Martinez et al. (2021) [14] to screen self-care activities in the COVID-19 epidemic. This questionnaire comprises 14 items, coded on a Likert scale ranging from one (never) to six (always). The minimum and maximum possible scores of the questionnaire are 0 and 84, respectively. Higher scores indicate higher levels of self-care. The SASS-14 consists of four subscales: Health awareness (five items); nutrition and physical activity (three items); sleep quality (two items); and social support, interpersonal skills, and leisure activities (four items), encompassing personal and interpersonal coping strategies.
Satisfaction with life scale (SWLS)
This scale was developed by Diener et al. (1985) and consists of five statements that measure the cognitive component of actual well-being [15]. The psychometric properties of the Persian version of the scale were assessed by Bayani et al. (2007). Its structural validity was assessed via convergent validity using the Oxford Happiness Inventory and the Beck Depression Inventory; Cronbach’s α was 0.83, and test-re-test indicated 0.69 reliability [16].
The 36-item short-form health survey (SF-36)
This questionnaire was developed to assess the overall state of health and disability [17]. Scores range from 0 to 100, with higher scores indicating a better quality of life. The Persian version of this scale demonstrated good validity and reliability in Montazeri et al.’s 2005 study [17].
Stage 1: Translation process
The original version of SASS-14 was translated from English to Persian in several steps. In the first stage, two qualified and independent translators (a reproductive health specialist and a PhD. holder in teaching english as a foreign language [TEFL]) translated the original English version into Persian (backward translation). Next, the translations were compared and evaluated for quality, and the most appropriate phrasing was selected to achieve a single, reconciled translation. Subsequently, the final translated version was given to two other English Language Specialists, who had not observed the original English text, to perform a back-translation into English, ensuring translation accuracy. Finally, all translations and the original version were reviewed and compared by translators and authors, and the final Persian version was approved.
Stage 2: Psychometric properties
Design, participants, and sampling
Participants in this cross-sectional study were selected from the population of different towns in Iran using a convenience sampling strategy between March and November 2021. A link, including study objectives and questionnaire items, was disseminated via SMS and through relevant groups and channels on WhatsApp, Telegram, and Instagram applications. Participants completed the questionnaire if they met the inclusion criteria. They were also requested to share the questionnaire with other individuals, groups, and channels within their networks. The inclusion criteria included willingness to participate in the study, age over 18 years, literacy in reading and writing, and the absence of diagnosed mental disorders (e.g. depression, anxiety, and obsession) in recent weeks. The subject-to-item ratio method is frequently used to determine the sample size required for exploratory factor analysis (EFA) [18]. Recommendations for the subject-to-item ratio range from 2 to 20 individuals per item, with a minimum sample size of 100 to 250 suggested [18]. Moreover, literature recommendations for sample size in confirmatory factor analysis (CFA) vary from 150 to 1000 individuals [18]. In this study, based on the questionnaire’s 14 items, the minimum required sample size was 140 individuals (10 times the number of items) [19]; this was increased to 200 samples to comply with the minimum sample size recommendations. To perform EFA and CFA on separate samples, 400 samples were targeted.
Data analysis
All statistical analyses were conducted using IBM SPSS software, version 19.0 (IBM SPSS, Armonk, NY: IBM Corp.) and AMOS software, version 19.0.
Content validity
Eight health experts, one instrumentation specialist, and one clinical specialist (10 individuals in total) approved the content validity of the final Persian version. To determine the content validity ratio (CVR), a three-point Likert scale was used (necessary, useful but not necessary, not necessary). The content validity of each item was confirmed if its CVR was >0.62, according to the Lawshe Table [20]. To determine the content validity index (CVI), each expert was asked to rate the relevance, clarity, simplicity, and ambiguity of each item using a 4-point Likert scale; items with CVI>0.79 were considered appropriate.
Construct validity
The sample was randomly split into two equal subsamples (n=200 each) for cross-validation. The first subsample underwent EFA to identify the factor structure, while the second subsample was used for CFA to validate the derived structure. This approach follows established psychometric practices [21-23], serving three key purposes: mitigating overfitting, testing structural replicability, and enhancing the robustness of construct validity findings. Before performing EFA and CFA, univariate normality was assessed using the Kolmogorov–Smirnov test (with a P>0.05 indicating normality) and by examining the values of skewness and kurtosis. Multivariate normality assumptions were also tested using skewness and kurtosis values, as well as a chi-square versus Mahalanobis distance plot. Skewness and kurtosis values between -2 and +2, along with the placement of points on a straight line in the graph, indicate data normality [24]. The presence of multicollinearity was also assessed using the variance inflation factor (VIF); a VIF<3 was considered indicative of the absence of multicollinearity [25].
Data adequacy for EFA was also assessed using Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) index. Significance (P<0.05, indicating rejection of the null hypothesis) in Bartlett’s test and a KMO value above 0.7 were considered acceptable [26]. Principal component analysis and Varimax rotation were used to extract the factors. Based on the assumption that the scale is not unidimensional, four factors were extracted, consistent with the number of factors in the original version of the scale. The adequacy of the number of factors was evaluated based on eigenvalues greater than one and using scree plots.
To ensure a clear and interpretable factor structure, the EFA followed recommended guidelines regarding factor loadings. Items were considered acceptable if they had a loading of at least 0.40 on their primary factor, exhibited loadings below 0.30 on all other factors, and had at least a 0.20 difference between their highest and next highest loadings [27, 28]. CFA was conducted on the second sample based on the factors extracted from the EFA model, using maximum likelihood estimation. The model fit indices, including χ2/df, goodness-of-fit index (GFI), adjusted GFI (AGFI), comparative fit index (CFI), Tucker-Lewis Index (TLI), root mean square error of approximation (RMSEA), and normed fit index (NFI), were also evaluated.
Convergent validity
To determine convergent validity, participants completed the SASS-14, SWLS, and SF-36 concurrently. Then, the correlation coefficients between the responses of these scales were determined. Correlation coefficients were interpreted as follows: Less than 0.1, weak; between 0.1 and 0.5, moderate; between 0.5 and 0.8, strong; and greater than 0.8, very strong [29].
Reliability
The reliability of the Persian SASS-14 was assessed using Cronbach’s α coefficient and the test-re-test method, with a two-week interval, in a subsample of 30 individuals. A Cronbach’s α value between 0.6 and 0.7 indicates an acceptable level of reliability, while a value greater than or equal to 0.8 indicates good reliability [30]. Test-re-test reliability was determined using the intraclass correlation coefficient (ICC): Values greater than 0.75 were considered good reliability, between 0.5 and 0.75 moderate, and less than 0.5 poor [31].
Results
Participant characteristics
Most participants (78.2%) were from Khorasan Razavi Province, Iran, with the remaining participants representing South Khorasan (5.4%), North Khorasan (4.6%), Mazandaran (4.6%), East Azerbaijan (1.5%), Alborz (1.1%), Isfahan (1.9%), and other provinces (2.7%) in Iran. The Mean±SD age of participants was 33.18±15.76 years, with a range of 18 to 87 years; 51.5% of the participants were female. Table 1 presents participant characteristics for both EFA and CFA samples. The samples did not differ significantly in terms of individual characteristics.
Content validity
All questionnaire items obtained CVR scores greater than 0.62, based on the Lawshe Table (Table 2). The CVI value for 12 questionnaire items exceeded 0.79; only two items required revision and correction. After correction, the content validity of all 14 items was confirmed.
Construct validity
In EFA, the KMO value was 0.74, indicating sample adequacy. Bartlett’s test also yielded a significant result, indicating a relationship between items (χ2[78]=700.64, P<0.001). Thirteen items were retained in the four-factor EFA solution. Item 5 (‘I am constantly examining my health’) was removed from the analysis due to substantial cross-loading. Specifically, it loaded 0.424 on Factor 1 and 0.558 on Factor 4. Since the difference between these loadings was less than 0.20, and both loadings exceeded 0.30, the item did not meet the criteria for a simple structure and was therefore excluded to maintain the interpretability of the factor solution. The four factors with eigenvalues greater than one explained 61.45% of the variance. After Varimax rotation, the variance explained by the first through fourth factors was 22.85%, 13.85%, 12.92%, and 11.83%, respectively. Scree plots also confirmed the adequacy of the four-factor model. Factor loadings of items ranged from 0.56 to 0.82 (Table 2).
The CFA results confirmed the structure of the four-factor model with 13 items, and the model fit indices indicated that the model was sufficiently consistent with the data (Table 3).
Figure 1 shows the standardized coefficients of the approved CFA model.
Convergent validity
Spearman correlation coefficients between the scores of the SASS-14 and the SF-36 (r=0.21, P<0.001), as well as the SWLS (r=0.17, P=0.001), revealed positive and significant correlations, although not strong. The ICC value in the test-re-test reliability analysis was 0.96 for the whole scale, indicating excellent stability. For the subscales, ICC values ranged from 0.60 to 0.81. Additionally, the Cronbach’s α coefficient for the whole scale was 0.70, indicating a good level of internal consistency. For the subscales, Cronbach’s α values were: Health consciousness=0.82, nutrition and physical activity=0.62, sleep quality=0.61, and interpersonal and intrapersonal coping strategies=0.61.
Discussion
Self-care is an integral part of daily life, encompassing acquired, conscious, and purposeful actions individuals take for themselves, their children, and their families to maintain health, protect mental and physical well-being, address social and psychological needs, prevent illnesses or accidents, manage chronic conditions, and protect health following acute illness or hospital discharge. Self-care clearly enhances individual efficiency and skills and is a core concept for promoting healthy behavior [37].
Self-care is especially important during an epidemic outbreak, such as the COVID-19 pandemic. Epidemics are not only a concern for physical health but also contribute to various psychological illnesses, including stress and anxiety [38]. Therefore, standardized questionnaires are needed to assess self-care behaviors in the general population, which can be particularly useful for rapidly evaluating health behaviors. Given the absence of a Persian screening questionnaire for self-care activities in the Iranian community, the present study aimed to develop and validate a Persian self-care questionnaire. The results of the present study demonstrate that the Persian version of the SASS-14 and its dimensions possess adequate validity and reliability for use in Iranian society, similar to the original scale. We did not encounter major problems in the translation and cultural adaptation process of the SASS-14, indicating that the changes made to the questionnaire were not fundamental. The CVI values for 12 items of the questionnaire exceeded 0.79, with only two items requiring revision, which were subsequently confirmed. The Cronbach’s α coefficient for the whole scale was 0.70, indicating a desirable level of internal consistency. For the subscales, Cronbach’s α values ranged from 0.61 to 0.82, also demonstrating acceptable to good reliability. Furthermore, the ICC value in the test-re-test method was 0.96, indicating good internal reliability.
It should be noted that Item 5 was deliberately removed from the factor analysis to enhance the clarity and validity of the factor structure. This item exhibited substantial loadings on two factors, with a difference of less than 0.20 between them. Such cross-loading suggests that the item does not distinctly represent a single underlying construct, thereby complicating factor interpretability. According to established guidelines, items should ideally load above 0.40 on their primary factor, below 0.30 on other factors, and exhibit at least a 0.20 difference between primary and secondary loadings to ensure a simple structure and discriminant validity [28]. Retaining items with significant cross-loadings can obscure factor distinctiveness and potentially compromise the scale’s construct validity [39]. Additionally, Items 1 (‘I am alert to changes in my health’) and 2 (‘I am usually aware of my health’) were found to be conceptually related. Both items reflect different yet closely linked aspects of health self-awareness, which is a component of health literacy and self-regulation. Specifically, Item 1 captures an individual’s vigilance and sensitivity to changes in health status (reactive monitoring), whereas Item 2 assesses a broader, more stable awareness of one’s overall health state (proactive awareness). This relationship is consistent with previous findings suggesting that health-conscious individuals are more likely to understand their health, pay close attention to personal health issues, and take proactive steps to maintain their well-being [40]. Accordingly, the decision to allow correlation of error terms between these two items was theoretically justified. In CFA, correlating residuals is warranted when items share similar content, wording, or method variance not fully explained by the latent construct [27, 32]. Since both items involve self-perception processes related to health monitoring, some residual covariance beyond the latent factor was expected. Allowing correlated errors, when supported by substantive theory rather than solely by statistical fit indices, is an accepted practice to improve model fit while preserving theoretical validity [41]. Thus, the correlation between the error terms of Items 1 and 2 reflects meaningful shared variance attributable to the close conceptual alignment of these measures, rather than a statistical artifact.
Future research should prioritize replicating these findings in more diverse international samples to ensure broader applicability. Additionally, this study did not assess the temporal stability of the SASS-14, a crucial psychometric property that warrants investigation in subsequent research. Despite the aforementioned limitations, the SASS-14 offers significant strengths and crucial clinical implications. Its utility in screening self-care activities within the general population enables proactive identification of individuals at risk of developing detrimental health behaviors and subsequent health deterioration. Secondly, its brevity, rapid completion, and online accessibility make it an exceptionally practical instrument, facilitating the prevention of future health complications and the timely identification of individuals who would most benefit from supplementary physical and psychological support during challenging circumstances. Healthcare professionals can readily administer it remotely, enabling efficient screening of healthy routines across both general and clinical populations during periods of confinement. Future research should explore the relationship between SASS-14 scores and subsequent health behaviors. Such investigations would powerfully demonstrate the tool’s predictive value, highlighting its importance as a prerequisite for fostering healthy lifestyle choices. Moreover, to achieve a comprehensive understanding of the intricate self-care process, it is imperative to evaluate the SASS-14 in conjunction with measures of interconnected self-care elements, such as self-care agency and self-care efficacy.
Conclusion
The CFA results confirmed the structure of the 13-item model, and the model fit indicators showed that the model was sufficiently consistent with the data. Likewise, Spearman correlation coefficients between the scores of the Persian SASS-14 and the SF-36 Health Survey, as well as the SWLS, revealed positive and significant results, confirming the criterion validity of the Persian questionnaire, although the correlations were not strong. Finally, EFA results demonstrated that the Persian scale corresponds to the original scale in terms of the number of items within each category, and it was not necessary to delete or replace items, which confirms the construct validity of the questionnaire. This questionnaire had not been validated in Iran previously. To validate and localize it, sampling was performed in several cities and villages across Iran, which expands the generalizability of findings to the Iranian community and reduces the need for further localization. A well-established and validated scale in a society could be used with high confidence in future studies. Measuring self-care among individuals in Iran is necessary, and the localization of this questionnaire provides an innovative solution for this purpose.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Gonabad University of Medical Sciences, Gonabad, Iran (Code: IR.GMU.REC.1400.022). The study objectives were explained to participants at the beginning of the online questionnaire, and all participants provided informed consent. Participants were also informed of their right to withdraw from the study at any point, and the confidentiality of their information was maintained. This study adhered to the ethical principles outlined in the Declaration of Helsinki.
Funding
This study was supported by a Grant-in-Aid from the Social Development and Health Promotion Research Center, affiliated with Gonabad University of Medical Sciences.
Authors' contributions
Conseptualization, drafting of the manuscript and study design: Rasol Rahmani and Fatemeh Yaghoobi Moghaddam; Statistical analysis: Fatemeh Mohammadzadeh; revising the manuscript and providing the intellectual content: Morteza Rostamian.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors are immensely grateful to the anonymous reviewers for their invaluable feedback and to the esteemed editor of the Journal of Research & Health for the expert guidance.
References
- Huber M, Knottnerus JA, Green L, van der Horst H, Jadad AR, Kromhout D, et al. How should we define health? BMJ. 2011; 343:d4163. [DOI:10.1136/bmj.d4163] [PMID]
- El Osta A, Webber D, Gnani SL, Banarsee R, Mummery D, Majeed A, et al. The self-care matrix: a unifying framework for self-care. SelfCare. 2019; 10(3):38-56. [Link]
- Novak LL, Unertl KM, Holden RJ. Realizing the potential of patient engagement: Designing IT to support health in everyday life. Studies in Health Technology and Informatics. 2016; 222:237-47. [PMID]
- Riegel B, Dickson VV, Faulkner KM. The situation-specific theory of heart failure self-care: revised and updated. Journal of Cardiovascular Nursing. 2016; 31(3):226-35. [DOI:10.1097/JCN.0000000000000244] [PMID]
- Srinivas P, Cornet V, Holden R. Human factors analysis, design, and evaluation of Engage, a consumer health IT application for geriatric heart failure self-care. International Journal of Human–Computer Interaction. 2017; 33(4):298-312. [DOI:10.1080/10447318.2016.1265784] [PMID]
- Valdez RS, Holden RJ. Healthcare human factors/ergonomics fieldwork in home and community settings. Ergonomics in Design. 2016; 24(4):4-9 [DOI:10.1177/1064804615622111] [PMID]
- Fauci AS, Lane HC, Redfield RR. COVID-19-navigating the uncharted. The New England Journal of Medicine. 2020; 382(13):1268-9. [DOI:10.1056/NEJMe2002387] [PMID]
- Velavan TP, Meyer CG. The COVID-19 epidemic. Tropical Medicine & International Health. 2020; 25(3):278-80. [DOI:10.1111/tmi.13383] [PMID]
- Flesia L, Monaro M, Mazza C, Fietta V, Colicino E, Segatto B, et al. Predicting perceived stress related to the Covid-19 outbreak through stable psychological traits and machine learning models. Journal of Clinical Medicine. 2020; 9(10):3350. [DOI:10.3390/jcm9103350] [PMID]
- Dashraath P, Wong JLJ, Lim MXK, Lim LM, Li S, Biswas A, et al. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. American Journal of Obstetrics & Gynecology. 2020; 222(6):521-31. [DOI:10.1016/j.ajog.2020.03.021] [PMID]
- WHO. Mental health and psychosocial considerations during the COVID-19 outbreak. Geneva: World Health Organization; 2020. [Link]
- Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet. 2020; 395(10227):912-20. [DOI:10.1016/S0140-6736(20)30460-8] [PMID]
- Gibson Miller J, Hartman TK, Levita L, Martinez AP, Mason L, McBride O, et al. Capability, opportunity, and motivation to enact hygienic practices in the early stages of the COVID-19 outbreak in the United Kingdom. British Journal of Health Psychology. 2020; 25(4):856-64. [DOI:10.1111/bjhp.12426] [PMID]
- Martinez M, Luis EO, Oliveros EY, Fernandez-Berrocal P, Sarrionandia A, Vidaurreta M, et al. Validity and reliability of the Self-Care Activities Screening Scale (SASS-14) during COVID-19 lockdown. Health and Quality of life Outcomes. 2021; 19(1):1. [DOI:10.1186/s12955-020-01607-6] [PMID]
- Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. Journal of personality assessment. 1985; 49(1):71-5. [DOI:10.1207/s15327752jpa4901_13] [PMID]
- Bayani AA, Koocheky AM, Goodarzi H. [The reliability and validity of the satisfaction with life scale (Persian)]. Journal of Iranian Psychologists. 2007; 3(11):259-65. [Link]
- Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): Translation and validation study of the Iranian version. Quality of life research. 2005; 14(3):875-82. [DOI:10.1007/s11136-004-1014-5] [PMID]
- Anthoine E, Moret L, Regnault A, Sebille V, Hardouin JB. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health and Quality of Life Outcomes. 2014; 12:176. [DOI:10.1186/s12955-014-0176-2] [PMID]
- Bujang MA, Ghani PA, Soelar SA, Zulkifli NA. Sample size guideline for exploratory factor analysis when using small sample: Taking into considerations of different measurement scales. paper presented: International Conference on Statistics in Science, Business and Engineering. 10-12 Sept 2012; Langkawi, Malaysia. [DOI:10.1109/ICSSBE.2012.6396605]
- Lawshe CH. A quantitative approach to content validity. Personnel Psychology. 2006; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
- Byrne BM. Structural equation modeling with mplus: Basic concepts, applications, and programming. 1th ed. New York: routledge; 2013. [DOI:10.4324/9780203807644]
- Kyriazos TA. Applied psychometrics: The 3-faced construct validation method, a routine for evaluating a factor structure. Psychology. 2018; 9(8):2044-72 [DOI:10.4236/psych.2018.98117]
- Thompson B. The pivotal role of replication in psychological research: Empirically evaluating the replicability of sample results. Journal of Personality. 2006; 62(2):157-76. [DOI:10.1111/j.1467-6494.1994.tb00289.x]
- Burdenski T. Evaluating univariate, bivariate, and multivariate normality using graphical and statistical procedures. Multiple Linear Regression Viewpoints. 2000; 26(2):15-28. [Link]
- Hair JF Jr., Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. Cengage Learning; 2018. [DOI:10.1201/9781351076467]
- Watkins MW. Exploratory factor analysis: A guide to best practice. Journal of Black Psychology. 2018; 44(3):219-46. [DOI:10.1177/0095798418771807]
- Brown TA. Confirmatory factor analysis for applied research. 2th ed. New York: Guilford Publications; 2015. [Link]
- Howard MC. A review of exploratory factor analysis decisions and overview of current practices: What we are doing and how can we improve? International Journal of Human-Computer Interaction. 2015; 32(1):51-62. [DOI:10.1080/10447318.2015.1087664]
- Muijs D. Doing quantitative research in education with SPSS. 2th ed. Thousand Oaks: Sage Publications; 2011. [DOI:10.4135/9781849203241]
- Hulin C, Netemeyer RG, Cudeck R. Can a reliability coefficient be too high? Journal of Consumer Psychology. 2001; 10(1):55-8. [DOI:10.1207/S15327663JCP1001&2_05]
- Kuehl KS, Jones KR. Foundations of Clinical Research: Applications to Practice. Prentice Hall Health; 2000. [DOI:10.1016/B978-0-13-018722-8.X5000-0]
- Byrne BM. Structural equation modeling with AMOS: Basic concepts, applications, and programming. 3th ed. New York: Routledge; 2016. [DOI:10.4324/9781315757421]
- Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods of Psychological Research Online. 2003; 8(2):23-74. [Link]
- Marsh HW, Balla JR, McDonald RP. Goodness-of-fit indexes in confirmatory factor analysis: The effect of sample size. Psychological Bulletin. 1988; 103(3):391-410. [DOI:10.1037/0033-2909.103.3.391]
- Doll WJ, Xia W, Torkzadeh G. A confirmatory factor analysis of the end-user computing satisfaction instrument. MIS Quarterly. 1994; 18(4):453-61. [DOI:10.2307/249524]
- Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999; 6(1):1-55 [DOI:10.1080/10705519909540118]
- Rafieifar S. [Executive instruction of the national self-care program]. Tehran: Sculpture Publishing; 2015.
- Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open. 2020; 3(3):e203976. [DOI:10.1001/jamanetworkopen.2020.3976] [PMID]
- Matsunaga M. How to factor-analyze your data right: do’s, don’ts, and how-to’s. International Journal of Psychological Research. 2010; 3(1):97-110. [DOI:10.21500/20112084.854]
- Pu B, Zhang L, Tang Z, Qiu Y. The relationship between health consciousness and home-based exercise in China during the COVID-19 pandemic. International Journal of Environmental Research and Public Health. 2020; 17(16):5693. [DOI:10.3390/ijerph17165693] [PMID]
- MacCallum RC, Roznowski M, Necowitz LB. Model modifications in covariance structure analysis: The problem of capitalization on chance. Psychological Bulletin. 1992; 111(3):490-504. [DOI:10.1037/0033-2909.111.3.490] [PMID]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2025/01/26 | Accepted: 2025/06/25 | Published: 2026/03/1
Received: 2025/01/26 | Accepted: 2025/06/25 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
