

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 159-170 |
Back to browse issues page



Ethics code: KEC.2024.03C10
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Billieux J, Batthyany K, Saadati N, Rostami M, Wilson A, Longo V et al . Chronic Pain Management Experiences in Immigrant Populations: A Qualitative Study. J Research Health 2026; 16 (2) :159-170
URL: http://jrh.gmu.ac.ir/article-1-2772-en.html
URL: http://jrh.gmu.ac.ir/article-1-2772-en.html
Joel Billieux1 

 , Karina Batthyany2 , Nadereh Saadati3 , Mehdi Rostami4 , Abbie Wilson5 , Veronica Longo6 , Bridget Abalorio7
, Karina Batthyany2 , Nadereh Saadati3 , Mehdi Rostami4 , Abbie Wilson5 , Veronica Longo6 , Bridget Abalorio7
, Karina Batthyany2 , Nadereh Saadati3 , Mehdi Rostami4 , Abbie Wilson5 , Veronica Longo6 , Bridget Abalorio7
1- Institute for Behavioural Addictions, Sigmund Freud University, Vienna, Austria.
2- Department of Psychology, Queen’s University, Kingston, Canada.
3- Department of Psychology and Counseling, KMAN Research Institute, Richmond Hill, Canada. & Department of Rehabilitation, York Rehab Clinic, Toronto, Canada. ,nsaadati@kmanresce.ca
4- Department of Psychology and Counseling, KMAN Research Institute, Richmond Hill, Canada & Department of Rehabilitation, York Rehab Clinic, Toronto, Canada
5- Department of Psychology, Clark University, Worcester, USA.
6- Department of Rehabilitation, York Rehab Clinic, Toronto, Canada.
7- Department of Clinical Psychology, Faculty of Psychology, Peruvian University of Applied Sciences, Lima, Peru.
2- Department of Psychology, Queen’s University, Kingston, Canada.
3- Department of Psychology and Counseling, KMAN Research Institute, Richmond Hill, Canada. & Department of Rehabilitation, York Rehab Clinic, Toronto, Canada. ,
4- Department of Psychology and Counseling, KMAN Research Institute, Richmond Hill, Canada & Department of Rehabilitation, York Rehab Clinic, Toronto, Canada
5- Department of Psychology, Clark University, Worcester, USA.
6- Department of Rehabilitation, York Rehab Clinic, Toronto, Canada.
7- Department of Clinical Psychology, Faculty of Psychology, Peruvian University of Applied Sciences, Lima, Peru.
Full-Text [PDF 653 kb]
(192 Downloads)
| Abstract (HTML) (821 Views)
Full-Text: (132 Views)
Introduction
Chronic pain is a complex, long-lasting condition that affects physical functioning, emotional well-being, and overall quality of life. Defined as pain persisting for more than three months, it is increasingly recognized as a biopsychosocial phenomenon, shaped not only by biological injury or dysfunction but also by psychological and sociocultural dynamics [1, 2]. This conceptual shift is particularly relevant to immigrant populations, who experience chronic pain differently than the general population because of migration-related stressors, cultural norms, systemic inequities, and barriers to healthcare [3]. It affects nearly one in five adults worldwide. It occurs 1.5 to 2 times more frequently among immigrants due to migration-related stressors, acculturation challenges, and systemic inequities. It is increasingly recognized as a biopsychosocial phenomenon, shaped not only by biological injury or dysfunction but also by psychological and sociocultural dynamics [1-3]. This conceptual shift is particularly relevant to immigrant populations, whose experiences of chronic pain differ markedly from those of the general population because of cultural norms, discrimination, and structural barriers to healthcare. With global migration accelerating—over 280 million people now live outside their country of origin—and the rising prevalence of chronic pain, understanding its cultural and systemic dimensions among immigrants has become a pressing public health priority [4, 5].
Epidemiological studies show disproportionately high rates of chronic pain among immigrants, particularly those with refugee or precarious migration status [6]. These disparities stem from cumulative trauma exposure, socioeconomic disadvantage, and ongoing marginalization [7]. Migration-related factors—such as language limitations, differing cultural health beliefs, and unfamiliarity with host-country healthcare systems—often compound these risks [8]. Chronic pain has also been documented among younger immigrants, including children and adolescents, indicating that long-term health inequities begin early [3].
Pain management is challenging even within well-structured healthcare systems, but immigration compounds these difficulties through cultural incongruence, discrimination, and identity negotiation. For example, immigrants from the Middle East and North Africa are especially vulnerable to chronic musculoskeletal pain, yet often lack culturally responsive treatment options [9]. These vulnerabilities arise from pre-migration trauma, cultural variations in pain expression, and misalignment between traditional explanatory models (e.g. spiritual or moral framing) and Western biomedical paradigms [10]. Qualitative research also suggests that differences in interoceptive awareness—how individuals perceive internal bodily states—can affect symptom interpretation and coping responses [11].
Despite these insights, the literature on immigrant chronic pain remains fragmented, often leaning toward biomedical and psychiatric frameworks while overlooking how cultural beliefs and systemic barriers intersect. For instance, some studies focus on resilience and psychological adaptation—self-efficacy, ego strength, and personality traits, such as neuroticism or perfectionism—which influence vulnerability to pain-related distress [12-14]. Cognitive patterns, such as catastrophizing and helplessness, are also implicated in worsening pain outcomes, and these may be intensified by the migration experience [10, 15]. Acceptance and commitment therapy (ACT), for example, has been found effective in enhancing psychological flexibility and pain tolerance [2, 16]; however, the extent to which such interventions are culturally adapted for immigrant patients remains unclear.
Another critical gap involves system-level inequities. Immigrants frequently describe healthcare systems as “chaotic,” requiring navigation skills many do not possess [17]. This “navigation burden” includes language proficiency, health literacy, and advocacy skills; lacking these can result in delayed or foregone treatment [18, 19]. Fear of discrimination or legal repercussions further discourages timely help-seeking, while perceived stereotyping by providers erodes trust [8]. The COVID-19 pandemic worsened these barriers by disrupting access, intensifying pain symptoms, and increasing mental health strain among immigrants [20]. Many turned to community-based coping, such as family support and ethno-cultural healing practices, underscoring resilience but also revealing systemic service gaps [21].
Gendered experiences require particular attention. Women immigrants often shoulder dual burdens—managing pain while fulfilling caregiving and cultural expectations—which can lead to emotional isolation and pain silencing [8, 22]. Religious or moral interpretations of pain, such as seeing it as a divine test, may reinforce endurance but delay medical intervention [13, 23]. Conversely, some men minimize or suppress pain to maintain perceived roles as providers [4]. These gendered narratives highlight the importance of contextually sensitive qualitative approaches that capture how social roles and cultural identity shape pain expression and care engagement.
Meanwhile, resilience and culturally congruent coping strategies are central in immigrant communities. Religious rituals, family advice, and traditional medicine can help regulate emotions and preserve hope [24]. Yet these approaches sometimes delay evidence-based interventions, creating tension between culturally meaningful practices and clinical effectiveness [19, 25]. Thus, exploring how immigrants negotiate between these worlds is critical for developing integrative pain management models that respect cultural frameworks while maintaining clinical rigor.
Despite growing scholarship, there remains a substantial knowledge gap: few studies deeply examine how immigrant adults actively make sense of and cope with chronic pain while engaging with healthcare in an urban Canadian setting. Existing work rarely investigates how cultural identity, familial obligations, spirituality, and systemic barriers converge to shape help-seeking and self-care [3, 7]. Richmond Hill, Ontario, offers an ideal context for such exploration due to its highly diverse immigrant population and complex healthcare landscape. Richmond Hill, Ontario, offers an ideal context for such exploration, being one of Canada’s most diverse municipalities—home to over 70% visible minorities and more than 55% immigrants, predominantly from Asia and the Middle East [11]. This unique demographic composition provides a rich landscape for examining cross-cultural experiences of pain within a multicultural healthcare environment.
Understanding these dynamics is essential for designing culturally attuned, accessible, and patient-centered pain interventions that respond to the real contexts. Therefore, this study aimed to explore the lived experiences of chronic pain management among immigrant adults in Richmond Hill, Canada. By centering immigrants’ voices, it aims to uncover how cultural interpretations, coping patterns, and systemic inequities interact to influence pain trajectories and care engagement.
Methods
Study design and participants
This study employed a qualitative descriptive-phenomenological design to explore the lived experiences of chronic pain management among immigrant adults. The approach was chosen to capture participants’ subjective meanings, cultural interpretations, and contextual barriers in depth. In keeping with phenomenological rigor, the analytic process was guided by Husserlian principles, employing epoché or bracketing to suspend researchers’ preconceptions and remain focused on participants’ lived meanings as they naturally emerged. The goal was to describe the essence of the phenomenon rather than interpret it through theoretical bias, thereby ensuring alignment with descriptive phenomenology’s philosophical underpinnings. The study was conducted in Richmond Hill, Ontario, Canada, in 2024, an urban area with one of the country’s most ethnoculturally diverse populations.
A purposive maximum-variation sampling strategy was used to ensure diversity regarding age, gender, country of origin, type and duration of pain, and length of residence in Canada. Individuals were eligible if they:
Self-identified as immigrants; were 30 years or older (reflecting reviewer recommendations and the chronic pain onset pattern); had lived with chronic pain for at least six months; could communicate in English (to ensure rich narratives and reduce translation bias), and were willing to share their experiences in a one-on-one interview setting.
While English fluency was required to maintain narrative richness and minimize translation bias, this criterion inevitably excluded some non-English-speaking immigrants. To address this limitation prospectively, the study acknowledges the need for future expansions to multilingual facilitation through trained bilingual interviewers or translated instruments. This adjustment would enhance inclusivity while maintaining the narrative depth demonstrated in pilot interviews that informed the present study’s design.
Participants were recruited through community organizations, immigrant support groups, and healthcare providers using flyers and word-of-mouth. Sampling continued until theoretical saturation was reached—that is, when no new codes or themes emerged after iterative analysis. The final sample consisted of 26 participants representing diverse cultural and migration backgrounds.
Data collection tool
Semi-structured interview: Data were collected between February and June 2024 using in-depth, semi-structured interviews conducted either face-to-face in community settings (e.g. cultural centers, local clinics) or via secure video conferencing when preferred for convenience or safety.
A pilot-tested interview guide, informed by previous literature on immigrant chronic pain and refined after initial interviews, ensured conceptual coverage and cultural sensitivity. Key domains included:
Personal narratives of chronic pain; cultural and spiritual interpretations of pain; coping and self-management strategies; healthcare-seeking behaviors and systemic barriers, and experiences with trust, discrimination, and provider communication.
Each interview lasted 45–75 minutes and was audio-recorded with explicit, culturally sensitive informed consent. Consent procedures included plain-language explanations, opportunities for questions, and assurances regarding confidentiality and non-impact on immigration status. The interviewer maintained reflexive field notes to document contextual cues and nonverbal expressions, enriching data interpretation. All interviews were transcribed verbatim and de-identified.
Data analysis
Data were analyzed using Braun and Clarke’s six-phase thematic analysis framework: 1) Familiarization, 2) generating initial codes, 3) searching for themes, 4) reviewing themes, 5) defining and naming themes, and 6) reporting. Coding was inductive and iterative, grounded in participants’ narratives while also guided by emerging conceptual insights.
Transcripts were imported into NVivo software, version 14 for systematic coding and data management. Two researchers independently coded a subset of transcripts to ensure coder agreement, and differences were resolved through discussion and consensus. Inter-coder reliability was quantified, achieving approximately 85% initial agreement on 20% of transcripts before reconciliation, providing empirical support for analytic consistency and rigor. Reflexivity was maintained through analytic memos documenting the researcher’s positionality and potential biases.
To enhance trustworthiness, we incorporated:
Peer debriefing with experienced qualitative researchers to validate interpretations; member checking by sharing synthesized themes with participants willing to review them, and Maintaining an audit trail of coding decisions and theme refinements.
Saturation was confirmed when successive interviews yielded no new codes or conceptual insights, demonstrating that key aspects of participants’ lived experiences had been comprehensively captured.
Results
This study included 26 immigrant adults living in Richmond Hill, Ontario, all aged 30–45 years (mean=37.4). Although eligibility was set at ≥30 years, the observed range reflected emergent saturation among younger to mid-adulthood participants in the recruitment pool, suggesting that data sufficiency was reached before enrolling older individuals. Seventeen participants were women (65%) and nine were men (35%). Countries of origin included Iran (n=6), India (n=5), China (n=4), Pakistan (n=3), the Philippines (n=3), Syria (n=2), Nigeria (n=2), and Afghanistan (n=1). Sixteen participants (62%) had resided in Canada for more than five years, while ten (38%) had lived in the country for fewer than five years. Chronic pain conditions included musculoskeletal pain (n=9), fibromyalgia (n=6), neuropathic pain (n=5), chronic back pain (n=4), and migraine or chronic headache (n=2). Twelve participants (46%) were unemployed due to pain-related disability, six (23%) were employed part-time, five (19%) worked full-time, and three (12%) were homemakers. Educational backgrounds ranged from primary to post-secondary: 11 participants (42%) held a university degree, nine (35%) completed high school, and six (23%) had less than a high school education. Most (81%) lacked private insurance and relied on public health coverage or personal savings for care (Table 1).
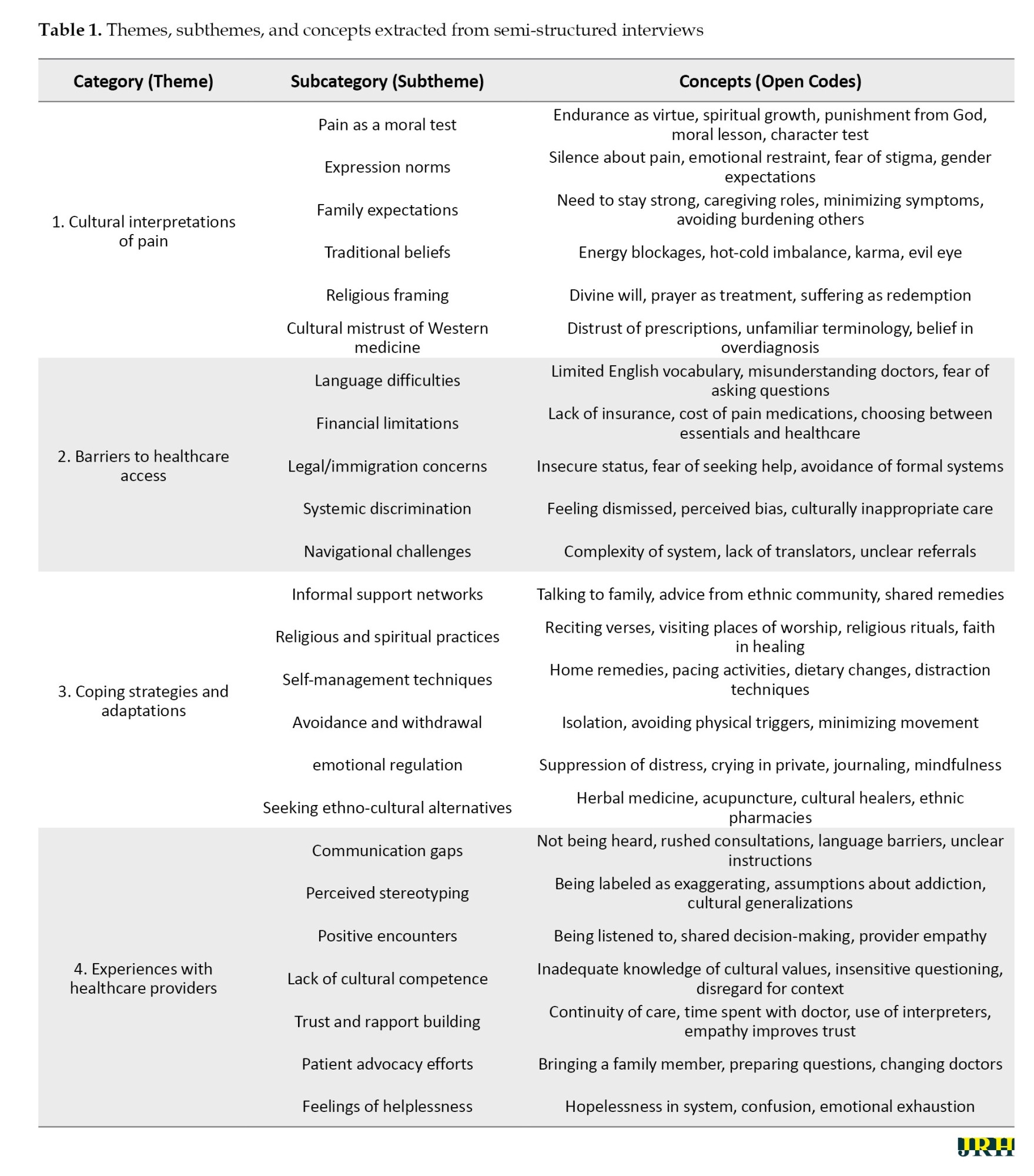
Thematic analysis revealed four overarching categories:
1) Cultural interpretations of pain; 2) barriers to healthcare access; 3) coping strategies and adaptations; 4) experiences with healthcare providers.
These categories show how cultural frameworks, systemic challenges, and personal agency intersect in shaping chronic pain management for immigrants.
Category 1: Cultural interpretations of pain
Moral and Spiritual Meaning. Many participants, instead of interpreting it through a spiritual or moral feeling, addressed their pain as more than a physical condition. Pain was understood as a divine test of character, an opportunity for growth, or even punishment for past actions, which was particularly pronounced among women and those with longer-standing cultural traditions, prizing endurance and patience. In this regard, many participants talked about concepts such “spiritually stronger” and finding meaning in suffering. One said, “I believe God gave me this pain for a reason—maybe to teach me patience or to purify me.” Especially among newcomers who felt anchored in familiar spiritual frameworks, although this quote provided comfort, it also contributed to acceptance rather than active treatment-seeking.
Expression norms and gender roles. Across cultures, participants described unwritten rules discouraging open discussion of pain. Women often endured quietly to avoid disrupting family life or being seen as weak, while men suppressed vulnerability to maintain their provider identity. One woman explained, “Even though I’m hurting, I cook and clean. My children shouldn’t see me as weak.” Another man noted he minimized symptoms because “a man must be strong.” These internalized expectations delayed disclosure, limited emotional support, and postponed help-seeking.
Traditional explanatory models. Participants frequently referenced cultural models of illness, including beliefs about “cold wind,” “energy blockages,” or the evil eye. These frameworks provided familiar explanations and a sense of control but also reinforced skepticism toward biomedical care. Some felt Western medicine ignored root causes or overemphasized pharmaceuticals: “Doctors here just give pills. Back home, we treat the root cause with herbs and massage.” Newer immigrants leaned heavily on these explanatory systems, while those with longer Canadian residence described gradual integration of Western concepts alongside traditional reasoning.
Religious coping and rituals. Prayer, fasting, attending spiritual gatherings, and reading sacred texts were used to manage both emotional and physical suffering. A woman noted, “When I pray, the pain doesn’t go away, but I feel calmer.” Such practices provided resilience and hope, especially where healthcare felt inaccessible. Yet, this reliance sometimes led to delayed or selective use of medical services when participants believed pain had a divine origin or would resolve with faith.
Skepticism toward western medicine. Mistrust of pharmaceutical treatment and perceptions of superficial biomedical approaches surfaced repeatedly. Many expressed discomfort with painkillers’ side effects or feared dependency. Some preferred culturally familiar care—herbs, massage, acupuncture—especially when early encounters with physicians felt rushed or dismissive. Over time, a few participants developed more balanced perspectives, combining traditional and Western approaches, but this shift depended heavily on positive provider experiences.
Category 2: Barriers to healthcare access
Language difficulties. communication barriers emerged as one of the most frustrating and isolating obstacles. Participants described lacking the precise vocabulary to explain pain and fearing misinterpretation. This often led to under-treatment or inappropriate prescriptions. One said, “I don’t know the right words to explain my pain… sometimes I just say ‘it hurts everywhere.’” The difficulty increased emotional strain and discouraged return visits, especially among recent arrivals with limited English.
Financial limitations. High costs of medication, therapy, and transportation discouraged continuous care. Several participants without private insurance or stable jobs described choosing between health and essential needs: “I had to choose between buying my medicine and paying rent.” Some stopped seeing specialists or abandoned recommended therapies due to cost. Those working part-time or informally were especially vulnerable to these trade-offs.
Legal and immigration concerns. Fear about immigration status discouraged help-seeking. Participants with pending applications or precarious visas worried that hospital visits or medical records might affect their cases: “I didn’t go to the hospital because I thought it might affect my immigration case.” This anxiety intensified delays in diagnosis and treatment, particularly among those newer to Canada and unfamiliar with rights and health policies.
Systemic discrimination and stereotyping. Multiple participants recounted experiences where their pain was minimized or treated with suspicion. They felt labeled as exaggerating or drug-seeking, which was deeply hurtful and damaging to trust. “When I told the doctor I was in pain, he just looked at me like I was exaggerating.” These negative encounters discouraged follow-up and contributed to a sense of alienation from the system.
Navigational complexity. The structure of the healthcare system felt overwhelming—lengthy referrals, unclear paperwork, and lack of interpretation services made it difficult to move forward with care. “Everything is complicated—so many steps, and I get lost,” said one woman. These logistical hurdles reinforced feelings of helplessness and led some to rely more heavily on community and informal care networks.
Category 3: Coping strategies and adaptations
Family and community networks. Participants relied heavily on trusted networks for advice, remedies, and emotional support. Shared cultural knowledge filled gaps left by formal care and created a sense of safety: “My aunt told me to drink turmeric milk every night—it helps more than the pills.” While this built solidarity, it sometimes delayed medical evaluation or reinforced non-evidence-based approaches.
Religious and spiritual coping. Faith was described as an anchor for endurance and mental peace. Prayer, scripture listening, and religious gatherings offered calm and strength: “When I can’t sleep because of pain, I just listen to Quran recitations—it calms my mind.” For some, religious framing replaced clinical engagement, but for others it complemented treatment by supporting psychological resilience.
Self-management and emotional regulation. Many described carefully pacing activities, adjusting diets, exercising gently, or distracting themselves with television, reading, or writing. Mothers often used emotional regulation—crying in private, journaling—to shield family members from their distress: “I don’t want my children to see me upset, so I cry in the shower.” These practices promoted daily functioning but sometimes masked symptom severity, delaying formal care.
Avoidance and social withdrawal. Some participants coped by retreating socially and reducing physical activity. While this initially protected against embarrassment or questions, it often deepened isolation and depression: “I stopped going out. I don’t want people asking what’s wrong with me.” Over time, avoidance created barriers to reintegration into the community and formal care pathways.
Use of ethno-cultural and complementary care. Several participants turned to culturally familiar clinics, acupuncture, herbal therapy, or massage. They valued being “understood” and culturally safe: “There’s a Chinese clinic near my house—I feel more understood there.” This approach enhanced comfort and control but sometimes fragmented care when providers were not integrated into mainstream health systems.
Category 4: Experiences with healthcare providers
Communication gaps. Many encounters were marked by rushed consultations and poor listening, leaving participants feeling invisible. “I tried to explain, but the doctor kept interrupting me.” Such breakdowns amplified mistrust and discouraged follow-up, especially among those already struggling with language.
Stereotyping and bias. Participants described feeling profiled as drug-seeking or exaggerating pain. These perceptions were particularly painful for those who had delayed care out of fear: “They think we just want painkillers. I’m not a liar—I just want help.” Negative assumptions undermined trust and reinforced avoidance.
Positive and empathic encounters. Despite challenges, some participants experienced deeply validating interactions. Providers who showed patience, compassion, and curiosity transformed care experiences: “One nurse held my hand and said, ‘I believe you.’ That meant a lot.” These moments restored confidence and motivated continued engagement with the healthcare system.
Cultural competence gaps. Lack of awareness about cultural narratives of pain was common. Participants reported awkward or insensitive questions about their beliefs or delays due to a misunderstanding of shame and stigma. Conversely, the use of interpreters and consistent providers improved understanding and trust.
Patient advocacy and self-empowerment. Several participants adapted by preparing questions, bringing trusted family members, or switching doctors until they felt heard: “I now write everything down before going—it helps me speak clearly.” While empowering, such advocacy was exhausting and not feasible for everyone, particularly those with severe pain or limited support.
Discussion
This qualitative study explored the lived experiences of chronic pain management among immigrant adults in Richmond Hill, revealing four overarching categories: Cultural interpretations of pain, barriers to healthcare access, coping strategies and adaptations, and experiences with healthcare providers. The findings show that chronic pain for immigrants is not merely a biomedical phenomenon but a deeply contextual experience shaped by cultural meaning-making, systemic inequities, and personal narratives. Extending prior work, our urban Canadian sample uniquely revealed how these cultural and systemic dynamics converge within a highly diverse municipal context—where 70% of residents identify as visible minorities—to produce both shared and locale-specific manifestations of chronic pain management. These results both confirm and expand prior research demonstrating the complex interplay of cultural, psychological, and structural factors in immigrant pain management [5, 8, 9].
One of the most striking findings was the framing of chronic pain as a moral or spiritual test. Participants often constructed pain as divine punishment, purification, or trial, a view that helped them endure suffering but also delayed active help-seeking. Unlike prior studies limited to homogeneous cultural groups, this study illustrates how moral framings interact with multicultural identity negotiation in Canada’s pluralistic setting, blending faith-based endurance with pragmatic adaptation to systemic constraints. This resonates with research on religious and metaphysical interpretations of pain among women from collectivist cultures [22, 23]. Gender norms strongly shaped expression: many women reported suppressing emotional pain to maintain family stability and caregiving responsibilities, while men suppressed vulnerability to preserve a provider identity. These patterns underscore a gendered moral economy of pain that, in our sample, intersected with migration experiences and role expectations more visibly than in prior work. Similar gendered dynamics have been noted in previous work, where immigrant women internalize pain as part of resilience and moral obligation [5, 8]. These narratives demonstrate how cultural scripts about strength and sacrifice can contribute to both coping and invisibility in healthcare.
Emotional restraint and self-silencing were prominent and echo literature linking cultural norms to delayed disclosure and psychological isolation [7, 24]. Participants described how family expectations reinforced stoicism and discouraged burdening loved ones, a dynamic observed in other qualitative studies of immigrant women with chronic pain [22]. Traditional explanatory frameworks—such as energy imbalance, the evil eye, or cold wind—provided coherence and comfort but sometimes clashed with biomedical reasoning [6, 10]. These findings contribute novel evidence that, within multiethnic urban contexts, these traditional beliefs often coexist rather than compete with Western explanatory models—producing hybrid coping logics that reflect simultaneous cultural preservation and acculturation. These beliefs can support resilience and agency, but when dismissed by providers, risk deepening mistrust and disengagement.
The study also revealed multiple, interwoven systemic barriers. Language difficulties repeatedly emerged as a primary obstacle, leading to misdiagnosis and communication breakdown, consistent with earlier findings linking limited English proficiency to under-treatment [18, 19]. Financial constraints restricted access to therapies and medications, particularly for those without private insurance—a pattern also identified in prior research on immigrant pain inequities [17, 25]. Additionally, legal and immigration-related anxieties deterred care-seeking for some participants, especially newcomers and those with uncertain status; this aligns with broader work linking precarious status to chronic pain burden [25]. Discrimination and stereotyping by providers—being seen as drug-seeking or exaggerating—exacerbated alienation and delayed care, confirming evidence of bias against racialized and immigrant patients [14, 19]. However, the present study extends this body of evidence by showing how these systemic barriers operate cumulatively within a single locality, generating a feedback loop where institutional mistrust reinforces cultural silence, which in turn reproduces delayed care. Together, these factors illustrate how systemic barriers compound cultural reasons for silence, creating a cycle of delayed help-seeking and worsened outcomes.
Despite barriers, participants demonstrated remarkable resourcefulness. They relied on family networks, spiritual practices, and ethno-cultural remedies to maintain control and emotional stability. These coping mechanisms echo other qualitative reports describing religious frameworks as powerful tools for emotional regulation [12, 13]. However, dependence on these strategies sometimes resulted in reduced engagement with biomedical care, highlighting the need for culturally responsive education about when formal intervention is necessary. Participants also described self-regulation practices—mindfulness, journaling, pacing—which are consistent with therapeutic strategies used in acceptance and commitment therapy (ACT) and mindfulness-based cognitive therapy [2, 13, 16]. By demonstrating how immigrants organically employ these techniques without formal training, this study identifies culturally grounded entry points for integrating mindfulness and acceptance-based interventions into community-level pain programs. These approaches supported psychological resilience even when physical pain remained, underscoring the importance of integrating psychosocial skill-building into culturally tailored pain programs [23, 26].
Experiences with healthcare providers constituted a major axis of divergence between positive adaptation and systemic disengagement. Negative encounters—characterized by stereotyping, rushed consultations, and cultural misunderstanding—paralleled findings from other studies showing systemic bias toward immigrant patients [17, 18]. Women, in particular, felt minimized or mischaracterized, reinforcing gendered vulnerability previously documented [8, 22]. Conversely, positive, empathic encounters—where providers listened, acknowledged cultural beliefs, and maintained continuity—restored trust and encouraged re-engagement. Beyond reaffirming the need for cultural competence, our data suggest specific policy implications: in diverse locales such as Richmond Hill, healthcare institutions should adopt mandatory annual training modules on immigrant pain narratives, intercultural communication, and interpreter-mediated care. Embedding such continuing education into licensing requirements could standardize empathy-based practice and reduce structural inequities in pain management. This reinforces calls for cross-cultural communication training and pain literacy among providers [4, 9]. When patients felt understood, adherence to treatment improved, and informal coping could be more safely integrated with biomedical care. In turn, these findings highlight the translational importance of coupling empathy training with structural supports—such as interpreter funding and culturally tailored pain education materials—to operationalize inclusion beyond individual goodwill.
The COVID-19 pandemic magnified existing inequities, disrupting healthcare access and worsening psychological strain. Our participants’ narratives of postponed appointments, intensified symptoms, and increased reliance on informal support echo emerging evidence on pandemic-driven disparities in chronic pain care [20, 21]. By situating these experiences within the broader context of migration-related stress and health system fragmentation, the study reveals how crisis conditions accentuate vulnerabilities unique to immigrant populations. These findings underscore that “universal” systems still leave immigrants vulnerable without targeted strategies addressing language, financial, and cultural barriers.
Conclusion
This study illuminates how chronic pain management among immigrant adults is profoundly shaped by the interplay of cultural beliefs, systemic barriers, emotional coping strategies, and healthcare experiences. The findings challenge the adequacy of a purely biomedical perspective and argue for approaches that honor personal narratives, cultural explanatory models, and social realities. Beyond local relevance, these findings also underscore the potential for scalability—offering a foundation for developing national guidelines that adapt locally effective, culturally responsive pain management models into broader healthcare frameworks across Canada. By centering immigrants’ voices, this research contributes to a more inclusive understanding of chronic pain and calls for integrative, empathetic, and equitable care practices that are responsive to diverse cultural and migration-related contexts.
Several limitations should be acknowledged. First, the sample was restricted to immigrants residing in Richmond Hill, an urban area with its own demographic profile and healthcare infrastructure; therefore, the transferability of findings to rural settings or other urban centers with different cultural compositions may be limited. Second, although purposive sampling sought maximum variation, participants who volunteered might have been those more comfortable discussing pain and healthcare, introducing potential self-selection bias. Third, language barriers may have constrained the richness of some interviews despite efforts to use accessible English and clarification techniques. Finally, the research team was composed of non-immigrant investigators; although reflexivity and peer debriefing were applied, some subtle cultural nuances may not have been fully captured.
To advance this field, future research should directly address the identified conceptual and temporal gaps. Specifically, to bridge the underexplored dimension of acculturation, scholars should prioritize longitudinal tracking of explanatory model shifts and coping adaptations across different migration phases. Comparative analyses with non-immigrant populations can further clarify how sociocultural integration shapes pain expression and healthcare engagement. In addition, mixed-method approaches combining qualitative depth with quantitative mapping of acculturation trajectories help reveal the evolving interaction between belief systems, systemic adaptation, and clinical outcomes. Incorporating participatory and community-based methods—such as photovoice, narrative inquiry, or ethnographic observation—may yield deeper insight into the embodied and relational dimensions of pain. Finally, there is a critical need for intervention studies testing culturally adapted pain management programs that integrate traditional belief systems, resilience-building skills, and community-based support structures. Such interventions, if scaled through national policy frameworks, could inform equitable chronic pain strategies that reflect the lived diversity of immigrant experiences.
Healthcare providers working with immigrant populations should be trained in culturally responsive care, with explicit attention to diverse pain expressions and traditional health frameworks. Routine use of medical interpreters, culturally tailored pain education, and collaborative, patient-centered treatment planning should become standard. At the policy level, integrating these findings into national chronic pain action plans—through dedicated funding for interpreter services, multicultural clinical training, and community liaison roles—would help institutionalize culturally safe care. Policymakers should reduce systemic barriers—especially those related to language access, insurance gaps, and immigration-related fears—that discourage timely care-seeking. Integrating mental health support into pain management is essential for addressing trauma, loss, and acculturation stress. Finally, healthcare systems should actively build trust through continuity of care, respectful communication, and recognition of patients’ cultural identities as valid frameworks for understanding and addressing chronic pain.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of KMAN Research Institute, Richmond Hill, Canada (Code: KEC.2024.03C10. Prior to the commencement of the study, all participants were informed about the research objectives, the confidentiality of their responses, and their right to withdraw from the study at any point. Written informed consent was obtained from all participants. Measures were taken to ensure the anonymity of participants, and personal identifiers were removed or altered in the transcription process.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express our gratitude to all individuals who helped us to do the project.
References
Chronic pain is a complex, long-lasting condition that affects physical functioning, emotional well-being, and overall quality of life. Defined as pain persisting for more than three months, it is increasingly recognized as a biopsychosocial phenomenon, shaped not only by biological injury or dysfunction but also by psychological and sociocultural dynamics [1, 2]. This conceptual shift is particularly relevant to immigrant populations, who experience chronic pain differently than the general population because of migration-related stressors, cultural norms, systemic inequities, and barriers to healthcare [3]. It affects nearly one in five adults worldwide. It occurs 1.5 to 2 times more frequently among immigrants due to migration-related stressors, acculturation challenges, and systemic inequities. It is increasingly recognized as a biopsychosocial phenomenon, shaped not only by biological injury or dysfunction but also by psychological and sociocultural dynamics [1-3]. This conceptual shift is particularly relevant to immigrant populations, whose experiences of chronic pain differ markedly from those of the general population because of cultural norms, discrimination, and structural barriers to healthcare. With global migration accelerating—over 280 million people now live outside their country of origin—and the rising prevalence of chronic pain, understanding its cultural and systemic dimensions among immigrants has become a pressing public health priority [4, 5].
Epidemiological studies show disproportionately high rates of chronic pain among immigrants, particularly those with refugee or precarious migration status [6]. These disparities stem from cumulative trauma exposure, socioeconomic disadvantage, and ongoing marginalization [7]. Migration-related factors—such as language limitations, differing cultural health beliefs, and unfamiliarity with host-country healthcare systems—often compound these risks [8]. Chronic pain has also been documented among younger immigrants, including children and adolescents, indicating that long-term health inequities begin early [3].
Pain management is challenging even within well-structured healthcare systems, but immigration compounds these difficulties through cultural incongruence, discrimination, and identity negotiation. For example, immigrants from the Middle East and North Africa are especially vulnerable to chronic musculoskeletal pain, yet often lack culturally responsive treatment options [9]. These vulnerabilities arise from pre-migration trauma, cultural variations in pain expression, and misalignment between traditional explanatory models (e.g. spiritual or moral framing) and Western biomedical paradigms [10]. Qualitative research also suggests that differences in interoceptive awareness—how individuals perceive internal bodily states—can affect symptom interpretation and coping responses [11].
Despite these insights, the literature on immigrant chronic pain remains fragmented, often leaning toward biomedical and psychiatric frameworks while overlooking how cultural beliefs and systemic barriers intersect. For instance, some studies focus on resilience and psychological adaptation—self-efficacy, ego strength, and personality traits, such as neuroticism or perfectionism—which influence vulnerability to pain-related distress [12-14]. Cognitive patterns, such as catastrophizing and helplessness, are also implicated in worsening pain outcomes, and these may be intensified by the migration experience [10, 15]. Acceptance and commitment therapy (ACT), for example, has been found effective in enhancing psychological flexibility and pain tolerance [2, 16]; however, the extent to which such interventions are culturally adapted for immigrant patients remains unclear.
Another critical gap involves system-level inequities. Immigrants frequently describe healthcare systems as “chaotic,” requiring navigation skills many do not possess [17]. This “navigation burden” includes language proficiency, health literacy, and advocacy skills; lacking these can result in delayed or foregone treatment [18, 19]. Fear of discrimination or legal repercussions further discourages timely help-seeking, while perceived stereotyping by providers erodes trust [8]. The COVID-19 pandemic worsened these barriers by disrupting access, intensifying pain symptoms, and increasing mental health strain among immigrants [20]. Many turned to community-based coping, such as family support and ethno-cultural healing practices, underscoring resilience but also revealing systemic service gaps [21].
Gendered experiences require particular attention. Women immigrants often shoulder dual burdens—managing pain while fulfilling caregiving and cultural expectations—which can lead to emotional isolation and pain silencing [8, 22]. Religious or moral interpretations of pain, such as seeing it as a divine test, may reinforce endurance but delay medical intervention [13, 23]. Conversely, some men minimize or suppress pain to maintain perceived roles as providers [4]. These gendered narratives highlight the importance of contextually sensitive qualitative approaches that capture how social roles and cultural identity shape pain expression and care engagement.
Meanwhile, resilience and culturally congruent coping strategies are central in immigrant communities. Religious rituals, family advice, and traditional medicine can help regulate emotions and preserve hope [24]. Yet these approaches sometimes delay evidence-based interventions, creating tension between culturally meaningful practices and clinical effectiveness [19, 25]. Thus, exploring how immigrants negotiate between these worlds is critical for developing integrative pain management models that respect cultural frameworks while maintaining clinical rigor.
Despite growing scholarship, there remains a substantial knowledge gap: few studies deeply examine how immigrant adults actively make sense of and cope with chronic pain while engaging with healthcare in an urban Canadian setting. Existing work rarely investigates how cultural identity, familial obligations, spirituality, and systemic barriers converge to shape help-seeking and self-care [3, 7]. Richmond Hill, Ontario, offers an ideal context for such exploration due to its highly diverse immigrant population and complex healthcare landscape. Richmond Hill, Ontario, offers an ideal context for such exploration, being one of Canada’s most diverse municipalities—home to over 70% visible minorities and more than 55% immigrants, predominantly from Asia and the Middle East [11]. This unique demographic composition provides a rich landscape for examining cross-cultural experiences of pain within a multicultural healthcare environment.
Understanding these dynamics is essential for designing culturally attuned, accessible, and patient-centered pain interventions that respond to the real contexts. Therefore, this study aimed to explore the lived experiences of chronic pain management among immigrant adults in Richmond Hill, Canada. By centering immigrants’ voices, it aims to uncover how cultural interpretations, coping patterns, and systemic inequities interact to influence pain trajectories and care engagement.
Methods
Study design and participants
This study employed a qualitative descriptive-phenomenological design to explore the lived experiences of chronic pain management among immigrant adults. The approach was chosen to capture participants’ subjective meanings, cultural interpretations, and contextual barriers in depth. In keeping with phenomenological rigor, the analytic process was guided by Husserlian principles, employing epoché or bracketing to suspend researchers’ preconceptions and remain focused on participants’ lived meanings as they naturally emerged. The goal was to describe the essence of the phenomenon rather than interpret it through theoretical bias, thereby ensuring alignment with descriptive phenomenology’s philosophical underpinnings. The study was conducted in Richmond Hill, Ontario, Canada, in 2024, an urban area with one of the country’s most ethnoculturally diverse populations.
A purposive maximum-variation sampling strategy was used to ensure diversity regarding age, gender, country of origin, type and duration of pain, and length of residence in Canada. Individuals were eligible if they:
Self-identified as immigrants; were 30 years or older (reflecting reviewer recommendations and the chronic pain onset pattern); had lived with chronic pain for at least six months; could communicate in English (to ensure rich narratives and reduce translation bias), and were willing to share their experiences in a one-on-one interview setting.
While English fluency was required to maintain narrative richness and minimize translation bias, this criterion inevitably excluded some non-English-speaking immigrants. To address this limitation prospectively, the study acknowledges the need for future expansions to multilingual facilitation through trained bilingual interviewers or translated instruments. This adjustment would enhance inclusivity while maintaining the narrative depth demonstrated in pilot interviews that informed the present study’s design.
Participants were recruited through community organizations, immigrant support groups, and healthcare providers using flyers and word-of-mouth. Sampling continued until theoretical saturation was reached—that is, when no new codes or themes emerged after iterative analysis. The final sample consisted of 26 participants representing diverse cultural and migration backgrounds.
Data collection tool
Semi-structured interview: Data were collected between February and June 2024 using in-depth, semi-structured interviews conducted either face-to-face in community settings (e.g. cultural centers, local clinics) or via secure video conferencing when preferred for convenience or safety.
A pilot-tested interview guide, informed by previous literature on immigrant chronic pain and refined after initial interviews, ensured conceptual coverage and cultural sensitivity. Key domains included:
Personal narratives of chronic pain; cultural and spiritual interpretations of pain; coping and self-management strategies; healthcare-seeking behaviors and systemic barriers, and experiences with trust, discrimination, and provider communication.
Each interview lasted 45–75 minutes and was audio-recorded with explicit, culturally sensitive informed consent. Consent procedures included plain-language explanations, opportunities for questions, and assurances regarding confidentiality and non-impact on immigration status. The interviewer maintained reflexive field notes to document contextual cues and nonverbal expressions, enriching data interpretation. All interviews were transcribed verbatim and de-identified.
Data analysis
Data were analyzed using Braun and Clarke’s six-phase thematic analysis framework: 1) Familiarization, 2) generating initial codes, 3) searching for themes, 4) reviewing themes, 5) defining and naming themes, and 6) reporting. Coding was inductive and iterative, grounded in participants’ narratives while also guided by emerging conceptual insights.
Transcripts were imported into NVivo software, version 14 for systematic coding and data management. Two researchers independently coded a subset of transcripts to ensure coder agreement, and differences were resolved through discussion and consensus. Inter-coder reliability was quantified, achieving approximately 85% initial agreement on 20% of transcripts before reconciliation, providing empirical support for analytic consistency and rigor. Reflexivity was maintained through analytic memos documenting the researcher’s positionality and potential biases.
To enhance trustworthiness, we incorporated:
Peer debriefing with experienced qualitative researchers to validate interpretations; member checking by sharing synthesized themes with participants willing to review them, and Maintaining an audit trail of coding decisions and theme refinements.
Saturation was confirmed when successive interviews yielded no new codes or conceptual insights, demonstrating that key aspects of participants’ lived experiences had been comprehensively captured.
Results
This study included 26 immigrant adults living in Richmond Hill, Ontario, all aged 30–45 years (mean=37.4). Although eligibility was set at ≥30 years, the observed range reflected emergent saturation among younger to mid-adulthood participants in the recruitment pool, suggesting that data sufficiency was reached before enrolling older individuals. Seventeen participants were women (65%) and nine were men (35%). Countries of origin included Iran (n=6), India (n=5), China (n=4), Pakistan (n=3), the Philippines (n=3), Syria (n=2), Nigeria (n=2), and Afghanistan (n=1). Sixteen participants (62%) had resided in Canada for more than five years, while ten (38%) had lived in the country for fewer than five years. Chronic pain conditions included musculoskeletal pain (n=9), fibromyalgia (n=6), neuropathic pain (n=5), chronic back pain (n=4), and migraine or chronic headache (n=2). Twelve participants (46%) were unemployed due to pain-related disability, six (23%) were employed part-time, five (19%) worked full-time, and three (12%) were homemakers. Educational backgrounds ranged from primary to post-secondary: 11 participants (42%) held a university degree, nine (35%) completed high school, and six (23%) had less than a high school education. Most (81%) lacked private insurance and relied on public health coverage or personal savings for care (Table 1).
Thematic analysis revealed four overarching categories:
1) Cultural interpretations of pain; 2) barriers to healthcare access; 3) coping strategies and adaptations; 4) experiences with healthcare providers.
These categories show how cultural frameworks, systemic challenges, and personal agency intersect in shaping chronic pain management for immigrants.
Category 1: Cultural interpretations of pain
Moral and Spiritual Meaning. Many participants, instead of interpreting it through a spiritual or moral feeling, addressed their pain as more than a physical condition. Pain was understood as a divine test of character, an opportunity for growth, or even punishment for past actions, which was particularly pronounced among women and those with longer-standing cultural traditions, prizing endurance and patience. In this regard, many participants talked about concepts such “spiritually stronger” and finding meaning in suffering. One said, “I believe God gave me this pain for a reason—maybe to teach me patience or to purify me.” Especially among newcomers who felt anchored in familiar spiritual frameworks, although this quote provided comfort, it also contributed to acceptance rather than active treatment-seeking.
Expression norms and gender roles. Across cultures, participants described unwritten rules discouraging open discussion of pain. Women often endured quietly to avoid disrupting family life or being seen as weak, while men suppressed vulnerability to maintain their provider identity. One woman explained, “Even though I’m hurting, I cook and clean. My children shouldn’t see me as weak.” Another man noted he minimized symptoms because “a man must be strong.” These internalized expectations delayed disclosure, limited emotional support, and postponed help-seeking.
Traditional explanatory models. Participants frequently referenced cultural models of illness, including beliefs about “cold wind,” “energy blockages,” or the evil eye. These frameworks provided familiar explanations and a sense of control but also reinforced skepticism toward biomedical care. Some felt Western medicine ignored root causes or overemphasized pharmaceuticals: “Doctors here just give pills. Back home, we treat the root cause with herbs and massage.” Newer immigrants leaned heavily on these explanatory systems, while those with longer Canadian residence described gradual integration of Western concepts alongside traditional reasoning.
Religious coping and rituals. Prayer, fasting, attending spiritual gatherings, and reading sacred texts were used to manage both emotional and physical suffering. A woman noted, “When I pray, the pain doesn’t go away, but I feel calmer.” Such practices provided resilience and hope, especially where healthcare felt inaccessible. Yet, this reliance sometimes led to delayed or selective use of medical services when participants believed pain had a divine origin or would resolve with faith.
Skepticism toward western medicine. Mistrust of pharmaceutical treatment and perceptions of superficial biomedical approaches surfaced repeatedly. Many expressed discomfort with painkillers’ side effects or feared dependency. Some preferred culturally familiar care—herbs, massage, acupuncture—especially when early encounters with physicians felt rushed or dismissive. Over time, a few participants developed more balanced perspectives, combining traditional and Western approaches, but this shift depended heavily on positive provider experiences.
Category 2: Barriers to healthcare access
Language difficulties. communication barriers emerged as one of the most frustrating and isolating obstacles. Participants described lacking the precise vocabulary to explain pain and fearing misinterpretation. This often led to under-treatment or inappropriate prescriptions. One said, “I don’t know the right words to explain my pain… sometimes I just say ‘it hurts everywhere.’” The difficulty increased emotional strain and discouraged return visits, especially among recent arrivals with limited English.
Financial limitations. High costs of medication, therapy, and transportation discouraged continuous care. Several participants without private insurance or stable jobs described choosing between health and essential needs: “I had to choose between buying my medicine and paying rent.” Some stopped seeing specialists or abandoned recommended therapies due to cost. Those working part-time or informally were especially vulnerable to these trade-offs.
Legal and immigration concerns. Fear about immigration status discouraged help-seeking. Participants with pending applications or precarious visas worried that hospital visits or medical records might affect their cases: “I didn’t go to the hospital because I thought it might affect my immigration case.” This anxiety intensified delays in diagnosis and treatment, particularly among those newer to Canada and unfamiliar with rights and health policies.
Systemic discrimination and stereotyping. Multiple participants recounted experiences where their pain was minimized or treated with suspicion. They felt labeled as exaggerating or drug-seeking, which was deeply hurtful and damaging to trust. “When I told the doctor I was in pain, he just looked at me like I was exaggerating.” These negative encounters discouraged follow-up and contributed to a sense of alienation from the system.
Navigational complexity. The structure of the healthcare system felt overwhelming—lengthy referrals, unclear paperwork, and lack of interpretation services made it difficult to move forward with care. “Everything is complicated—so many steps, and I get lost,” said one woman. These logistical hurdles reinforced feelings of helplessness and led some to rely more heavily on community and informal care networks.
Category 3: Coping strategies and adaptations
Family and community networks. Participants relied heavily on trusted networks for advice, remedies, and emotional support. Shared cultural knowledge filled gaps left by formal care and created a sense of safety: “My aunt told me to drink turmeric milk every night—it helps more than the pills.” While this built solidarity, it sometimes delayed medical evaluation or reinforced non-evidence-based approaches.
Religious and spiritual coping. Faith was described as an anchor for endurance and mental peace. Prayer, scripture listening, and religious gatherings offered calm and strength: “When I can’t sleep because of pain, I just listen to Quran recitations—it calms my mind.” For some, religious framing replaced clinical engagement, but for others it complemented treatment by supporting psychological resilience.
Self-management and emotional regulation. Many described carefully pacing activities, adjusting diets, exercising gently, or distracting themselves with television, reading, or writing. Mothers often used emotional regulation—crying in private, journaling—to shield family members from their distress: “I don’t want my children to see me upset, so I cry in the shower.” These practices promoted daily functioning but sometimes masked symptom severity, delaying formal care.
Avoidance and social withdrawal. Some participants coped by retreating socially and reducing physical activity. While this initially protected against embarrassment or questions, it often deepened isolation and depression: “I stopped going out. I don’t want people asking what’s wrong with me.” Over time, avoidance created barriers to reintegration into the community and formal care pathways.
Use of ethno-cultural and complementary care. Several participants turned to culturally familiar clinics, acupuncture, herbal therapy, or massage. They valued being “understood” and culturally safe: “There’s a Chinese clinic near my house—I feel more understood there.” This approach enhanced comfort and control but sometimes fragmented care when providers were not integrated into mainstream health systems.
Category 4: Experiences with healthcare providers
Communication gaps. Many encounters were marked by rushed consultations and poor listening, leaving participants feeling invisible. “I tried to explain, but the doctor kept interrupting me.” Such breakdowns amplified mistrust and discouraged follow-up, especially among those already struggling with language.
Stereotyping and bias. Participants described feeling profiled as drug-seeking or exaggerating pain. These perceptions were particularly painful for those who had delayed care out of fear: “They think we just want painkillers. I’m not a liar—I just want help.” Negative assumptions undermined trust and reinforced avoidance.
Positive and empathic encounters. Despite challenges, some participants experienced deeply validating interactions. Providers who showed patience, compassion, and curiosity transformed care experiences: “One nurse held my hand and said, ‘I believe you.’ That meant a lot.” These moments restored confidence and motivated continued engagement with the healthcare system.
Cultural competence gaps. Lack of awareness about cultural narratives of pain was common. Participants reported awkward or insensitive questions about their beliefs or delays due to a misunderstanding of shame and stigma. Conversely, the use of interpreters and consistent providers improved understanding and trust.
Patient advocacy and self-empowerment. Several participants adapted by preparing questions, bringing trusted family members, or switching doctors until they felt heard: “I now write everything down before going—it helps me speak clearly.” While empowering, such advocacy was exhausting and not feasible for everyone, particularly those with severe pain or limited support.
Discussion
This qualitative study explored the lived experiences of chronic pain management among immigrant adults in Richmond Hill, revealing four overarching categories: Cultural interpretations of pain, barriers to healthcare access, coping strategies and adaptations, and experiences with healthcare providers. The findings show that chronic pain for immigrants is not merely a biomedical phenomenon but a deeply contextual experience shaped by cultural meaning-making, systemic inequities, and personal narratives. Extending prior work, our urban Canadian sample uniquely revealed how these cultural and systemic dynamics converge within a highly diverse municipal context—where 70% of residents identify as visible minorities—to produce both shared and locale-specific manifestations of chronic pain management. These results both confirm and expand prior research demonstrating the complex interplay of cultural, psychological, and structural factors in immigrant pain management [5, 8, 9].
One of the most striking findings was the framing of chronic pain as a moral or spiritual test. Participants often constructed pain as divine punishment, purification, or trial, a view that helped them endure suffering but also delayed active help-seeking. Unlike prior studies limited to homogeneous cultural groups, this study illustrates how moral framings interact with multicultural identity negotiation in Canada’s pluralistic setting, blending faith-based endurance with pragmatic adaptation to systemic constraints. This resonates with research on religious and metaphysical interpretations of pain among women from collectivist cultures [22, 23]. Gender norms strongly shaped expression: many women reported suppressing emotional pain to maintain family stability and caregiving responsibilities, while men suppressed vulnerability to preserve a provider identity. These patterns underscore a gendered moral economy of pain that, in our sample, intersected with migration experiences and role expectations more visibly than in prior work. Similar gendered dynamics have been noted in previous work, where immigrant women internalize pain as part of resilience and moral obligation [5, 8]. These narratives demonstrate how cultural scripts about strength and sacrifice can contribute to both coping and invisibility in healthcare.
Emotional restraint and self-silencing were prominent and echo literature linking cultural norms to delayed disclosure and psychological isolation [7, 24]. Participants described how family expectations reinforced stoicism and discouraged burdening loved ones, a dynamic observed in other qualitative studies of immigrant women with chronic pain [22]. Traditional explanatory frameworks—such as energy imbalance, the evil eye, or cold wind—provided coherence and comfort but sometimes clashed with biomedical reasoning [6, 10]. These findings contribute novel evidence that, within multiethnic urban contexts, these traditional beliefs often coexist rather than compete with Western explanatory models—producing hybrid coping logics that reflect simultaneous cultural preservation and acculturation. These beliefs can support resilience and agency, but when dismissed by providers, risk deepening mistrust and disengagement.
The study also revealed multiple, interwoven systemic barriers. Language difficulties repeatedly emerged as a primary obstacle, leading to misdiagnosis and communication breakdown, consistent with earlier findings linking limited English proficiency to under-treatment [18, 19]. Financial constraints restricted access to therapies and medications, particularly for those without private insurance—a pattern also identified in prior research on immigrant pain inequities [17, 25]. Additionally, legal and immigration-related anxieties deterred care-seeking for some participants, especially newcomers and those with uncertain status; this aligns with broader work linking precarious status to chronic pain burden [25]. Discrimination and stereotyping by providers—being seen as drug-seeking or exaggerating—exacerbated alienation and delayed care, confirming evidence of bias against racialized and immigrant patients [14, 19]. However, the present study extends this body of evidence by showing how these systemic barriers operate cumulatively within a single locality, generating a feedback loop where institutional mistrust reinforces cultural silence, which in turn reproduces delayed care. Together, these factors illustrate how systemic barriers compound cultural reasons for silence, creating a cycle of delayed help-seeking and worsened outcomes.
Despite barriers, participants demonstrated remarkable resourcefulness. They relied on family networks, spiritual practices, and ethno-cultural remedies to maintain control and emotional stability. These coping mechanisms echo other qualitative reports describing religious frameworks as powerful tools for emotional regulation [12, 13]. However, dependence on these strategies sometimes resulted in reduced engagement with biomedical care, highlighting the need for culturally responsive education about when formal intervention is necessary. Participants also described self-regulation practices—mindfulness, journaling, pacing—which are consistent with therapeutic strategies used in acceptance and commitment therapy (ACT) and mindfulness-based cognitive therapy [2, 13, 16]. By demonstrating how immigrants organically employ these techniques without formal training, this study identifies culturally grounded entry points for integrating mindfulness and acceptance-based interventions into community-level pain programs. These approaches supported psychological resilience even when physical pain remained, underscoring the importance of integrating psychosocial skill-building into culturally tailored pain programs [23, 26].
Experiences with healthcare providers constituted a major axis of divergence between positive adaptation and systemic disengagement. Negative encounters—characterized by stereotyping, rushed consultations, and cultural misunderstanding—paralleled findings from other studies showing systemic bias toward immigrant patients [17, 18]. Women, in particular, felt minimized or mischaracterized, reinforcing gendered vulnerability previously documented [8, 22]. Conversely, positive, empathic encounters—where providers listened, acknowledged cultural beliefs, and maintained continuity—restored trust and encouraged re-engagement. Beyond reaffirming the need for cultural competence, our data suggest specific policy implications: in diverse locales such as Richmond Hill, healthcare institutions should adopt mandatory annual training modules on immigrant pain narratives, intercultural communication, and interpreter-mediated care. Embedding such continuing education into licensing requirements could standardize empathy-based practice and reduce structural inequities in pain management. This reinforces calls for cross-cultural communication training and pain literacy among providers [4, 9]. When patients felt understood, adherence to treatment improved, and informal coping could be more safely integrated with biomedical care. In turn, these findings highlight the translational importance of coupling empathy training with structural supports—such as interpreter funding and culturally tailored pain education materials—to operationalize inclusion beyond individual goodwill.
The COVID-19 pandemic magnified existing inequities, disrupting healthcare access and worsening psychological strain. Our participants’ narratives of postponed appointments, intensified symptoms, and increased reliance on informal support echo emerging evidence on pandemic-driven disparities in chronic pain care [20, 21]. By situating these experiences within the broader context of migration-related stress and health system fragmentation, the study reveals how crisis conditions accentuate vulnerabilities unique to immigrant populations. These findings underscore that “universal” systems still leave immigrants vulnerable without targeted strategies addressing language, financial, and cultural barriers.
Conclusion
This study illuminates how chronic pain management among immigrant adults is profoundly shaped by the interplay of cultural beliefs, systemic barriers, emotional coping strategies, and healthcare experiences. The findings challenge the adequacy of a purely biomedical perspective and argue for approaches that honor personal narratives, cultural explanatory models, and social realities. Beyond local relevance, these findings also underscore the potential for scalability—offering a foundation for developing national guidelines that adapt locally effective, culturally responsive pain management models into broader healthcare frameworks across Canada. By centering immigrants’ voices, this research contributes to a more inclusive understanding of chronic pain and calls for integrative, empathetic, and equitable care practices that are responsive to diverse cultural and migration-related contexts.
Several limitations should be acknowledged. First, the sample was restricted to immigrants residing in Richmond Hill, an urban area with its own demographic profile and healthcare infrastructure; therefore, the transferability of findings to rural settings or other urban centers with different cultural compositions may be limited. Second, although purposive sampling sought maximum variation, participants who volunteered might have been those more comfortable discussing pain and healthcare, introducing potential self-selection bias. Third, language barriers may have constrained the richness of some interviews despite efforts to use accessible English and clarification techniques. Finally, the research team was composed of non-immigrant investigators; although reflexivity and peer debriefing were applied, some subtle cultural nuances may not have been fully captured.
To advance this field, future research should directly address the identified conceptual and temporal gaps. Specifically, to bridge the underexplored dimension of acculturation, scholars should prioritize longitudinal tracking of explanatory model shifts and coping adaptations across different migration phases. Comparative analyses with non-immigrant populations can further clarify how sociocultural integration shapes pain expression and healthcare engagement. In addition, mixed-method approaches combining qualitative depth with quantitative mapping of acculturation trajectories help reveal the evolving interaction between belief systems, systemic adaptation, and clinical outcomes. Incorporating participatory and community-based methods—such as photovoice, narrative inquiry, or ethnographic observation—may yield deeper insight into the embodied and relational dimensions of pain. Finally, there is a critical need for intervention studies testing culturally adapted pain management programs that integrate traditional belief systems, resilience-building skills, and community-based support structures. Such interventions, if scaled through national policy frameworks, could inform equitable chronic pain strategies that reflect the lived diversity of immigrant experiences.
Healthcare providers working with immigrant populations should be trained in culturally responsive care, with explicit attention to diverse pain expressions and traditional health frameworks. Routine use of medical interpreters, culturally tailored pain education, and collaborative, patient-centered treatment planning should become standard. At the policy level, integrating these findings into national chronic pain action plans—through dedicated funding for interpreter services, multicultural clinical training, and community liaison roles—would help institutionalize culturally safe care. Policymakers should reduce systemic barriers—especially those related to language access, insurance gaps, and immigration-related fears—that discourage timely care-seeking. Integrating mental health support into pain management is essential for addressing trauma, loss, and acculturation stress. Finally, healthcare systems should actively build trust through continuity of care, respectful communication, and recognition of patients’ cultural identities as valid frameworks for understanding and addressing chronic pain.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of KMAN Research Institute, Richmond Hill, Canada (Code: KEC.2024.03C10. Prior to the commencement of the study, all participants were informed about the research objectives, the confidentiality of their responses, and their right to withdraw from the study at any point. Written informed consent was obtained from all participants. Measures were taken to ensure the anonymity of participants, and personal identifiers were removed or altered in the transcription process.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express our gratitude to all individuals who helped us to do the project.
References
- Goli F. Beyond Biology: The personality underpinnings of chronic pain. Journal of Personality and Psychosomatic Research. 2024; 2(2):1-3. [DOI:10.61838/kman.jppr.2.2.1]
- Alizadeh P, Kooshki S, Tarvirdizadeh H. The effectiveness of acceptance and commitment therapy and on pain intensity, childhood trauma, perfectionism and psychological flexibility in patients with chronic pain. Journal of Assessment and Research in Applied Counseling. 2023; 5(2):123-36. [DOI:10.61838/kman.jarac.5.2.15]
- Roman‐Juan J, Sánchez‐Rodríguez E, Solé E, Castarlenas E, Jensen MP, Miró J. Immigration background as a risk factor of chronic pain and high-impact chronic pain in children and adolescents living in Spain: differences as a function of age. Pain. 2024; 165(6):1372-9. [DOI:10.1097/j.pain.0000000000003142] [PMID]
- Grant AR, Westhorp G, Mardon AK, White M, Hibbert P, Karran EL, et al. How is chronic pain managed in rural Australia? A qualitative study exploring rural healthcare professional and consumer experiences. Australian Journal of Rural Health. 2025; 33(1):e70000. [DOI:10.1111/ajr.70000] [PMID]
- Mustafa N, Ramana S, MacNeill M, Watt‐Watson J, Einstein G. Chronic pain experiences of immigrant Indian women in Canada: A photovoice exploration. Canadian Journal of Pain. 2024; 8(2):2390355. [DOI:10.1080/24740527.2024.2390355] [PMID]
- Tsetseri MN, Keene DJ, Silman AJ, Dakin SG. Exploring the burden of chronic musculoskeletal pain in immigrant populations: A scoping review. Research Square. 2023. [DOI:10.21203/rs.3.rs-3109549/v1]
- Shen Q, Mu Y, Shin PY. Health behavior change in post-traumatic stress disorder: Patient perspectives. Journal of Personality and Psychosomatic Research. 2024; 2(3):35-42. [DOI:10.61838/kman.jppr.2.3.6]
- Campbell K, Ford‐Gilboe M, Kennedy K, Jackson KT, Mantler T, Oudshoorn A. Women's experiences of navigating chronic pain within the context of living with an episodic disability. Women's Health. 2022; 18:17455057221103994. [DOI:10.1177/17455057221103994] [PMID]
- Tsetseri MN, Keene DJ, Silman AJ, Dakin SG. Exploring the burden, prevalence and associated factors of chronic musculoskeletal pain in migrants from North Africa and Middle East living in Europe: A scoping review. BMC Public Health. 2024; 24(1):769. [DOI:10.1186/s12889-023-17542-2] [PMID]
- Hooshmandi R, Aljaberi MA, Hammadi F, Ma J. The impact of interoceptive awareness on pain catastrophizing and illness perception. Journal of Personality and Psychosomatic Research. 2024; 2(2):4-10. [DOI:10.61838/kman.jppr.2.2.2]
- Bulut S, Saadati N, Al-Dossary SA, Coelho O, Rostami M, Parsakia K, et al. Introspective awareness and its predictive power on health anxiety: A cross-sectional study. Journal of Research and Health. 2025; 15(1):71-80. [DOI:10.32598/JRH.15.1.2449.1]
- Ebrahimkhani M, Norouzi E, Hosseini A, Jamshidi F. A randomized controlled trial on cognitive therapy’s role in enhancing pain self-efficacy and reducing catastrophizing in breast cancer patients. Psychology of Woman Journal. 2024; 5(2):114-23. [DOI:10.61838/kman.pwj.5.2.15]
- Pouryounes Abkenar R, Ebrahimi Looyeh M, Shamsaldini A. The effectiveness of mindfulness-based cognitive therapy on quality of life and resilience in women with chronic pain. Applied Family Therapy Journal. 2024; 5(1):187-94. [DOI:10.61838/kman.aftj.5.1.20]
- Gholami Gharahchenagh K, Haghayegh SA, Jabalameli S, Raeisi Z. Structural model presentation of psychological maladjustment based on post-traumatic stress symptoms with the mediating role of ego strength in individuals with chronic pain. Applied Family Therapy Journal. 2024; 5(3):56-65. [DOI:10.61838/kman.aftj.5.3.6]
- Nakhaei Moghadam R, Bahrainian SA, Nasri M. The effectiveness of intensive and short-term dynamic psychotherapy on attachment styles, somatization and health anxiety in patients with chronic pain. Journal of Assessment and Research in Applied Counseling. 2024; 6(1):142-9. [DOI:10.61838/kman.jarac.6.1.16]
- Ensandoost T, Samari AA, Bayazi MH, Rajaei A. The effectiveness of acceptance and commitment therapy on psychological well-being in men and women with chronic musculoskeletal pain. Applied Family Therapy Journal. 2022; 3(4):404-20. [DOI:10.61838/kman.aftj.3.4.22]
- Crockett K, Lovo S, Irvine A, Trask C, Oosman S, McKinney V, et al. “Navigating chaos”: urban, rural, and remote patient experiences in accessing healthcare with indigenous and non-indigenous perspectives of living with chronic low back pain. Canadian Journal of Pain. 2024; 8(2):2318706. [DOI:10.1080/24740527.2024.2318706] [PMID]
- Nakase-Richardson R, Cotner BA, Agtarap SD, Martin AM, Ching D, O'Connor DR, et al. Provider perceived facilitators and barriers to identifying, perceiving, and seeking healthcare for chronic pain after TBI: a qualitative NIDILRR and VA TBI Model Systems Collaborative Project. Journal of Head Trauma Rehabilitation. 2024; 39(1):E1-14. [DOI:10.1097/HTR.0000000000000922]
- Martos-Méndez MJ, Jacinto LG, Hombrados‐Mendieta I, Melguizo-Garín A, Ruiz-Rodríguez I. Psychosocial and sociodemographic Determinants related to chronic diseases in immigrants residing in Spain. International Journal of Environmental Research and Public Health. 2022; 19(7):3900. [DOI:10.3390/ijerph19073900] [PMID]
- Smyrnioti ME, Batistaki C, Yotsidi V, Matsota P. A comparative study of the impact of the Covid-19 pandemic on mental health, healthcare access, and pain levels of patients with chronic pain from spring 2020 to spring 2021. Risk Management and Healthcare Policy. 2024; 17:1323-38.[DOI:10.2147/RMHP.S460184] [PMID]
- Parsirad M, Oomen-Lochtefeld S, Suerig B, Wang C. Has the COVID 19 pandemic impacted the management of chronic musculoskeletal pain? Current Rheumatology Reports. 2023; 25(7):128-43. [DOI:10.1007/s11926-023-01103-y] [PMID]
- Mustafa N, Einstein G, MacNeill M, Watt‐Watson J. The lived experiences of chronic pain among immigrant Indian-Canadian women: A phenomenological analysis. Canadian Journal of Pain. 2020; 4(3):40-50. [DOI:10.1080/24740527.2020.1768835] [PMID]
- Gholami Gharahchenagh K, Haghayegh SA, Jabalameli S, Raeisi Z. Structural modeling of psychological maladjustment based on resilience with the mediating role of ego strength in patients with chronic pain. Journal of Adolescent and Youth Psychological Studies. 2024; 5(2):140-8. [DOI:10.61838/kman.jayps.5.2.16]
- Kawi J, Reyes AT, Arenas RA. Exploring pain management among Asian immigrants with chronic pain: self-management and resilience. Journal of Immigrant and Minority Health. 2018; 21(5):1123-36. [DOI:10.1007/s10903-018-0820-8] [PMID]
- Dragioti E, Tsamakis K, Larsson B, Gerdle B. Predictive association between immigration status and chronic pain in the general population: results from the SwePain cohort. BMC Public Health. 2020; 20(1):1462. [DOI:10.1186/s12889-020-09546-z] [PMID]
- Aghaziarati A, Jun H, Dai GS. Mind-body interactions in chronic pain sufferers: A qualitative study on personality factors. Journal of Personality and Psychosomatic Research (JPPR). 2024; 1(3):27-33. [DOI:10.61838/kman.jppr.1.3.5]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2025/03/31 | Accepted: 2025/11/22 | Published: 2026/03/1
Received: 2025/03/31 | Accepted: 2025/11/22 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
