

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 189-194 |
Back to browse issues page


Ethics code: IR.MUMS.FHMPM.REC.1403.128
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mosa Farkhani E, Ghasemi K. Occupational Noise Exposure and Hypertension Risk in Textile Industry Workers: A Historical Cohort Study. J Research Health 2026; 16 (2) :189-194
URL: http://jrh.gmu.ac.ir/article-1-2778-en.html
URL: http://jrh.gmu.ac.ir/article-1-2778-en.html



1- Department of Epidemiology, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. , farkhanie@mums.ac.ir
2- Department of Epidemiology, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Epidemiology, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
Full-Text [PDF 562 kb]
(146 Downloads)
| Abstract (HTML) (756 Views)
Full-Text: (96 Views)
Introduction
Occupational noise pollution is one of the most widespread harmful physical exposures in industrial settings and has been linked to adverse auditory and non-auditory health outcomes [1]. With increasing industrialization, especially in textile manufacturing, workers are frequently exposed to prolonged high-decibel environments that may influence cardiovascular function [2]. Although the auditory impacts of noise exposure are well recognized, recent studies suggest that chronic exposure may contribute to systemic physiological responses, including elevated blood pressure and stress hormone dysregulation [3, 4]. Noise is not only a major cause of hearing impairment but has also been increasingly linked to non-auditory health issues, such as endocrine disruptions, sleep disturbances, and psychological stress. Despite mixed evidence, some occupational studies have shown plausible physiological mechanisms including activation of the hypothalamic–pituitary–adrenal axis and sympathetic nervous system.
Hypertension is a major public health concern, affecting over one billion people globally and contributing to significant morbidity and mortality through stroke, ischemic heart disease, and kidney failure [5]. Several studies have reported associations between occupational noise and elevated blood pressure or cardiovascular disease [6, 7]. However, these findings are inconsistent across populations and settings. For example, while some meta-analyses have found a significant positive association between chronic noise exposure and hypertension [8–17], others have failed to detect such links, possibly due to variations in study design, exposure assessment, population characteristics, or adjustments for confounding variables.
Given the high burden of hypertension and widespread exposure to noise in industrial sectors, understanding this relationship is essential for preventive occupational health strategies. Despite substantial literature, evidence from Iranian textile workers, a population with high exposure potential, remains limited. This study contributes methodologically by using a historical cohort design and classifying chronic noise exposure based on direct sound-level measurements at the workstation. Unlike many cross-sectional studies, we adjusted for demographic and lifestyle confounders, such as age, body mass index (BMI), and work experience. These methodological improvements aim to clarify inconsistencies in the literature and offer context-specific evidence for occupational health policymaking in similar industrial settings.
Methods
Study population and sampling
This historical cohort study was conducted in 2024 among 200 male textile workers in Mashhad City, Iran. Eligible participants were aged 25–55 years, had ≥5 years of work experience, and had no prior history of cardiovascular disease at the time of employment. The exclusion criteria included prior diagnosis of hypertension or cardiovascular disease before employment and incomplete medical records during the study period. The sample size was estimated based on a hypertension prevalence of 25%, confidence level of 95%, and precision of 6%, yielding a minimum sample of 200 using the Equation 1:
1. n=Z²P(1-P)/d²
A census sampling method was used, including all eligible workers.
Noise exposure assessment
The main exposure variable was workplace noise intensity, which was objectively measured using standardized and calibrated devices. Each workstation’s sound pressure level was measured using an ES1358 (SN:111102963) and TES52A (SN:110905495) sound level meter, both of which were verified by a TES1356 acoustic calibrator (SN:100607246) prior to data collection. Based on these measurements, participants were categorized into three exposure groups according to their average 8-hour time-weighted noise levels over the past five years [1]:
Low: 60–70 dB; Moderate: 75–85 dB; High: 85–95 dB
Outcome measurement
Hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg, diastolic blood pressure (DBP) ≥90 mmHg, or current antihypertensive medication use. Blood pressure was measured twice daily (pre- and post-shift) on two separate days using a Beurer BM28 sphygmomanometer, with the average used for diagnosis.
Covariates and data collection
Data on demographic and occupational variables, including age, BMI, education, marital status, work duration, smoking, substance use, comorbidities, and hearing loss, were collected via validated questionnaires and verified health records. Age was categorized as ≤40 and > 40 years due to occupational relevance.
Statistical analysis
Statistical analysis was performed using Stata software, version 16. Logistic regression models were used to estimate crude and adjusted odds ratios (ORs and AORs) for the association between noise exposure and hypertension. Adjustments were made for age, BMI, education, work duration, and other potential confounders. Model fitness was evaluated using the Hosmer–Lemeshow test and multicollinearity using variance inflation factors (VIF). A P<0.05 was considered statistically significant. A VIF threshold of >5 was considered indicative of multicollinearity; all covariates had VIF<2.
Results
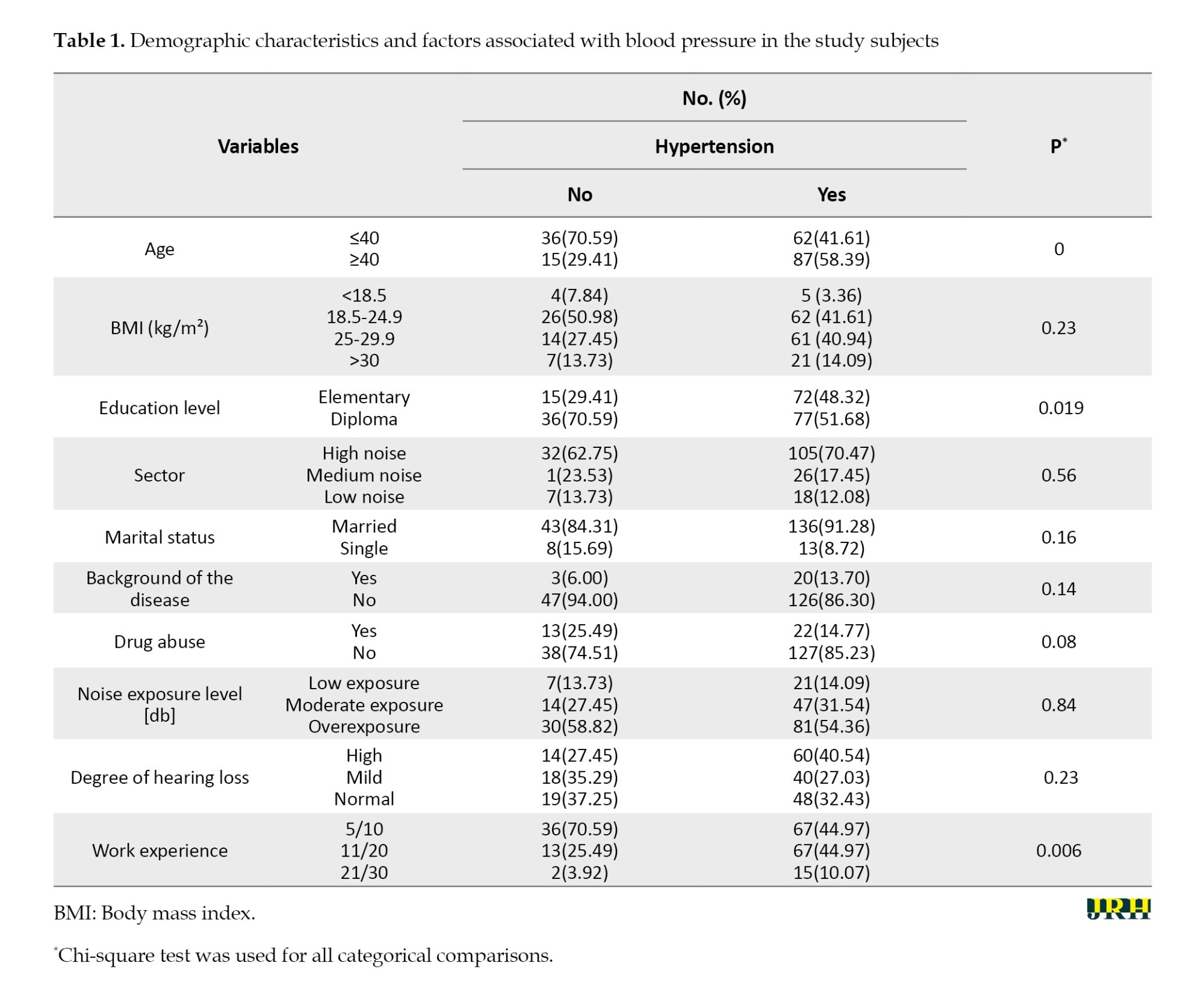
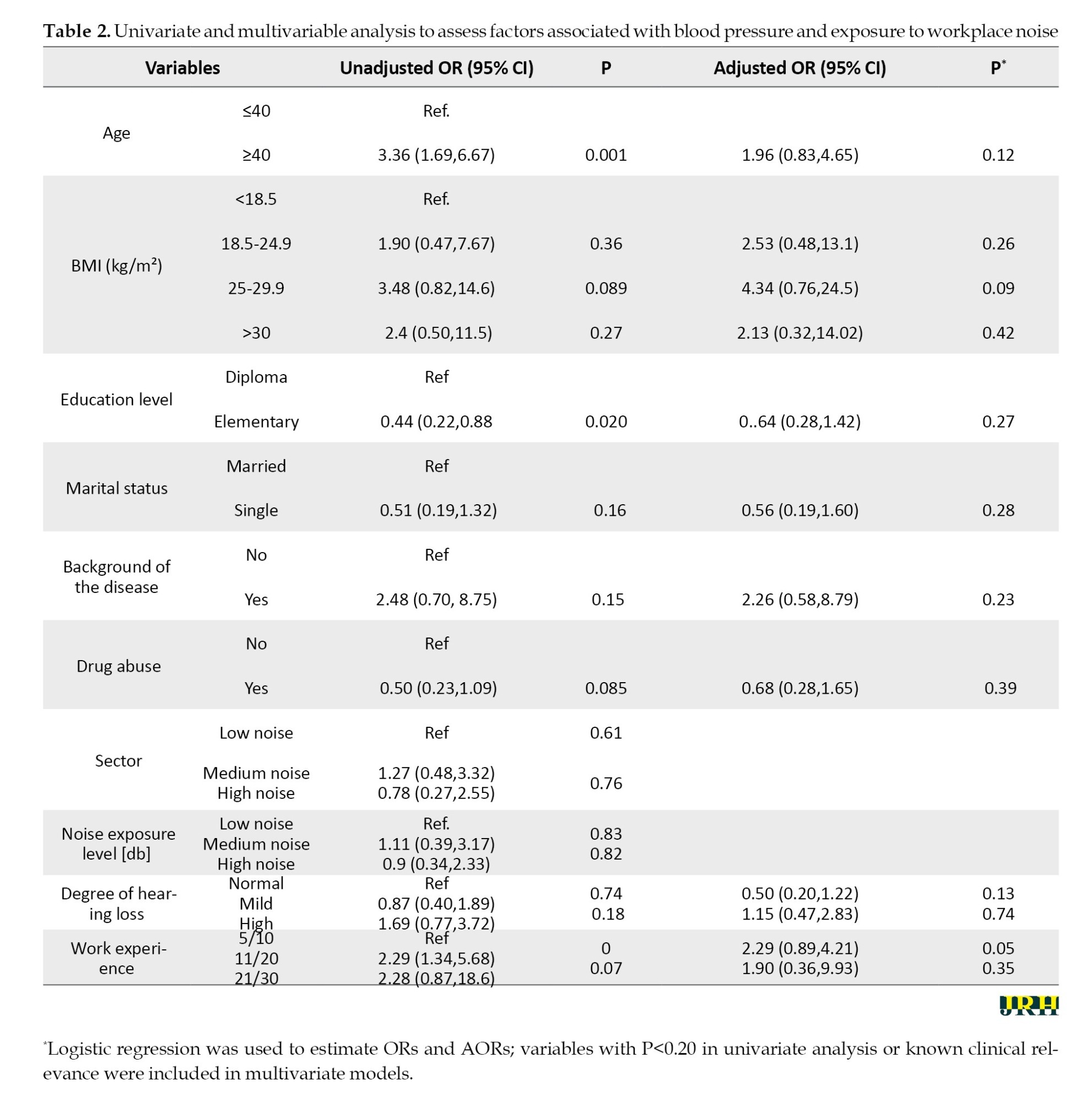
Of the 200 textile workers included in the study, 51 individuals (25.5%) met the criteria for hypertension. The mean age of participants was 42.3±7.5 years, and 61% were aged ≥40 years. The prevalence of hypertension was significantly higher among workers aged ≥40 compared to those ≤40 (58.4% vs 29.4%; P<0.001). In unadjusted logistic regression, age ≥40 was strongly associated with hypertension (OR=3.36; 95% CI, 1.69%, 6.67%; P<0.001), though the association attenuated and lost significance after adjustment for confounders (AOR=1.96; 95% CI, 0.83%, 4.65%; P=0.12). Age was categorized based on occupational risk stratification and retirement thresholds to improve interpretability.
Work experience was also associated with hypertension. Workers with 11–20 years of experience had a higher prevalence of hypertension (44.97%) than those with ≤10 years (25.49%) (P=0.006). In the multivariable model, 11–20 years of experience remained marginally associated with increased risk (AOR=2.29; 95% confidence interval [CI], 0.89%, 4.21%; P=0.05), holding other variables constant. Variables were included in the multivariable model based on clinical relevance and/or a univariate P<0.20.
BMI was not significantly associated with hypertension (P=0.23), although overweight participants (BMI 25–29.9) showed a higher, but statistically nonsignificant, adjusted risk (AOR=4.34; 95% CI, 0.76%, 24.5%; P=0.09). Similarly, education level, marital status, and comorbid disease history were not significantly associated with hypertension in adjusted models.
Noise exposure level (low: 60–70 dB; moderate: 75–85 dB; high: 85–95 dB) was not significantly associated with hypertension in either bivariate (P=0.84) or multivariable models. Compared to the low exposure group, neither moderate (AOR=1.11; 95% CI, 0.39%, 3.17%) nor high exposure (AOR=0.90; 95% CI, 0.34%, 2.33%) showed a statistically significant effect.
Although high-grade hearing loss was more common among hypertensive workers (40.5%) than among non-hypertensive workers (27.5%), the difference was not statistically significant (P=0.23). Table 1 summarizes the full distribution of demographic and occupational variables by hypertension status, and Table 2 presents regression estimates.
Discussion
This study evaluated the association between chronic workplace noise exposure and hypertension among textile workers in Mashhad. Although the overall prevalence of hypertension was substantial (25.5%), we found no statistically significant association between occupational noise exposure levels and hypertension after adjusting for confounders. Instead, age and work experience were more robust predictors of elevated blood pressure.
The observed association between age and hypertension aligns with established evidence demonstrating age as a dominant risk factor for increased vascular resistance and arterial stiffness [9, 10]. Similarly, the association with longer work experience may reflect cumulative occupational stress, consistent with findings from Rosenthal et al. [11]. and others who have linked prolonged job-related stress with adverse cardiovascular outcomes [12-14].
Contrary to some earlier studies suggesting a positive relationship between noise exposure and hypertension [15-17], our findings did not reveal a statistically significant effect. Several explanations may account for this inconsistency: Differences in noise exposure assessment, potential underestimation of cumulative or peak noise levels, or the use of hearing protection among workers. Moreover, cross-sectional noise measurements may not fully capture chronic exposure profiles, limiting exposure-response inferences.
Although hearing loss was more prevalent among hypertensive workers, the association was not statistically significant. However, this trend supports existing literature suggesting overlapping pathophysiological pathways involving oxidative stress and vascular dysfunction in both auditory and cardiovascular systems [3, 4].
The non-significant role of BMI and educational status, despite their known links with hypertension [18, 19], may be explained by the relatively homogenous socioeconomic and lifestyle characteristics in this workforce. Nonetheless, the inverse trend between education and hypertension aligns with prior reports highlighting the role of social determinants and health literacy in managing chronic disease risk [20, 21].
The limitations of this study include its retrospective design, reliance on periodic BP readings, potential residual confounding (e.g. psychosocial stressors and diet), and the healthy worker effect. Moreover, noise exposure was based on current workstation levels, which may not reflect historical exposure.
Conclusion
Our study investigated the association between occupational noise exposure and hypertension among textile industry workers, revealing significant correlations with age and work experience rather than direct noise exposure. These findings highlight the multifactorial nature of hypertension in occupational settings and underscore the necessity for comprehensive health programs addressing broader risk factors, including age and employment duration.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences, Mashhad, Iran (Code: IR.MUMS.FHMPM.REC.1403.128) and conducted in accordance with the Declaration of Helsinki. This study was conducted in compliance with ethical standards and regulations, ensuring the protection of participants’ rights and confidentiality.
Funding
This research was funded by Mashhad University of Medical Sciences, Mashhad, Iran (Grant No.: 4030696).
Authors' contributions
Conceptualization, methodology, data analysis, manuscript drafting, and final approval: Ehsan Mosa Farkhani;
Data collection, literature review, manuscript preparation, and final approval: Khadijah Ghasemi.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The author sincerely thanks the factory managers and personnel for their valuable cooperation and support throughout the conduct of this study.
References
Occupational noise pollution is one of the most widespread harmful physical exposures in industrial settings and has been linked to adverse auditory and non-auditory health outcomes [1]. With increasing industrialization, especially in textile manufacturing, workers are frequently exposed to prolonged high-decibel environments that may influence cardiovascular function [2]. Although the auditory impacts of noise exposure are well recognized, recent studies suggest that chronic exposure may contribute to systemic physiological responses, including elevated blood pressure and stress hormone dysregulation [3, 4]. Noise is not only a major cause of hearing impairment but has also been increasingly linked to non-auditory health issues, such as endocrine disruptions, sleep disturbances, and psychological stress. Despite mixed evidence, some occupational studies have shown plausible physiological mechanisms including activation of the hypothalamic–pituitary–adrenal axis and sympathetic nervous system.
Hypertension is a major public health concern, affecting over one billion people globally and contributing to significant morbidity and mortality through stroke, ischemic heart disease, and kidney failure [5]. Several studies have reported associations between occupational noise and elevated blood pressure or cardiovascular disease [6, 7]. However, these findings are inconsistent across populations and settings. For example, while some meta-analyses have found a significant positive association between chronic noise exposure and hypertension [8–17], others have failed to detect such links, possibly due to variations in study design, exposure assessment, population characteristics, or adjustments for confounding variables.
Given the high burden of hypertension and widespread exposure to noise in industrial sectors, understanding this relationship is essential for preventive occupational health strategies. Despite substantial literature, evidence from Iranian textile workers, a population with high exposure potential, remains limited. This study contributes methodologically by using a historical cohort design and classifying chronic noise exposure based on direct sound-level measurements at the workstation. Unlike many cross-sectional studies, we adjusted for demographic and lifestyle confounders, such as age, body mass index (BMI), and work experience. These methodological improvements aim to clarify inconsistencies in the literature and offer context-specific evidence for occupational health policymaking in similar industrial settings.
Methods
Study population and sampling
This historical cohort study was conducted in 2024 among 200 male textile workers in Mashhad City, Iran. Eligible participants were aged 25–55 years, had ≥5 years of work experience, and had no prior history of cardiovascular disease at the time of employment. The exclusion criteria included prior diagnosis of hypertension or cardiovascular disease before employment and incomplete medical records during the study period. The sample size was estimated based on a hypertension prevalence of 25%, confidence level of 95%, and precision of 6%, yielding a minimum sample of 200 using the Equation 1:
1. n=Z²P(1-P)/d²
A census sampling method was used, including all eligible workers.
Noise exposure assessment
The main exposure variable was workplace noise intensity, which was objectively measured using standardized and calibrated devices. Each workstation’s sound pressure level was measured using an ES1358 (SN:111102963) and TES52A (SN:110905495) sound level meter, both of which were verified by a TES1356 acoustic calibrator (SN:100607246) prior to data collection. Based on these measurements, participants were categorized into three exposure groups according to their average 8-hour time-weighted noise levels over the past five years [1]:
Low: 60–70 dB; Moderate: 75–85 dB; High: 85–95 dB
Outcome measurement
Hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg, diastolic blood pressure (DBP) ≥90 mmHg, or current antihypertensive medication use. Blood pressure was measured twice daily (pre- and post-shift) on two separate days using a Beurer BM28 sphygmomanometer, with the average used for diagnosis.
Covariates and data collection
Data on demographic and occupational variables, including age, BMI, education, marital status, work duration, smoking, substance use, comorbidities, and hearing loss, were collected via validated questionnaires and verified health records. Age was categorized as ≤40 and > 40 years due to occupational relevance.
Statistical analysis
Statistical analysis was performed using Stata software, version 16. Logistic regression models were used to estimate crude and adjusted odds ratios (ORs and AORs) for the association between noise exposure and hypertension. Adjustments were made for age, BMI, education, work duration, and other potential confounders. Model fitness was evaluated using the Hosmer–Lemeshow test and multicollinearity using variance inflation factors (VIF). A P<0.05 was considered statistically significant. A VIF threshold of >5 was considered indicative of multicollinearity; all covariates had VIF<2.
Results
Of the 200 textile workers included in the study, 51 individuals (25.5%) met the criteria for hypertension. The mean age of participants was 42.3±7.5 years, and 61% were aged ≥40 years. The prevalence of hypertension was significantly higher among workers aged ≥40 compared to those ≤40 (58.4% vs 29.4%; P<0.001). In unadjusted logistic regression, age ≥40 was strongly associated with hypertension (OR=3.36; 95% CI, 1.69%, 6.67%; P<0.001), though the association attenuated and lost significance after adjustment for confounders (AOR=1.96; 95% CI, 0.83%, 4.65%; P=0.12). Age was categorized based on occupational risk stratification and retirement thresholds to improve interpretability.
Work experience was also associated with hypertension. Workers with 11–20 years of experience had a higher prevalence of hypertension (44.97%) than those with ≤10 years (25.49%) (P=0.006). In the multivariable model, 11–20 years of experience remained marginally associated with increased risk (AOR=2.29; 95% confidence interval [CI], 0.89%, 4.21%; P=0.05), holding other variables constant. Variables were included in the multivariable model based on clinical relevance and/or a univariate P<0.20.
BMI was not significantly associated with hypertension (P=0.23), although overweight participants (BMI 25–29.9) showed a higher, but statistically nonsignificant, adjusted risk (AOR=4.34; 95% CI, 0.76%, 24.5%; P=0.09). Similarly, education level, marital status, and comorbid disease history were not significantly associated with hypertension in adjusted models.
Noise exposure level (low: 60–70 dB; moderate: 75–85 dB; high: 85–95 dB) was not significantly associated with hypertension in either bivariate (P=0.84) or multivariable models. Compared to the low exposure group, neither moderate (AOR=1.11; 95% CI, 0.39%, 3.17%) nor high exposure (AOR=0.90; 95% CI, 0.34%, 2.33%) showed a statistically significant effect.
Although high-grade hearing loss was more common among hypertensive workers (40.5%) than among non-hypertensive workers (27.5%), the difference was not statistically significant (P=0.23). Table 1 summarizes the full distribution of demographic and occupational variables by hypertension status, and Table 2 presents regression estimates.
Discussion
This study evaluated the association between chronic workplace noise exposure and hypertension among textile workers in Mashhad. Although the overall prevalence of hypertension was substantial (25.5%), we found no statistically significant association between occupational noise exposure levels and hypertension after adjusting for confounders. Instead, age and work experience were more robust predictors of elevated blood pressure.
The observed association between age and hypertension aligns with established evidence demonstrating age as a dominant risk factor for increased vascular resistance and arterial stiffness [9, 10]. Similarly, the association with longer work experience may reflect cumulative occupational stress, consistent with findings from Rosenthal et al. [11]. and others who have linked prolonged job-related stress with adverse cardiovascular outcomes [12-14].
Contrary to some earlier studies suggesting a positive relationship between noise exposure and hypertension [15-17], our findings did not reveal a statistically significant effect. Several explanations may account for this inconsistency: Differences in noise exposure assessment, potential underestimation of cumulative or peak noise levels, or the use of hearing protection among workers. Moreover, cross-sectional noise measurements may not fully capture chronic exposure profiles, limiting exposure-response inferences.
Although hearing loss was more prevalent among hypertensive workers, the association was not statistically significant. However, this trend supports existing literature suggesting overlapping pathophysiological pathways involving oxidative stress and vascular dysfunction in both auditory and cardiovascular systems [3, 4].
The non-significant role of BMI and educational status, despite their known links with hypertension [18, 19], may be explained by the relatively homogenous socioeconomic and lifestyle characteristics in this workforce. Nonetheless, the inverse trend between education and hypertension aligns with prior reports highlighting the role of social determinants and health literacy in managing chronic disease risk [20, 21].
The limitations of this study include its retrospective design, reliance on periodic BP readings, potential residual confounding (e.g. psychosocial stressors and diet), and the healthy worker effect. Moreover, noise exposure was based on current workstation levels, which may not reflect historical exposure.
Conclusion
Our study investigated the association between occupational noise exposure and hypertension among textile industry workers, revealing significant correlations with age and work experience rather than direct noise exposure. These findings highlight the multifactorial nature of hypertension in occupational settings and underscore the necessity for comprehensive health programs addressing broader risk factors, including age and employment duration.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences, Mashhad, Iran (Code: IR.MUMS.FHMPM.REC.1403.128) and conducted in accordance with the Declaration of Helsinki. This study was conducted in compliance with ethical standards and regulations, ensuring the protection of participants’ rights and confidentiality.
Funding
This research was funded by Mashhad University of Medical Sciences, Mashhad, Iran (Grant No.: 4030696).
Authors' contributions
Conceptualization, methodology, data analysis, manuscript drafting, and final approval: Ehsan Mosa Farkhani;
Data collection, literature review, manuscript preparation, and final approval: Khadijah Ghasemi.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The author sincerely thanks the factory managers and personnel for their valuable cooperation and support throughout the conduct of this study.
References
- Mohammadi G. Occupational Noise Pollution and Hearing protection in selected industries. Iranian Journal of Health, Safety and Environment. 2014; 1(1):30-5. [Link]
- Waye KP, Öhrström E. Psycho-acoustic characters of relevance for annoyance of wind turbine noise. Journal of Sound and Vibration. 2002; 250(1):65-73. [DOI:10.1006/jsvi.2001.3905]
- Münzel T, Schmidt FP, Steven S, Herzog J, Daiber A, Sørensen M. Environmental noise and the cardiovascular system. Journal of the American College of Cardiology. 2018; 71(6):688-97. [DOI:10.1016/j.jacc.2017.12.015] [PMID]
- Foraster M, Künzli N, Aguilera I, Rivera M, Agis D, Vila J, et al. High blood pressure and long-term exposure to indoor noise and air pollution from road traffic. Environmental Health Perspectives. 2014; 122(11):1193-200. [DOI:10.1289/ehp.1307156] [PMID]
- MacGregor GA, He FJ. Importance of controlling blood pressure. Climacteric. 2005; 8(S 3):13-8. [DOI:10.1080/13697130500330325] [PMID]
- Mohammad-Ghasemi M, Dehghani-Bidgoli S, Ahmadi T, Nikbakht N, Heidarifar S, Sadeghi-Yarandi M. Investigating the effect of workplace noise exposure on cardiovascular disease risk factors in a power plant industry: A case-control study. Work. 2023; 76(4):1429-40. [DOI:10.3233/WOR-220396] [PMID]
- Melamed S, Fried Y, Froom P. The interactive effect of chronic exposure to noise and job complexity on changes in blood pressure and job satisfaction: a longitudinal study of industrial employees. Journal of Occupational Health Psychology. 2001; 6(3):182-95. [PMID]
- Pawlaczyk-Łuszczyńska M, Dudarewicz A, Waszkowska M, Szymczak W, Śliwińska-Kowalska M. The impact of low frequency noise on human mental performance. International Journal of Occupational Medicine & Environmental Health. 2005; 18(2):185-98. [PMID]
- Azizi A, Abasi M, Abdoli G. [The prevalence of hypertension and its association with age, sex and BMI in a population being educated using community-based medicine in Kermanshah: 2003 (Persian)]. Iranian Journal of Endocrinology and Metabolism. 2008; 10(4):323-9. [Link]
- Rampal L, Rampal S, Azhar MZ, Rahman AR. Prevalence, awareness, treatment and control of hypertension in Malaysia: A national study of 16,440 subjects. Public Health. 2008; 122(1):11-8. [DOI:10.1016/j.puhe.2007.05.008] [PMID]
- Rosenthal T, Alter A. Occupational stress and hypertension. Journal of the American Society of Hypertension. 2012; 6(1):2-22. [DOI:10.1016/j.jash.2011.09.002] [PMID]
- Lazaridis K, Jovanović J, Jovanović J, Šarac I, Jovanović S. The impact of occupational stress factors on temporary work disability related to arterial hypertension and its complications. International Journal of Occupational Safety and Ergonomics. 2017; 23(2):259-66. [DOI:10.1080/10803548.2016.1179524] [PMID]
- Hu S, Xu X, Li C, Zhang L, Xing X, He J, et al. Long-term exposure to ambient ozone at workplace is positively and non-linearly associated with incident hypertension and blood pressure: longitudinal evidence from the Beijing-Tianjin-Hebei medical examination cohort. BMC Public Health. 2023; 23(1):2011. [DOI:10.1186/s12889-023-16932-w] [PMID]
- Khonde Kumbu R, Matondo H, Labat A, Kianu B, Godin I, Kiyombo G, et al. Job stress, a source of hypertension among workers in Sub-saharan Africa: A scoping review. BMC Public Health. 2023; 23(1):2316. [DOI:10.1186/s12889-023-17248-5] [PMID]
- Bolm-Audorff U, Hegewald J, Pretzsch A, Freiberg A, Nienhaus A, Seidler A. Occupational noise and hypertension risk: a systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2020; 17(17):6281. [DOI:10.3390/ijerph17176281] [PMID]
- Yang Y, Zhang E, Zhang J, Chen S, Yu G, Liu X, et al. Relationship between occupational noise exposure and the risk factors of cardiovascular disease in China: a meta-analysis. Medicine. 2018; 97(30):e11720. [DOI:10.1097/MD.0000000000011720] [PMID]
- Sivakumaran K, Ritonja JA, Waseem H, AlShenaibar L, Morgan E, Ahmadi SA, et al. Impact of noise exposure on risk of developing stress-related health effects related to the cardiovascular system: A systematic review and meta-analysis. Noise and Health. 2022; 24(114):107-29. [DOI:10.4103/nah.nah_83_21]
- Chaturvedi A, Zhu A, Gadela NV, Prabhakaran D, Jafar TH. Social determinants of health and disparities in hypertension and cardiovascular diseases. Hypertension. 2024; 81(3):387-99. [DOI:10.1161/HYPERTENSIONAHA.123.21354] [PMID]
- Blok S, Haggenburg S, Collard D, Van Der Linden EL, Galenkamp H, Van Charante EPM, et al. The association between socioeconomic status and prevalence, awareness, treatment and control of hypertension in different ethnic groups: the Healthy Life in an Urban Setting study. Journal of hypertension. 2022; 40(5):897-907. [DOI:10.1097/HJH.0000000000003092] [PMID]
- Abba MS, Nduka CU, Anjorin S, Mohamed SF, Agogo E, Uthman OA. Influence of contextual socioeconomic position on hypertension risk in low-and middle-income countries: disentangling context from composition. BMC public health. 2021; 21(1):2218. [DOI:10.1186/s12889-021-12238-x] [PMID]
- Kibria GMA, Swasey K, Sharmeen A, Sakib MN, Burrowes V. Prevalence and associated factors of pre-hypertension and hypertension in Nepal: Analysis of the Nepal Demographic and Health Survey 2016. Health science reports. 2018; 1(10):e83. [DOI:10.1002/hsr2.83] [PMID]
Type of Study: Short Communication |
Subject:
● Disease Control
Received: 2025/04/8 | Accepted: 2025/06/25 | Published: 2026/03/1
Received: 2025/04/8 | Accepted: 2025/06/25 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
