

Volume 16, Issue 3 (May & June 2026)
J Research Health 2026, 16(3): 243-254 |
Back to browse issues page

Ethics code: IRCT2016030510426N10
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alafchi N, Norouzi M, Eghbalian M. The Effect of Health Education on Self-efficacy, Social Support, and Perceived Barriers in the Postpartum Period. J Research Health 2026; 16 (3) :243-254
URL: http://jrh.gmu.ac.ir/article-1-2796-en.html
URL: http://jrh.gmu.ac.ir/article-1-2796-en.html



1- Department of Science in Midwifery, School of School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran.
2- Department of Epidemiology and Biostatistics, School of Health, Shahrekord University of Medical Sciences, Shahrekord, Iran.
3- Department of Public Health, Social Determinants of Health Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran. ,eghbalian1992@gmail.com
2- Department of Epidemiology and Biostatistics, School of Health, Shahrekord University of Medical Sciences, Shahrekord, Iran.
3- Department of Public Health, Social Determinants of Health Research Center, School of Health, Gonabad University of Medical Sciences, Gonabad, Iran. ,
Full-Text [PDF 816 kb]
(185 Downloads)
| Abstract (HTML) (470 Views)
Full-Text: (24 Views)
Introduction
Postpartum care plays a vital role in ensuring the survival and longterm health of mothers and their newborns during the initial six weeks following childbirth, a period during which the majority of maternal and infant deaths occur [1]. According to the World Health Organization (WHO), over 30% of women and newborns worldwide do not receive postnatal care during these crucial early days, leaving many physical and emotional consequences of childbirth untreated, which can be debilitating but are often manageable with timely care [2].
Lack of postpartum care leads to significant adverse outcomes for mothers and infants, including increased risks of long-term physical and mental health problems and higher mortality rates. A 2024 study found that more than one-third of women experience persistent health issues after childbirth, such as dyspareunia (35%), low back pain (32%), anxiety (9–24%), and depression (11–17%), many of which remain underrecognized and untreated without adequate postpartum care [3]. Postpartum depression affects a mother’s physical and mental health, relationships, and daily functioning, and it also has significant consequences for the infant’s growth, health, sleep patterns, and various aspects of development, such as motor skills, cognition, language, emotional regulation, social behavior, and overall well-being. Additionally, it negatively influences mother–infant interactions, including bonding, breastfeeding, and the mother’s ability to fulfill her maternal role [4, 5].
Implementation of effective postpartum care is hindered by numerous obstacles, particularly those stemming directly from the mother’s circumstances. A key issue is that some women may not fully understand the importance of postpartum care or may perceive it as unnecessary, leading to reduced engagement with services. Furthermore, limited family or social support, psychological stress, and broader socioeconomic factors can hinder a woman’s ability to access essential postpartum services [6, 7].
Self-efficacy, social support, and perceived barriers are key psychosocial determinants that influence women’s ability to address and overcome challenges related to postpartum care [8-10]. Self-efficacy can impact various aspects of maternal health during the postpartum period. Mothers higher confidence in their breastfeeding abilities are better equipped to manage breastfeeding related difficulties. This can improve both the quality and duration of breastfeeding [11]. Physical activity self-efficacy refers to an individual’s confidence in their ability to maintain physical activity even when facing challenges. This confidence is a key factor in initiating and maintaining new health promoting behaviors [12]. A study’s findings indicate a significant association between maternal health literacy and physical activity self efficacy. Insufficient knowledge about a particular health issue can negatively impact individuals’ confidence in their ability to follow a self-care plan [13].
Although social support is defined in various ways, research consistently demonstrates a strong correlation between social support and mothers’ mental health during the postpartum period [14]. Postpartum social support is vital for maternal recovery, helping to prevent mental health disorders and reduce stress. Furthermore, it promotes lasting health benefits for both children and their mothers [15].
Perceived barriers can be categorized into intrapersonal, interpersonal, and environmental factors. Conditions, such as postpartum depression and anxiety, significantly impact women’s perceptions of their capabilities and overall health [16]. Concerns about burdening others or straining relationships can inhibit women from seeking assistance when needed [17]. Women often face challenges related to transportation, financial constraints, and availability of appropriate services (e.g. childcare, health care) that can limit their ability to engage in postpartum care [6].
Counseling is a crucial intervention that empowers individuals to improve their quality of life [18]. It facilitates active listening, mutual understanding, responsive communication, and targeted interventions [19]. A continuum of care approach beginning in the third trimester and extending through the postpartum period may provide more comprehensive counseling to address patients’ concerns [20]. Therefore, there is a clear demand for interventions like counseling.
While some studies in Iran have explored interventions, such as clinical guidelines, supportive counseling, and various educational programs during the postpartum period [21, 22], a notable research gap persists regarding group-based counseling interventions for first-time mothers. In particular, few studies have addressed interventions that concurrently address self-efficacy, social support, and perceived barriers. These three constructs are critical. Self-efficacy enhances mothers’ confidence to engage in health-promoting behaviors, social support provides emotional and practical resources that improve mental health and coping, and perceived barriers often hinder the adoption of healthy practices. Addressing all three within a group counseling framework could significantly improve maternal health outcomes, such as breastfeeding success, postpartum depression reduction, and adherence to care. This study aimed to evaluate the effects of a structured counseling intervention on key psychosocial factors among postpartum mothers. Specifically, it examined how counseling influences maternal self-efficacy, perceived social support, and perceived barriers to adopting health-promoting behaviors during the postpartum period.
Methods
Study design and sampling
A randomized controlled trial with a parallel-group design was conducted involving 112 first-time mothers recruited from Hamadan University of Medical Sciences, Iran. No changes were made after trial commencement. A two-stage cluster sampling strategy was employed to ensure a representative sample within Hamadan City. In the first stage, the city was divided into five geographical zones based on official administrative boundaries and population distribution data. These regions served as clusters representing different community profiles. In the second stage, two health centers were randomly selected from each geographical region, resulting in a total of 10 centers out of 20 operating in Hamadan City. To allocate health centers to intervention conditions, a randomization process was conducted at the cluster (health center) level rather than the individual level. This approach minimized the risk of contamination between groups. The 10 selected health centers were randomly assigned to the intervention group (counseling plus standard care) or the control group (standard care only), with five centers per group. Within each selected health center, eligible first-time mothers were contacted and screened for inclusion. Mothers who had undergone cesarean delivery were excluded to maintain sample homogeneity regarding delivery type. If an eligible participant declined or did not meet the inclusion criteria, a replacement was recruited using the same procedures within the same center to maintain cluster integrity and sample size. Randomization of clusters into groups employed a permuted-block design at the cluster level, with block sizes of four to six centers to ensure balanced allocation across regions. The randomization sequence was computer-generated by an independent researcher not involved in recruitment or data collection. Allocation was concealed using sealed opaque envelopes, which were confirmed eligible. Participants in both groups completed standardized questionnaires administered through face-to-face interviews by trained research staff. This approach aimed to reduce missing data and ensure consistency in data collection.
Inclusion and exclusion criteria
The inclusion criteria included literacy in Persian to ensure comprehension of study materials and questionnaires; vaginal childbirth, as the study specifically aimed to evaluate outcomes in this population and avoid potential confounding effects associated with cesarean deliveries, which can differ significantly in maternal recovery and breastfeeding outcomes; delivery of healthy, full-term infants weighing between 2500 and 4000 grams to exclude infants with low or high birth weight that might affect maternal and infant health; absence of physical or psychiatric conditions and obstetric complications during the current pregnancy, to reduce variability due to underlying health factors that could influence study measures; and non-participation in other educational programs to avoid potential contamination of the intervention effects. Mothers and infants hospitalized for more than 48 hours post-delivery were excluded to ensure a more uniform postpartum recovery period, as prolonged hospitalization could impact participation and outcomes. Mothers who missed two or more counseling sessions were excluded to maintain intervention fidelity and protocol adherence; adherence to the counseling sessions was monitored through attendance logs maintained by the facilitators, and participants were contacted promptly upon missed sessions to encourage ongoing engagement. The threshold of two missed sessions was based on prior literature indicating that reduced session attendance can significantly diminish intervention effectiveness [23].
Additionally, mothers who underwent divorce during the study period were excluded due to the potential psychosocial stressors impacting study outcomes. Mothers who were unable to breastfeed, suffered severe infections, or experienced postpartum hemorrhage were excluded because these conditions could directly affect both maternal and infant health and confound the assessment of the counseling program’s effects.
Randomization
Participants were randomly assigned to the intervention or control group according to the cluster level permuted block randomization with a 1:1 allocation ratio. Randomization was performed by a researcher not involved in participant recruitment or intervention delivery to ensure allocation concealment. To maintain confidentiality, each participant received a unique identification code placed inside sealed, and opaque envelopes, which were opened sequentially at enrollment. The control group received standard care, while the intervention group received standard care plus the counseling interventions. Due to the nature of the counseling intervention, participants and facilitators were not blinded to group assignment. However, outcome assessors and the data analyst were blinded to group allocation to minimize assessment and analysis bias. Participants in the experimental group were further divided into 10 small counseling groups, each consisting of 5_10 participants, to facilitate more personalized and effective delivery. Missing data from the questionnaires were anticipated due to potential non-response or incomplete answers. To address this, questionnaires were checked for completeness at the time of collection, and participants were encouraged to complete missing items whenever feasible. Quality control measures included training sessions for intervention facilitators to standardize the delivery of counseling, regular supervision meetings to ensure protocol adherence, and periodic audits of data entries. An independent data monitoring committee periodically reviewed study progress and data quality.
Data collection tool
Four questionnaires were used for data collection. The first questionnaire collected socio-demographic information about the participants, including details, such as the mother’s age, employment status, education level, housing situation, whether the pregnancy was planned, the newborn’s gender, and any history of abortion.
Perceived self-efficacy questionnaire
This tool has been previously validated and shown to be reliable for use in the Iranian context [24]. This questionnaire consists of 8 questions, each rated on a 5-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree.’ For questions 8, 6, 5, 4, 2, and 1, the scoring is from 1 to 5, while questions 3 and 7 are scored in reverse. The total score ranges from 8 to 40, with higher scores indicating a greater ability to manage the outcomes of health-related programs. The questionnaire’s reliability was assessed using Cronbach’s α, yielding a coefficient of 0.81. To ensure validity, the content validity method was employed, involving feedback from 7 nursing and midwifery faculty members and 2 health faculty members, which led to necessary revisions.
Perceived social support questionnaire
This 16-question questionnaire is structured into two parts. The first part includes 10 questions using a 4-point Likert scale, with options ranging from ‘a lot’ to ‘not at all,’ scored from 3 to 0. The second part, questions 11 to 16, uses a binary ‘yes/no’ format, where ‘yes’ is scored as 1 and ‘no’ as 0. Scores range from 0 to 36, with higher scores indicating perceived social support. In our study, the reliability was confirmed at 0.92 using Cronbach’s α. To ensure validity, we also employed content validation, distributing the questionnaire to 7 nursing and midwifery faculty members and 2 health faculty members, which led to necessary revisions.
Perceived barriers questionnaire
This questionnaire comprises 18 items, measured on a 4-point Likert scale with options ranging from ‘never’ to ‘always,’ scored from 1 to 4. It assesses the barriers that hinder respondents from engaging in health-promoting behaviors. The total score can range from 18 to 72, with higher scores indicating more significant obstacles to adopting healthy behaviors. In our study, the questionnaire’s reliability was confirmed with a Cronbach’s α coefficient of 0.81. Additionally, content validity was ensured by distributing the questionnaire to 7 nursing and midwifery faculty members and 2 health faculty members, leading to necessary revisions.
The content and face validity of this instrument were confirmed in Iran by Mohammadian et al. in 2009 at the University of Tehran, Iran, with a Cronbach’s α coefficient of 0.72 [24].
Counseling interventions
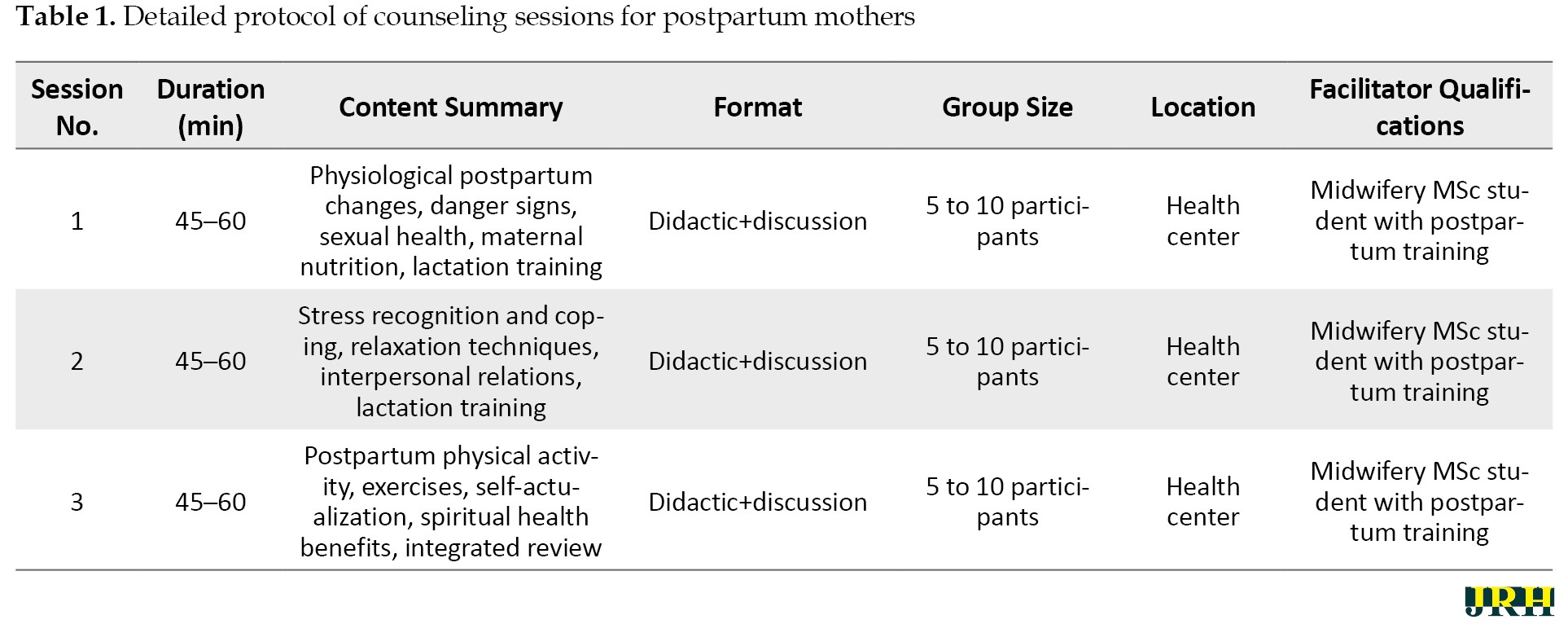
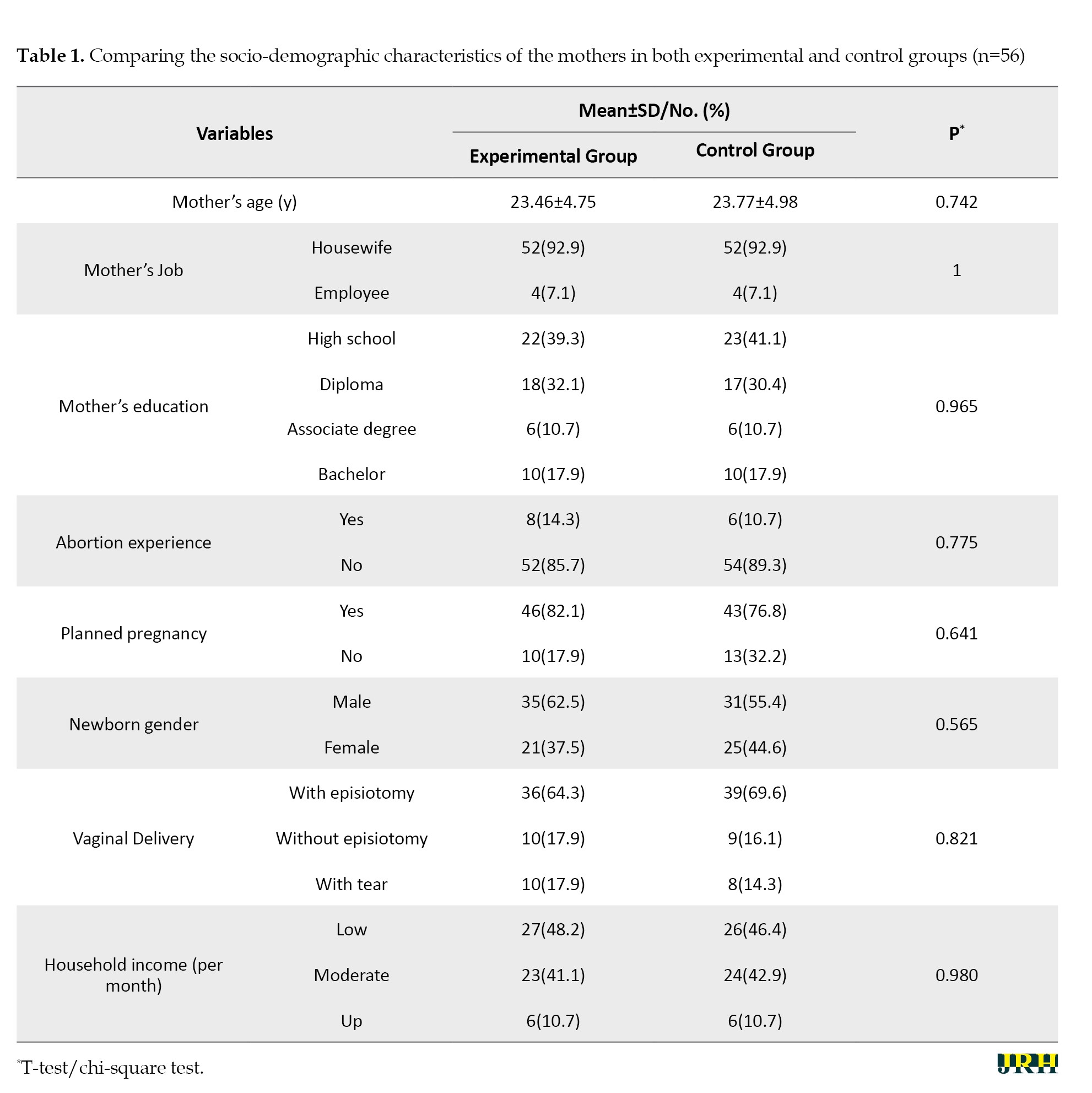
The experimental group participated in a structured counseling program conducted in small groups of 5–10 women at the health center, with each session lasting 45–60 minutes. These sessions were scheduled at specific postpartum intervals to address the evolving needs of new mothers. The first session, held 3–5 days postpartum, focused on group education for participants about physiological changes occurring during the postpartum period, identifying postpartum danger signs, sexual health concerns, lactation techniques, and maternal nutrition to support recovery and infant care. The second session took place 10–15 days postpartum and emphasized recognizing stress and its symptoms, teaching effective coping and relaxation methods, and exploring factors influencing interpersonal relationships. The third session was conducted 17–20 days postpartum and addressed the importance of physical activity by discussing suitable postpartum exercises, promoting self-actualization, enhancing spiritual well-being, and highlighting the overall benefits of maintaining good health during this critical period. Following the counseling sessions, weekly follow-up contacts were conducted for an additional three weeks to provide ongoing support, answer questions, and reinforce key messages, and participants were provided with contact information. Participants received a comprehensive booklet compiled from credible scientific sources, summarizing the advice and strategies discussed during the sessions to reinforce learning and provide a reference at home. To evaluate the intervention’s impact, mothers from both the experimental and control groups completed standardized questionnaires during routine postnatal care visits, approximately 42 days postpartum. After study completion, the booklet was offered to the control group to ensure equitable access to informational resources (Table 1).
Sample size
We considered a type I error rate (α) of 5%, a type II error rate (β) of 20%, and an attrition rate of 10%. Based on a previous study [25], the required sample size was calculated to be 60 participants per group [25].
Statistical analysis
Maternal occupation was categorized into two groups: Housewife and employee. This binary classification reflected the characteristics of the study population, in which most participants were either primarily homemakers or formally employed outside the home. This approach allowed us to clearly distinguish between mothers engaged in paid employment and those dedicating most of their time to household and childcare responsibilities. Due to sample size considerations and the need to maintain sufficient group numbers for meaningful statistical analysis, more detailed occupational categories were not used. Mean±SD were used for descriptive statistics. Difference in the mean or frequency of demographic variables between the two groups was examined using the independent t-test and the chi-square. Then, a paired t-test was used to compare the means before and after the intervention. If necessary, analysis of covariance (ANCOVA) was also performed. All statistical tests were performed at a 95% confidence level and using the SPSS software, version 24.
Results
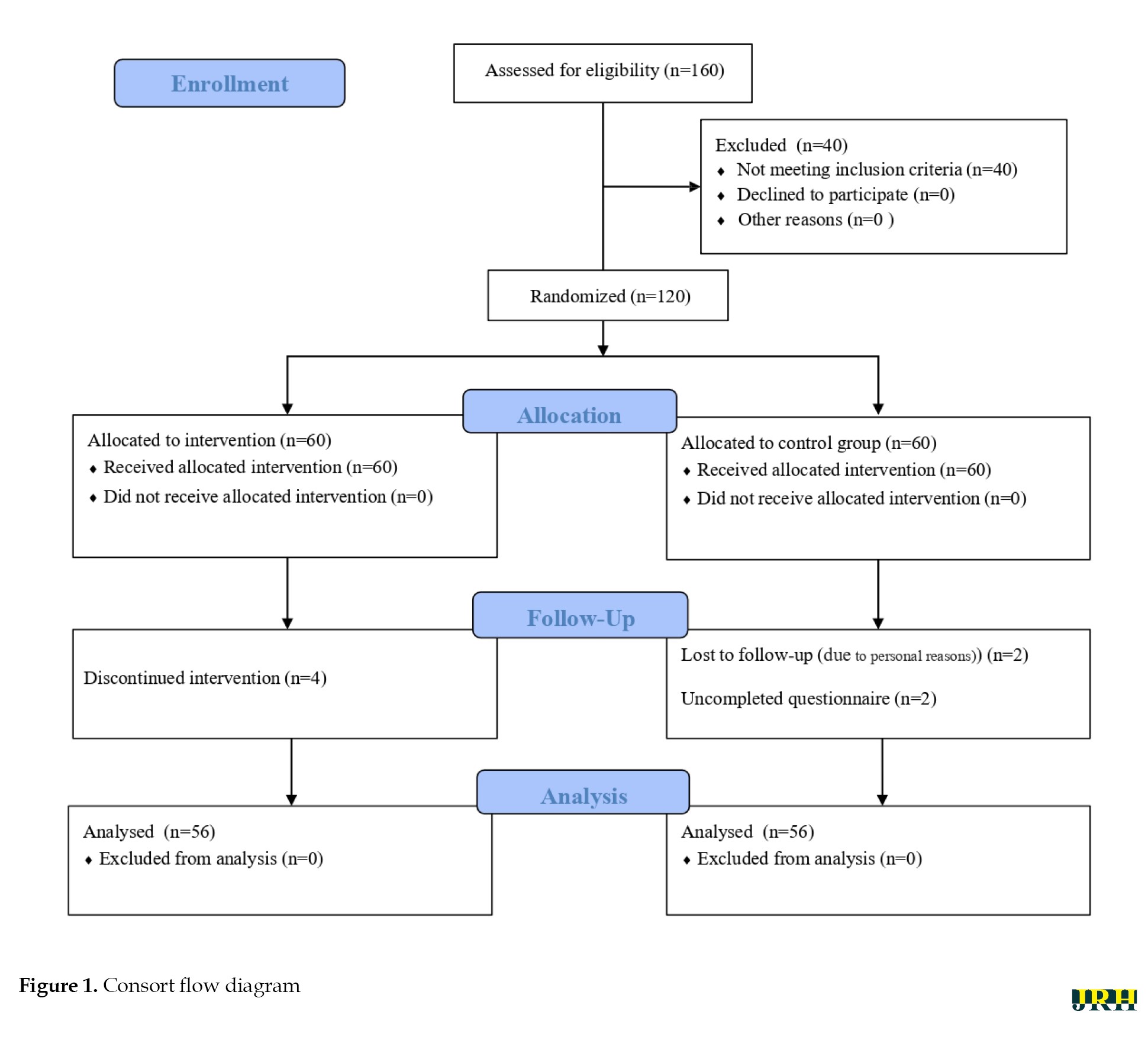
A total of 160 women completed informed consent and were assessed for eligibility, of whom 40 were excluded based on the predefined criteria. The remaining 120 eligible participants were randomly assigned equally to the experimental (n=60) and control (n=60) groups. During follow-up, four women in the experimental group discontinued the intervention for personal reasons. In the control group, two participants were lost to follow-up and two failed to complete the post-intervention questionnaire. Consequently, 56 women from each group completed the study and were included in the final analysis (Figure 1).
Postpartum care plays a vital role in ensuring the survival and longterm health of mothers and their newborns during the initial six weeks following childbirth, a period during which the majority of maternal and infant deaths occur [1]. According to the World Health Organization (WHO), over 30% of women and newborns worldwide do not receive postnatal care during these crucial early days, leaving many physical and emotional consequences of childbirth untreated, which can be debilitating but are often manageable with timely care [2].
Lack of postpartum care leads to significant adverse outcomes for mothers and infants, including increased risks of long-term physical and mental health problems and higher mortality rates. A 2024 study found that more than one-third of women experience persistent health issues after childbirth, such as dyspareunia (35%), low back pain (32%), anxiety (9–24%), and depression (11–17%), many of which remain underrecognized and untreated without adequate postpartum care [3]. Postpartum depression affects a mother’s physical and mental health, relationships, and daily functioning, and it also has significant consequences for the infant’s growth, health, sleep patterns, and various aspects of development, such as motor skills, cognition, language, emotional regulation, social behavior, and overall well-being. Additionally, it negatively influences mother–infant interactions, including bonding, breastfeeding, and the mother’s ability to fulfill her maternal role [4, 5].
Implementation of effective postpartum care is hindered by numerous obstacles, particularly those stemming directly from the mother’s circumstances. A key issue is that some women may not fully understand the importance of postpartum care or may perceive it as unnecessary, leading to reduced engagement with services. Furthermore, limited family or social support, psychological stress, and broader socioeconomic factors can hinder a woman’s ability to access essential postpartum services [6, 7].
Self-efficacy, social support, and perceived barriers are key psychosocial determinants that influence women’s ability to address and overcome challenges related to postpartum care [8-10]. Self-efficacy can impact various aspects of maternal health during the postpartum period. Mothers higher confidence in their breastfeeding abilities are better equipped to manage breastfeeding related difficulties. This can improve both the quality and duration of breastfeeding [11]. Physical activity self-efficacy refers to an individual’s confidence in their ability to maintain physical activity even when facing challenges. This confidence is a key factor in initiating and maintaining new health promoting behaviors [12]. A study’s findings indicate a significant association between maternal health literacy and physical activity self efficacy. Insufficient knowledge about a particular health issue can negatively impact individuals’ confidence in their ability to follow a self-care plan [13].
Although social support is defined in various ways, research consistently demonstrates a strong correlation between social support and mothers’ mental health during the postpartum period [14]. Postpartum social support is vital for maternal recovery, helping to prevent mental health disorders and reduce stress. Furthermore, it promotes lasting health benefits for both children and their mothers [15].
Perceived barriers can be categorized into intrapersonal, interpersonal, and environmental factors. Conditions, such as postpartum depression and anxiety, significantly impact women’s perceptions of their capabilities and overall health [16]. Concerns about burdening others or straining relationships can inhibit women from seeking assistance when needed [17]. Women often face challenges related to transportation, financial constraints, and availability of appropriate services (e.g. childcare, health care) that can limit their ability to engage in postpartum care [6].
Counseling is a crucial intervention that empowers individuals to improve their quality of life [18]. It facilitates active listening, mutual understanding, responsive communication, and targeted interventions [19]. A continuum of care approach beginning in the third trimester and extending through the postpartum period may provide more comprehensive counseling to address patients’ concerns [20]. Therefore, there is a clear demand for interventions like counseling.
While some studies in Iran have explored interventions, such as clinical guidelines, supportive counseling, and various educational programs during the postpartum period [21, 22], a notable research gap persists regarding group-based counseling interventions for first-time mothers. In particular, few studies have addressed interventions that concurrently address self-efficacy, social support, and perceived barriers. These three constructs are critical. Self-efficacy enhances mothers’ confidence to engage in health-promoting behaviors, social support provides emotional and practical resources that improve mental health and coping, and perceived barriers often hinder the adoption of healthy practices. Addressing all three within a group counseling framework could significantly improve maternal health outcomes, such as breastfeeding success, postpartum depression reduction, and adherence to care. This study aimed to evaluate the effects of a structured counseling intervention on key psychosocial factors among postpartum mothers. Specifically, it examined how counseling influences maternal self-efficacy, perceived social support, and perceived barriers to adopting health-promoting behaviors during the postpartum period.
Methods
Study design and sampling
A randomized controlled trial with a parallel-group design was conducted involving 112 first-time mothers recruited from Hamadan University of Medical Sciences, Iran. No changes were made after trial commencement. A two-stage cluster sampling strategy was employed to ensure a representative sample within Hamadan City. In the first stage, the city was divided into five geographical zones based on official administrative boundaries and population distribution data. These regions served as clusters representing different community profiles. In the second stage, two health centers were randomly selected from each geographical region, resulting in a total of 10 centers out of 20 operating in Hamadan City. To allocate health centers to intervention conditions, a randomization process was conducted at the cluster (health center) level rather than the individual level. This approach minimized the risk of contamination between groups. The 10 selected health centers were randomly assigned to the intervention group (counseling plus standard care) or the control group (standard care only), with five centers per group. Within each selected health center, eligible first-time mothers were contacted and screened for inclusion. Mothers who had undergone cesarean delivery were excluded to maintain sample homogeneity regarding delivery type. If an eligible participant declined or did not meet the inclusion criteria, a replacement was recruited using the same procedures within the same center to maintain cluster integrity and sample size. Randomization of clusters into groups employed a permuted-block design at the cluster level, with block sizes of four to six centers to ensure balanced allocation across regions. The randomization sequence was computer-generated by an independent researcher not involved in recruitment or data collection. Allocation was concealed using sealed opaque envelopes, which were confirmed eligible. Participants in both groups completed standardized questionnaires administered through face-to-face interviews by trained research staff. This approach aimed to reduce missing data and ensure consistency in data collection.
Inclusion and exclusion criteria
The inclusion criteria included literacy in Persian to ensure comprehension of study materials and questionnaires; vaginal childbirth, as the study specifically aimed to evaluate outcomes in this population and avoid potential confounding effects associated with cesarean deliveries, which can differ significantly in maternal recovery and breastfeeding outcomes; delivery of healthy, full-term infants weighing between 2500 and 4000 grams to exclude infants with low or high birth weight that might affect maternal and infant health; absence of physical or psychiatric conditions and obstetric complications during the current pregnancy, to reduce variability due to underlying health factors that could influence study measures; and non-participation in other educational programs to avoid potential contamination of the intervention effects. Mothers and infants hospitalized for more than 48 hours post-delivery were excluded to ensure a more uniform postpartum recovery period, as prolonged hospitalization could impact participation and outcomes. Mothers who missed two or more counseling sessions were excluded to maintain intervention fidelity and protocol adherence; adherence to the counseling sessions was monitored through attendance logs maintained by the facilitators, and participants were contacted promptly upon missed sessions to encourage ongoing engagement. The threshold of two missed sessions was based on prior literature indicating that reduced session attendance can significantly diminish intervention effectiveness [23].
Additionally, mothers who underwent divorce during the study period were excluded due to the potential psychosocial stressors impacting study outcomes. Mothers who were unable to breastfeed, suffered severe infections, or experienced postpartum hemorrhage were excluded because these conditions could directly affect both maternal and infant health and confound the assessment of the counseling program’s effects.
Randomization
Participants were randomly assigned to the intervention or control group according to the cluster level permuted block randomization with a 1:1 allocation ratio. Randomization was performed by a researcher not involved in participant recruitment or intervention delivery to ensure allocation concealment. To maintain confidentiality, each participant received a unique identification code placed inside sealed, and opaque envelopes, which were opened sequentially at enrollment. The control group received standard care, while the intervention group received standard care plus the counseling interventions. Due to the nature of the counseling intervention, participants and facilitators were not blinded to group assignment. However, outcome assessors and the data analyst were blinded to group allocation to minimize assessment and analysis bias. Participants in the experimental group were further divided into 10 small counseling groups, each consisting of 5_10 participants, to facilitate more personalized and effective delivery. Missing data from the questionnaires were anticipated due to potential non-response or incomplete answers. To address this, questionnaires were checked for completeness at the time of collection, and participants were encouraged to complete missing items whenever feasible. Quality control measures included training sessions for intervention facilitators to standardize the delivery of counseling, regular supervision meetings to ensure protocol adherence, and periodic audits of data entries. An independent data monitoring committee periodically reviewed study progress and data quality.
Data collection tool
Four questionnaires were used for data collection. The first questionnaire collected socio-demographic information about the participants, including details, such as the mother’s age, employment status, education level, housing situation, whether the pregnancy was planned, the newborn’s gender, and any history of abortion.
Perceived self-efficacy questionnaire
This tool has been previously validated and shown to be reliable for use in the Iranian context [24]. This questionnaire consists of 8 questions, each rated on a 5-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree.’ For questions 8, 6, 5, 4, 2, and 1, the scoring is from 1 to 5, while questions 3 and 7 are scored in reverse. The total score ranges from 8 to 40, with higher scores indicating a greater ability to manage the outcomes of health-related programs. The questionnaire’s reliability was assessed using Cronbach’s α, yielding a coefficient of 0.81. To ensure validity, the content validity method was employed, involving feedback from 7 nursing and midwifery faculty members and 2 health faculty members, which led to necessary revisions.
Perceived social support questionnaire
This 16-question questionnaire is structured into two parts. The first part includes 10 questions using a 4-point Likert scale, with options ranging from ‘a lot’ to ‘not at all,’ scored from 3 to 0. The second part, questions 11 to 16, uses a binary ‘yes/no’ format, where ‘yes’ is scored as 1 and ‘no’ as 0. Scores range from 0 to 36, with higher scores indicating perceived social support. In our study, the reliability was confirmed at 0.92 using Cronbach’s α. To ensure validity, we also employed content validation, distributing the questionnaire to 7 nursing and midwifery faculty members and 2 health faculty members, which led to necessary revisions.
Perceived barriers questionnaire
This questionnaire comprises 18 items, measured on a 4-point Likert scale with options ranging from ‘never’ to ‘always,’ scored from 1 to 4. It assesses the barriers that hinder respondents from engaging in health-promoting behaviors. The total score can range from 18 to 72, with higher scores indicating more significant obstacles to adopting healthy behaviors. In our study, the questionnaire’s reliability was confirmed with a Cronbach’s α coefficient of 0.81. Additionally, content validity was ensured by distributing the questionnaire to 7 nursing and midwifery faculty members and 2 health faculty members, leading to necessary revisions.
The content and face validity of this instrument were confirmed in Iran by Mohammadian et al. in 2009 at the University of Tehran, Iran, with a Cronbach’s α coefficient of 0.72 [24].
Counseling interventions
The experimental group participated in a structured counseling program conducted in small groups of 5–10 women at the health center, with each session lasting 45–60 minutes. These sessions were scheduled at specific postpartum intervals to address the evolving needs of new mothers. The first session, held 3–5 days postpartum, focused on group education for participants about physiological changes occurring during the postpartum period, identifying postpartum danger signs, sexual health concerns, lactation techniques, and maternal nutrition to support recovery and infant care. The second session took place 10–15 days postpartum and emphasized recognizing stress and its symptoms, teaching effective coping and relaxation methods, and exploring factors influencing interpersonal relationships. The third session was conducted 17–20 days postpartum and addressed the importance of physical activity by discussing suitable postpartum exercises, promoting self-actualization, enhancing spiritual well-being, and highlighting the overall benefits of maintaining good health during this critical period. Following the counseling sessions, weekly follow-up contacts were conducted for an additional three weeks to provide ongoing support, answer questions, and reinforce key messages, and participants were provided with contact information. Participants received a comprehensive booklet compiled from credible scientific sources, summarizing the advice and strategies discussed during the sessions to reinforce learning and provide a reference at home. To evaluate the intervention’s impact, mothers from both the experimental and control groups completed standardized questionnaires during routine postnatal care visits, approximately 42 days postpartum. After study completion, the booklet was offered to the control group to ensure equitable access to informational resources (Table 1).
Sample size
We considered a type I error rate (α) of 5%, a type II error rate (β) of 20%, and an attrition rate of 10%. Based on a previous study [25], the required sample size was calculated to be 60 participants per group [25].
Statistical analysis
Maternal occupation was categorized into two groups: Housewife and employee. This binary classification reflected the characteristics of the study population, in which most participants were either primarily homemakers or formally employed outside the home. This approach allowed us to clearly distinguish between mothers engaged in paid employment and those dedicating most of their time to household and childcare responsibilities. Due to sample size considerations and the need to maintain sufficient group numbers for meaningful statistical analysis, more detailed occupational categories were not used. Mean±SD were used for descriptive statistics. Difference in the mean or frequency of demographic variables between the two groups was examined using the independent t-test and the chi-square. Then, a paired t-test was used to compare the means before and after the intervention. If necessary, analysis of covariance (ANCOVA) was also performed. All statistical tests were performed at a 95% confidence level and using the SPSS software, version 24.
Results
A total of 160 women completed informed consent and were assessed for eligibility, of whom 40 were excluded based on the predefined criteria. The remaining 120 eligible participants were randomly assigned equally to the experimental (n=60) and control (n=60) groups. During follow-up, four women in the experimental group discontinued the intervention for personal reasons. In the control group, two participants were lost to follow-up and two failed to complete the post-intervention questionnaire. Consequently, 56 women from each group completed the study and were included in the final analysis (Figure 1).
The mean ages of mothers in the experimental and control groups were 23.46 and 23.77, respectively. No significant differences were observed in the distribution of any demographic variable between the two groups (P>0.05). Table 1 presents the number and percentage of demographic variables by group.
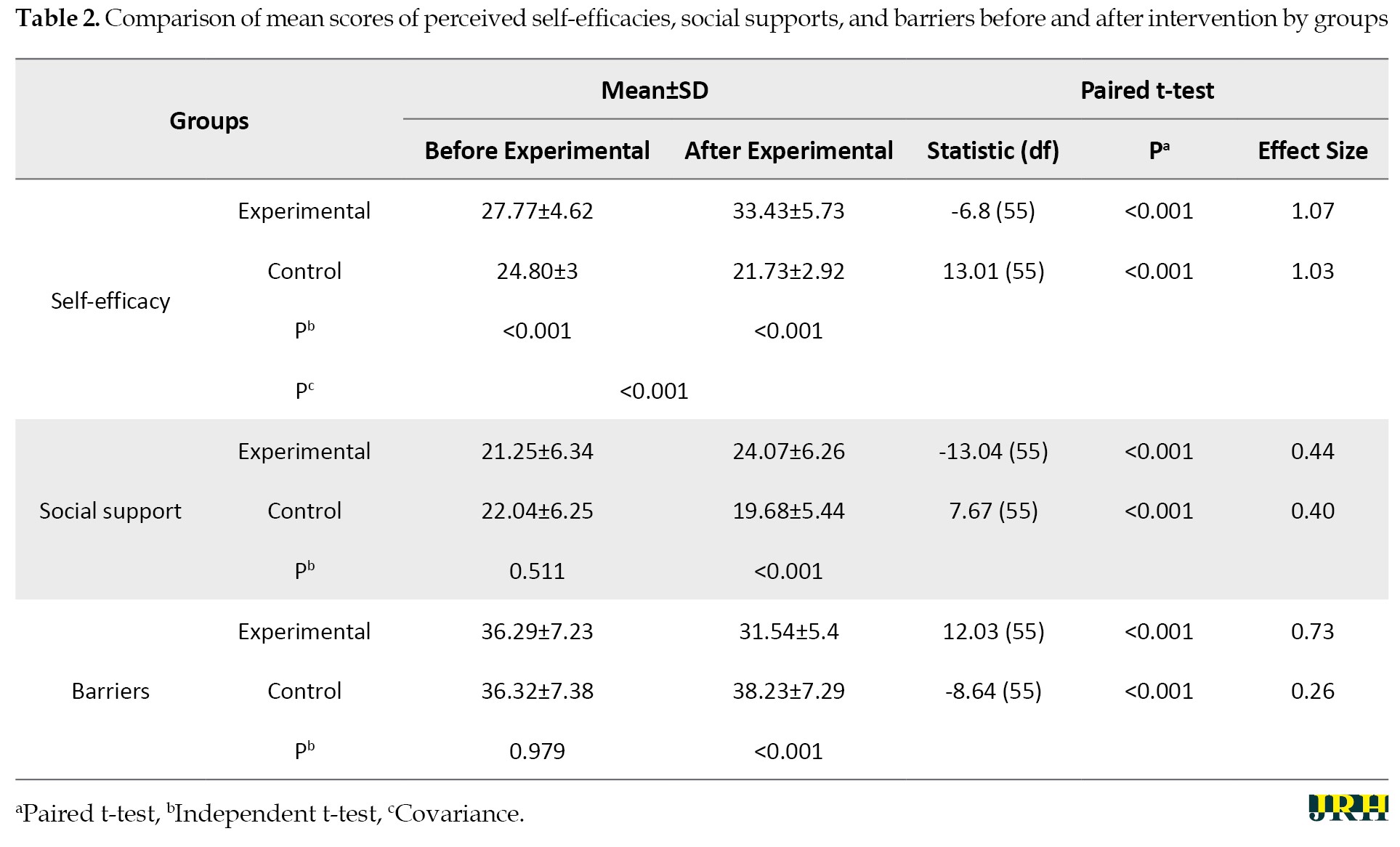
Self-efficacy: The mean self-efficacy score in the experimental group before the intervention was 27.77±4.62, which increased to 33.43±5.73 after the intervention (P<0.001, effect size=1.07). In contrast, in the control group, the mean self-efficacy score before the intervention was 24.80±3.00, which decreased to 21.73±2.92 after the intervention (P<0.001, effect size=1.03).
Social support: The mean perceived social support score in the experimental group before the intervention was 21.25±6.34, which increased to 24.07±6.26 after the intervention (P<0.001, effect size=0.44). In contrast, in the control group, the mean perceived social support score before the intervention was 22.04±6.25, which decreased to 19.68±5.44 after the intervention (P<0.001, effect size=0.40).
Perceived barriers: The mean perceived barriers score in the experimental group before the intervention was 36.29±7.23, which decreased to 31.54±5.4 after the intervention (P<0.001, effect size=0.73). In contrast, in the control group, the mean perceived barriers score before the intervention was 36.32±7.38, which increased to 38.23±7.29 after the intervention (P<0.001, effect size=0.26) (Table 2).
Discussion
The results indicated that the intervention group, which received counseling, experienced a significant improvement in perceived self-efficacy scores compared to the control group. Moreover, following the intervention, the intervention group showed a significant increase in perceived social support scores compared to the control group. Regarding perceived barriers, the intervention group significantly reported lower scores compared to the control group, which indicates that counseling improves the adoption of healthy behaviors.
The present study’s finding that counseling significantly enhanced breastfeeding self-efficacy and maternal functioning reinforces prior research emphasizing counseling’s pivotal role in postpartum care. For example, Fahim et al. demonstrated that three prenatal counseling sessions increased mothers’ self-efficacy compared to controls, supporting the effectiveness of targeted counseling in boosting maternal confidence [26].
Bandura’s self-efficacy theory explains these effects through four main sources: mastery experiences, vicarious learning, verbal persuasion, and emotional regulation. Counseling facilitates skill-building (mastery), provides encouragement (verbal persuasion), normalizes challenges via shared experiences (vicarious learning), and helps manage stress (emotional regulation), collectively strengthening mothers’ belief in their breastfeeding capabilities and improving performance [27]. Similarly, Farasati et al. showed that home-based supportive counseling for first-time mothers after cesarean delivery fostered maternal functioning and self-efficacy over time [28].
While our results confirm and build upon this body of evidence, it is notable that some studies have reported mixed outcomes regarding the effectiveness of counseling interventions. For example, a systematic review observed limited effects on breastfeeding self-efficacy when counseling was brief or not specifically tailored to individual needs, suggesting that intervention intensity and personalization may be critical moderators of efficacy [29]. Moreover, differences in cultural and healthcare systems might influence how counseling impacts mothers’ perceptions and behaviors [30]. Our study contributes to this discourse by demonstrating that repeated and comprehensive counseling sessions administered prenatally and postpartum can produce meaningful improvements, thereby highlighting the importance of timing and sustained support in postpartum care models.
Our study revealed a significant increase in perceived social support among first-time mothers in the test group compared to the control group following counseling. This outcome aligns with findings by Leahy-Warren et al., who identified strong links between functional and informal social support, maternal self-efficacy, and reduced postnatal depression in first-time mothers six weeks postpartum. Counseling appears to enhance perceived support by equipping mothers with the resources they need during the transition to parenthood [31]. Additionally, research by Machado et al. indicates that women often prefer informal support from peers or family over professional assistance, suggesting that counseling can fill this gap by offering individualized support and offering personalized guidance [16]. Another study highlighted that insufficient or inappropriate professional support during the postpartum period often leaves mothers feeling isolated. Counseling programs that focus on individual needs can address these shortcomings, improving perceived social support [32]. The ‘healthy moms and babies’ program emphasized preventive interventions to minimize perceived barriers during pregnancy [33].
Our study showed that first-time mothers in the intervention group reported lower perceived barrier scores, indicating that counseling effectively enabled them to overcome challenges and adopt healthier habits. This outcome is supported by a study by Dafei et al. which found that similar interventions reduced stress, anxiety, and postpartum depression while promoting healthier behaviors. These results suggest that addressing psychological barriers through tailored interventions leads to improved health outcomes [34]. First-time mothers commonly face uncertainty regarding infant care, exclusive breastfeeding, and balancing personal well-being with caregiving demands, often compounded by emotional vulnerability. Professional counseling addresses these challenges by delivering tailored information, normalizing common experiences, and enhancing mothers’ emotional resilience. This multidimensional support helps reduce cognitive and emotional barriers, giving mothers a stronger sense of control and confidence, which fosters healthier parenting practices [35].
This study has several limitations that warrant careful consideration when interpreting the findings and their applicability. First, the intervention was delivered over a relatively short postpartum period and was not maintained over the long-term. Given that behavior change, especially in breastfeeding and maternal self-efficacy, typically requires ongoing reinforcement and support, the limited duration may have attenuated the intervention’s full potential impact. This temporal constraint likely influenced the magnitude and sustainability of observed improvements in self-efficacy, perceived barriers, and social support. Without extended follow-up, it remains uncertain whether the positive effects endure beyond the immediate postpartum window. Future studies employing longer intervention periods and follow-up assessments are necessary to confirm the durability of these outcomes.
Second, the exclusively urban study population raises concerns about the generalizability of the findings. Urban mothers may experience different social dynamics, access to healthcare services, educational resources, and cultural norms compared to their rural counterparts, all of which can shape perceived barriers and social support networks. For example, urban settings might offer more breastfeeding-friendly environments and greater access to professional counseling, potentially amplifying intervention effectiveness. Conversely, rural mothers often face unique challenges, such as limited healthcare access and stronger traditional beliefs, which might modify both baseline outcomes and response to counseling. Thus, the urban-centric sample limits the extent to which these findings can be extrapolated to broader, more diverse postpartum populations across different geographic and socioeconomic contexts.
Third, although the questionnaires used to assess outcomes were previously validated in the general Iranian population, they have not been specifically validated for postpartum mothers. This may affect the sensitivity of the tools to detect postpartum-specific psychological and behavioral nuances. Such limitations in measurement validity could lead to under- or over-estimation of constructs, such as perceived social support and barriers. Consequently, caution is necessary when interpreting the precision of these results. Future research should prioritize the adaptation and rigorous validation of assessment instruments tailored to postpartum populations to ensure capture of nuanced maternal experiences and improve measurement accuracy.
Conclusion
This study shows that postpartum counseling significantly improves first-time mothers’ breastfeeding self-efficacy and social support while reducing perceived barriers to healthy behaviors. By addressing the unique psychological and informational challenges of early motherhood, the intervention enhanced maternal confidence and support networks, which are key factors for lasting behavior change. While the findings highlight counseling’s benefits in urban first-time mothers, further research should assess its effectiveness in rural settings and among multiparous women to broaden generalizability. To apply these results, policymakers should integrate structured, theory-based counseling into maternal health programs by training midwives and community health workers to provide tailored support during antenatal and postpartum care. Sustained follow-up resources will be crucial to maintain these positive outcomes.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Hamadan University of Medical Sciences, Hamadan, Iran (Code: IR.UMSHA.REC.1394.343). This study was registered by the Iranian Registry of Clinical Trials, Tehran, Iran (Code: IRCT2016030510426N10). Written informed consent was obtained from each participant before the study was conducted.
Funding
This research did not receive any grant from public, commercial, or non-profit funding agencies.
Authors' contributions
Conceptualization, study design, data analysis and interpretation: Nazli Alafchi and Mostafa Eghbalian; Statistical analysis: Mostafa Eghbalian; Writing, project administration, technical, and material support: All authors; Supervision: Nazli Alafchi.
Conflict of interest
This study declared no conflict of interest.
Acknowledgments
The authors express their gratitude to all the women who participated in the study.
Self-efficacy: The mean self-efficacy score in the experimental group before the intervention was 27.77±4.62, which increased to 33.43±5.73 after the intervention (P<0.001, effect size=1.07). In contrast, in the control group, the mean self-efficacy score before the intervention was 24.80±3.00, which decreased to 21.73±2.92 after the intervention (P<0.001, effect size=1.03).
Social support: The mean perceived social support score in the experimental group before the intervention was 21.25±6.34, which increased to 24.07±6.26 after the intervention (P<0.001, effect size=0.44). In contrast, in the control group, the mean perceived social support score before the intervention was 22.04±6.25, which decreased to 19.68±5.44 after the intervention (P<0.001, effect size=0.40).
Perceived barriers: The mean perceived barriers score in the experimental group before the intervention was 36.29±7.23, which decreased to 31.54±5.4 after the intervention (P<0.001, effect size=0.73). In contrast, in the control group, the mean perceived barriers score before the intervention was 36.32±7.38, which increased to 38.23±7.29 after the intervention (P<0.001, effect size=0.26) (Table 2).
Discussion
The results indicated that the intervention group, which received counseling, experienced a significant improvement in perceived self-efficacy scores compared to the control group. Moreover, following the intervention, the intervention group showed a significant increase in perceived social support scores compared to the control group. Regarding perceived barriers, the intervention group significantly reported lower scores compared to the control group, which indicates that counseling improves the adoption of healthy behaviors.
The present study’s finding that counseling significantly enhanced breastfeeding self-efficacy and maternal functioning reinforces prior research emphasizing counseling’s pivotal role in postpartum care. For example, Fahim et al. demonstrated that three prenatal counseling sessions increased mothers’ self-efficacy compared to controls, supporting the effectiveness of targeted counseling in boosting maternal confidence [26].
Bandura’s self-efficacy theory explains these effects through four main sources: mastery experiences, vicarious learning, verbal persuasion, and emotional regulation. Counseling facilitates skill-building (mastery), provides encouragement (verbal persuasion), normalizes challenges via shared experiences (vicarious learning), and helps manage stress (emotional regulation), collectively strengthening mothers’ belief in their breastfeeding capabilities and improving performance [27]. Similarly, Farasati et al. showed that home-based supportive counseling for first-time mothers after cesarean delivery fostered maternal functioning and self-efficacy over time [28].
While our results confirm and build upon this body of evidence, it is notable that some studies have reported mixed outcomes regarding the effectiveness of counseling interventions. For example, a systematic review observed limited effects on breastfeeding self-efficacy when counseling was brief or not specifically tailored to individual needs, suggesting that intervention intensity and personalization may be critical moderators of efficacy [29]. Moreover, differences in cultural and healthcare systems might influence how counseling impacts mothers’ perceptions and behaviors [30]. Our study contributes to this discourse by demonstrating that repeated and comprehensive counseling sessions administered prenatally and postpartum can produce meaningful improvements, thereby highlighting the importance of timing and sustained support in postpartum care models.
Our study revealed a significant increase in perceived social support among first-time mothers in the test group compared to the control group following counseling. This outcome aligns with findings by Leahy-Warren et al., who identified strong links between functional and informal social support, maternal self-efficacy, and reduced postnatal depression in first-time mothers six weeks postpartum. Counseling appears to enhance perceived support by equipping mothers with the resources they need during the transition to parenthood [31]. Additionally, research by Machado et al. indicates that women often prefer informal support from peers or family over professional assistance, suggesting that counseling can fill this gap by offering individualized support and offering personalized guidance [16]. Another study highlighted that insufficient or inappropriate professional support during the postpartum period often leaves mothers feeling isolated. Counseling programs that focus on individual needs can address these shortcomings, improving perceived social support [32]. The ‘healthy moms and babies’ program emphasized preventive interventions to minimize perceived barriers during pregnancy [33].
Our study showed that first-time mothers in the intervention group reported lower perceived barrier scores, indicating that counseling effectively enabled them to overcome challenges and adopt healthier habits. This outcome is supported by a study by Dafei et al. which found that similar interventions reduced stress, anxiety, and postpartum depression while promoting healthier behaviors. These results suggest that addressing psychological barriers through tailored interventions leads to improved health outcomes [34]. First-time mothers commonly face uncertainty regarding infant care, exclusive breastfeeding, and balancing personal well-being with caregiving demands, often compounded by emotional vulnerability. Professional counseling addresses these challenges by delivering tailored information, normalizing common experiences, and enhancing mothers’ emotional resilience. This multidimensional support helps reduce cognitive and emotional barriers, giving mothers a stronger sense of control and confidence, which fosters healthier parenting practices [35].
This study has several limitations that warrant careful consideration when interpreting the findings and their applicability. First, the intervention was delivered over a relatively short postpartum period and was not maintained over the long-term. Given that behavior change, especially in breastfeeding and maternal self-efficacy, typically requires ongoing reinforcement and support, the limited duration may have attenuated the intervention’s full potential impact. This temporal constraint likely influenced the magnitude and sustainability of observed improvements in self-efficacy, perceived barriers, and social support. Without extended follow-up, it remains uncertain whether the positive effects endure beyond the immediate postpartum window. Future studies employing longer intervention periods and follow-up assessments are necessary to confirm the durability of these outcomes.
Second, the exclusively urban study population raises concerns about the generalizability of the findings. Urban mothers may experience different social dynamics, access to healthcare services, educational resources, and cultural norms compared to their rural counterparts, all of which can shape perceived barriers and social support networks. For example, urban settings might offer more breastfeeding-friendly environments and greater access to professional counseling, potentially amplifying intervention effectiveness. Conversely, rural mothers often face unique challenges, such as limited healthcare access and stronger traditional beliefs, which might modify both baseline outcomes and response to counseling. Thus, the urban-centric sample limits the extent to which these findings can be extrapolated to broader, more diverse postpartum populations across different geographic and socioeconomic contexts.
Third, although the questionnaires used to assess outcomes were previously validated in the general Iranian population, they have not been specifically validated for postpartum mothers. This may affect the sensitivity of the tools to detect postpartum-specific psychological and behavioral nuances. Such limitations in measurement validity could lead to under- or over-estimation of constructs, such as perceived social support and barriers. Consequently, caution is necessary when interpreting the precision of these results. Future research should prioritize the adaptation and rigorous validation of assessment instruments tailored to postpartum populations to ensure capture of nuanced maternal experiences and improve measurement accuracy.
Conclusion
This study shows that postpartum counseling significantly improves first-time mothers’ breastfeeding self-efficacy and social support while reducing perceived barriers to healthy behaviors. By addressing the unique psychological and informational challenges of early motherhood, the intervention enhanced maternal confidence and support networks, which are key factors for lasting behavior change. While the findings highlight counseling’s benefits in urban first-time mothers, further research should assess its effectiveness in rural settings and among multiparous women to broaden generalizability. To apply these results, policymakers should integrate structured, theory-based counseling into maternal health programs by training midwives and community health workers to provide tailored support during antenatal and postpartum care. Sustained follow-up resources will be crucial to maintain these positive outcomes.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Hamadan University of Medical Sciences, Hamadan, Iran (Code: IR.UMSHA.REC.1394.343). This study was registered by the Iranian Registry of Clinical Trials, Tehran, Iran (Code: IRCT2016030510426N10). Written informed consent was obtained from each participant before the study was conducted.
Funding
This research did not receive any grant from public, commercial, or non-profit funding agencies.
Authors' contributions
Conceptualization, study design, data analysis and interpretation: Nazli Alafchi and Mostafa Eghbalian; Statistical analysis: Mostafa Eghbalian; Writing, project administration, technical, and material support: All authors; Supervision: Nazli Alafchi.
Conflict of interest
This study declared no conflict of interest.
Acknowledgments
The authors express their gratitude to all the women who participated in the study.
References
- Dol J, Hughes B, Bonet M, Dorey R, Dorling J, Grant A, et al. Timing of maternal mortality and severe morbidity during the postpartum period: A systematic review. JBI Evidence Synthesis. 2022; 20(9):2119-94. [DOI:10.11124/jbies-20-00578] [PMID]
- WHO. Urges quality care for women and newborns in critical first weeks after childbirth. Geneva: World health organization; 2022. [Link]
- Vogel JP, Jung J, Lavin T, Simpson G, Kluwgant D, Abalos E, et al. Neglected medium-term and long-term consequences of labour and childbirth: A systematic analysis of the burden, recommended practices, and a way forward. The Lancet. Global Health. 2024; 12(2):e317-30. [DOI:10.1016/s2214-109x(23)00454-0] [PMID]
- Pelayo I. Exploring the impact that social media has on the lived experiences of mothers who have gone through postpartum depression [MAthesis]. California: California State University; 2025. [Link]
- Slomian J, Honvo G, Emonts P, Reginster JY, Bruyère O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Women's Health (London, England). 2019; 15:1745506519844044. [DOI:10.1177/1745506519844044] [PMID]
- Ruderman RS, Dahl EC, Williams BR, Davis K, Feinglass JM, Grobman WA, Kominiarek MA, Yee LM. Provider perspectives on barriers and facilitators to postpartum care for low-income individuals. women's health reports (New Rochelle). 2021; 2(1):254-62. [DOI:10.1089/whr.2021.0009] [PMID]
- Pettus PG, Gavlinski LW, Beermann S, Chapple AG, Scheib SA, Quebedeaux TM, et al. Implementation of and barriers to optimizing postpartum care by resident and attending physicians. Ochsner Journal. 2023; 23(3):180-7. [DOI:10.31486/toj.22.0119] [PMID]
- Brani P, Mrvoljak-Theodoropoulou I, Pechlivani F, Gourounti K, Iliadou M, et al. Mothers' breastfeeding self-efficacy after a high-risk or normal pregnancy: A Greek longitudinal cohort study. European Journal of Investigation in Health, Psychology and Education. 2024; 14(6):1803-20. [DOI:10.3390/ejihpe14060119] [PMID]
- Eslahi Z, Bahrami N, Allen KA, Alimoradi Z. Spouse's social support in the postpartum period, predictors and its relationship with postpartum depression in a sample of Iranian primiparous women. International Journal of Gynaecology and Obstetrics. 2021; 154(1):24-30. [DOI:10.1002/ijgo.13488] [PMID]
- Hajimiri K, Shakibazadeh E, Haeri Mehrizi AA, Shab-Bidar S, Sadeghi R. The role of perceived barrier in the postpartum women's health promoting lifestyle: A partial mediator between self-efficacy and health promoting lifestyle. Journal of Education and Health Promotion. 2018; 7:38. [DOI:10.4103/jehp.jehp_70_17] [PMID]
- Ouyang YQ, Guo J, Zhou J, Zhouchen Y, Huang C, Huang Y, et al. Theoretical approaches in the development of interventions to promote breastfeeding: A scoping review. Midwifery. 2024; 132:103988. [DOI:10.1016/j.midw.2024.103988] [PMID]
- Shang X, Ye L, Gu X, Zhou A, Xu Y, Zhang Y, et al. Attitudes and barriers to physical activity and exercise self-efficacy among Chinese pregnant women: A cross-sectional study. Journal of Multidisciplinary Healthcare. 2023; 16:3561-73. [DOI:10.2147/jmdh.s441210] [PMID]
- Masoumy M, Hamedi-Shahraki S, Zeraatpishe F. The relationship between maternal health literacy with physical activity self-efficacy in postpartum women. Journal of Multidisciplinary Care. 2024; 12(4):203-8. [Link]
- Lee MS, Lee JJ, Park S, Kim S, Lee H. Is social support associated with postpartum depression, anxiety and perceived stress among Korean women within the first year postpartum? Journal of Psychosomatic Obstetrics and Gynaecology. 2023; 44(1):2231629. [DOI:10.1080/0167482x.2023.2231629] [PMID]
- Asselmann E, Kunas SL, Wittchen HU, Martini J. Maternal personality, social support, and changes in depressive, anxiety, and stress symptoms during pregnancy and after delivery: A prospective-longitudinal study. PLoS One. 2020; 15(8):e0237609. [DOI:10.1371/journal.pone.0237609] [PMID]
- De Sousa Machado T, Chur-Hansen A, Due C. First-time mothers' perceptions of social support: Recommendations for best practice. Health Psychology Open. 2020; 7(1):2055102919898611. [DOI:10.1177/2055102919898611] [PMID]
- Negron R, Martin A, Almog M, Balbierz A, Howell EA. Social support during the postpartum period: Mothers' views on needs, expectations, and mobilization of support. Maternal and Child Health Journal. 2013; 17(4):616-23. [DOI:10.1007/s10995-012-1037-4] [PMID]
- Karimlou V, Charandabi SM, Malakouti J, Mirghafourvand M. Effect of counselling on health-promoting lifestyle and the quality of life in Iranian middle-aged women: A randomised controlled clinical trial. BMC Health Services Research. 2019; 19(1):350. [DOI:10.1186/s12913-019-4176-0] [PMID]
- Chamgurdani FK, Barkin JL, Esmaeilpour K, Malakouti J, Buoli M, Mirghafourvand M. The effect of counseling with a skills training approach on maternal functioning: A randomized controlled clinical trial. BMC Womens Health. 2020; 20(1):51. [DOI:10.1186/s12905-020-00914-w] [PMID]
- Prince A, Wade J, Power ML, Gunawansa N, Cruz-Bendezú A, Schulkin J, et al. Postpartum care: discussions and counseling for the peripartum period. Journal of Neonatal-Perinatal Medicine. 2023; 16(4):657-64. [DOI:10.3233/npm-230167] [PMID]
- Seiiedi-Biarag L, Mirghafourvand M, Esmaeilpour K, Hasanpour S. A randomized controlled clinical trial of the effect of supportive counseling on mental health in Iranian mothers of premature infants. BMC Pregnancy and Childbirth. 2021; 21(1):6. [DOI:10.1186/s12884-020-03502-w] [PMID]
- Najmi LA, Mohammad-Alizadeh-Charandabi S, Jahanfar S, Abbasalizadeh F, Poormehr HS, Mirghafourvand M. Effect of postpartum clinical guideline on maternal outcomes in Iranian women: A randomized controlled clinical trial. BMC Pregnancy Childbirth. 2024; 24(1):886. [DOI:10.1186/s12884-024-07109-3] [PMID]
- Dev S, Griffith J, Ncube C, Patel V, Lincoln A. Impact of treatment attendance on mental health outcomes within task-shared psychological treatments: A causal analysis from the PRIME India study. Global Mental Health. 2025; 12:e42. [DOI:10.1017/gmh.2025.36] [PMID]
- Mohamadian H, Eftekhar Ardebili H, Rahimi Foroushani A, Taghdisi M, Shojaiezade D. Evaluation of Pender’s health promotion model for predicting adolescent girls’ quality of life. Journal of School of Public Health & Institute of Public Health Research. 2011; 8(4):1-13. [Link]
- Ghodsbin F, Yazdani K, Jahanbin I, Keshavarzi S. The effect of education on health-promoting behaviors at the first six weeks post-delivery on the quality of life of primiparous women. Armaghane Danesh. 2012; 17(4):279-88. [Link]
- Fahim SH, Kazemi F, Masoumi SZ, Refaei M. The effect of midwife-oriented breastfeeding counseling on self-efficacy and performance of adolescent mothers: A clinical trial study. BMC Pregnancy and Childbirth. 2023; 23(1):672. [DOI:10.1186/s12884-023-05982-y] [PMID]
- Ghasemi V, Simbar M, Banaei M, Saei Ghare Naz M, Jahani Z, Nazem H. The effect of interventions on breastfeeding self-efficacy by using Bandura’s theory in Iranian mothers: A systematic review. Journal of Pediatric Perspectives. 2019; 7(8):9939-54. [Link]
- Farasati M, Nourizadeh R, Sattarzadeh-Jahdi N, Esmaeilpour K, Mehrabi E, Reisy L. The effect of in-home supportive counseling on maternal functioning and self-efficacy following cesarean section among primiparous women. Journal of Education and Health Promotion. 2024; 13(1):26. [PMID]
- McFadden A, Siebelt L, Marshall JL, Gavine A, Girard LC, Symon A, MacGillivray S. Counselling interventions to enable women to initiate and continue breastfeeding: A systematic review and meta-analysis. International Breastfeeding Journal. 2019; 14(1):42. [DOI:10.1186/s13006-019-0235-8] [PMID]
- Bazrriz S, Yazdanpanah A, Khani Jeihooni A. [Effective factors in empowering mothers for breastfeeding: A qualitative study (Persian)]. Sadra Medical Journal. 2021; 9(1):43-56. [Link]
- Mannocci A, Ciavardini S, Mattioli F, Massimi A, D'Egidio V, Lia L, et al. HAPPY MAMA Project (Part 2)-maternal distress and self-efficacy: A pilot randomized controlled field trial. International Journal of Environmental Research and Public Health. 2022; 19(3):1461. [DOI:10.3390/ijerph19031461] [PMID]
- Schobinger E, Vanetti M, Ramelet AS, Horsch A. Social support needs of first-time parents in the early-postpartum period: A qualitative study. Frontiers in Psychiatry. 2022; 13:1043990. [DOI:10.3389/fpsyt.2022.1043990] [PMID]
- Ruiz-Segovia N, Rodriguez-Muñoz MF, Olivares ME, Izquierdo N, Coronado P, Le HN. Healthy moms and babies preventive psychological intervention application: A study protocol. International Journal of Environmental Research and Public Health. 2021; 18(23):12485. [DOI:10.3390/ijerph182312485] [PMID]
- Dafei M, Mojahed S, Dastjerdi G, Dehghani A, Ardakani TS. The effect of cognitive–behavioral counseling of pregnant women with the presence of a spouse on stress, anxiety, and postpartum depression. Journal of Education and Health Promotion. 2021; 10(1):131. [DOI:10.4103/jehp.jehp_926_20] [PMID]
- McLeish J, Harvey M, Redshaw M, Alderdice F. A qualitative study of first time mothers’ experiences of postnatal social support from health professionals in England. Women and Birth. 2021; 34(5):e451-e60. [DOI:10.1016/j.wombi.2020.10.012] [PMID]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2025/05/3 | Accepted: 2025/08/17 | Published: 2026/03/14
Received: 2025/05/3 | Accepted: 2025/08/17 | Published: 2026/03/14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
