

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 171-180 |
Back to browse issues page


Ethics code: IR.IAU.NEYSHABUR.REC.1403.031
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khodabakhsh M R. Beyond Stress: Critical Role of Mental Health Literacy in Women's Vulnerability to Generalized Anxiety. J Research Health 2026; 16 (2) :171-180
URL: http://jrh.gmu.ac.ir/article-1-2801-en.html
URL: http://jrh.gmu.ac.ir/article-1-2801-en.html



Department of Psychology, Ne. C., Islamic Azad University, Neyshabur, Iran. , khodabakhsh@ut.ac.ir
Full-Text [PDF 632 kb]
(161 Downloads)
| Abstract (HTML) (603 Views)
Full-Text: (103 Views)
Introduction
Mental health, as a fundamental pillar of human well-being, plays a vital role in individual quality of life, social functioning, and the sustainable development of societies. Mental disorders, particularly anxiety disorders, impose a significant burden on health systems, economies, and human relationships, and are recognized as one of the main public health challenges globally. Among the wide spectrum of anxiety disorders, GAD holds a special position due to its chronic nature, the pervasiveness of worries, and its profound impact on various aspects of life [1]. In 2020, before COVID-19, the estimated global incidence of AD reached 298 million people, and after the pandemic, the incidence increased by 25.6% to an estimated global prevalence of 374 million people. This increase was also greater for women (27.9%; 51.8 million people) than for men (21.7%; 24.4 million people). The considerable prevalence of GAD in the general population, with recent estimates emphasizing the need for active screening for undiagnosed cases [2], its higher prevalence in women [1] and its association with reduced occupational, academic, and social functioning, as well as increased use of health services, highlight the necessity for a deeper understanding of its related risk and protective factors [3, 4].
GAD, extending beyond typical daily worries, is a debilitating clinical condition defined by excessive and uncontrollable anxiety and apprehension about various topics, even in the absence of a real threat or out of proportion to the importance of the situation [1, 5]. Understanding the etiology of GAD requires an integrated and multifactorial approach that considers the complex interaction between biological vulnerabilities, psychological factors (such as intolerance of uncertainty, positive beliefs about worry, and cognitive avoidance), and environmental and social influences [4, 6]. One of the crucial risk factors for the onset, exacerbation, and persistence of anxiety and mood disorders is the experience of stressful life events [7, 8]. These events can contribute to the development of mental disorders by disrupting the individual’s psychophysiological balance and straining coping resources. These events range from severe and traumatic events (such as bereavement, abuse, natural disasters) to chronic stressors (such as financial problems or marital conflicts) [8, 9]. Epidemiological and clinical studies, including longitudinal studies, have consistently shown that exposure to stressful life events, particularly adverse childhood experiences and the accumulation of stressors throughout life, significantly increases the risk of developing anxiety disorders (including GAD), depression, and even psychosis, and is associated with adverse physical and mental health outcomes in adulthood [7, 10, 11]. These events appear to occur through various pathways, including psychological pathways (such as creating or activating negative cognitive schemas, reinforcing attentional biases towards threat, reducing feelings of control and self-efficacy, weakening coping strategies), leading to increased vulnerability to mental disorders [12, 13].
In the context of GAD, stressful life events can act as triggers that initiate or exacerbate periods of intense and pervasive worry in susceptible individuals [6]. These events, particularly those that are unexpected, uncontrollable, and threatening to an individual’s crucial goals or values, may challenge fundamental beliefs about the safety, controllability, and predictability of the world, leading to the activation of negative cognitive schemas related to threat, danger, and inability to cope, which are prominent features of GAD [4]. Furthermore, chronic stress resulting from stressful life events can deplete an individual’s cognitive and emotional resources, reducing their capacity for emotion regulation and the use of adaptive coping strategies, which in turn can contribute to the persistence of the worry and anxiety cycle [7, 13]. Therefore, understanding how individuals react to stressful events and, more importantly, what factors might moderate these reactions (i.e. change the strength or direction of the relationship between stress and outcome) is crucial for a better understanding of the etiology and course of GAD and for designing effective preventive and therapeutic interventions.
The present study specifically focuses on the population of married women. Epidemiological studies have consistently reported a higher prevalence of anxiety disorders, including GAD, in women compared to men (approximately twice as high) [1, 5]. Married women may also face a unique or exacerbated combination of stressors resulting from multiple and sometimes conflicting responsibilities in family, work, and social domains. The pressures of managing household chores, caring for children (especially if there is a child with special needs [14]), maintaining the quality of marital relationships, employment (and work-life balance), family financial issues, caring for aging parents, and cultural pressures related to expectations of the roles of wife and motherhood can all act as crucial sources of acute and chronic stressful life events [15], adding to the importance of examining factors affecting mental health in this specific context. Therefore, understanding how married women cope with the multiple stresses of their lives and what individual or social resources might enhance their resilience against the development or exacerbation of GAD is of high importance and can contribute to the design of gender-sensitive and culturally-contextualized interventions.
Meanwhile, identifying protective factors that can reduce the negative effects of stress on mental health has become increasingly crucial. One such potential protective factor is the concept of “mental health literacy,” defined as “knowledge and beliefs about mental disorders that help diagnose, manage, or prevent them” [16, 17]. This concept is multifaceted and includes various components, such as the ability to recognize the onset or presence of specific mental disorders (e.g. recognizing symptoms of anxiety or depression), knowledge and beliefs about the causes, risk factors, and prognosis of mental disorders, awareness of various professional help-seeking options (e.g. psychotherapy, pharmacotherapy) and available self-help resources, knowledge and skills necessary to provide psychological first aid to others, and attitudes that facilitate the recognition and seeking of appropriate help and reduce the social stigma associated with mental illness [18, 19]. Research increasingly shows that higher levels of mental health literacy are associated with a wide range of positive mental health outcomes, including more positive attitudes towards individuals with mental illness and mental health treatments, reduced personal and social stigma, increased intention and effective help-seeking behavior, improved adherence to treatment, and higher levels of psychological and social well-being in various populations (such as students, teachers, employees, outpatients, general population) [20-23].
Considering the various components of mental health literacy, it can be argued that mental health literacy has the potential to act as a protective shield or moderating factor against the harmful effects of stressful life events on the development or exacerbation of GAD. Firstly, individuals with higher mental health literacy are likely better able to recognize early signs of psychological distress resulting from stress (such as excessive worry, restlessness, sleep disturbance) in themselves or others and identify it as a potential mental health problem, rather than attributing it merely to personal weakness or transient conditions [19, 24]. This early recognition can lead to timely seeking of professional help or the use of evidence-based self-help strategies before symptoms become chronic and reach the level of a full-blown clinical disorder [21]. Knowledge about the causes and risk factors of mental disorders, which is part of mental health literacy, may help individuals better understand the role of life stressors in their mental state and avoid unhelpful rumination or self-blame [25]. Awareness of effective treatment options and more positive attitudes towards treatment (associated with higher mental health literacy) can increase an individual’s motivation and adherence to pursuing treatment and actively using healthy coping strategies (such as problem-solving, cognitive restructuring, relaxation exercises) [26]. Mental health literacy can, by reducing the stigma associated with mental health problems, encourage individuals to share their stressful experiences and resulting emotions with their support network (spouse, family, friends) and benefit from social support, which is itself a very important protective factor against stress [14, 27]. Consequently, mental health literacy not only aids in recognition and treatment but also potentially strengthens an individual’s coping processes and adaptation to life’s adversities and stresses, contributing to the maintenance or improvement of overall well-being [28, 29].
Given the strong theoretical and empirical link between stressful life events and GAD on one hand, and the protective and empowering potential of mental health literacy on the other, the central question of this research is whether mental health literacy can moderate the negative and detrimental impact of stressful life events on the severity of GAD symptoms.
Despite the potential theoretical and clinical importance of this topic, a distinct research gap exists in the detailed examination of the moderating role of mental health literacy in the relationship between stressful life events and GAD, particularly within the specific population of married Iranian women. Most previous studies in the field of mental health literacy have either focused on bivariate relationships between these variables (such as examining the association of stressful life events with GAD or the relationship of mental health literacy with help-seeking, stigma, or general well-being) or have investigated the role of mental health literacy as a direct predictor of mental health outcomes or as a mediator in other pathways [23, 30, 31]. Studies specifically examining the moderating role of mental health literacy in the relationship between stress and mental health outcomes are relatively limited and have often been conducted in student populations [32], the general population during crises, such as the COVID-19 pandemic [33], or specific occupational groups [20] and have less frequently focused specifically on married women and their unique challenges and resources within a specific cultural context like Iran. The present study, by focusing on married women in Iran and examining the moderating role of mental health literacy (using appropriate tools) in an integrated model that considers both environmental risk factors (stressful life events) and cognitive-social protective factors (mental health literacy) in relation to a common and debilitating disorder (GAD), seeks to fill this important research gap. Therefore, this study seeks to answer the main question: Does the level of mental health literacy moderate the relationship between stressful life events and GAD in married women?
The findings of this research can have significant theoretical and practical implications in the fields of clinical psychology, health psychology, and public health. From a theoretical perspective, this study contributes to a better understanding of the complex interplay between environmental stressors, individual protective resources, and psychopathology, providing further empirical evidence for vulnerability-stress models as well as models based on resilience and protective factors. From a practical and clinical perspective, the results of this research can provide useful guidance for the design and implementation of targeted preventive and therapeutic interventions. These programs could focus on increasing practical knowledge about anxiety, its causes, and effective management strategies, normalizing experiences related to stress and anxiety, reducing the stigma of mental illness and help-seeking, strengthening effective help-seeking skills (for oneself and others), and promoting adaptive coping strategies [17, 18].
Methods
Procedure
This descriptive-correlational research employed a cross-sectional design. The inclusion criteria included married women residing in Neyshabur City, Iran, and voluntary participation. Incomplete completion of the questionnaire was an exclusion criterion.
Sample and sampling method
The sample of the present study was 226 married women living in Neyshabur City. Considering the purpose of the study and the time and place constraints, the sampling method was used. In this way, the sample was selected from among the individuals who were available to the researcher at the time of the study and who met the inclusion criteria for the study. This method was chosen due to the time constraints and the implementation facilities of the study. It should be noted that in selecting individuals, an attempt was made to observe relative diversity in terms of age, gender, and social conditions, to reduce the incidence of bias in the results. In this regard, the inclusion and exclusion criteria were carefully determined and implemented.
Given the aim of the study, which is to investigate the mediating role of mental health literacy in the relationship between stressful life events and generalized anxiety in married women in Neyshabur City, a sample size of 226 people was determined based on Cohen’s formula for the regression test. Based on previous studies and methodological standards, considering the medium effect size (f²=0.15), the statistical power level of 0.80, and the significance level (α) of 0.05, a sample size of 226 people is appropriate.
The inclusion criteria included being a woman and having an official marriage (legal or religious) at the time of the study, age between 18 and 55 years, residing in Neyshabur City, having at least one year of cohabitation, ability to read and write in Persian, and willingness and informed consent to participate in the study. The exclusion criteria also included no severe psychiatric diagnosis or history of psychiatric illness in the past year, experience of divorce or remarriage or severe emotional separation in the past six months, chronic debilitating physical illnesses such as cancer or kidney failure, pregnancy or childbirth in the past six months, and incomplete or distorted completion of the questionnaires.
Data were collected using the completion of three mental health literacy questionnaires, the generalized anxiety scale, and the life events scale (LES) in person.
For this purpose, after obtaining the necessary ethical permission from the university research committee, the researcher visited centers and environments related to the target community (such as health centers, health homes, cultural centers, etc.) with prior coordination. In these centers, while introducing the purpose and importance of the research, eligible participants were selected voluntarily. To comply with ethical principles, before completing the questionnaire, comprehensive explanations were given on how to complete the questionnaire, ensuring the confidentiality of the information, and the possibility of withdrawing from the study at any stage without any harm or problem. They were informed that participation in the research was completely voluntary, and it was also explained that these tests did not contain any “identifying information”. They were asked to answer the questions accurately and honestly. The approximate time to complete all three questionnaires was estimated to be about 20 to 30 minutes, which was provided in a quiet and undisturbed environment. The process of completing the questionnaires took one month.
Tools
Generalized anxiety disorder scale (GAD-15)
GAD-15 scale is a revised version of the questionnaire by Mishra & Varma [5] expanded to 15 items in 2021 to provide a more precise assessment of generalized anxiety symptoms. This instrument uses a 6-point Likert scale (0=never to 5=always) to measure symptoms, such as persistent worry, restlessness, muscle tension, and sleep disturbance. Various studies, including those by Calear et al. [34], have confirmed its construct validity and high reliability (Cronbach’s α of 0.83). In a study by Villarreal-Zegarra et al. [2] on 199 students at Shahed University and 24 subjects diagnosed with GAD, the internal consistency of the questionnaire was calculated using Cronbach’s α and the number was 0.85% and the correlation between the two halves of the test was 0.65%. The reliability of the questionnaire was calculated by the test-retest method at an interval of 2 weeks and was 0.48%. The concurrent validity of the questionnaire was obtained using the Spielberger State Anxiety Scale of 0.71%, the Spielberger Trait Anxiety Scale of 0.52%, and the Symptom Checklist-90 Anxiety Subscale of 0.63%.
LES This 27-item questionnaire was designed by Scherbakov et al. [9] to measure chronic life stress. It assesses stress caused by life events in five main areas (family, work/education, finances, health, and other). Scoring is based on a 6-point Likert scale (0=no stress to 5=very high stress), and the total score ranges from 0 to 135. Ghasemi -Nawab et al. reported a Cronbach’s α coefficient of 0.78 in their study on a sample of middle-aged Iranian men and women (60 years and older) in 2016.
Mental health literacy scale
This 30-item scale, developed by Haslam and Tse [17], measures three main components of mental health literacy (awareness of thoughts/emotions, mindfulness, and self-knowledge) using a 6-point Likert scale (0=not at all to 5=completely). The total score ranges from 0 to 150 and categorizes mental health literacy levels into low, medium, and high. Its construct validity has been confirmed in factor analyses (CFI=0.91) and reliability with a Cronbach’s α of 0.87 in the original version. Jafari et al. in their study of 346 students at Shahrood University in 2020, reported a Cronbach’s α of 0.87.
Results
Demographic attributes
In the present study, the demographic characteristics of the participants included factors, such as age group, employment status, education level, and number of children, each of which can have different effects on the relationship between stressful life events and GAD.
The largest number of participants were in the 31-40 years (39.06%) and 18-30 years (31.25%) age groups, indicating a broad presence of young and middle-aged women in the study. The 41-50 years age group also constituted a reasonable number of participants at 20.83%, indicating active participation of women in older age groups. Finally, the 51-year-old and older age group had the lowest frequency at (8.85%). The results showed that more than half of the participants (54.69%) were employed, and a significant portion were housewives and unemployed (45.31%). The highest percentage of participants (46.88%) had a bachelor’s degree, which indicates a population with relatively high education. A total of 26.04% of participants had a diploma or less, and 27.08% had a master’s degree or higher. Finally, the number of children was a demographic characteristic significantly examined in this study. The results showed that 31.25% of participants had one child, 33.85% had two children, and 21.88% of participants had three or more children. 13.02% of women were childless.
Descriptive analysis
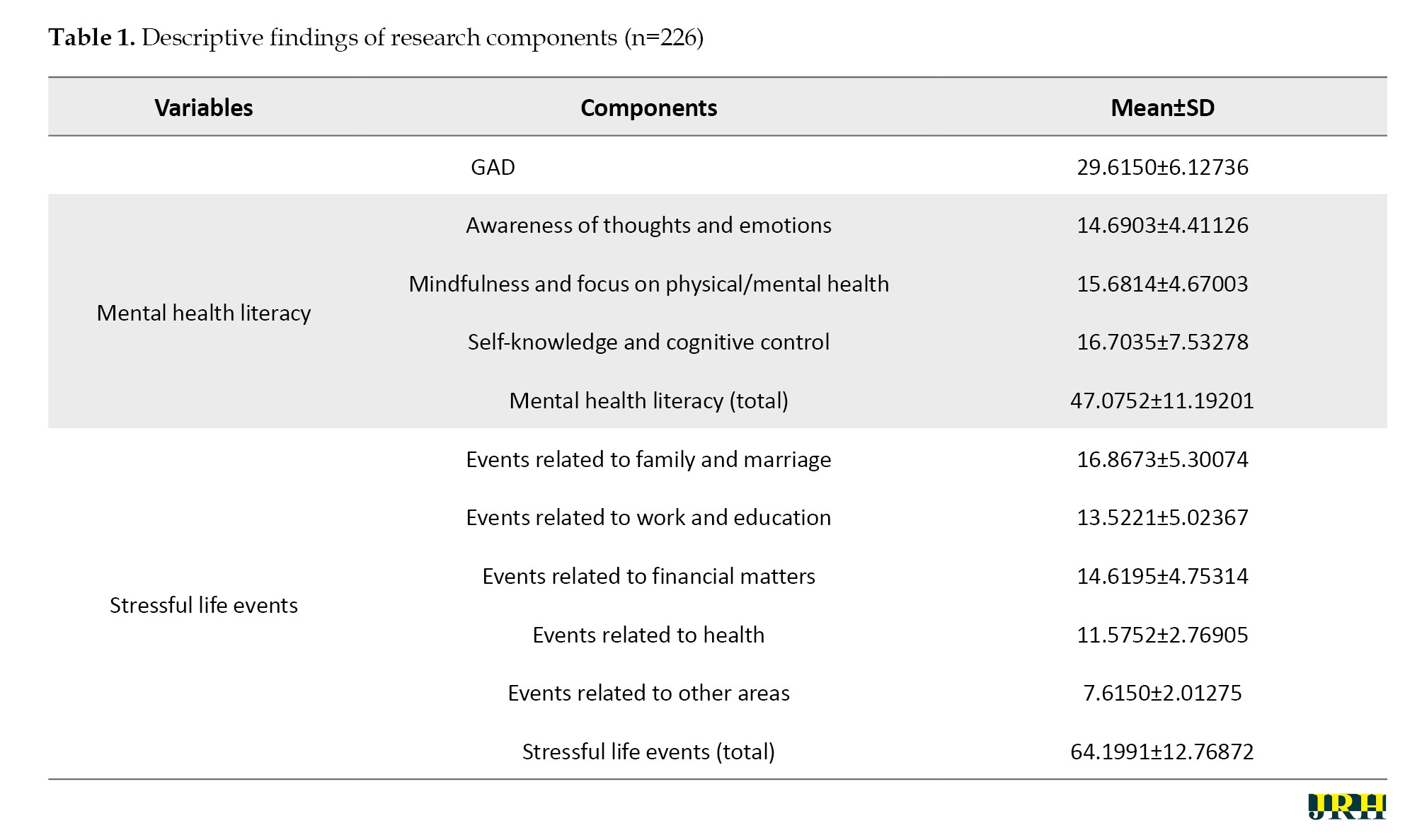
In Table 1, the information obtained from the administration of questionnaires to the sample members was subjected to descriptive analysis. The information presented in this section included the mean and standard deviation of the results from the questionnaires administered to the research participants. The descriptive results of the present study show the mean and standard deviation of the various components examined in a sample of 226 individuals. The variable value of GAD indicates a high level of anxiety in the study sample and indicates a high degree of stress and worry among the participants. The total score of mental health literacy indicates a wide range of different cognitive and emotional abilities among the participants. The total score of stressful life events indicates that the participants in this study experienced a significant amount of stress in different areas of their lives.
Regression analysis
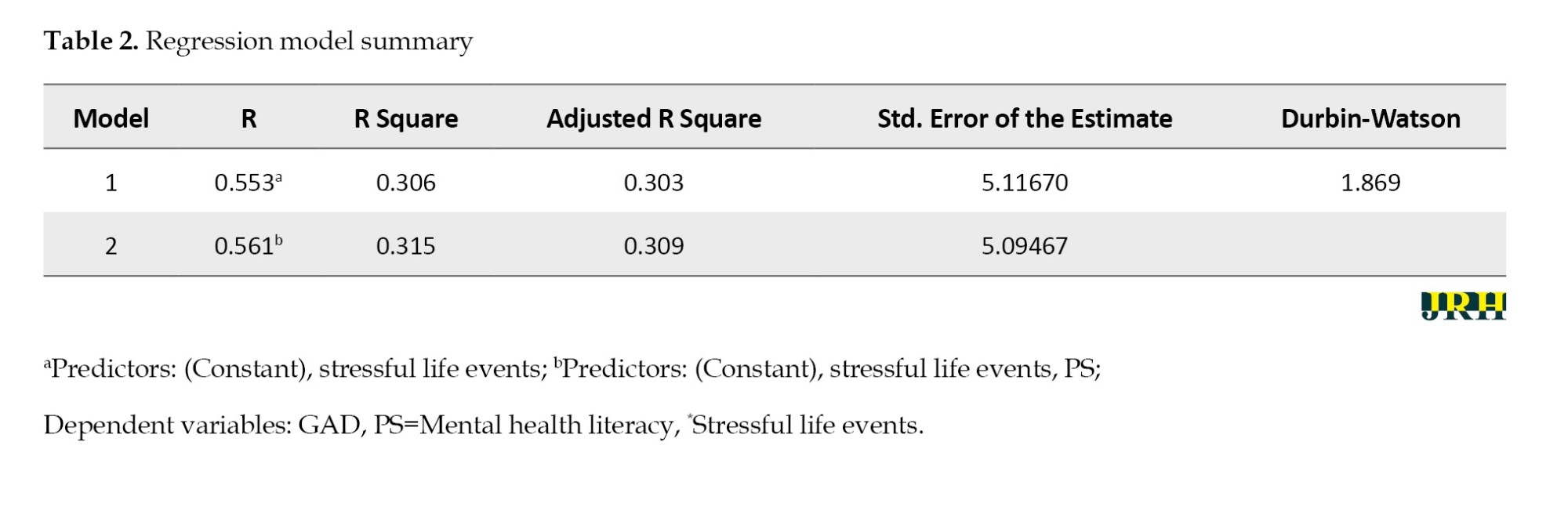
To examine the moderating role of mental health literacy, stepwise regression analysis and the creation of a new variable, namely the product of the centered mental health literacy score and stressful life events (Mental Health Literacy×Stressful Events [P×S]), were used. In stepwise regression, predictor variables are added or removed one by one, depending on the criteria, to examine the importance of each. In stepwise regression, there is a backward or forward approach, although both are often best used during exploratory research because predictions are sometimes inaccurate. The results in Table 2 indicate that in the first model, the correlation coefficient (R) is 0.553, showing a relatively strong relationship between stressful events and GAD. Also, R² is 0.306, meaning that stressful life events explain 30.6% of the variance in GAD scores. The standard error of the model is also 5.11670. In the second model, the R value increased to 0.561, indicating an improvement in the model with the addition of the moderating variable. Also, the R² value increased from 0.306 to 0.315, indicating that with the addition of the interaction variable, another 0.9% of the variance in the dependent variable (GAD) was explained. This value indicates the moderating role of mental health literacy.
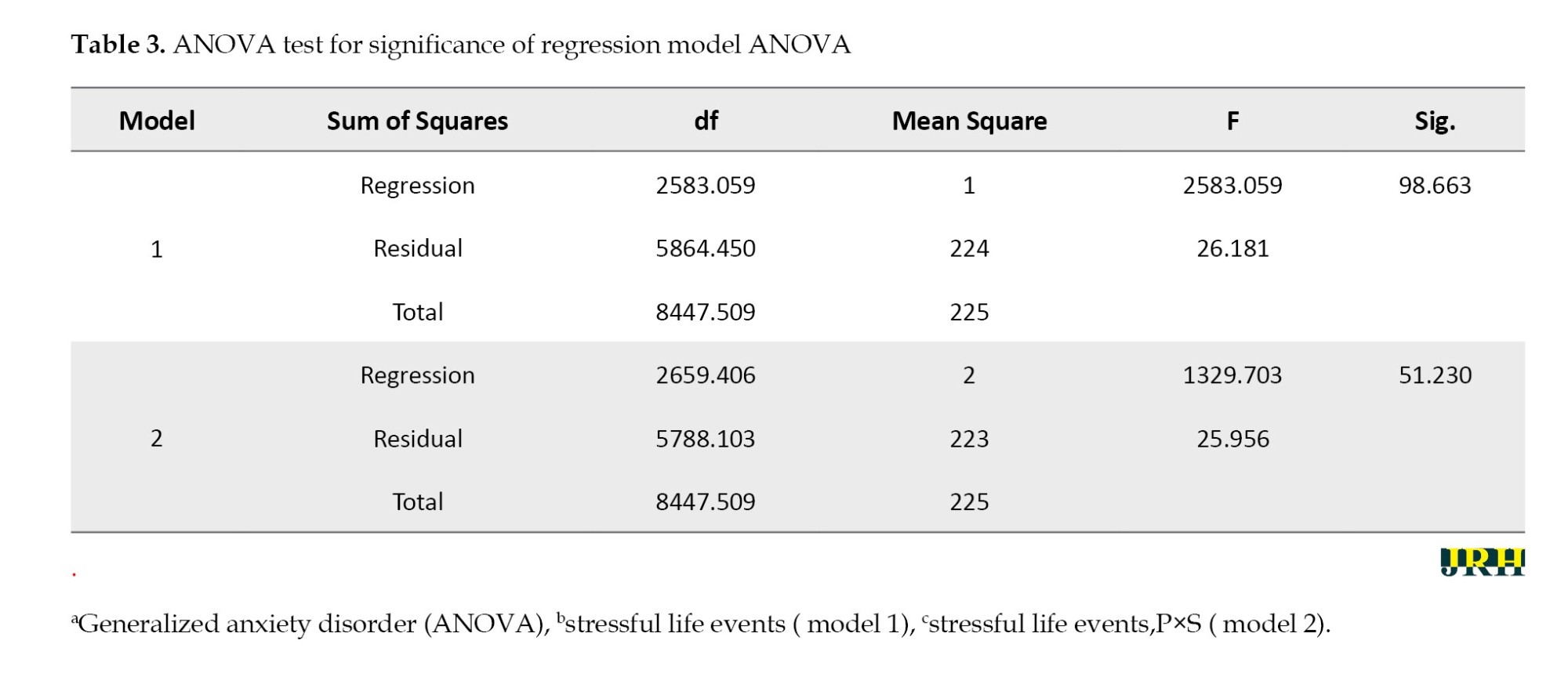
The results of the analysis of variance (ANOVA) test in Table 3 showed that the regression models could significantly predict GAD. In the first model, which only included the variable of stressful life events, the F value was 98.663, and the significance level was less than 0.001, indicating the significant impact of this variable on GAD. In the second model, with the addition of the interaction variable (P×S=mental health literacy×stressful events), the F value reached 51.230 and was still significant at the 0.001 level. Also, the increase in the sum of squares for regression from 2583.059 to 2659.406 and the decrease in the sum of squares for residuals from 5864.450 to 5788.103 showed that adding the interaction variable improved the model.
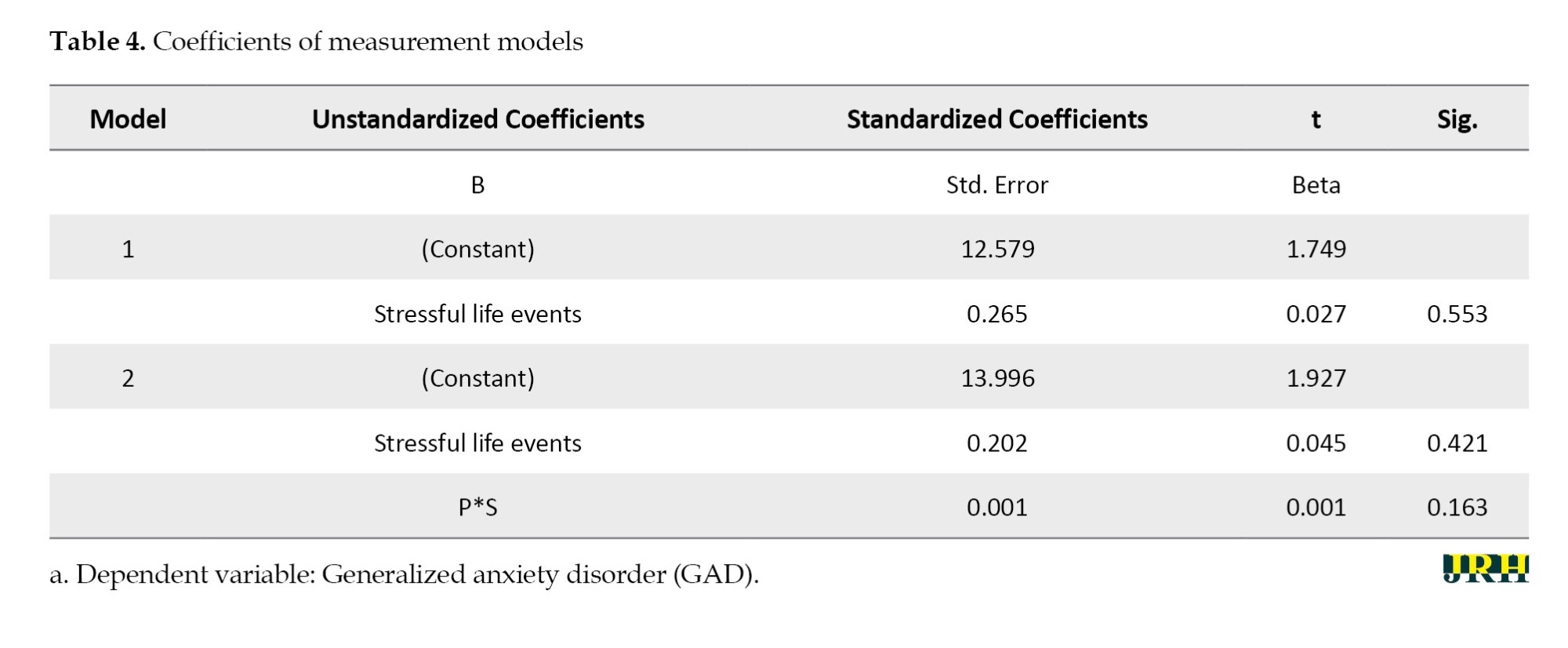
According to the results in Table 4, the results of the stepwise multiple regression analysis show that stressful life events are significant predictors of GAD, and mental health literacy has a moderating role in this relationship. In the first model, only the stressful life events variable was entered into the equation, and the beta coefficient (β) was 0.553 with a significance level of less than 0.001. This finding indicates that an increase in stressful life events leads to an increase in the level of GAD. Also, the B value of 0.265 indicates that for every unit increase in stressful life events, the GAD level increases by 0.265 units. In the second model, after adding the interaction variable (P×S), the beta coefficient of stressful life events decreased (β=0.421), indicating that the direct effect of this variable decreased after considering the moderating role of mental health literacy. The standardized coefficient (β) for the interaction variable was 0.163, and its significance level was 0.048, indicating the significant moderating role of mental health literacy. The B value for the interaction variable is 0.001, which shows that the interaction between mental health literacy and stressful life events influences the reduction of the effect of stressful life events on generalized anxiety. The findings confirm that stressful events play a decisive role in increasing GAD, and mental health literacy can moderate this relationship.
Discussion
The results of the present study showed that mental health literacy could have a moderating role in this relationship. This means that married women with higher levels of mental health literacy are less likely to experience symptoms of GAD in response to the negative effects of stressful events. In fact, increasing the level of mental health literacy helps individuals to cope effectively with stressful events and use them as stimuli for personal growth and development. The results obtained from the main hypothesis of the study are consistent with the findings of studies [35, 36]. All of these studies point to the crucial role of mental health literacy and awareness in reducing anxiety and improving the management of stressful situations. For example, research [35]shows that low health literacy is common among psychiatric patients, especially those with anxiety disorders and schizophrenia. This research suggests that people with lower health literacy are less likely to understand and manage their health better, which can directly affect the severity of their anxiety and mental disorders. Married women may be exposed to stressful events due to family and social life responsibilities, which can predispose them to anxiety disorders, such as GAD. However, when they are mentally literate, they can effectively use healthy coping strategies and reduce their anxiety levels. Previous research has also shown that people with better mental health literacy can identify anxiety symptoms early and use more effective treatment interventions. This study [36] also shows that anxiety literacy and social stigma have a direct impact on adolescents’ help-seeking for GAD. These findings indicate that individuals with high anxiety literacy are more likely to seek help, and positive attitudes toward help-seeking are associated with high anxiety literacy and lower social stigma. Health literacy, similar to anxiety literacy, can have a significant impact on an individual’s ability to cope with anxiety and seek help from various support resources. Therefore, health literacy can indirectly help individuals identify their anxiety and seek effective treatments and solutions to reduce it. The results of this study are consistent with cognitive-behavioral theories of anxiety, which emphasize that anxiety arises from individuals’ cognitive appraisals of stressful situations. According to cognitive models, life stresses themselves do not cause anxiety; rather, how an individual interprets and processes these stressful situations determines whether or not anxiety increases. Individuals with higher levels of mental health literacy tend to have a more balanced attitude toward stressful situations, are better able to recognize negative automatic thoughts, and, as a result, experience less anxiety. On the other hand, individuals with lower mental health literacy may be influenced by negative thoughts, perceive life stresses as uncontrollable threats, and experience more severe anxiety. Furthermore, the findings of this study are consistent with previous studies. For example, studies that have emphasized the role of mindfulness in reducing anxiety have shown that being aware of thoughts and feelings, without getting emotionally involved with them, can reduce the impact of stressful events. In one study [34], people who practice mindfulness exercises were found to have lower levels of anxiety because the exercises help them observe their thoughts and feelings without overreacting. On the other hand, the research has shown that increased mental health literacy is also associated with better emotional regulation. Being aware and understanding one’s own emotions, accepting those emotions, controlling impulses, being resilient in the face of unpleasant emotions, and implementing appropriate emotion regulation techniques in dealing with stressful life events reduce levels of anxiety and worry [37].
Conclusion
The present study showed that married women with higher levels of mental health literacy experienced less anxiety, even when their life stress levels were high.
From a positive psychology perspective, mental health literacy can act as a supportive resource against stress. Individuals with high levels of mental health literacy can adopt an adaptive approach instead of becoming overly involved with stressful events and can use positive emotion regulation strategies. They can observe stressful situations from different angles and control their emotional reactions. In contrast, individuals with low levels of mental health literacy are usually caught in negative thought patterns. They are unable to manage life stresses, which ultimately leads to increased generalized anxiety. Given the importance and special position of married women in the family, investing in increasing mental health literacy in this group in particular can have preventive and multifaceted effects in optimizing the mental health status of individuals in society and be a crucial step in moving towards a healthy society.
The policymakers should facilitate easier access to these facilities for married women by adopting appropriate programs and measures to consider support resources and reduce costs related to mental health care. Officials need to include educational programs in the mass media and hold workshops to promote mental health literacy and reduce the social stigma associated with it, focusing on married women.
Limitations
This study used a cross-sectional research design, which limits the ability to establish causal relationships between variables. Future studies with a longitudinal design to collect data at multiple time points would allow for a more comprehensive examination of the relationship between variables. The sample only included married women in Neyshabur City, which limits the generalizability of the findings to other geographical and cultural areas. Convenience sampling was another limitation that suggests that other sampling methods be used in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University of Neyshabur, Iran (Code: IR.IAU.NEYSHABUR.REC.1403.031).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Acknowledgments
The author thanks the people who contributed to this research.
References
Mental health, as a fundamental pillar of human well-being, plays a vital role in individual quality of life, social functioning, and the sustainable development of societies. Mental disorders, particularly anxiety disorders, impose a significant burden on health systems, economies, and human relationships, and are recognized as one of the main public health challenges globally. Among the wide spectrum of anxiety disorders, GAD holds a special position due to its chronic nature, the pervasiveness of worries, and its profound impact on various aspects of life [1]. In 2020, before COVID-19, the estimated global incidence of AD reached 298 million people, and after the pandemic, the incidence increased by 25.6% to an estimated global prevalence of 374 million people. This increase was also greater for women (27.9%; 51.8 million people) than for men (21.7%; 24.4 million people). The considerable prevalence of GAD in the general population, with recent estimates emphasizing the need for active screening for undiagnosed cases [2], its higher prevalence in women [1] and its association with reduced occupational, academic, and social functioning, as well as increased use of health services, highlight the necessity for a deeper understanding of its related risk and protective factors [3, 4].
GAD, extending beyond typical daily worries, is a debilitating clinical condition defined by excessive and uncontrollable anxiety and apprehension about various topics, even in the absence of a real threat or out of proportion to the importance of the situation [1, 5]. Understanding the etiology of GAD requires an integrated and multifactorial approach that considers the complex interaction between biological vulnerabilities, psychological factors (such as intolerance of uncertainty, positive beliefs about worry, and cognitive avoidance), and environmental and social influences [4, 6]. One of the crucial risk factors for the onset, exacerbation, and persistence of anxiety and mood disorders is the experience of stressful life events [7, 8]. These events can contribute to the development of mental disorders by disrupting the individual’s psychophysiological balance and straining coping resources. These events range from severe and traumatic events (such as bereavement, abuse, natural disasters) to chronic stressors (such as financial problems or marital conflicts) [8, 9]. Epidemiological and clinical studies, including longitudinal studies, have consistently shown that exposure to stressful life events, particularly adverse childhood experiences and the accumulation of stressors throughout life, significantly increases the risk of developing anxiety disorders (including GAD), depression, and even psychosis, and is associated with adverse physical and mental health outcomes in adulthood [7, 10, 11]. These events appear to occur through various pathways, including psychological pathways (such as creating or activating negative cognitive schemas, reinforcing attentional biases towards threat, reducing feelings of control and self-efficacy, weakening coping strategies), leading to increased vulnerability to mental disorders [12, 13].
In the context of GAD, stressful life events can act as triggers that initiate or exacerbate periods of intense and pervasive worry in susceptible individuals [6]. These events, particularly those that are unexpected, uncontrollable, and threatening to an individual’s crucial goals or values, may challenge fundamental beliefs about the safety, controllability, and predictability of the world, leading to the activation of negative cognitive schemas related to threat, danger, and inability to cope, which are prominent features of GAD [4]. Furthermore, chronic stress resulting from stressful life events can deplete an individual’s cognitive and emotional resources, reducing their capacity for emotion regulation and the use of adaptive coping strategies, which in turn can contribute to the persistence of the worry and anxiety cycle [7, 13]. Therefore, understanding how individuals react to stressful events and, more importantly, what factors might moderate these reactions (i.e. change the strength or direction of the relationship between stress and outcome) is crucial for a better understanding of the etiology and course of GAD and for designing effective preventive and therapeutic interventions.
The present study specifically focuses on the population of married women. Epidemiological studies have consistently reported a higher prevalence of anxiety disorders, including GAD, in women compared to men (approximately twice as high) [1, 5]. Married women may also face a unique or exacerbated combination of stressors resulting from multiple and sometimes conflicting responsibilities in family, work, and social domains. The pressures of managing household chores, caring for children (especially if there is a child with special needs [14]), maintaining the quality of marital relationships, employment (and work-life balance), family financial issues, caring for aging parents, and cultural pressures related to expectations of the roles of wife and motherhood can all act as crucial sources of acute and chronic stressful life events [15], adding to the importance of examining factors affecting mental health in this specific context. Therefore, understanding how married women cope with the multiple stresses of their lives and what individual or social resources might enhance their resilience against the development or exacerbation of GAD is of high importance and can contribute to the design of gender-sensitive and culturally-contextualized interventions.
Meanwhile, identifying protective factors that can reduce the negative effects of stress on mental health has become increasingly crucial. One such potential protective factor is the concept of “mental health literacy,” defined as “knowledge and beliefs about mental disorders that help diagnose, manage, or prevent them” [16, 17]. This concept is multifaceted and includes various components, such as the ability to recognize the onset or presence of specific mental disorders (e.g. recognizing symptoms of anxiety or depression), knowledge and beliefs about the causes, risk factors, and prognosis of mental disorders, awareness of various professional help-seeking options (e.g. psychotherapy, pharmacotherapy) and available self-help resources, knowledge and skills necessary to provide psychological first aid to others, and attitudes that facilitate the recognition and seeking of appropriate help and reduce the social stigma associated with mental illness [18, 19]. Research increasingly shows that higher levels of mental health literacy are associated with a wide range of positive mental health outcomes, including more positive attitudes towards individuals with mental illness and mental health treatments, reduced personal and social stigma, increased intention and effective help-seeking behavior, improved adherence to treatment, and higher levels of psychological and social well-being in various populations (such as students, teachers, employees, outpatients, general population) [20-23].
Considering the various components of mental health literacy, it can be argued that mental health literacy has the potential to act as a protective shield or moderating factor against the harmful effects of stressful life events on the development or exacerbation of GAD. Firstly, individuals with higher mental health literacy are likely better able to recognize early signs of psychological distress resulting from stress (such as excessive worry, restlessness, sleep disturbance) in themselves or others and identify it as a potential mental health problem, rather than attributing it merely to personal weakness or transient conditions [19, 24]. This early recognition can lead to timely seeking of professional help or the use of evidence-based self-help strategies before symptoms become chronic and reach the level of a full-blown clinical disorder [21]. Knowledge about the causes and risk factors of mental disorders, which is part of mental health literacy, may help individuals better understand the role of life stressors in their mental state and avoid unhelpful rumination or self-blame [25]. Awareness of effective treatment options and more positive attitudes towards treatment (associated with higher mental health literacy) can increase an individual’s motivation and adherence to pursuing treatment and actively using healthy coping strategies (such as problem-solving, cognitive restructuring, relaxation exercises) [26]. Mental health literacy can, by reducing the stigma associated with mental health problems, encourage individuals to share their stressful experiences and resulting emotions with their support network (spouse, family, friends) and benefit from social support, which is itself a very important protective factor against stress [14, 27]. Consequently, mental health literacy not only aids in recognition and treatment but also potentially strengthens an individual’s coping processes and adaptation to life’s adversities and stresses, contributing to the maintenance or improvement of overall well-being [28, 29].
Given the strong theoretical and empirical link between stressful life events and GAD on one hand, and the protective and empowering potential of mental health literacy on the other, the central question of this research is whether mental health literacy can moderate the negative and detrimental impact of stressful life events on the severity of GAD symptoms.
Despite the potential theoretical and clinical importance of this topic, a distinct research gap exists in the detailed examination of the moderating role of mental health literacy in the relationship between stressful life events and GAD, particularly within the specific population of married Iranian women. Most previous studies in the field of mental health literacy have either focused on bivariate relationships between these variables (such as examining the association of stressful life events with GAD or the relationship of mental health literacy with help-seeking, stigma, or general well-being) or have investigated the role of mental health literacy as a direct predictor of mental health outcomes or as a mediator in other pathways [23, 30, 31]. Studies specifically examining the moderating role of mental health literacy in the relationship between stress and mental health outcomes are relatively limited and have often been conducted in student populations [32], the general population during crises, such as the COVID-19 pandemic [33], or specific occupational groups [20] and have less frequently focused specifically on married women and their unique challenges and resources within a specific cultural context like Iran. The present study, by focusing on married women in Iran and examining the moderating role of mental health literacy (using appropriate tools) in an integrated model that considers both environmental risk factors (stressful life events) and cognitive-social protective factors (mental health literacy) in relation to a common and debilitating disorder (GAD), seeks to fill this important research gap. Therefore, this study seeks to answer the main question: Does the level of mental health literacy moderate the relationship between stressful life events and GAD in married women?
The findings of this research can have significant theoretical and practical implications in the fields of clinical psychology, health psychology, and public health. From a theoretical perspective, this study contributes to a better understanding of the complex interplay between environmental stressors, individual protective resources, and psychopathology, providing further empirical evidence for vulnerability-stress models as well as models based on resilience and protective factors. From a practical and clinical perspective, the results of this research can provide useful guidance for the design and implementation of targeted preventive and therapeutic interventions. These programs could focus on increasing practical knowledge about anxiety, its causes, and effective management strategies, normalizing experiences related to stress and anxiety, reducing the stigma of mental illness and help-seeking, strengthening effective help-seeking skills (for oneself and others), and promoting adaptive coping strategies [17, 18].
Methods
Procedure
This descriptive-correlational research employed a cross-sectional design. The inclusion criteria included married women residing in Neyshabur City, Iran, and voluntary participation. Incomplete completion of the questionnaire was an exclusion criterion.
Sample and sampling method
The sample of the present study was 226 married women living in Neyshabur City. Considering the purpose of the study and the time and place constraints, the sampling method was used. In this way, the sample was selected from among the individuals who were available to the researcher at the time of the study and who met the inclusion criteria for the study. This method was chosen due to the time constraints and the implementation facilities of the study. It should be noted that in selecting individuals, an attempt was made to observe relative diversity in terms of age, gender, and social conditions, to reduce the incidence of bias in the results. In this regard, the inclusion and exclusion criteria were carefully determined and implemented.
Given the aim of the study, which is to investigate the mediating role of mental health literacy in the relationship between stressful life events and generalized anxiety in married women in Neyshabur City, a sample size of 226 people was determined based on Cohen’s formula for the regression test. Based on previous studies and methodological standards, considering the medium effect size (f²=0.15), the statistical power level of 0.80, and the significance level (α) of 0.05, a sample size of 226 people is appropriate.
The inclusion criteria included being a woman and having an official marriage (legal or religious) at the time of the study, age between 18 and 55 years, residing in Neyshabur City, having at least one year of cohabitation, ability to read and write in Persian, and willingness and informed consent to participate in the study. The exclusion criteria also included no severe psychiatric diagnosis or history of psychiatric illness in the past year, experience of divorce or remarriage or severe emotional separation in the past six months, chronic debilitating physical illnesses such as cancer or kidney failure, pregnancy or childbirth in the past six months, and incomplete or distorted completion of the questionnaires.
Data were collected using the completion of three mental health literacy questionnaires, the generalized anxiety scale, and the life events scale (LES) in person.
For this purpose, after obtaining the necessary ethical permission from the university research committee, the researcher visited centers and environments related to the target community (such as health centers, health homes, cultural centers, etc.) with prior coordination. In these centers, while introducing the purpose and importance of the research, eligible participants were selected voluntarily. To comply with ethical principles, before completing the questionnaire, comprehensive explanations were given on how to complete the questionnaire, ensuring the confidentiality of the information, and the possibility of withdrawing from the study at any stage without any harm or problem. They were informed that participation in the research was completely voluntary, and it was also explained that these tests did not contain any “identifying information”. They were asked to answer the questions accurately and honestly. The approximate time to complete all three questionnaires was estimated to be about 20 to 30 minutes, which was provided in a quiet and undisturbed environment. The process of completing the questionnaires took one month.
Tools
Generalized anxiety disorder scale (GAD-15)
GAD-15 scale is a revised version of the questionnaire by Mishra & Varma [5] expanded to 15 items in 2021 to provide a more precise assessment of generalized anxiety symptoms. This instrument uses a 6-point Likert scale (0=never to 5=always) to measure symptoms, such as persistent worry, restlessness, muscle tension, and sleep disturbance. Various studies, including those by Calear et al. [34], have confirmed its construct validity and high reliability (Cronbach’s α of 0.83). In a study by Villarreal-Zegarra et al. [2] on 199 students at Shahed University and 24 subjects diagnosed with GAD, the internal consistency of the questionnaire was calculated using Cronbach’s α and the number was 0.85% and the correlation between the two halves of the test was 0.65%. The reliability of the questionnaire was calculated by the test-retest method at an interval of 2 weeks and was 0.48%. The concurrent validity of the questionnaire was obtained using the Spielberger State Anxiety Scale of 0.71%, the Spielberger Trait Anxiety Scale of 0.52%, and the Symptom Checklist-90 Anxiety Subscale of 0.63%.
LES This 27-item questionnaire was designed by Scherbakov et al. [9] to measure chronic life stress. It assesses stress caused by life events in five main areas (family, work/education, finances, health, and other). Scoring is based on a 6-point Likert scale (0=no stress to 5=very high stress), and the total score ranges from 0 to 135. Ghasemi -Nawab et al. reported a Cronbach’s α coefficient of 0.78 in their study on a sample of middle-aged Iranian men and women (60 years and older) in 2016.
Mental health literacy scale
This 30-item scale, developed by Haslam and Tse [17], measures three main components of mental health literacy (awareness of thoughts/emotions, mindfulness, and self-knowledge) using a 6-point Likert scale (0=not at all to 5=completely). The total score ranges from 0 to 150 and categorizes mental health literacy levels into low, medium, and high. Its construct validity has been confirmed in factor analyses (CFI=0.91) and reliability with a Cronbach’s α of 0.87 in the original version. Jafari et al. in their study of 346 students at Shahrood University in 2020, reported a Cronbach’s α of 0.87.
Results
Demographic attributes
In the present study, the demographic characteristics of the participants included factors, such as age group, employment status, education level, and number of children, each of which can have different effects on the relationship between stressful life events and GAD.
The largest number of participants were in the 31-40 years (39.06%) and 18-30 years (31.25%) age groups, indicating a broad presence of young and middle-aged women in the study. The 41-50 years age group also constituted a reasonable number of participants at 20.83%, indicating active participation of women in older age groups. Finally, the 51-year-old and older age group had the lowest frequency at (8.85%). The results showed that more than half of the participants (54.69%) were employed, and a significant portion were housewives and unemployed (45.31%). The highest percentage of participants (46.88%) had a bachelor’s degree, which indicates a population with relatively high education. A total of 26.04% of participants had a diploma or less, and 27.08% had a master’s degree or higher. Finally, the number of children was a demographic characteristic significantly examined in this study. The results showed that 31.25% of participants had one child, 33.85% had two children, and 21.88% of participants had three or more children. 13.02% of women were childless.
Descriptive analysis
In Table 1, the information obtained from the administration of questionnaires to the sample members was subjected to descriptive analysis. The information presented in this section included the mean and standard deviation of the results from the questionnaires administered to the research participants. The descriptive results of the present study show the mean and standard deviation of the various components examined in a sample of 226 individuals. The variable value of GAD indicates a high level of anxiety in the study sample and indicates a high degree of stress and worry among the participants. The total score of mental health literacy indicates a wide range of different cognitive and emotional abilities among the participants. The total score of stressful life events indicates that the participants in this study experienced a significant amount of stress in different areas of their lives.
Regression analysis
To examine the moderating role of mental health literacy, stepwise regression analysis and the creation of a new variable, namely the product of the centered mental health literacy score and stressful life events (Mental Health Literacy×Stressful Events [P×S]), were used. In stepwise regression, predictor variables are added or removed one by one, depending on the criteria, to examine the importance of each. In stepwise regression, there is a backward or forward approach, although both are often best used during exploratory research because predictions are sometimes inaccurate. The results in Table 2 indicate that in the first model, the correlation coefficient (R) is 0.553, showing a relatively strong relationship between stressful events and GAD. Also, R² is 0.306, meaning that stressful life events explain 30.6% of the variance in GAD scores. The standard error of the model is also 5.11670. In the second model, the R value increased to 0.561, indicating an improvement in the model with the addition of the moderating variable. Also, the R² value increased from 0.306 to 0.315, indicating that with the addition of the interaction variable, another 0.9% of the variance in the dependent variable (GAD) was explained. This value indicates the moderating role of mental health literacy.
The results of the analysis of variance (ANOVA) test in Table 3 showed that the regression models could significantly predict GAD. In the first model, which only included the variable of stressful life events, the F value was 98.663, and the significance level was less than 0.001, indicating the significant impact of this variable on GAD. In the second model, with the addition of the interaction variable (P×S=mental health literacy×stressful events), the F value reached 51.230 and was still significant at the 0.001 level. Also, the increase in the sum of squares for regression from 2583.059 to 2659.406 and the decrease in the sum of squares for residuals from 5864.450 to 5788.103 showed that adding the interaction variable improved the model.
According to the results in Table 4, the results of the stepwise multiple regression analysis show that stressful life events are significant predictors of GAD, and mental health literacy has a moderating role in this relationship. In the first model, only the stressful life events variable was entered into the equation, and the beta coefficient (β) was 0.553 with a significance level of less than 0.001. This finding indicates that an increase in stressful life events leads to an increase in the level of GAD. Also, the B value of 0.265 indicates that for every unit increase in stressful life events, the GAD level increases by 0.265 units. In the second model, after adding the interaction variable (P×S), the beta coefficient of stressful life events decreased (β=0.421), indicating that the direct effect of this variable decreased after considering the moderating role of mental health literacy. The standardized coefficient (β) for the interaction variable was 0.163, and its significance level was 0.048, indicating the significant moderating role of mental health literacy. The B value for the interaction variable is 0.001, which shows that the interaction between mental health literacy and stressful life events influences the reduction of the effect of stressful life events on generalized anxiety. The findings confirm that stressful events play a decisive role in increasing GAD, and mental health literacy can moderate this relationship.
Discussion
The results of the present study showed that mental health literacy could have a moderating role in this relationship. This means that married women with higher levels of mental health literacy are less likely to experience symptoms of GAD in response to the negative effects of stressful events. In fact, increasing the level of mental health literacy helps individuals to cope effectively with stressful events and use them as stimuli for personal growth and development. The results obtained from the main hypothesis of the study are consistent with the findings of studies [35, 36]. All of these studies point to the crucial role of mental health literacy and awareness in reducing anxiety and improving the management of stressful situations. For example, research [35]shows that low health literacy is common among psychiatric patients, especially those with anxiety disorders and schizophrenia. This research suggests that people with lower health literacy are less likely to understand and manage their health better, which can directly affect the severity of their anxiety and mental disorders. Married women may be exposed to stressful events due to family and social life responsibilities, which can predispose them to anxiety disorders, such as GAD. However, when they are mentally literate, they can effectively use healthy coping strategies and reduce their anxiety levels. Previous research has also shown that people with better mental health literacy can identify anxiety symptoms early and use more effective treatment interventions. This study [36] also shows that anxiety literacy and social stigma have a direct impact on adolescents’ help-seeking for GAD. These findings indicate that individuals with high anxiety literacy are more likely to seek help, and positive attitudes toward help-seeking are associated with high anxiety literacy and lower social stigma. Health literacy, similar to anxiety literacy, can have a significant impact on an individual’s ability to cope with anxiety and seek help from various support resources. Therefore, health literacy can indirectly help individuals identify their anxiety and seek effective treatments and solutions to reduce it. The results of this study are consistent with cognitive-behavioral theories of anxiety, which emphasize that anxiety arises from individuals’ cognitive appraisals of stressful situations. According to cognitive models, life stresses themselves do not cause anxiety; rather, how an individual interprets and processes these stressful situations determines whether or not anxiety increases. Individuals with higher levels of mental health literacy tend to have a more balanced attitude toward stressful situations, are better able to recognize negative automatic thoughts, and, as a result, experience less anxiety. On the other hand, individuals with lower mental health literacy may be influenced by negative thoughts, perceive life stresses as uncontrollable threats, and experience more severe anxiety. Furthermore, the findings of this study are consistent with previous studies. For example, studies that have emphasized the role of mindfulness in reducing anxiety have shown that being aware of thoughts and feelings, without getting emotionally involved with them, can reduce the impact of stressful events. In one study [34], people who practice mindfulness exercises were found to have lower levels of anxiety because the exercises help them observe their thoughts and feelings without overreacting. On the other hand, the research has shown that increased mental health literacy is also associated with better emotional regulation. Being aware and understanding one’s own emotions, accepting those emotions, controlling impulses, being resilient in the face of unpleasant emotions, and implementing appropriate emotion regulation techniques in dealing with stressful life events reduce levels of anxiety and worry [37].
Conclusion
The present study showed that married women with higher levels of mental health literacy experienced less anxiety, even when their life stress levels were high.
From a positive psychology perspective, mental health literacy can act as a supportive resource against stress. Individuals with high levels of mental health literacy can adopt an adaptive approach instead of becoming overly involved with stressful events and can use positive emotion regulation strategies. They can observe stressful situations from different angles and control their emotional reactions. In contrast, individuals with low levels of mental health literacy are usually caught in negative thought patterns. They are unable to manage life stresses, which ultimately leads to increased generalized anxiety. Given the importance and special position of married women in the family, investing in increasing mental health literacy in this group in particular can have preventive and multifaceted effects in optimizing the mental health status of individuals in society and be a crucial step in moving towards a healthy society.
The policymakers should facilitate easier access to these facilities for married women by adopting appropriate programs and measures to consider support resources and reduce costs related to mental health care. Officials need to include educational programs in the mass media and hold workshops to promote mental health literacy and reduce the social stigma associated with it, focusing on married women.
Limitations
This study used a cross-sectional research design, which limits the ability to establish causal relationships between variables. Future studies with a longitudinal design to collect data at multiple time points would allow for a more comprehensive examination of the relationship between variables. The sample only included married women in Neyshabur City, which limits the generalizability of the findings to other geographical and cultural areas. Convenience sampling was another limitation that suggests that other sampling methods be used in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University of Neyshabur, Iran (Code: IR.IAU.NEYSHABUR.REC.1403.031).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Acknowledgments
The author thanks the people who contributed to this research.
References
- Putra AA, Dwiputri AR, Madani AF, Ramadhani DA, Maolidi J, Rabbani MA, et al. Generalized anxiety disorder (GAD): A literature review. Jurnal Biologi Tropis. 2024; 24(1b):597-603. [DOI:10.29303/jbt.v24i1b.7958]
- Villarreal-Zegarra D, Paredes-Angeles R, Mayo-Puchoc N, Arenas-Minaya E, Huarcaya-Victoria J, Copez-Lonzoy A. Psychometric properties of the GAD-7 (General Anxiety Disorder-7): A cross-sectional study of the Peruvian general population. BMC Psychology. 2024; 12(1):183. [DOI:10.1186/s40359-024-01688-8] [PMID]
- Bandelow B, Reitt M, Röver C, Michaelis S, Görlich Y, Wedekind D. Efficacy of treatments for anxiety disorders: A meta-analysis. International Clinical Psychopharmacology. 2015; 30:183–92. [DOI:10.1097/yic.0000000000000078]
- Zhang Z. A comprehensive overview on the generalized anxiety disorder - Etiology and treatment. SHS Web of Conferences. 2024; 193:03008. [DOI:10.1051/shsconf/202419303008]
- Mishra AK, Varma AR. A comprehensive review of the generalized anxiety disorder. Cureus. 2023; 15(9):e46115. [DOI:10.7759/cureus.46115]
- Bamalan OA, Alosaimi NM, Alfryyan AA, Aljubran HJ, Alanazi FH, Siddiqui ZI. Generalized anxiety disorder: A review of current literature in Saudi Arabia. Psychology. 2023; 14:35-51. [DOI:10.4236/psych.2023.141003]
- Jiang S. A comprehensive assessment of generalized anxiety disorder treatments. Interdisciplinary Humanities and Communication Studies. 2024; 2(8). [DOI:10.61173/ebzgas68]
- Liu T, Zou H, Tao Z, Qiu B, He X, Chen Y, et al. The relationship between stressful life events, sleep, emotional regulation, and depression in freshmen college students. Psychology in the Schools.2023; 60(11):4653-66. [DOI:10.1002/pits.23002]
- Scherbakov D, Mollalo A, Lenert L. Stressful life events in electronic health records: A scoping review. Journal of the American Medical Informatics Association. 2024; 31(4):1025-35. [DOI:10.1093/jamia/ocae023 ] [PMID]
- Kring L, Iversen E, Ibsen B, Fehsenfeld M. Exploring the impact of stressful life events on quality of life: Meaning making and narrative reconstruction. International Journal of Qualitative Studies on Health and Well-Being. 2024; 19(1):2330117. [DOI:10.1080/17482631.2024.2330117] [PMID]
- Roth A, Meigen C, Hiemisch A, Kiess W, Poulain T. Associations between stressful life events and increased physical and psychological health risks in adolescents: A longitudinal study. International Journal of Environmental Research and Public Health. 2024; 20(2):1050. [DOI:10.3390/ijerph20021050] [PMID]
- Colizzi M, Cullen AE, Martland N, Di Forti M, Murray R, Schoeler T, et al. Association between stressful life events and psychosis relapse: A 2-year prospective study in first-episode psychosis. World Psychiatry. 2023; 22(1):159-60. [DOI:10.1002/wps.21046] [PMID]
- Xie J, Cheng G, Zhou M, Liang Q, Wang Q. Exploring the relationship between mental health status and life events in children and adolescents: The role of mediating factors. Frontiers in psychiatry. 2025; 16:1520353. [DOI:10.3389/fpsyt.2025.1520353] [PMID]
- Hudson G, Fung C, Sureshkumar DS, Gómez-Restrepo C, Uribe-Restrepo JM, Ariza-Salazar K, et al. Do coping mechanisms moderate the effect of stressful life events on depression and anxiety in young people? A case-control study from Latin America. BMJ Mental Health. 2025; 28(1):e301087. [DOI:10.1136/bmjment-2024-301087] [PMID]
- Du X, Dong Q, Sun L, Chen X, Jiang J. The effect of social support on the mental health literacy of parents who have children with special needs: A moderated mediating effect. Psychology Research and Behavior Management. 2024; 17:1283-94. [DOI:10.2147/PRBM.S379762]
- Min Fui W, Abdul Majid H, Ismail R, Su TT, Maw Pin T, Said MA. Psychosocial factors associated with mental health and quality of life during the COVID-19 pandemic among low-income urban dwellers in Peninsular Malaysia. PLoS One. 2022; 17(8):e0264886. [DOI:10.1371/journal.pone.0264886] [PMID]
- Haslam N, Tse JS. Public awareness of mental illness: Mental health literacy or concept creep? Australasian psychiatry. 2025; 33(1):18-20. [DOI:10.1177/10398562241292202] [PMID]
- Jabari Z, Eslami M, Jalali Nadoushan AH, Goharinezhad S, Tavallaei M, Khodadoust E, et al. Psycheutopia: An innovative educational program to enhance mental health literacy among medical students. Frontiers in Psychiatry. 2025; 16:1538476. [DOI:10.3389/fpsyt.2025.1538476] [PMID]
- Marinucci A, Grové C, Allen KA, Hsu BN. Consulting the experts: young people's experiences of a school-based mental health literacy program. Australian Journal of Psychology. 2025; 77(1):2478089. [DOI:10.1080/00049530.2025.2478089] [PMID]
- Teixeira AI, Martins S, Lima S, Pinto F, Morgado T, Valentim O. A mixed methods approach to understanding mental health literacy among university health students. Healthcare. 2025; 13(7):724. [DOI:10.3390/ijerph22073594] [PMID]
- Garcia Colato E, Liu N, Chow A, Sherwood-Laughlin C, Macy JT. The association between IT-profession-specific stressors and mental health conditions plus the role of mental health literacy in help-seeking. medRxiv. 2025. [DOI:10.1101/2025.02.24.25322785]
- Lien YJ, Chen L, Cai J, Wang YH, Liu YY. The power of knowledge: How mental health literacy can overcome barriers to seeking help. American Journal of Orthopsychiatry. 2024; 94(2):127-47. [DOI:10.1037/ort0000708] [PMID]
- Ruscio AM, Borkovec TD. Experience and appraisal of worry among high worriers with and without generalized anxiety disorder. Behavior Research and Therapy. 2024; 42:1469–82. [DOI:10.1016/j.brat.2003.10.007]
- Jeong YW, Kim JH, Park HK. Study on the relationship between mental health literacy and psychological symptoms of university students: Mediating effect of grit. International Journal of Mental Health Promotion. 2023; 25(7):813-21.[DOI:10.32604/ijmhp.2023.027383]
- Jesse SY, Haslam N. Broad concepts of mental disorder predict self-diagnosis. SSM-Mental Health. 2024; 6:100326.[DOI:10.1016/j.ssmmh.2024.100326]
- Ahuvia IL, Schleider JL, Kneeland ET, Moser JS, Schroder HS. Depression self-labeling in U.S. college students: Associations with perceived control and coping strategies. Journal of Affective Disorders. 2024; 351:202-10. [DOI:10.1016/j.jad.2024.01.160] [PMID]
- Zhang JY, Ji XZ, Zhou YQ. The mediating effect of mental health literacy on psychological resilience and psychological distress of medical college students. Perspectives in Psychiatric Care. 2023; 2023:3461121. [DOI:10.1155/2023/3461121]
- Yazıcı H, Özdemir M. Predictors of secondary traumatic stress in mental health professionals: Trauma history, self-compassion, emotional intelligence. Journal of Rational-Emotive & Cognitive-Behavior Therapy. 2023; 41(1):162-75. [DOI:10.1007/s10942-022-00458-y ]
- Song J, Feng K, Zhang D, Wang S, Wang W, Li Y. The relationship between mental health literacy, overall adaptation and mental health of university freshers. Psychology Research and Behavior Management. 2023; 16:4935-47. [DOI:10.2147/PRBM.S437718] [PMID]
- Lindert L, Choi KE, Pfaff H, Zeike S. Health literacy at work - Individual and organizational health literacy, health supporting leadership and employee wellbeing. BMC Health Services Research. 2023; 23(1):736. [DOI:10.1186/s12913-023-09766-0] [PMID]
- Pan J, Xu T, Li D. The relationship between mental health literacy and social well-being: A longitudinal study in China. Behavioral Sciences. 2024; 15(1):29. [DOI:10.3390/bs15010029] [PMID]
- Dadgarinejad A, Nazarihermoshi N, Hematichegeni N, Jazaiery M, Yousefishad S, Mohammadian H, et al. Relationship between health literacy and generalized anxiety disorder during the COVID-19 pandemic in Khuzestan province, Iran. Frontiers in Psychology. 2024; 14:1294562. [DOI:10.3389/fpsyg.2023.1294562] [PMID]
- D’Aniello-Heyda C, Tambling RR, Kapeli SA, Sundram F. Rethinking measurement: A preliminary study of mental health literacy among college students. Cogent Psychology. 2025; 12(1):2480421. [DOI:10.1080/23311908.2025.2480421]
- Calear AL, Batterham PJ, Torok M, McCallum S. Help-seeking attitudes and intentions for generalized anxiety disorder in adolescents: The role of anxiety literacy and stigma. European Child & Adolescent Psychiatry. 2020; 30(2):243-51. [DOI:10.1007/s00787-020-01512-9] [PMID]
- Hu Y, Ye B, Tan J. Stress of COVID-19, anxiety, economic insecurity, and mental health literacy: A structural equation modeling approach. Frontiers in Psychology. 2021; 12:707079. [DOI:10.3389/fpsyg.2021.707079]
- Sato Y, Sugawara N, Kawamata Y, Shimoda K, Yasui-Furukori N. Survey of health literacy among Japanese outpatients with mental illness. Neuropsychiatric Disease and Treatment. 2023; 19:1369-78. [DOI:10.2147/NDT.S409882] [PMID]
- Fang S, Mushtaque I. The moderating role of health literacy and health promoting behavior in the relationship among health anxiety, emotional regulation, and Cyberchondria. Psychology Research and Behavior Management. 2024: 17:51-62. [DOI:10.2147/PRBM.S446448] [PMID]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2025/05/11 | Accepted: 2025/07/14 | Published: 2026/03/1
Received: 2025/05/11 | Accepted: 2025/07/14 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
