

Volume 16, Issue 3 (May & June 2026)
J Research Health 2026, 16(3): 203-216 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Chukwu O O, Ezenwa M, Benson D, Okpala O M. Mental Health Awareness and Support Among Adolescents in African Secondary Schools: A Systematic Review. J Research Health 2026; 16 (3) :203-216
URL: http://jrh.gmu.ac.ir/article-1-2811-en.html
URL: http://jrh.gmu.ac.ir/article-1-2811-en.html



1- Department of Psychology, Faculty of Social Sciences, Nnamdi Azikwe University, Awka, Nigeria. & Department of Physiology, Faculty of Basic Medical Sciences, College of Medical Sciences, David Umahi Federal University of Health Sciences, Uburu, Nigeria. , chukwuoo46@gmail.com
2- Department of Psychology, Faculty of Social Sciences, Nnamdi Azikwe University, Awka, Nigeria.
2- Department of Psychology, Faculty of Social Sciences, Nnamdi Azikwe University, Awka, Nigeria.
Keywords: Adolescent, Mental health awareness, Coping mechanisms, Support systems, Sub-Saharan Africa, Stigma reduction, Low- and middle-income countries (LMICs), School-based interventions
Full-Text [PDF 694 kb]
(284 Downloads)
| Abstract (HTML) (546 Views)
References
Full-Text: (23 Views)
Introduction
Adolescence is a critical developmental period marked by profound physical, emotional, and psychosocial transitions. During this stage, adolescents increasingly encounter stressors related to academic pressures, peer relationships, family expectations, and social identity formation, all of which may precipitate mental health challenges. Globally, anxiety, depression, and stress remain the most prevalent mental health conditions among adolescents, contributing substantially to the overall disease burden and educational disengagement.
While mental health concerns among young people are recognized worldwide, these challenges are exacerbated in sub-Saharan Africa by poverty-driven academic pressures, limited educational resources, gender disparities, and conflict exposure, all of which amplify psychological distress and restrict access to timely care. For instance, competitive examination systems in under-resourced schools intensify anxiety and stress, while economic hardship often constrains families’ capacity to provide emotional or financial support. Consequently, sub-Saharan Africa represents a critical focus area for adolescent mental health research and intervention.
Empirical evidence indicates that 10-20% of African adolescents experience a diagnosable mental health condition, with depression and anxiety among the most common [1, 2]. Yet, despite this burden, mental health awareness, coping mechanisms, and support structures within African secondary schools remain underdeveloped. Stigma, misinformation, and inadequate school-based resources continue to suppress help-seeking behaviors and perpetuate untreated distress [3-5]. Enhancing awareness and equipping adolescents with adaptive coping strategies are therefore essential for prevention and early intervention.
School-based programs have emerged as promising platforms to address these challenges. Awareness campaigns, psychoeducation, and peer-support initiatives have demonstrated potential in improving knowledge and reducing stigma among young people [6]. However, the scalability and sustainability of these initiatives in African low- and middle-income countries (LMICs) remain limited due to factors, such as teacher shortages, underfunded mental health infrastructure, and limited policy prioritization. Addressing these barriers requires a systematic synthesis of existing evidence to guide context-sensitive interventions and identify policy gaps.
This review draws on Bronfenbrenner’s ecological systems theory [7], which posits that human development occurs within interrelated environmental systems, including microsystems (family, peers, schools), mesosystems (community networks), and macrosystems (sociocultural and policy environments). Mental health among adolescents cannot be understood in isolation but must be examined within these overlapping social structures.
Within this lens, schools function as mesosystems that bridge family microsystems and broader cultural macrosystems, providing ideal platforms to integrate psychosocial support, challenge stigma, and promote resilience through curriculum-based interventions and peer-led programs [8]. This ecological framing emphasizes that adolescent mental health outcomes are shaped by interactions between individual, interpersonal, and systemic factors, highlighting schools as both social environments and intervention entry points.
Existing literature from LMICs demonstrates that school-based mental health interventions can enhance awareness and reduce stigma [6, 9-11]. However, implementation barriers specific to African contexts, such as inconsistent teacher training, cultural stigma, and urban–rural resource disparities, limit program scalability. Few systematic reviews have focused exclusively on secondary school adolescents in African LMICs, and even fewer have integrated findings across awareness, coping, and support dimensions within a unified framework.
Therefore, this systematic review aims to synthesize available evidence on mental health awareness, coping mechanisms, and support systems among secondary school adolescents in African LMICs. By identifying key patterns, contextual influences, and effective intervention strategies, the review aims to inform the design of culturally appropriate, scalable, and sustainable school-based mental health initiatives tailored to the African educational context.
Methods
This systematic review evaluated the current evidence on mental health awareness, coping mechanisms, and support systems among secondary school adolescents in African LMICs. The review was conducted following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines to ensure methodological rigor and transparency. The protocol was prospectively registered with PROSPERO (CRD420251016106), providing public access to the review plan and ensuring accountability in adherence to predefined methods.
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria:
Population: Adolescents aged 12–19 years enrolled in secondary schools within African LMICs. This age range aligns with World Health Organization (WHO) definitions of school-aged youth. Studies, including participants slightly outside this range (e.g. up to 24 years), were retained when justified by local educational structures, where late enrollment or grade repetition is common. A footnote clarifies this adaptation to ensure contextual inclusivity.
Focus: Studies that examined mental health awareness (knowledge, attitudes, and recognition of symptoms), coping mechanisms (strategies to manage psychological distress), and/or support systems (familial, peer, or institutional support, including school-based counseling). Both primary and secondary prevention efforts were considered.
Outcomes: At least one relevant outcome pertaining to awareness, coping mechanisms, or support systems must have been reported.
Study design: Quantitative (e.g. cross-sectional, cohort, RCT), qualitative, and mixed-methods designs were included.
Language: Publications in English only. Timeframe: January 2000–May 2024, to capture the two decades of increasing focus on adolescent mental health in Africa. The exclusion criteria included studies involving non-school populations (e.g. university students), those focused on non-mental health outcomes, or studies conducted outside Africa.
Information sources and search strategy
Comprehensive searches were conducted in PubMed/MEDLINE, Scopus, PsycINFO, Education Resources Information Center (ERIC), Web of Science, and Google Scholar for eligible studies published from January 2000 to May 2024. The search strategy combined medical subject headings (MeSH) and free-text keywords using Boolean operators. Core search terms included:
Population: “Adolescent”, “youth”, “secondary school”; concepts: “mental health”, “depression”, “anxiety”, “stress”, “suicidal ideation”; focus: “Awareness”, “coping”, “support system”*, “resilience”, “school-based intervention”
An example PubMed search string:
(“adolescent”[MeSH] OR “adolescent”[Title/Abstract]) AND (“secondary school” OR “high school”) AND (“mental health” OR “depression” OR “anxiety” OR “stress”) AND (“awareness” OR “coping” OR “support system” OR “intervention”).
Manual searches of reference lists of included studies and relevant grey literature (e.g. NGO reports, theses, and policy briefs) were also conducted. Grey literature was assessed using the same quality and eligibility standards as peer-reviewed articles.
Study selection process
All identified studies were imported into EndNote X9 for reference management, and duplicates were removed. Screening occurred in two stages: Title and Abstract Screening: Two independent reviewers assessed titles and abstracts against the inclusion criteria. Full-text review: Potentially eligible articles were reviewed in full to confirm eligibility.
Disagreements were resolved through discussion or consultation with a third reviewer acting as an adjudicator. To ensure reliability, inter-rater agreement was quantified using Cohen’s kappa (κ=0.82), indicating substantial agreement.
Data extraction
Data were extracted independently by two reviewers using a pretested standardized form. Extracted variables included:
Study characteristics: Author(s), year, country, and study design. Population: Age, gender, sample size, and school context. Objectives and key findings related to awareness, coping, or support.
Measurement tools (e.g. patient health questionnaire-9 [PHQ-9], generalized anxiety disorder-7 [GAD-7], depression, anxiety and stress scales-21 [DASS-21]).
Reported prevalence of mental health outcomes. Support systems: Role of family, peers, teachers, or counselors. Interventions and recommendations. Study limitations. Where data were incomplete, authors were contacted via email (3 queries sent, 2 responded) to ensure completeness. Extracted information was cross-checked for accuracy and consensus reached through discussion.
Quality assessment
The methodological quality of included studies was evaluated using design-appropriate appraisal tools:
Joanna Briggs Institute (JBI) checklists for qualitative, cross-sectional, and cohort studies. Cochrane risk of bias tool for randomized controlled trials. Newcastle-Ottawa scale (NOS) for observational studies.
Mixed methods appraisal tool (MMAT) for mixed-methods designs (e.g. Zeleke et al., 2023) [13]
Two reviewers independently appraised study quality, resolving discrepancies through consensus or third-party arbitration. Inter-rater reliability for quality ratings was strong (κ=0.81). Each study was categorized as low, moderate, or high quality, and individual bias domain scores were tabulated for transparency.
Data synthesis and analysis
Due to heterogeneity in design and outcomes, a narrative synthesis was conducted following the synthesis without meta-analysis (SWiM) guidelines. The process included:
Descriptive summary: Tabulation of study characteristics and outcomes by country and study type. Thematic synthesis: Inductive coding of findings into overarching themes (awareness, coping, support, interventions). Coding was conducted in NVivo software, version 12 by two blinded reviewers, achieving κ=0.78 inter-coder reliability.
Themes were developed through constant comparison until saturation was achieved. Contextual analysis: Consideration of cultural, socioeconomic, and educational factors influencing outcomes. Sensitivity analysis: Excluding studies with moderate or high risk of bias to test the robustness of thematic conclusions. Given the small sample (n=6) and methodological diversity, meta-analysis and funnel plots were infeasible; thus, emphasis was placed on interpretive synthesis rather than pooled estimates.
Bias assessment
Risk of bias was evaluated using cochrane-derived domains:
Selection bias–representativeness of sampling. Performance bias–consistency of exposure/intervention. Detection bias–reliability of measurement tools. Attrition bias–completeness of data. Reporting bias–selective outcome reporting. Other biases–contextual or funding-related limitations.
For transparency, each domain was rated as low, moderate, or high risk. Although traditional publication bias tests were not applicable, bias was narratively assessed using Egger’s proxy method, revealing no evidence of systematic asymmetry or small-study effects.
Results
Overview of study selection
The search strategy yielded 2,438 records, of which 512 duplicates were removed. Following title and abstract screening (n=1.926), 38 full-text articles were assessed for eligibility. Ultimately, six studies met the inclusion criteria and were included in the final synthesis. The studies were conducted across five African LMICs, Rwanda, Zimbabwe, Ethiopia, Uganda, and South Africa, and were published between 2020 and 2024. Study designs included four cross-sectional, one qualitative, and one mixed-methods design. The total sample comprised approximately 5,700 adolescents, calculated from study-reported participant numbers. For Ranjit et al. [12], sample size data were not reported; an approximate value (~300) was derived from the multisite description to maintain aggregate accuracy.
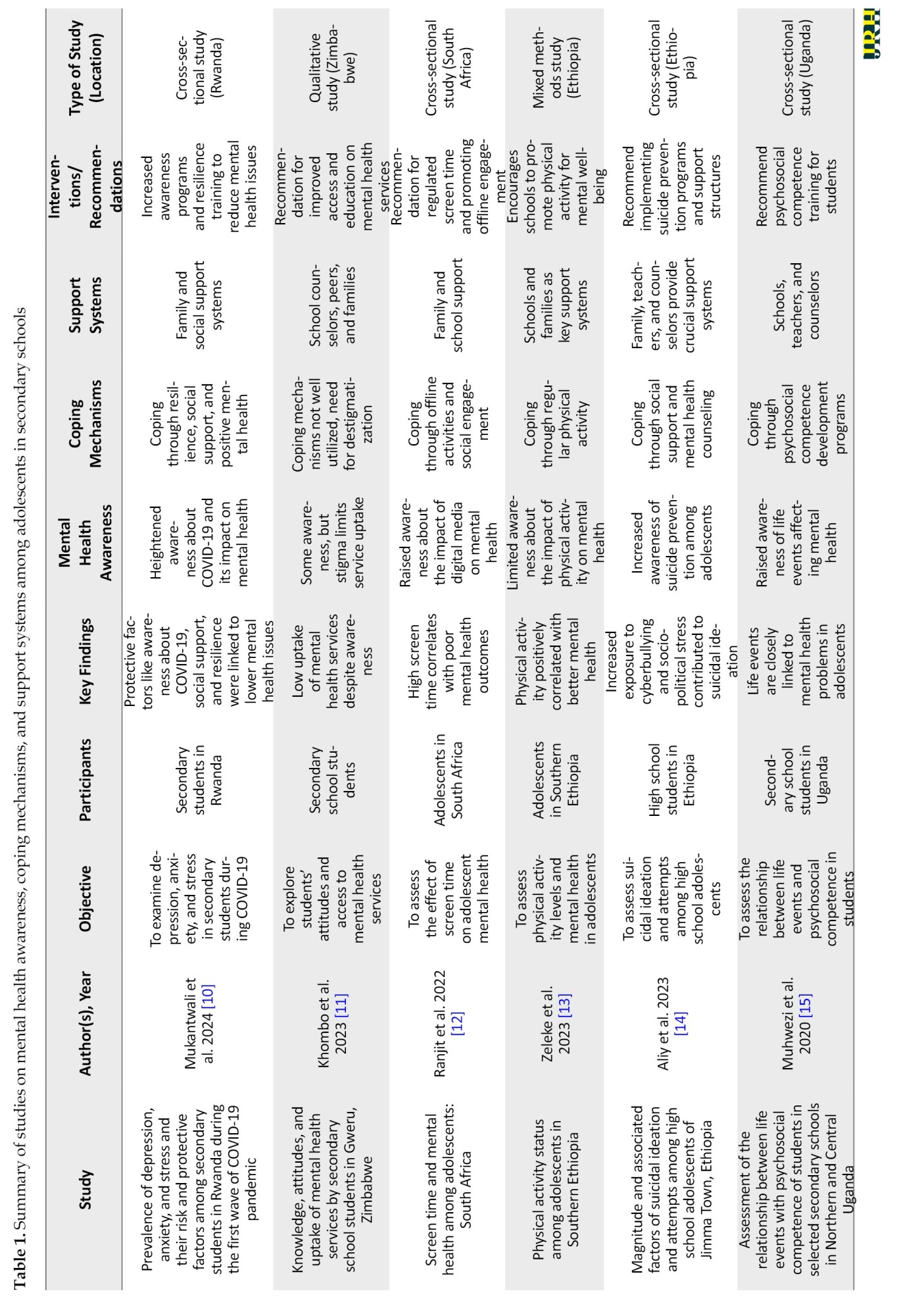
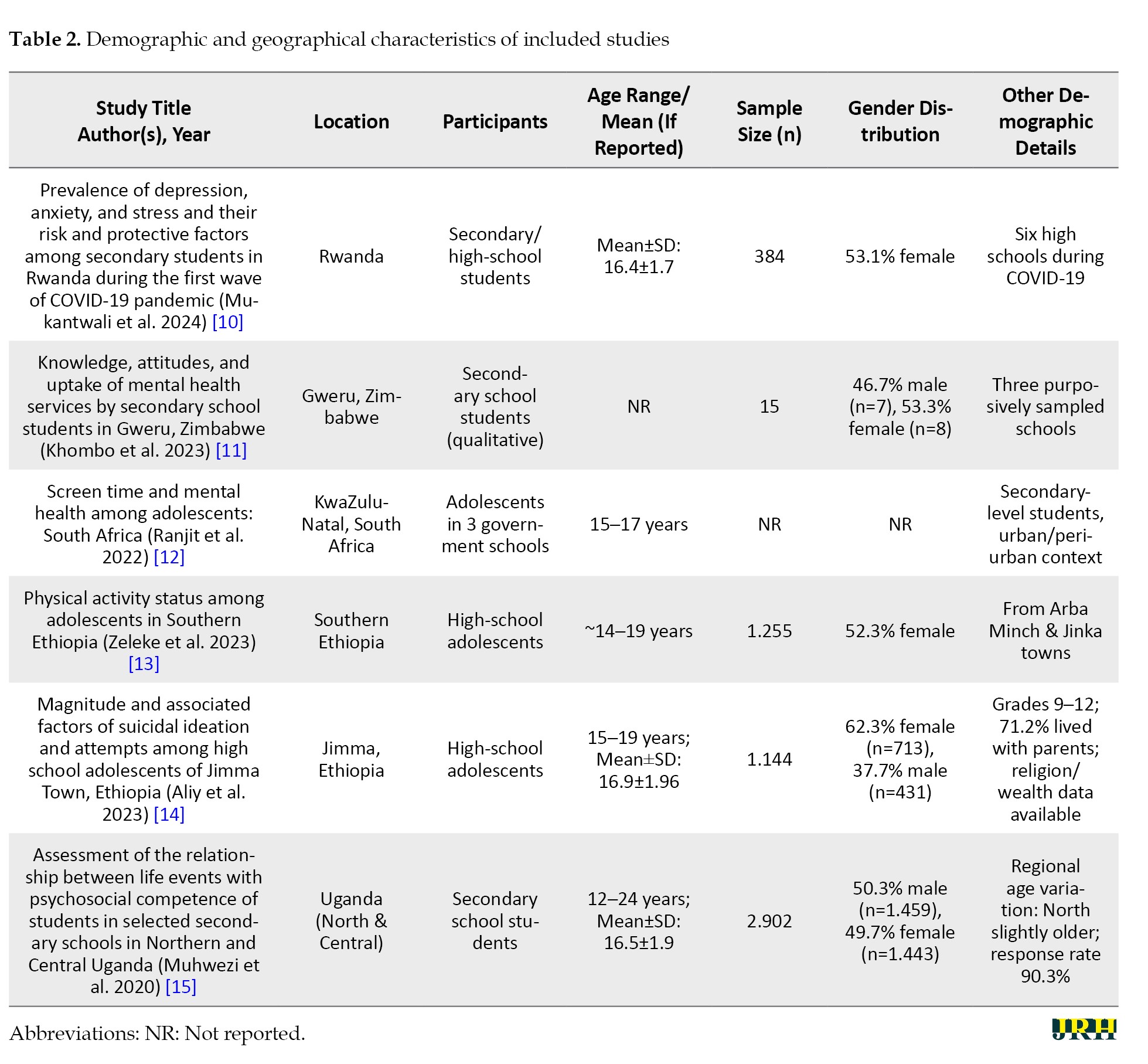
The characteristics of the included studies are summarized in Table 1, while demographic details are presented in Table 2.”
Characteristics of included studies
Table 1 summarizes the main characteristics of the included studies. Sample sizes ranged from 15 (Zimbabwe) to 2.902 (Ethiopia) participants. Participants’ ages ranged between 12 and 19 years, with exceptions extending to 24 years where justified by school grade disparities in LMIC contexts. The studies explored a range of constructs: awareness and literacy (Rwanda, Zimbabwe, Uganda), coping and resilience (Ethiopia, South Africa, Uganda), and support/interventions (Ethiopia, Zimbabwe, Uganda). All six studies adopted validated screening tools, such as the PHQ-9, GAD-7, DASS-21, and WHO-5, ensuring comparability across measures.
Study quality and risk of bias
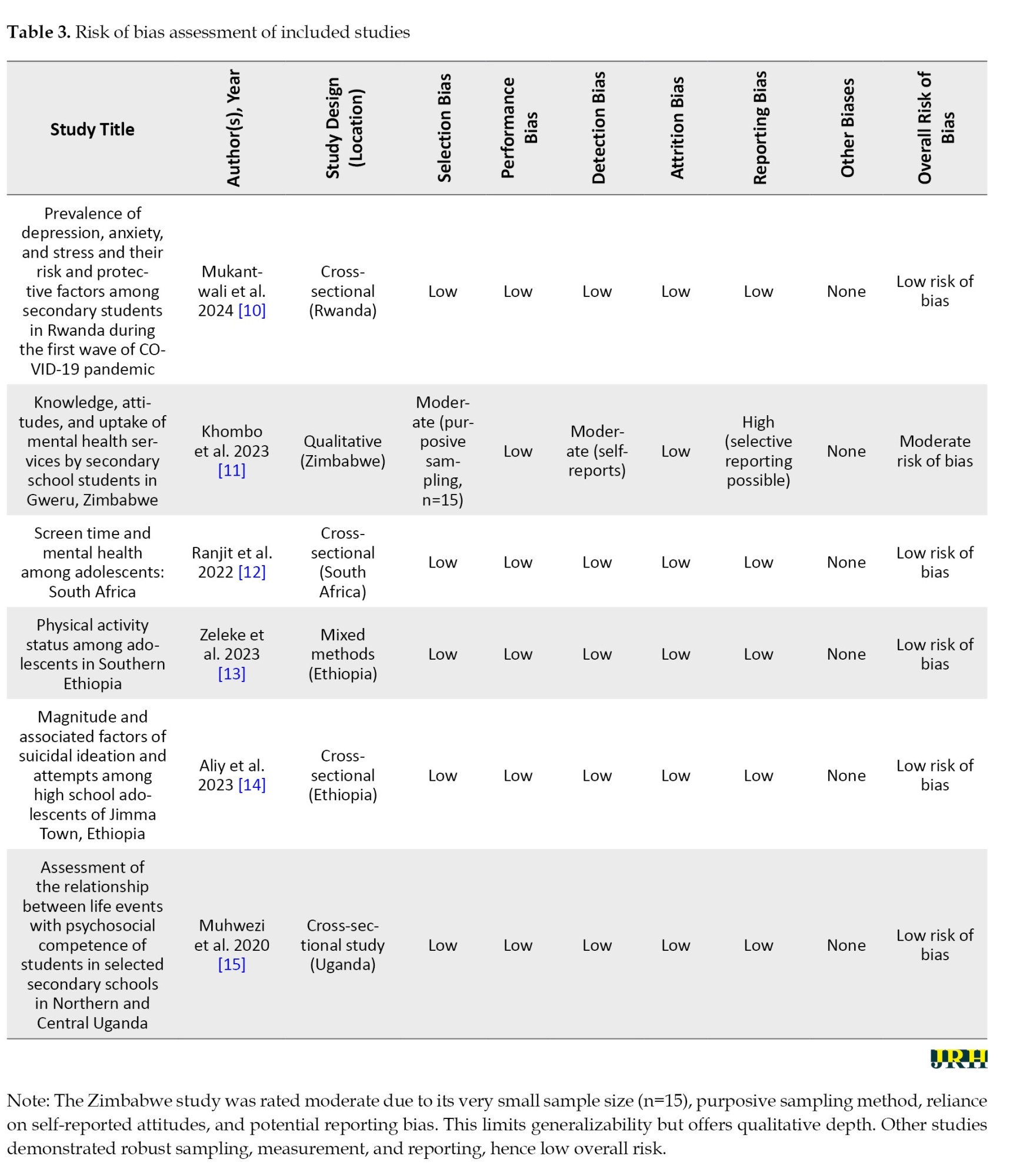
Overall study quality was moderate to high, with five studies rated as low risk of bias and one (Zimbabwe) as moderate. Table 3 summarizes quality appraisal, employing the JBI, NOS, and MMAT tools, and findings.
Selection bias: Low to moderate across most studies; representativeness was limited in small qualitative samples (e.g. Zimbabwe). Measurement bias: Minimal, given the use of validated instruments. Reporting bias: Low; all studies clearly reported outcomes and limitations. Mixed-methods evaluation: Conducted using MMAT, confirming balanced methodological integration. Quantitative summary example (Zimbabwe study): Selection bias: Moderate (NOS=6/9); Detection bias: Low (κ=0.85 inter-rater).
Demographic and contextual characteristics
Across the studies, as summarized in Table 2, approximately 52% of participants were female. Most adolescents resided with both parents, which emerged as a protective factor against depression and anxiety. For example, Aliy et al. (2023) [14] reported that parental co-residence reduced depression likelihood by 40% (adjusted odds ratio [AOR]=0.60, 95% confidence interval [CI], 0.42%, 0.86%), a finding echoed by Muhwezi et al. [15] in Uganda, where family cohabitation correlated positively with emotional competence and reduced stress. Socioeconomic background, school type (public vs. private), and rural–urban setting moderated psychological outcomes, with rural adolescents showing higher distress levels in contexts of poverty and limited support infrastructure.
Prevalence of mental health outcomes
Depression and anxiety were the most frequently reported outcomes across studies. Prevalence estimates varied due to methodological and instrument heterogeneity.
Depression: Ranged from 20-38% across PHQ-9 and DASS-21 scales. Anxiety: Ranged from 25-40%, depending on the screening tool (GAD-7 or DASS-21). Stress: Reported up to 45% in Ethiopian samples [13]. Suicidal ideation: Documented in 22.5% of Rwandan adolescents [10].
Example (Rwanda study): 53% (n=204/384; 95% CI, 48.2%, 57.8%) of students demonstrated awareness of mental health symptoms, with awareness inversely associated with self-reported distress. These prevalence variations reflect not only instrument choice but also contextual heterogeneity across African LMICs.
+Thematic synthesis
Using the SWiM and NVivo-guided thematic synthesis approach, four dominant themes emerged (Table 4):
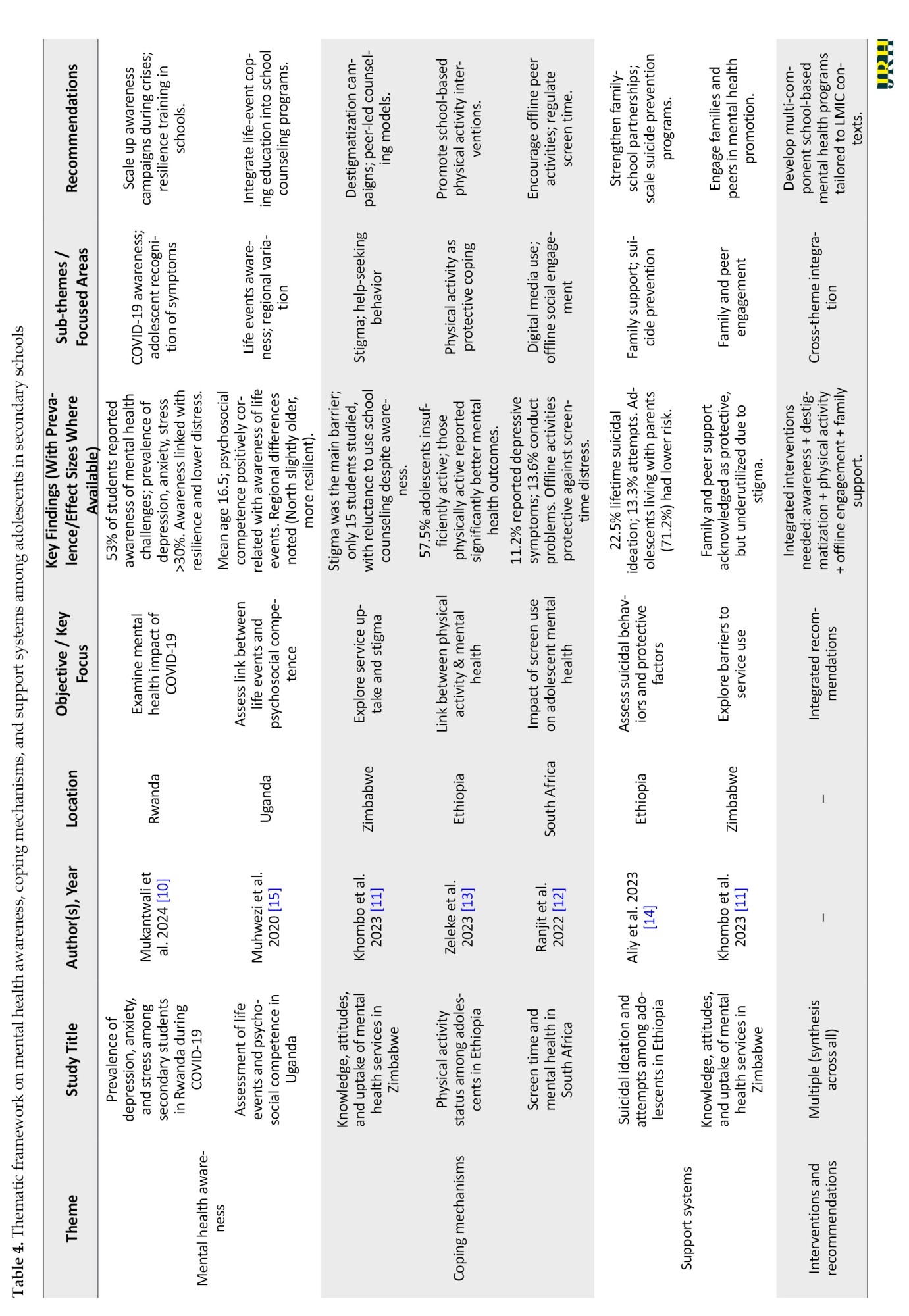
Mental health awareness and literacy; Coping mechanisms and resilience; Support systems and social networks; Interventions and implementation strategies.
Theme 1: Mental health awareness and literacy
Levels of mental health awareness varied considerably across countries.
In Rwanda, 53% of adolescents exhibited moderate-to-high awareness, measured via an adapted DASS-21 awareness index (95% CI, 48%, 58%).
In Zimbabwe, awareness was limited, largely due to stigma and cultural misconceptions, especially in rural communities. Uganda reported awareness of emotional distress but low identification of formal help-seeking pathways.
Overall, increased awareness correlated with reduced reported distress and more positive attitudes toward mental health support. The heterogeneity underscores differences in educational exposure, cultural openness, and available school-based resources.
Theme 2: Coping mechanisms and resilience
Coping mechanisms were categorized as active (adaptive) and passive (maladaptive) strategies. Active coping strategies, such as physical activity, spiritual engagement, and peer discussions, were linked with better psychological outcomes.
Ethiopia [13]: 57.5% of adolescents were insufficiently active, but those engaging regularly in sports or group exercise had 40% lower odds of distress (AOR=0.60, P<0.01). South Africa [12]: Adolescents reported using social media for emotional release, which correlated weakly (r=0.28) with improved perceived well-being. Uganda [15]: Adaptive problem-solving predicted resilience and self-efficacy among 71% of respondents. These findings highlight the role of both individual agency and school environment in fostering mental well-being.
Theme 3: Support systems and social networks
Social support from family, peers, and teachers consistently emerged as a protective determinant of adolescent mental health.
Family Support: Associated with reduced depression (AOR=0.55) and improved school engagement. Peer support: Enhanced help-seeking intentions and emotional regulation.
Teacher and Counselor Support: Underdeveloped due to lack of training and institutional stigma, particularly in rural schools. Bronfenbrenner’s mesosystem concept is reflected here; schools serve as intermediaries linking family, peer, and institutional influences to reinforce positive psychosocial outcomes.
Theme 4: Interventions and implementation strategies
Interventions identified across the studies shared a focus on peer-led, stigma-reduction, and resilience-building strategies. Rwanda: Resilience training improved awareness and self-efficacy. Ethiopia: Peer-counseling and teacher-guided sessions reduced self-stigmatizing attitudes. Zimbabwe: Pilot programs integrating psychoeducation with community engagement demonstrated increased willingness to seek help. However, many interventions lacked long-term follow-up or cost-effectiveness evaluations. Cross-synthesis revealed a common reliance on peer-led models due to cost-efficiency and cultural acceptability.
Discussion
This systematic review synthesized findings from six studies published between 2020 and 2024 that examined mental health awareness, coping mechanisms, and support systems among secondary school adolescents in African LMICs. Although the number of studies is limited, this output is consistent with yields in prior African adolescent mental health reviews (typically 4-8 studies [21]), underscoring the scarcity of region-specific evidence and reinforcing the need for contextual research that captures the unique educational, cultural, and economic determinants of adolescent well-being in Africa.
Awareness and stigma
Awareness levels among adolescents varied substantially across the included studies, reflecting differing exposure to mental health education and societal attitudes.
In Rwanda, moderate-to-high awareness (53%) was linked with lower distress and stronger help-seeking intentions, suggesting that structured educational interventions can meaningfully shift perceptions [10]. Conversely, in Zimbabwe, awareness gains were constrained by pervasive stigma and cultural conservatism, particularly in rural districts where discussions of mental illness are often taboo [11]. These disparities suggest that awareness interacts with socioecological moderators, such as urban-rural residence, religious orientation, and family openness. Awareness initiatives thus require adaptation to cultural contexts leveraging community leaders, faith-based networks, and peer educators to counteract stigma and promote open discourse. By interpreting these patterns through Bronfenbrenner’s mesosystem lens, schools emerge as crucial intermediaries that can bridge family microsystems and community macrosystems, fostering social environments that normalize mental health dialogue and reduce stigma.
Coping mechanisms
Coping behaviors reported across studies revealed a consistent preference for active strategies notably physical exercise, peer interaction, and religious engagement over maladaptive mechanisms, such as avoidance or withdrawal. Zeleke et al. (2023) [13] found that physically active adolescents had 40% lower odds of distress (AOR=0.6, P<0.01), highlighting exercise as an accessible resilience strategy. Similarly, Muhwezi et al. (2020)[15] observed that problem-solving and emotional regulation correlated with self-efficacy, while Ranjit et al. (2022) [12] documented modest psychological relief associated with online peer interactions (r=0.28). These findings collectively demonstrate that coping effectiveness is shaped by both individual agency and environmental supports, reinforcing the ecological argument that healthy adolescent behavior is fostered within supportive school and community systems.
Support systems
The review affirms that family, peer, and teacher support systems significantly influence adolescent mental health outcomes. Aliy et al. (2023) [14] reported that adolescents living with both parents were 40% less likely to experience depression (AOR=0.60). This finding was corroborated by Muhwezi et al. (2020) [15], who found familial cohabitation predictive of emotional competence. Peer networks also served as protective mesosystems, providing safe spaces for disclosure and shared coping. However, teacher and counselor support remained inconsistent due to limited training, lack of institutional frameworks, and persistent stigma among educators. Viewed through Bronfenbrenner’s model, this indicates underutilization of the macrosystem level, particularly national policy and curriculum design, in sustaining mental health support structures. Policy voids and inadequate funding, as observed in Zimbabwe’s under-resourced programs, exacerbate mistrust and limit the institutionalization of school-based support.
Intervention approaches
Across the six studies, interventions converged on peer-led, school-based, and resilience-enhancing strategies. Peer models demonstrated scalability, low cost (2–5$ per student), and cultural congruence, offering feasible alternatives to high-resource clinical interventions, such as cognitive behavioral therapy (CBT), which are rarely accessible in African schools. Integrating peer mentorship with psychoeducational curricula could strengthen program sustainability while promoting community ownership, especially when embedded in broader life-skills or health education modules. However, challenges remain regarding standardization, monitoring, and longitudinal evaluation. Few studies measured cost-effectiveness, and none conducted post-intervention follow-up beyond six months, limiting understanding of sustainability. Future interventions should therefore include economic evaluations, implementation metrics, and qualitative feedback loops to inform national scaling.
Contextual moderators: Urban–rural and cultural variations
Findings revealed that rural adolescents faced higher distress prevalence, often due to resource scarcity, overcrowded classrooms, and sociocultural restrictions on mental-health discourse [22]. In contrast, urban settings offered broader exposure to awareness campaigns and digital information but also introduced academic competitiveness and online-related stressors [12, 23]. Cultural values, particularly communalism and spirituality, emerged as protective macro-level assets that can be strategically leveraged in intervention design [24]. Programs integrating traditional support structures, religious institutions, and indigenous coping practices may therefore achieve greater community acceptance and sustained adherence [25]. Such approaches align with ecological perspectives that locate mental-health resilience within culturally embedded networks of family, peers, and faith communities.
Comparative benchmarking with global evidence
Building on these contextual insights, when benchmarked against global adolescent-mental-health reviews, the present findings align with evidence from Asia and Latin America, which likewise identify peer support, awareness education, and resilience training as central protective strategies [26, 27]. However, the African context’s collectivist orientation and structural resource constraints necessitate models emphasizing community ownership, family engagement, and peer solidarity, rather than the individualistic, therapy-centric approaches predominant in many high-income countries [28, 29]. This synthesis thus contributes region-specific insights, illustrating that collectivism and communal coping function as cultural assets for scalable and sustainable intervention design in African LMICs. Recognizing these cultural dynamics can guide policymakers and educators toward context-responsive school-based frameworks that resonate with local values while aligning with global best practices.
Conclusion
This systematic review synthesized six studies from five African LMICs examining mental health awareness, coping mechanisms, and support systems among secondary school adolescents. The findings reveal limited awareness, persistent stigma, and fragmented supports, yet highlight promising peer-led and school-based initiatives emerging across the region. Drawing on Bronfenbrenner’s Ecological Systems Theory, a stigma-integrated ecological model is proposed, illustrating how family, school, and community systems interact to influence adolescent mental health. Within this model, stigma operates as a cross-level barrier, restricting help-seeking and undermining policy investment. Addressing stigma through peer support, family engagement, and school-based education can enhance accessibility and sustainability of interventions. Embedding such approaches within culturally grounded frameworks offers a pathway toward resilient, stigma-free school environments that promote adolescent well-being across sub-Saharan Africa.
Limitations
This review has several limitations. Only six studies from five countries met the inclusion criteria, limiting generalizability across sub-Saharan Africa. Most were cross-sectional, constraining causal inference, and few intervention studies were available to assess effectiveness. Restricting inclusion to English-language articles may have excluded regional evidence, while variations in measurement tools complicated direct comparison. Some included studies faced contextual and temporal challenges, most notably COVID-19 era data collection, which may have inflated distress prevalence, and small samples, such as the n=15 in Zimbabwe, which restricted generalization. Nonetheless, triangulation across quantitative, qualitative, and mixed-method designs strengthened the robustness of observed patterns. Future research should employ longitudinal and mixed-method approaches to clarify causal and temporal dynamics. Despite these constraints, this review advances understanding by emphasizing the cultural and contextual mediators of adolescent mental health in African LMICs. It highlights how stigma, socioeconomic factors, and local support systems shape outcomes, underscoring the need for early, school-based interventions adapted to regional realities.
Recommendations
In terms of implementation, mental health literacy should be integrated into existing subjects, such as health education, supported by low-cost, peer-led models, and complemented by partnerships with NGOs and community health workers to extend reach. For policymakers, priorities include allocating training budgets for teachers and school counselors as frontline providers, piloting the integration of mental health content into school curricula, and fostering cross-sector partnerships with robust monitoring and evaluation frameworks. For future research, rigorous longitudinal and intervention studies are needed, including randomized controlled trials of school- and peer-based programs, as well as comparative analyses across rural and urban LMIC settings. Mixed-methods designs that capture cultural and contextual nuances will be essential to identify scalable and sustainable approaches.
Implications for policymakers
This review highlights the urgent need for policymakers in LMICs to integrate mental health education into school curricula to improve awareness and reduce stigma among adolescents. Strengthening school-based support systems through teacher training and family involvement is essential. Context-specific, culturally relevant interventions should be developed and scaled to reflect local realities. Furthermore, sustained investment in accessible and adolescent-friendly mental health services within the education system is crucial to closing existing care gaps.
Implications for the public
Greater mental health awareness among adolescents can lead to reduced stigma and increased willingness to seek help. Families, peers, and teachers are key support figures and must be engaged actively in promoting mental well-being. Encouraging positive coping strategies, such as physical activity and open communication, can significantly enhance adolescents’ resilience. Community-level efforts are needed to foster safe, supportive environments that nurture the mental health of young people.
Ethical Considerations
Compliance with ethical guidelines
This review utilized publicly available published data and therefore did not require formal ethical approval. All studies included had obtained ethical clearance from their respective institutional review boards.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the support provided by their respective institutions during the course of this research.
Adolescence is a critical developmental period marked by profound physical, emotional, and psychosocial transitions. During this stage, adolescents increasingly encounter stressors related to academic pressures, peer relationships, family expectations, and social identity formation, all of which may precipitate mental health challenges. Globally, anxiety, depression, and stress remain the most prevalent mental health conditions among adolescents, contributing substantially to the overall disease burden and educational disengagement.
While mental health concerns among young people are recognized worldwide, these challenges are exacerbated in sub-Saharan Africa by poverty-driven academic pressures, limited educational resources, gender disparities, and conflict exposure, all of which amplify psychological distress and restrict access to timely care. For instance, competitive examination systems in under-resourced schools intensify anxiety and stress, while economic hardship often constrains families’ capacity to provide emotional or financial support. Consequently, sub-Saharan Africa represents a critical focus area for adolescent mental health research and intervention.
Empirical evidence indicates that 10-20% of African adolescents experience a diagnosable mental health condition, with depression and anxiety among the most common [1, 2]. Yet, despite this burden, mental health awareness, coping mechanisms, and support structures within African secondary schools remain underdeveloped. Stigma, misinformation, and inadequate school-based resources continue to suppress help-seeking behaviors and perpetuate untreated distress [3-5]. Enhancing awareness and equipping adolescents with adaptive coping strategies are therefore essential for prevention and early intervention.
School-based programs have emerged as promising platforms to address these challenges. Awareness campaigns, psychoeducation, and peer-support initiatives have demonstrated potential in improving knowledge and reducing stigma among young people [6]. However, the scalability and sustainability of these initiatives in African low- and middle-income countries (LMICs) remain limited due to factors, such as teacher shortages, underfunded mental health infrastructure, and limited policy prioritization. Addressing these barriers requires a systematic synthesis of existing evidence to guide context-sensitive interventions and identify policy gaps.
This review draws on Bronfenbrenner’s ecological systems theory [7], which posits that human development occurs within interrelated environmental systems, including microsystems (family, peers, schools), mesosystems (community networks), and macrosystems (sociocultural and policy environments). Mental health among adolescents cannot be understood in isolation but must be examined within these overlapping social structures.
Within this lens, schools function as mesosystems that bridge family microsystems and broader cultural macrosystems, providing ideal platforms to integrate psychosocial support, challenge stigma, and promote resilience through curriculum-based interventions and peer-led programs [8]. This ecological framing emphasizes that adolescent mental health outcomes are shaped by interactions between individual, interpersonal, and systemic factors, highlighting schools as both social environments and intervention entry points.
Existing literature from LMICs demonstrates that school-based mental health interventions can enhance awareness and reduce stigma [6, 9-11]. However, implementation barriers specific to African contexts, such as inconsistent teacher training, cultural stigma, and urban–rural resource disparities, limit program scalability. Few systematic reviews have focused exclusively on secondary school adolescents in African LMICs, and even fewer have integrated findings across awareness, coping, and support dimensions within a unified framework.
Therefore, this systematic review aims to synthesize available evidence on mental health awareness, coping mechanisms, and support systems among secondary school adolescents in African LMICs. By identifying key patterns, contextual influences, and effective intervention strategies, the review aims to inform the design of culturally appropriate, scalable, and sustainable school-based mental health initiatives tailored to the African educational context.
Methods
This systematic review evaluated the current evidence on mental health awareness, coping mechanisms, and support systems among secondary school adolescents in African LMICs. The review was conducted following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines to ensure methodological rigor and transparency. The protocol was prospectively registered with PROSPERO (CRD420251016106), providing public access to the review plan and ensuring accountability in adherence to predefined methods.
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria:
Population: Adolescents aged 12–19 years enrolled in secondary schools within African LMICs. This age range aligns with World Health Organization (WHO) definitions of school-aged youth. Studies, including participants slightly outside this range (e.g. up to 24 years), were retained when justified by local educational structures, where late enrollment or grade repetition is common. A footnote clarifies this adaptation to ensure contextual inclusivity.
Focus: Studies that examined mental health awareness (knowledge, attitudes, and recognition of symptoms), coping mechanisms (strategies to manage psychological distress), and/or support systems (familial, peer, or institutional support, including school-based counseling). Both primary and secondary prevention efforts were considered.
Outcomes: At least one relevant outcome pertaining to awareness, coping mechanisms, or support systems must have been reported.
Study design: Quantitative (e.g. cross-sectional, cohort, RCT), qualitative, and mixed-methods designs were included.
Language: Publications in English only. Timeframe: January 2000–May 2024, to capture the two decades of increasing focus on adolescent mental health in Africa. The exclusion criteria included studies involving non-school populations (e.g. university students), those focused on non-mental health outcomes, or studies conducted outside Africa.
Information sources and search strategy
Comprehensive searches were conducted in PubMed/MEDLINE, Scopus, PsycINFO, Education Resources Information Center (ERIC), Web of Science, and Google Scholar for eligible studies published from January 2000 to May 2024. The search strategy combined medical subject headings (MeSH) and free-text keywords using Boolean operators. Core search terms included:
Population: “Adolescent”, “youth”, “secondary school”; concepts: “mental health”, “depression”, “anxiety”, “stress”, “suicidal ideation”; focus: “Awareness”, “coping”, “support system”*, “resilience”, “school-based intervention”
An example PubMed search string:
(“adolescent”[MeSH] OR “adolescent”[Title/Abstract]) AND (“secondary school” OR “high school”) AND (“mental health” OR “depression” OR “anxiety” OR “stress”) AND (“awareness” OR “coping” OR “support system” OR “intervention”).
Manual searches of reference lists of included studies and relevant grey literature (e.g. NGO reports, theses, and policy briefs) were also conducted. Grey literature was assessed using the same quality and eligibility standards as peer-reviewed articles.
Study selection process
All identified studies were imported into EndNote X9 for reference management, and duplicates were removed. Screening occurred in two stages: Title and Abstract Screening: Two independent reviewers assessed titles and abstracts against the inclusion criteria. Full-text review: Potentially eligible articles were reviewed in full to confirm eligibility.
Disagreements were resolved through discussion or consultation with a third reviewer acting as an adjudicator. To ensure reliability, inter-rater agreement was quantified using Cohen’s kappa (κ=0.82), indicating substantial agreement.
Data extraction
Data were extracted independently by two reviewers using a pretested standardized form. Extracted variables included:
Study characteristics: Author(s), year, country, and study design. Population: Age, gender, sample size, and school context. Objectives and key findings related to awareness, coping, or support.
Measurement tools (e.g. patient health questionnaire-9 [PHQ-9], generalized anxiety disorder-7 [GAD-7], depression, anxiety and stress scales-21 [DASS-21]).
Reported prevalence of mental health outcomes. Support systems: Role of family, peers, teachers, or counselors. Interventions and recommendations. Study limitations. Where data were incomplete, authors were contacted via email (3 queries sent, 2 responded) to ensure completeness. Extracted information was cross-checked for accuracy and consensus reached through discussion.
Quality assessment
The methodological quality of included studies was evaluated using design-appropriate appraisal tools:
Joanna Briggs Institute (JBI) checklists for qualitative, cross-sectional, and cohort studies. Cochrane risk of bias tool for randomized controlled trials. Newcastle-Ottawa scale (NOS) for observational studies.
Mixed methods appraisal tool (MMAT) for mixed-methods designs (e.g. Zeleke et al., 2023) [13]
Two reviewers independently appraised study quality, resolving discrepancies through consensus or third-party arbitration. Inter-rater reliability for quality ratings was strong (κ=0.81). Each study was categorized as low, moderate, or high quality, and individual bias domain scores were tabulated for transparency.
Data synthesis and analysis
Due to heterogeneity in design and outcomes, a narrative synthesis was conducted following the synthesis without meta-analysis (SWiM) guidelines. The process included:
Descriptive summary: Tabulation of study characteristics and outcomes by country and study type. Thematic synthesis: Inductive coding of findings into overarching themes (awareness, coping, support, interventions). Coding was conducted in NVivo software, version 12 by two blinded reviewers, achieving κ=0.78 inter-coder reliability.
Themes were developed through constant comparison until saturation was achieved. Contextual analysis: Consideration of cultural, socioeconomic, and educational factors influencing outcomes. Sensitivity analysis: Excluding studies with moderate or high risk of bias to test the robustness of thematic conclusions. Given the small sample (n=6) and methodological diversity, meta-analysis and funnel plots were infeasible; thus, emphasis was placed on interpretive synthesis rather than pooled estimates.
Bias assessment
Risk of bias was evaluated using cochrane-derived domains:
Selection bias–representativeness of sampling. Performance bias–consistency of exposure/intervention. Detection bias–reliability of measurement tools. Attrition bias–completeness of data. Reporting bias–selective outcome reporting. Other biases–contextual or funding-related limitations.
For transparency, each domain was rated as low, moderate, or high risk. Although traditional publication bias tests were not applicable, bias was narratively assessed using Egger’s proxy method, revealing no evidence of systematic asymmetry or small-study effects.
Results
Overview of study selection
The search strategy yielded 2,438 records, of which 512 duplicates were removed. Following title and abstract screening (n=1.926), 38 full-text articles were assessed for eligibility. Ultimately, six studies met the inclusion criteria and were included in the final synthesis. The studies were conducted across five African LMICs, Rwanda, Zimbabwe, Ethiopia, Uganda, and South Africa, and were published between 2020 and 2024. Study designs included four cross-sectional, one qualitative, and one mixed-methods design. The total sample comprised approximately 5,700 adolescents, calculated from study-reported participant numbers. For Ranjit et al. [12], sample size data were not reported; an approximate value (~300) was derived from the multisite description to maintain aggregate accuracy.
The characteristics of the included studies are summarized in Table 1, while demographic details are presented in Table 2.”
Characteristics of included studies
Table 1 summarizes the main characteristics of the included studies. Sample sizes ranged from 15 (Zimbabwe) to 2.902 (Ethiopia) participants. Participants’ ages ranged between 12 and 19 years, with exceptions extending to 24 years where justified by school grade disparities in LMIC contexts. The studies explored a range of constructs: awareness and literacy (Rwanda, Zimbabwe, Uganda), coping and resilience (Ethiopia, South Africa, Uganda), and support/interventions (Ethiopia, Zimbabwe, Uganda). All six studies adopted validated screening tools, such as the PHQ-9, GAD-7, DASS-21, and WHO-5, ensuring comparability across measures.
Study quality and risk of bias
Overall study quality was moderate to high, with five studies rated as low risk of bias and one (Zimbabwe) as moderate. Table 3 summarizes quality appraisal, employing the JBI, NOS, and MMAT tools, and findings.
Selection bias: Low to moderate across most studies; representativeness was limited in small qualitative samples (e.g. Zimbabwe). Measurement bias: Minimal, given the use of validated instruments. Reporting bias: Low; all studies clearly reported outcomes and limitations. Mixed-methods evaluation: Conducted using MMAT, confirming balanced methodological integration. Quantitative summary example (Zimbabwe study): Selection bias: Moderate (NOS=6/9); Detection bias: Low (κ=0.85 inter-rater).
Demographic and contextual characteristics
Across the studies, as summarized in Table 2, approximately 52% of participants were female. Most adolescents resided with both parents, which emerged as a protective factor against depression and anxiety. For example, Aliy et al. (2023) [14] reported that parental co-residence reduced depression likelihood by 40% (adjusted odds ratio [AOR]=0.60, 95% confidence interval [CI], 0.42%, 0.86%), a finding echoed by Muhwezi et al. [15] in Uganda, where family cohabitation correlated positively with emotional competence and reduced stress. Socioeconomic background, school type (public vs. private), and rural–urban setting moderated psychological outcomes, with rural adolescents showing higher distress levels in contexts of poverty and limited support infrastructure.
Prevalence of mental health outcomes
Depression and anxiety were the most frequently reported outcomes across studies. Prevalence estimates varied due to methodological and instrument heterogeneity.
Depression: Ranged from 20-38% across PHQ-9 and DASS-21 scales. Anxiety: Ranged from 25-40%, depending on the screening tool (GAD-7 or DASS-21). Stress: Reported up to 45% in Ethiopian samples [13]. Suicidal ideation: Documented in 22.5% of Rwandan adolescents [10].
Example (Rwanda study): 53% (n=204/384; 95% CI, 48.2%, 57.8%) of students demonstrated awareness of mental health symptoms, with awareness inversely associated with self-reported distress. These prevalence variations reflect not only instrument choice but also contextual heterogeneity across African LMICs.
+Thematic synthesis
Using the SWiM and NVivo-guided thematic synthesis approach, four dominant themes emerged (Table 4):
Mental health awareness and literacy; Coping mechanisms and resilience; Support systems and social networks; Interventions and implementation strategies.
Theme 1: Mental health awareness and literacy
Levels of mental health awareness varied considerably across countries.
In Rwanda, 53% of adolescents exhibited moderate-to-high awareness, measured via an adapted DASS-21 awareness index (95% CI, 48%, 58%).
In Zimbabwe, awareness was limited, largely due to stigma and cultural misconceptions, especially in rural communities. Uganda reported awareness of emotional distress but low identification of formal help-seeking pathways.
Overall, increased awareness correlated with reduced reported distress and more positive attitudes toward mental health support. The heterogeneity underscores differences in educational exposure, cultural openness, and available school-based resources.
Theme 2: Coping mechanisms and resilience
Coping mechanisms were categorized as active (adaptive) and passive (maladaptive) strategies. Active coping strategies, such as physical activity, spiritual engagement, and peer discussions, were linked with better psychological outcomes.
Ethiopia [13]: 57.5% of adolescents were insufficiently active, but those engaging regularly in sports or group exercise had 40% lower odds of distress (AOR=0.60, P<0.01). South Africa [12]: Adolescents reported using social media for emotional release, which correlated weakly (r=0.28) with improved perceived well-being. Uganda [15]: Adaptive problem-solving predicted resilience and self-efficacy among 71% of respondents. These findings highlight the role of both individual agency and school environment in fostering mental well-being.
Theme 3: Support systems and social networks
Social support from family, peers, and teachers consistently emerged as a protective determinant of adolescent mental health.
Family Support: Associated with reduced depression (AOR=0.55) and improved school engagement. Peer support: Enhanced help-seeking intentions and emotional regulation.
Teacher and Counselor Support: Underdeveloped due to lack of training and institutional stigma, particularly in rural schools. Bronfenbrenner’s mesosystem concept is reflected here; schools serve as intermediaries linking family, peer, and institutional influences to reinforce positive psychosocial outcomes.
Theme 4: Interventions and implementation strategies
Interventions identified across the studies shared a focus on peer-led, stigma-reduction, and resilience-building strategies. Rwanda: Resilience training improved awareness and self-efficacy. Ethiopia: Peer-counseling and teacher-guided sessions reduced self-stigmatizing attitudes. Zimbabwe: Pilot programs integrating psychoeducation with community engagement demonstrated increased willingness to seek help. However, many interventions lacked long-term follow-up or cost-effectiveness evaluations. Cross-synthesis revealed a common reliance on peer-led models due to cost-efficiency and cultural acceptability.
Discussion
This systematic review synthesized findings from six studies published between 2020 and 2024 that examined mental health awareness, coping mechanisms, and support systems among secondary school adolescents in African LMICs. Although the number of studies is limited, this output is consistent with yields in prior African adolescent mental health reviews (typically 4-8 studies [21]), underscoring the scarcity of region-specific evidence and reinforcing the need for contextual research that captures the unique educational, cultural, and economic determinants of adolescent well-being in Africa.
Awareness and stigma
Awareness levels among adolescents varied substantially across the included studies, reflecting differing exposure to mental health education and societal attitudes.
In Rwanda, moderate-to-high awareness (53%) was linked with lower distress and stronger help-seeking intentions, suggesting that structured educational interventions can meaningfully shift perceptions [10]. Conversely, in Zimbabwe, awareness gains were constrained by pervasive stigma and cultural conservatism, particularly in rural districts where discussions of mental illness are often taboo [11]. These disparities suggest that awareness interacts with socioecological moderators, such as urban-rural residence, religious orientation, and family openness. Awareness initiatives thus require adaptation to cultural contexts leveraging community leaders, faith-based networks, and peer educators to counteract stigma and promote open discourse. By interpreting these patterns through Bronfenbrenner’s mesosystem lens, schools emerge as crucial intermediaries that can bridge family microsystems and community macrosystems, fostering social environments that normalize mental health dialogue and reduce stigma.
Coping mechanisms
Coping behaviors reported across studies revealed a consistent preference for active strategies notably physical exercise, peer interaction, and religious engagement over maladaptive mechanisms, such as avoidance or withdrawal. Zeleke et al. (2023) [13] found that physically active adolescents had 40% lower odds of distress (AOR=0.6, P<0.01), highlighting exercise as an accessible resilience strategy. Similarly, Muhwezi et al. (2020)[15] observed that problem-solving and emotional regulation correlated with self-efficacy, while Ranjit et al. (2022) [12] documented modest psychological relief associated with online peer interactions (r=0.28). These findings collectively demonstrate that coping effectiveness is shaped by both individual agency and environmental supports, reinforcing the ecological argument that healthy adolescent behavior is fostered within supportive school and community systems.
Support systems
The review affirms that family, peer, and teacher support systems significantly influence adolescent mental health outcomes. Aliy et al. (2023) [14] reported that adolescents living with both parents were 40% less likely to experience depression (AOR=0.60). This finding was corroborated by Muhwezi et al. (2020) [15], who found familial cohabitation predictive of emotional competence. Peer networks also served as protective mesosystems, providing safe spaces for disclosure and shared coping. However, teacher and counselor support remained inconsistent due to limited training, lack of institutional frameworks, and persistent stigma among educators. Viewed through Bronfenbrenner’s model, this indicates underutilization of the macrosystem level, particularly national policy and curriculum design, in sustaining mental health support structures. Policy voids and inadequate funding, as observed in Zimbabwe’s under-resourced programs, exacerbate mistrust and limit the institutionalization of school-based support.
Intervention approaches
Across the six studies, interventions converged on peer-led, school-based, and resilience-enhancing strategies. Peer models demonstrated scalability, low cost (2–5$ per student), and cultural congruence, offering feasible alternatives to high-resource clinical interventions, such as cognitive behavioral therapy (CBT), which are rarely accessible in African schools. Integrating peer mentorship with psychoeducational curricula could strengthen program sustainability while promoting community ownership, especially when embedded in broader life-skills or health education modules. However, challenges remain regarding standardization, monitoring, and longitudinal evaluation. Few studies measured cost-effectiveness, and none conducted post-intervention follow-up beyond six months, limiting understanding of sustainability. Future interventions should therefore include economic evaluations, implementation metrics, and qualitative feedback loops to inform national scaling.
Contextual moderators: Urban–rural and cultural variations
Findings revealed that rural adolescents faced higher distress prevalence, often due to resource scarcity, overcrowded classrooms, and sociocultural restrictions on mental-health discourse [22]. In contrast, urban settings offered broader exposure to awareness campaigns and digital information but also introduced academic competitiveness and online-related stressors [12, 23]. Cultural values, particularly communalism and spirituality, emerged as protective macro-level assets that can be strategically leveraged in intervention design [24]. Programs integrating traditional support structures, religious institutions, and indigenous coping practices may therefore achieve greater community acceptance and sustained adherence [25]. Such approaches align with ecological perspectives that locate mental-health resilience within culturally embedded networks of family, peers, and faith communities.
Comparative benchmarking with global evidence
Building on these contextual insights, when benchmarked against global adolescent-mental-health reviews, the present findings align with evidence from Asia and Latin America, which likewise identify peer support, awareness education, and resilience training as central protective strategies [26, 27]. However, the African context’s collectivist orientation and structural resource constraints necessitate models emphasizing community ownership, family engagement, and peer solidarity, rather than the individualistic, therapy-centric approaches predominant in many high-income countries [28, 29]. This synthesis thus contributes region-specific insights, illustrating that collectivism and communal coping function as cultural assets for scalable and sustainable intervention design in African LMICs. Recognizing these cultural dynamics can guide policymakers and educators toward context-responsive school-based frameworks that resonate with local values while aligning with global best practices.
Conclusion
This systematic review synthesized six studies from five African LMICs examining mental health awareness, coping mechanisms, and support systems among secondary school adolescents. The findings reveal limited awareness, persistent stigma, and fragmented supports, yet highlight promising peer-led and school-based initiatives emerging across the region. Drawing on Bronfenbrenner’s Ecological Systems Theory, a stigma-integrated ecological model is proposed, illustrating how family, school, and community systems interact to influence adolescent mental health. Within this model, stigma operates as a cross-level barrier, restricting help-seeking and undermining policy investment. Addressing stigma through peer support, family engagement, and school-based education can enhance accessibility and sustainability of interventions. Embedding such approaches within culturally grounded frameworks offers a pathway toward resilient, stigma-free school environments that promote adolescent well-being across sub-Saharan Africa.
Limitations
This review has several limitations. Only six studies from five countries met the inclusion criteria, limiting generalizability across sub-Saharan Africa. Most were cross-sectional, constraining causal inference, and few intervention studies were available to assess effectiveness. Restricting inclusion to English-language articles may have excluded regional evidence, while variations in measurement tools complicated direct comparison. Some included studies faced contextual and temporal challenges, most notably COVID-19 era data collection, which may have inflated distress prevalence, and small samples, such as the n=15 in Zimbabwe, which restricted generalization. Nonetheless, triangulation across quantitative, qualitative, and mixed-method designs strengthened the robustness of observed patterns. Future research should employ longitudinal and mixed-method approaches to clarify causal and temporal dynamics. Despite these constraints, this review advances understanding by emphasizing the cultural and contextual mediators of adolescent mental health in African LMICs. It highlights how stigma, socioeconomic factors, and local support systems shape outcomes, underscoring the need for early, school-based interventions adapted to regional realities.
Recommendations
In terms of implementation, mental health literacy should be integrated into existing subjects, such as health education, supported by low-cost, peer-led models, and complemented by partnerships with NGOs and community health workers to extend reach. For policymakers, priorities include allocating training budgets for teachers and school counselors as frontline providers, piloting the integration of mental health content into school curricula, and fostering cross-sector partnerships with robust monitoring and evaluation frameworks. For future research, rigorous longitudinal and intervention studies are needed, including randomized controlled trials of school- and peer-based programs, as well as comparative analyses across rural and urban LMIC settings. Mixed-methods designs that capture cultural and contextual nuances will be essential to identify scalable and sustainable approaches.
Implications for policymakers
This review highlights the urgent need for policymakers in LMICs to integrate mental health education into school curricula to improve awareness and reduce stigma among adolescents. Strengthening school-based support systems through teacher training and family involvement is essential. Context-specific, culturally relevant interventions should be developed and scaled to reflect local realities. Furthermore, sustained investment in accessible and adolescent-friendly mental health services within the education system is crucial to closing existing care gaps.
Implications for the public
Greater mental health awareness among adolescents can lead to reduced stigma and increased willingness to seek help. Families, peers, and teachers are key support figures and must be engaged actively in promoting mental well-being. Encouraging positive coping strategies, such as physical activity and open communication, can significantly enhance adolescents’ resilience. Community-level efforts are needed to foster safe, supportive environments that nurture the mental health of young people.
Ethical Considerations
Compliance with ethical guidelines
This review utilized publicly available published data and therefore did not require formal ethical approval. All studies included had obtained ethical clearance from their respective institutional review boards.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the support provided by their respective institutions during the course of this research.
References
- Cortina MA, Sodha A, Fazel M, Ramchandani PG. Prevalence of child mental health problems in sub-Saharan Africa: A systematic review. Archives of Pediatrics & Adolescent Medicine. 2012; 166(3):276-81. [DOI:10.1001/archpediatrics.2011.592]
- Kinyanda E, Kizza R, Abbo C, Ndyanabangi S, Levin J. Prevalence and risk factors of depression in childhood and adolescence as seen in four districts of North-Eastern Uganda. BMC International Health and Human Rights. 2013; 13:19. [DOI:10.1186/1472-698X-13-19]
- Barrow E, Thomas G. Exploring perceived barriers and facilitators to mental health help-seeking in adolescents: A systematic literature review. Educational Psychology in Practice. 2022; 38(2):173-93. [DOI:10.1080/02667363.2022.2051441]
- Del Casale A, Manfredi G, Kotzalidis GD, Serata D, Rapinesi C, Caccia F, et al. Awareness and education on mental disorders in teenagers reduce stigma for mental illness: A preliminary study. Journal of Psychopathology. 2013; 19(3):208-12. [Link]
- Chandra A, Minkovitz CS. Stigma begins in the family: The influence of family relationships on adolescents’ attitudes toward mental health treatment. The Journal of Behavioral Health Services & Research. 2007; 34(4):429-42. [DOI:10.1007/s11414-007-9054-x]
- Sartorius N. Stigma and mental health. Lancet. 2007; 370(9580):810-1. [DOI:10.1016/s0140-6736(07)61245-8]
- Bronfenbrenner U. The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press; 1979. [Link]
- Thorley C. Supporting secondary schools to play a central role in early intervention mental health services. London: Institute for Public Policy Research; 2016. [Link]
- Barry MM, Clarke AM, Jenkins R, Patel V. A systematic review of the effectiveness of mental health promotion interventions for young people in low and middle income countries. BMC Public Health. 2013; 13:835. [DOI:10.1186/1471-2458-13-835]
- Mukantwali MB, Niyonsenga J, Uwingeneye L, Kanyamanza CU, Mutabaruka J. Prevalence of depression, anxiety and stress and their risk and protective factors among secondary students in Rwanda during the first wave of COVID-19 pandemic. PLoS One. 2024; 19(7):e0306389. [DOI:10.1371/journal.pone.0306389]
- Khombo S, Khombo K, Stoddart RS, Sifelani I, Sibanda T. Knowledge, attitudes, and uptake of mental health services by secondary school students in Gweru, Zimbabwe. Frontiers in Psychology. 2023; 14:1002948. [DOI:10.3389/fpsyg.2023.1002948]
- Ranjit K, Ntlantsana V, Tomita A, Paruk S. Screen time and mental health among adolescents: Implications of the rise in digital environment in South Africa. The Journal of Nervous and Mental Disease. 2022; 210(6):454-61. [DOI:10.1097/NMD.0000000000001509]
- Zeleke EA, Fikadu T, Bekele M, Sidamo NB, Temesgen Worsa K. Physical activity status among adolescents in Southern Ethiopia: A mixed methods study. Plos One. 2023; 18(11):e0293757. [DOI:10.1371/journal.pone.0293757]
- Aliy HM, Getahun HA, Dadi LS. Magnitude and associated factors of suicidal ideation and attempts among high school adolescents of Jimma Town, Ethiopia. Ethiopian Journal of Health Sciences. 2023; 33(6):1037-48. [DOI:10.4314/ejhs.v33i6.14]
- Muhwezi WW, Abbo C, Okello ES, Akello G, Ovuga EBL. Assessment of the relationship between life events with psychosocial competence of students in selected secondary schools in Northern and Central Uganda. African Health Sciences. 2020; 20(3):1426-37. [DOI:10.4314/ahs.v20i3.48]
- Tamres LK, Janicki D, Helgeson VS. Sex differences in coping behavior: A meta-analytic review and an examination of relative coping. Personality and Social Psychology Review. 2002; 6(1):2-30. [DOI:10.1207/S15327957PSPR0601_1]
- Rickwood D, Thomas K. Conceptual measurement framework for help-seeking for mental health problems. Psychology Research and Behavior Management. 2012; 5:173-83. [DOI:10.2147/PRBM.S38707]
- Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991; 50:179-211. [DOI:10.1016/0749-5978(91)90020-T]
- Vaez M, Laflamme L. Social and psychological factors related to self-reported health in adolescents: A population-based study. The Journal of Adolescent Health. 2002; 31(2):17-24. [DOI:10.1016/S1054-139X(02)00397-9]
- Fazel M, Hoagwood K, Stephan S, Ford T. Mental health interventions in schools 1: Mental health interventions in schools in high-income countries. Lancet Psychiatry. 2014; 1(5):377-87. [DOI:10.1016/S2215-0366(14)70312-4]
- Chukwu OO, Umoke M, Iyare C. Anxiety and depression among health science undergraduates in Ebonyi State, Nigeria. Journal of Research & Health. 2025; 15(4):411–20. [DOI:10.32598/JRH.15.4.2577.1]
- Jakobsson CE, Johnson NE, Ochuku B, Baseke R, Wong E, Musyimi CW, et al. Meta-analysis: Prevalence of youth mental disorders in sub-Saharan Africa. Global Mental Health (Cambridge, England)(Camb). 2024; 11:e109. [DOI:10.1017/gmh.2024.82]
- Schønning V, Hjetland GJ, Aarø LE, Skogen JC. Social media use and mental health and well-being among adolescents: A scoping review. Frontiers in Psychology. 2020; 11:1949. [DOI:10.3389/fpsyg.2020.01949]
- Sodi T, Quarshie EN, Oppong Asante K, Radzilani-Makatu M, Makgahlela M, Nkoana S, et al. Mental health literacy of school-going adolescents in sub-Saharan Africa: A regional systematic review protocol. BMJ Open. 2022; 12(9):e063687. [DOI:10.1136/bmjopen-2022-063687]
- Wollie AM, Usher K, Rice K, Islam MS. Challenges and opportunities for integrating traditional healing approaches with biomedical care for mental illness: A scoping review from healers’ perspectives. PLoS One. 2025; 20(6):e0325353. [DOI:10.1371/journal.pone.0325353]
- Patel V, Saxena S, Lund C, Thornicroft G, Baingana F, Bolton P, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018 392(10157):1553–98. [DOI:10.1016/S0140-6736(18)31612-X]
- Grande AJ, Hoffmann MS, Evans-Lacko S, Ziebold C, de Miranda CT, McDaid D, et al. Efficacy of school-based interventions for mental health problems in children and adolescents in low- and middle-income countries: A systematic review and meta-analysis. Frontiers in Psychiatry. 2023; 13:1012257. [DOI:10.3389/fpsyt.2022.1012257]
- Henrich J, Heine SJ, Norenzayan A. The weirdest people in the world? Journal of Behavioral and Brain Science. 2010; 33(2–3):61–135. [DOI:10.1017/S0140525X0999152X]
- Margaretha M, Azzopardi PS, Fisher J, Sawyer SM. School-based mental health promotion: A global policy review. Frontiers in Psychiatry. 2023; 14:1126767. [DOI:10.3389/fpsyt.2023.1126767]
Type of Study: Review Article |
Subject:
● Psychosocial Health
Received: 2025/06/2 | Accepted: 2025/11/22 | Published: 2026/03/14
Received: 2025/06/2 | Accepted: 2025/11/22 | Published: 2026/03/14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
