

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 129-138 |
Back to browse issues page


Ethics code: No: 370/367KEPK-LE/LL-02/2023
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hasanah U, Mohd Noh M, Arsat N, Ping Pang N T. Group Cognitive Behaviour Therapy Combined With Mindfulness on Quality of Life and Clinical Outcomes in Haemodialysis Patients: A Quasi- Experimental Study. J Research Health 2026; 16 (2) :129-138
URL: http://jrh.gmu.ac.ir/article-1-2817-en.html
URL: http://jrh.gmu.ac.ir/article-1-2817-en.html



1- Faculty of Health Sciences, Universitas Dharma Wacana, Lampung, Indonesia. , emailnyauus@gmail.com
2- Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Kinabalu, Malaysia.
2- Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Kinabalu, Malaysia.
Keywords: Cognitive behaviour therapy (CBT), Clinical outcomes, Haemodialysis, Mindfulness, Quality of life (QoL)
Full-Text [PDF 637 kb]
(189 Downloads)
| Abstract (HTML) (784 Views)
Full-Text: (114 Views)
Introduction
Haemodialysis is a critical intervention for patients suffering from end-stage renal disease (ESRD), with its prevalence increasing globally due to rising chronic kidney disease (CKD) rates. Recent estimates indicate that approximately 2.6 million patients worldwide are undergoing maintenance haemodialysis, a number projected to rise to about 5.4 million by 2030 [1]. The number of people with kidney failure in Indonesia is quite high. Riskesdas data 2018 explained that the prevalence of chronic renal failure increased by 1.8% (2% to 3.8%) in 2013-2018. New patients with haemodialysis in Indonesia increased from 25446 to 66433. While active patients undergoing haemodialysis from 52835 to 132142 in 2016-2018. Lampung is ranked 8th out of 34 provinces in Indonesia with 16,64% [2]. However, the physical and psychosocial burdens associated with haemodialysis are profound, leading to decreased quality of life (QoL) among these individuals. Factors contributing to diminished QoL include physical complications associated with the dialysis procedure, comorbid conditions, and environmental factors.
One notable aspect of this burden is the association between decreased levels of clinical outcomes in haemodialysis patients, often compounded by anaemia, a condition frequently encountered due to the underlying renal failure and the effects of haemodialysis itself, characterized by low hemoglobin (Hb), hematocrit (Hct), and erythrocyte levels [3]. Anaemia in ESRD patients contributes to symptoms such as fatigue, weakness, and cognitive dysfunction, significantly impacting their QoL [4, 5]. Research indicates a relationship between anaemia and QoL, particularly for ESRD patients undergoing regular haemodialysis. One study found that a significant number of patients with CKD on haemodialysis (71.9%) suffered from severe anaemia, and a majority (56.3%) reported a poor QoL. Low Hb and Hct levels in haemodialysis patients correlate with increased fatigue, diminished physical functionality, and an overall decreased QoL [6, 7]. Numerous studies have demonstrated that anaemia prevalence increases as CKD progresses, affecting up to 68% of patients starting dialysis [6]. This persistent anaemia leads to debilitating symptoms, such as fatigue, and is also linked to impaired exercise capacity and QoL. For instance, research suggests that patients with more severe anaemia report greater difficulty performing daily tasks, such as climbing stairs or walking short distances, emphasizing the need for interventions that can raise Hb levels and alleviate symptoms. Furthermore, studies have shown clear associations between lower Hb levels and diminished health-related QoL metrics in CKD patients [8, 9]. Statistically, a notable connection is observed between anaemia and QoL in CKD patients receiving haemodialysis. It is advisable to manage the incidence and symptoms of anaemia in CKD patients. Furthermore, the multifactorial aetiology of anaemia in these patients, encompassing inadequate erythropoietin production, iron deficiency, and inflammation, further complicates management and highlights the need for effective therapeutic strategies [10].
In addressing the multifaceted nature of haemodialysis patients’ challenges, group cognitive behavioral therapy (CBT) combined with mindfulness techniques has emerged as a promising intervention to improve psychological well-being and overall health-related QoL (HRQoL). CBT is a structured, goal-oriented therapeutic approach that utilizes cognitive restructuring and behavioral activation to modify dysfunctional thoughts and behaviors [5]. Mindfulness, on the other hand, involves cultivating a non-judgmental awareness of the present moment, which can enhance emotional regulation and reduce psychological distress.
Research has shown that the integration of CBT and mindfulness can lead to improvements in depressive symptoms, anxiety, stress, and QoL, conditions that are prevalent among individuals undergoing haemodialysis. This combined approach not only empowers patients to develop coping strategies for managing their treatment and the associated lifestyle changes but also serves to enhance their engagement with their healthcare, potentially leading to better clinical outcomes. Moreover, systematic reviews indicate that CBT, particularly when augmented with mindfulness techniques, can positively impact both depressive symptoms and QoL among patients on maintenance haemodialysis. There are research results that show that after the group CBT with mindfulness in ESRD hemodialysis patients, ESRD patients undergoing Haemodialysis showed significant improvements in QoL, mood, anxiety, and perceived stress after 12 weeks of group CBT [5]. The growing body of evidence supports the assertion that such psychological interventions are crucial in addressing the emotional and psychosocial aspects of chronic illness management.
Understanding the relationship between haemodialysis prevalence, resultant decreases in QoL, and clinical parameters, such as Hb, Hct, and erythrocyte levels, is vital in formulating comprehensive treatment strategies. Decreased clinical outcomes can lead to anaemia. Anaemia is the most frequent complication in patients undergoing chronic haemodialysis, which can affect QoL. HRQoL is a factor that correlates with patient morbidity, mortality, and cost of care. One of the therapies that can be utilized in the improvement of the QoL of ESRD patients is CBT. The implementation of integrative psychological approaches, such as Group CBT with mindfulness, holds significant potential for improving both clinical outcomes and the emotional health of haemodialysis patients. The current study has been conducted to assess the effect of group CBT combined with mindfulness on QoL and clinical outcome improvement in haemodialysis patients. This study addresses a significant gap in the literature by exploring the combined effects of CBT and mindfulness in a group setting specifically for hemodialysis patients. This population is often underrepresented in mental health research.
Methods
Study design and setting
This study utilized a quasi-experimental design featuring pre and post-tests alongside a control group. Questionnaires were administered both prior to and following the intervention to collect responses from respondents, who were divided into two groups: the control group and the intervention group. The intervention group was given group CBT with mindfulness, meanwhile, the control group received standard care. Only the respondents do not know which treatment they are receiving, while the researchers do. This design helps to reduce bias in participants’ responses, as they do not know whether they are receiving experimental treatment or standard care. Instead, the researchers knew the treatment assignment, which allowed them to effectively monitor the study. Comprehensive blood laboratory tests were conducted to evaluate clinical outcomes before and after the group CBT with mindfulness intervention.
Population and sample
This research was conducted in the hemodialysis room at Jendral Ahmad Yani Hospital, Lampung, from the first week of November 2023 to January 2024. The study respondents were chosen from the patients registered at the haemodialysis room of the Jendral Ahmad Yani Hospital who met the inclusion criteria of the study. The inclusion criteria are kidney disease qol short form-36 (KDQOL-SF) score <50, age >18, and >3 months of haemodialysis. A total of 66 respondents were chosen through purposive sampling, with 33 in the intervention group and 33 in the control group.
Research instrument
The independent variable in this study was the group CBT combined with mindfulness, while the dependent variables included the QoL and clinical outcomes. The KDQOL SF-36 questionnaire served as the tool for assessing patient QoL. The KDQOL-SF 36 scale produces scores ranging from 0 to 100, with 0 indicating the worst QoL and 100 indicating the best QoL.
The SF-36 component consists of eight subscales assessing physical functioning, role limitations due to physical health, bodily pain, general health perception, vitality, social functioning, role limitations due to emotional problems, and mental health [11]. Content validity was calculated using the content validity index (CVI) formula. The KDQOL-36 instrument was tested by six experts who provided input and comments on the content of the instrument, which was easy to understand and adapted to the culture and customs of Indonesians. The validity test results yielded a value of 1.00, indicating that the Indonesian version of the KDQOL-36 has very high accuracy or validity. The reliability of the Indonesian version of the KDQOL-36 was tested using Cronbach’s α coefficient. The Cronbach’s α coefficient for the Indonesian version of the KDQOL-36 was 0.708, indicating that the Indonesian version of the KDQOL-36 is reliable [12].
In this study, it was found that the KDQOL-SF had a Cronbach’s α coefficient of 0.94 for the overall scale, reflecting excellent internal consistency. The subscales included in the analysis, such as the physical health and mental health components, showed high reliability coefficients. The physical function subscale had a Cronbach’s α coefficient of 0.88, while the mental health subscale yielded a coefficient of 0.90. The reliability of each subscale reinforces the accuracy of this tool in measuring various dimensions of QoL relevant to patients undergoing haemodialysis. Three mL EDTA venous blood samples were collected, and a complete blood count examination was performed using the Sysmex XN-1000. Clinical outcomes were measured both before and after the group CBT with mindfulness intervention. A total of 33 respondents participated in the CBT intervention.
The theoretical foundations of CBT are predominantly anchored in the work of Aaron T. Beck, who originally developed cognitive therapy in the 1960s and 1970s. Beck’s framework posits that cognitive distortions contribute to emotional distress and maladaptive behaviors. At its core, CBT is built upon several key theoretical constructs. One fundamental concept is the cognitive triad, which consists of negative views about the self, the world, and the future [13]. Beck’s later work, particularly the introduction of the concept of “modes,” further expanded the CBT framework. Modes are observed as sub-organizations within an individual’s personality that comprise relevant cognitive, emotional, motivational, and behavioral patterns developed through experiences. Each mode represents a distinct way of responding to situations, especially those perceived as threatening [14].
This therapy was developed by researchers based on existing CBT modules, namely Cognitive Behavioural Therapy for Depression in Veterans and Military Servicemembers: Therapist Manual. Washington, DC: U.S. Department of Veterans Affairs [15], Manual for Group Cognitive-Behavioural Therapy of Major Depression from University of California [16], San Francisco, and Cognitive-Behavioural Therapy Group from University of Michigan [17]. Seven sessions were held for this therapy, with an explanation of each session detailed in the Table 1.
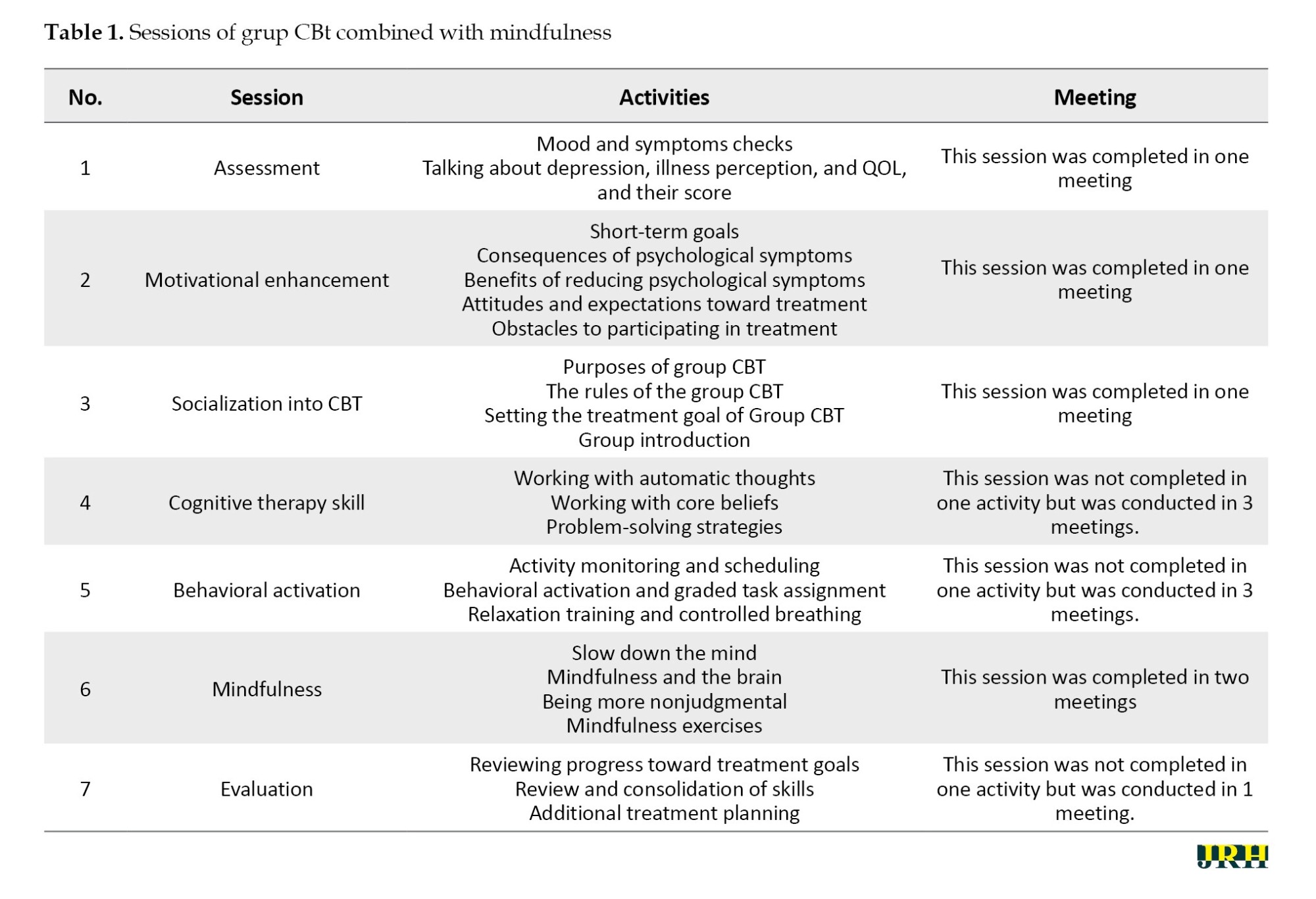
The researcher was the one, who conducted the therapy on the intervention group who is a trained psychiatric nurse specialist and trained in CBT. The researcher has a Master’s background in psychiatry nursing and has a degree as a specialist in mental health nursing. The researcher conducted therapy based on the CBT module that had been created. The therapy consisted of 7 sessions that were completed in 12 meetings as some sessions required more than one meeting. Two meetings are held every week. A total of 33 respondents were divided into 3 small groups. The therapy was conducted at different times for each small group. Follow up is done 1 month after treatment. In addition, respondents in the intervention group received a workbook that was filled in at each session. The sessions in the respondent’s workbook were the same as the sessions in the CBT module used by the therapist.
Statistical analysis
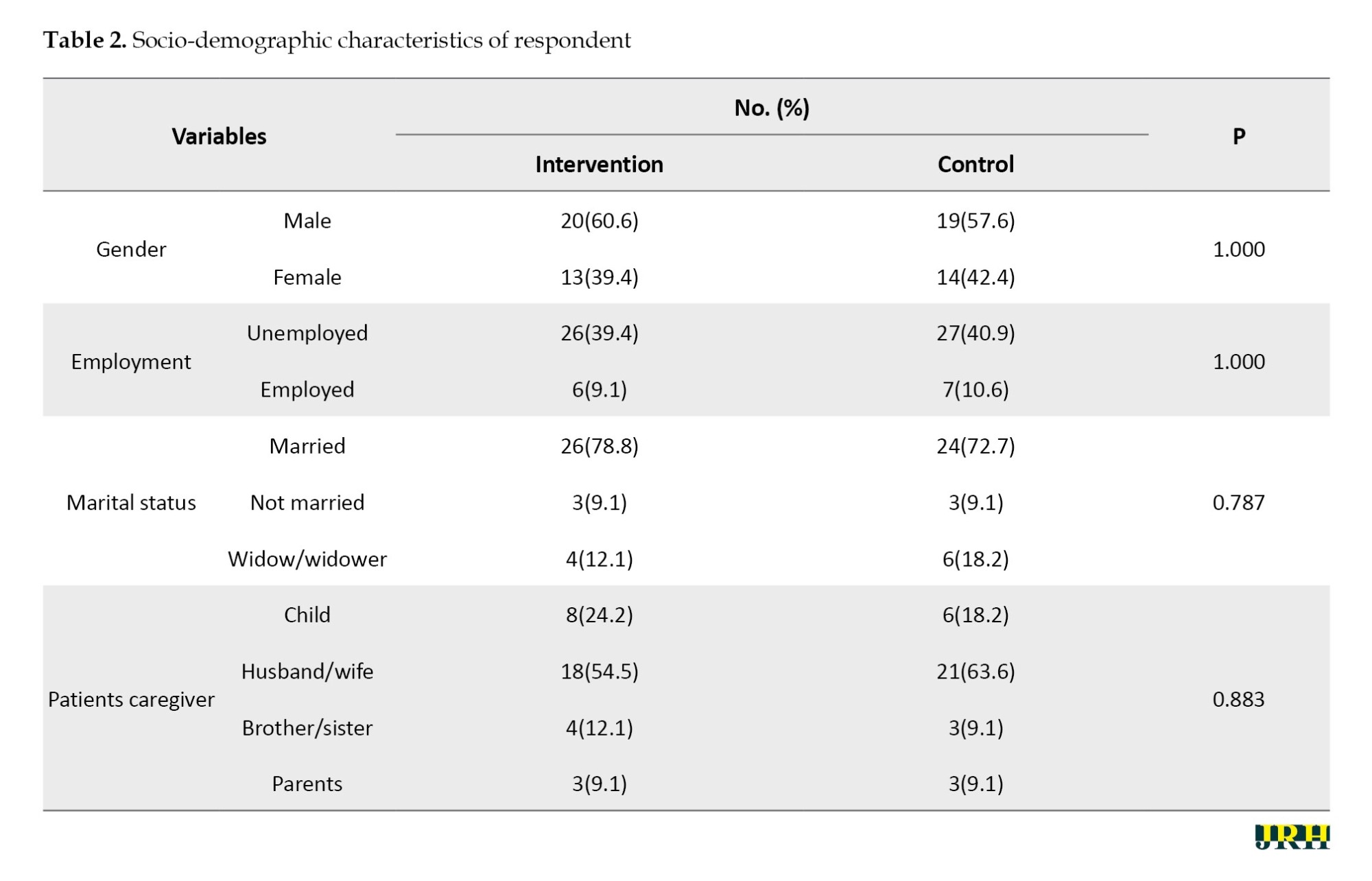
Data were cleaned, processed, and analyzed using computer software (SPSS software, version 24). All variables underwent univariate analysis to get a typical description. The effect of group CBT on patients’ QoL and clinical outcome, and the difference in QoL and clinical outcome scores before and after intervention were analyzed using bivariate analysis. The normality test of Shapiro-Wilk is effective and valid for small samples. For quality-of-life data before and after the intervention, the P=0.117 (P>0.05) so that the data is normally distributed and uses a paired t-test. While for clinical outcomes, the data is not normally distributed, therefore, it uses the Wilcoxon test. The independent t-test has been used to compare post-test scores between intervention and control groups, whereas the Mann-Whitney test has been used for clinical outcomes (Hct, Hb, erythrocyte) (Tables 2 and 3).
Results
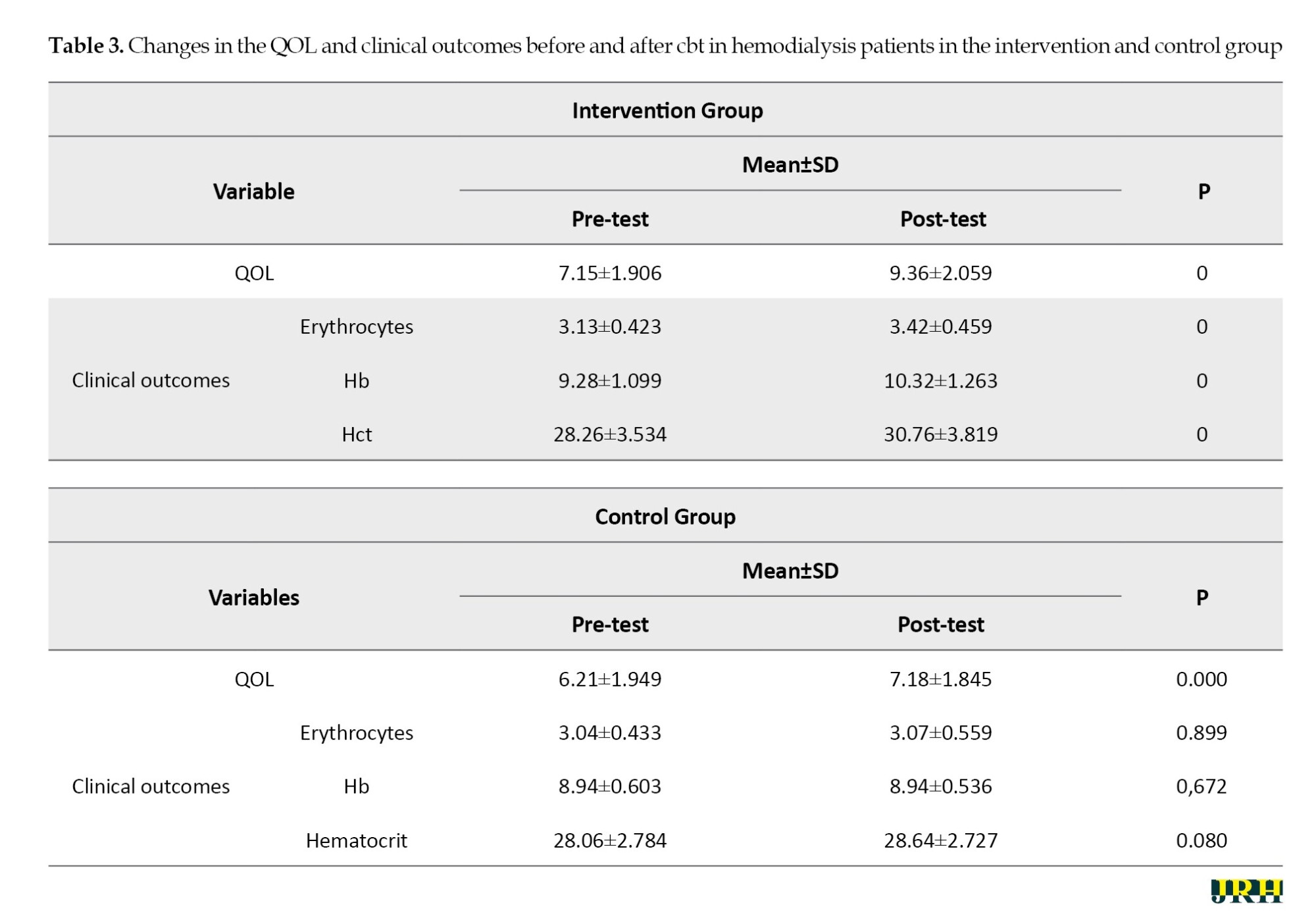
The results of QoL in the intervention group using the paired t-test (P<0.05); therefore, it can be concluded that there are changes in QoL pre (Mean±SD, 7.15±1.906) and post (Mean±SD, 9.36±2.059) given therapy in patients undergoing haemodialysis in the intervention group. Analysis of changes in erythrocytes, Hct, and Hb before and after therapy using the Wilcoxon test obtained a P =0.000 (P<0.05); therefore, it can be concluded that there are changes in clinical outcomes.
The results of QoL in the control group using the paired t-test (P<0.05); therefore, it can be concluded that there are changes in QoL pre (Mean±SD, 6.21±1.949) and post (Mean±SD, 7.18±1.845) in the control group. Analysis of changes in clinical outcomes was tested using the Wilcoxon test, Erythrocytes (P=0.899), Hb (P=0.672), Hct (P=0.080), all P>0.05; therefore, there was no change in clinical outcomes in the control group.
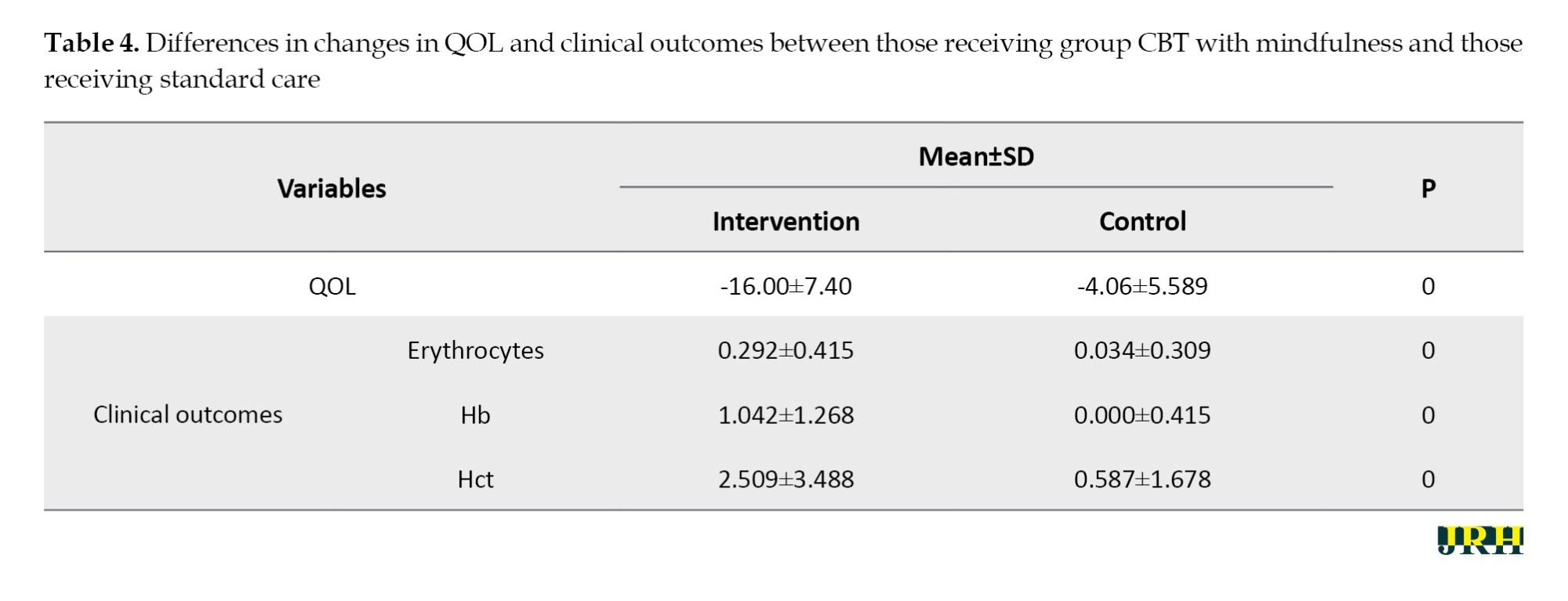
Table 4 presents an analysis of the differences in changes in QoL and clinical outcomes between the groups that received group CBT with mindfulness and those that received standard care in hemodialysis patients. The results of the statistical trial using the independent t-test obtained a P=0.000 (mean=-16.00, MD=2.726, SD=7.40, 95% CI, 0.697%, 1.787%); therefore, there is a difference in QoL between the two groups. While the clinical outcome variation between the groups that received and those that did not receive CBT in hemodialysis patients was tested using the Mann-Whitney trial, the P=0.000 (P<0.05); therefore, there is a difference in the change in the level of the clinical outcome between the two groups.
Discussion
The results showed that the QoL of haemodialysis patients was very low (mean=6.09). Some of the main factors contributing to this low QoL include family support, medication adherence, psychological state, and the patient’s experience with the disease and treatment itself. One factor that is synonymous with low QoL among haemodialysis patients is family support. The study by Titusman et al. [6] showed that patients who received good family support had higher levels of adherence to haemodialysis schedules, and this adherence was directly related to improved QoL. Patients who are not adherent to the schedule and nutritional restrictions are more at risk of experiencing poor QoL, about 4.7 times higher than those who are adherent to treatment [6].
The psychological condition of patients also has a major influence on QoL. Increased anxiety, depression, and sleep disturbances are often experienced by patients undergoing haemodialysis therapy. Several studies have shown that these psychological disorders contribute significantly to the decline in QoL [18]. In addition, the lack of supportive psychosocial approaches may also exacerbate the situation because some patients do not receive enough help to cope with the mental burden they experience [19].
Another factor that contributes to low QoL is the patient’s experience of haemodialysis itself. The time-consuming method of haemodialysis that limits patients’ physical activity can have a negative impact on QoL. Research by Mathew et al. showed that patients undergoing haemodialysis experienced a significant reduction in QoL scores compared to patients receiving other therapies [20]. These limitations can include a reduction in the ability to undertake daily activities and social participation, as well as increased feelings of dependence on healthcare facilities. Changes in living habits, dietary and activity restrictions, can also worsen patients’ QoL, especially in physical and social terms. Haemodialysis patients often experience physical complaints and unpleasant symptoms, which further lead to increased anxiety and depression, as well as reduced motivation to participate in daily activities that they previously enjoyed [21].
Clinical outcome before therapy also showed low values (erythrocytes: mean=3.13, Hb: mean=9.28, Htc: mean=28.26). Several studies have established that HRQoL is inversely correlated with erythrocyte levels. For instance, patients experiencing lower QoL often exhibit higher instances of anemia, characterized by reduced Hb levels. These reduced Hb levels correlate with poorer functional outcomes and increased fatigue, affecting patients’ ability to engage in daily activities and adhere to treatment protocols [20]. Additionally, patients undergoing hemodialysis frequently experience nutrient deficiencies that can further exacerbate anemia, thereby contributing to a reduction in their overall QoL.
Moreover, HRQoL is closely linked with laboratory markers, including Hb and Hct. They reported that impairments in QoL were found to predict poor outcomes in CKD patients, signifying that those with lower Hb levels consistently reported worse QoL outcomes [20]. This aligns with findings from Anderson et al. which indicated that adverse clinical outcomes, such as reduced Hb concentrations, were associated with a decline in QoL among dialysis patients, impacting both their physical and psychological well-being.
Furthermore, the research conducted by Dmitrieva et al. supports the premise that frailty, a contributing factor to reduced QoL also correlates significantly with lower Hb levels in hemodialysis patients. They observed that frail patients often exhibit not only diminished QoL but also laboratory results indicating inadequate erythropoiesis [8]. This interrelatedness suggests that improving patients’ QoL might have beneficial effects on their clinical parameters, including Hb and Hct levels. In connection with psychosocial factors, Celik et al. noted that perceived social support improved QoL in hemodialysis patients, leading to better adherence to treatment regimens and consequently more favorable laboratory outcomes, including higher erythrocyte, haemoglobin, and Hct levels [4]. This highlights the complex interplay between emotional well-being, social factors, and clinical outcomes, underscoring the significance of holistic patient management in improving both QoL and clinical metrics.
The negative impact of low QoL on clinical outcomes such as Hb and Hct in hemodialysis patients is well-documented. Interventions aimed at enhancing QoL, whether through psychosocial support or adequate medical management, can have far-reaching implications for clinical outcomes and patient well-being.
In this study, Group CBT therapy combined with mindfulness was shown to improve the QoL of patients and can also improve clinical outcomes of haemodialysis patients (P=0.000). CBT, developed in the 1960s by Aaron T. Beck, was initially designed to treat depression through a structured approach that challenges and modifies dysfunctional thought patterns. Beck’s approach was grounded in the cognitive model of emotional response, which posits that feelings and behaviors are governed by one’s thoughts. As he and others expanded the principles of CBT, it became a method used to address various mental health concerns, including anxiety disorders and symptoms of post-traumatic stress disorder (PTSD) [5].
The therapy emphasizes a collaborative effort between therapist and patient, focusing on identifying and restructuring cognitive distortions that contribute to emotional distress. Over the years, it has become widely researched and validated, with meta-analyses demonstrating its effectiveness in treating a range of psychological issues [5]. CBT techniques, such as cognitive restructuring and behavioral activation, allow patients to develop practical skills that can be utilized beyond the therapy sessions, thereby fostering long-lasting behavioral change. The mechanisms of mindfulness operate primarily through the frameworks of monitoring and acceptance, as described by Lindsay and Creswell in their exploration of mindfulness craving theory. Through the ongoing monitoring of present experiences, individuals become attuned to their internal states and external environments, which cultivates an awareness that fosters acceptance of thoughts and feelings rather than avoidance. This capacity to observe without judgment allows individuals to develop greater emotional regulation, thereby reducing psychological distress and enhancing well-being [22].
Group CBT combined with mindfulness therapy joins the list of treatments aimed at improving the QoL among patients undergoing hemodialysis. The unpleasant scenario is that individuals undergoing hemodialysis are prone to depression, which has been shown to be highly detrimental to their QoL and compliance with treatment regimens. A variety of research studies indicate that chronic physiologic stressors and treatments alongside the lifestyle changes they need to adopt lead patients on hemodialysis to experience distress on a mammoth scale [23, 24]. As people begin taking renal replacement therapy, there is a drop in the social roles occupied and an increase in stress levels, thereby affecting the QoL [23].
Meta-analysis, which explains the benefits of CBT in patients undergoing dialysis therapy points out that group CBT helps to reduce levels of depression and anxiety among these patients [23, 25]. Additionally, CBT is further supplemented by mindfulness techniques aimed at focusing and accepting the moment, where patients are guided towards regulating their emotional reactions to the triggers of the condition [24]. According to Sohn et al., ESRD patients who participated in a structured group CBT program that included elements of mindfulness meditation significantly improved in their QoL, mood states, and stress perception [26]. It concurs with findings from a small number of randomized control trials to suggest that mindfulness-based therapies help patients reduce anxiety and depressive symptoms thereby raising their overall heath [27].
Apart from the psychological symptoms, the integration of CBT and mindfulness cultivates a sense of community among the participants. A study demonstrated that patients who took part in group CBT recorded greater life satisfaction improvement compared with their counterparts receiving standard treatment [28]. Furthermore, mindfulness techniques have been found to impact the body positively in terms of minimising inflammation and enhancing sleep, which is important for patients on hemodialysis [29]. Such individuals suffer from various levels of cognitive impairment, but recovery of both cognitive and emotional functions using integrative treatment might help improve their health conditions in general [30, 31]. As a result of the recovery of cognitive function as well as emotional health, people tend to take a more active part in self-care measures that improve their QoL [32].
The implementation of mindfulness in CBT is more effective because it fosters a greater sense of control and acceptance among patients. It can improve the focus of individuals, which may reduce anxiety about one’s condition or treatment. In addition, mindfulness-based cognitive therapy has been found to be effective in the prevention of depressive relapses in previously depressed individuals, and this is likely to be the case for other chronic diseases, such as ESRD, as well [33]. The enhancement of QoL through these interventions is reasoned to be beneficial to the clinical outcomes. In addition, there is also a better chance of adhering to treatment, which is important in patients on hemodialysis because of improved psychological wellbeing. For instance, better adherence will help in ameliorating anemia as shown by the increased Hb and Hct levels [34]. Furthermore, it has been found that better mental status is a determinant of improved nutritional and general health status, which is vital in the care of dialysis patients [35], that may affect clinical outcomes.
It is possible that group CBT combined with mindfulness not only increases the mental health of patients receiving hemodialysis but also targets the improvement of other clinical aspects. Since these aspects are concerned with the mental state of the patient and compliance with the treatment, thus possibilities of these techniques increasing the life and health standards of such a disadvantaged group are high.
Conclusion
In summary, combining CBT with mindfulness techniques presents a novel approach to effectively improve QoL and improve clinical outcomes, especially in patients undergoing haemodialysis. Improved QoL leads patients to adhere to all treatment regimens set for them, including compliance with diets and fluids, which will affect clinical outcomes, especially Hb, Hct, and erythrocytes. This therapeutic integration utilises the strengths of both methodologies, addressing cognitive distortions while improving emotion regulation through mindfulness practice. The findings of this study could pave the way for the development of integrated psychosocial interventions in the routine care of hemodialysis patients, potentially leading to widespread adoption of such therapies in clinical settings. The results could influence healthcare policy by highlighting the importance of incorporating mental health interventions into the standard care regimen for chronic illness patients, particularly those undergoing hemodialysis.
Although the present quasi-experimental study provides valuable insights, it is important to underscore that its limited sample size constrains the generalizability of findings. Future research should include larger, more diverse populations with controlled experimental designs to mitigate biases and enhance the reliability of results. Randomized clinical trials could also explore the specific mechanisms through which CBT and mindfulness impact physiological parameters. For instance, studies might investigate if improvements in QoL as a result of successful therapy correspond with measurable changes in erythrocytes, Hb, or Hct, potentially using longitudinal designs to track these changes over time.
Ethical Considerations
Compliance with ethical guidelines
This study adhered to the ethical principles of research. It underwent ethical review at Jendral Ahmad Yani Hospital (Code: 370/367KEPK-LE/LL-02/2023).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Uswatun Hasanah; Data collection, data analysis, and final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank the people who contributed to this research.
References
Haemodialysis is a critical intervention for patients suffering from end-stage renal disease (ESRD), with its prevalence increasing globally due to rising chronic kidney disease (CKD) rates. Recent estimates indicate that approximately 2.6 million patients worldwide are undergoing maintenance haemodialysis, a number projected to rise to about 5.4 million by 2030 [1]. The number of people with kidney failure in Indonesia is quite high. Riskesdas data 2018 explained that the prevalence of chronic renal failure increased by 1.8% (2% to 3.8%) in 2013-2018. New patients with haemodialysis in Indonesia increased from 25446 to 66433. While active patients undergoing haemodialysis from 52835 to 132142 in 2016-2018. Lampung is ranked 8th out of 34 provinces in Indonesia with 16,64% [2]. However, the physical and psychosocial burdens associated with haemodialysis are profound, leading to decreased quality of life (QoL) among these individuals. Factors contributing to diminished QoL include physical complications associated with the dialysis procedure, comorbid conditions, and environmental factors.
One notable aspect of this burden is the association between decreased levels of clinical outcomes in haemodialysis patients, often compounded by anaemia, a condition frequently encountered due to the underlying renal failure and the effects of haemodialysis itself, characterized by low hemoglobin (Hb), hematocrit (Hct), and erythrocyte levels [3]. Anaemia in ESRD patients contributes to symptoms such as fatigue, weakness, and cognitive dysfunction, significantly impacting their QoL [4, 5]. Research indicates a relationship between anaemia and QoL, particularly for ESRD patients undergoing regular haemodialysis. One study found that a significant number of patients with CKD on haemodialysis (71.9%) suffered from severe anaemia, and a majority (56.3%) reported a poor QoL. Low Hb and Hct levels in haemodialysis patients correlate with increased fatigue, diminished physical functionality, and an overall decreased QoL [6, 7]. Numerous studies have demonstrated that anaemia prevalence increases as CKD progresses, affecting up to 68% of patients starting dialysis [6]. This persistent anaemia leads to debilitating symptoms, such as fatigue, and is also linked to impaired exercise capacity and QoL. For instance, research suggests that patients with more severe anaemia report greater difficulty performing daily tasks, such as climbing stairs or walking short distances, emphasizing the need for interventions that can raise Hb levels and alleviate symptoms. Furthermore, studies have shown clear associations between lower Hb levels and diminished health-related QoL metrics in CKD patients [8, 9]. Statistically, a notable connection is observed between anaemia and QoL in CKD patients receiving haemodialysis. It is advisable to manage the incidence and symptoms of anaemia in CKD patients. Furthermore, the multifactorial aetiology of anaemia in these patients, encompassing inadequate erythropoietin production, iron deficiency, and inflammation, further complicates management and highlights the need for effective therapeutic strategies [10].
In addressing the multifaceted nature of haemodialysis patients’ challenges, group cognitive behavioral therapy (CBT) combined with mindfulness techniques has emerged as a promising intervention to improve psychological well-being and overall health-related QoL (HRQoL). CBT is a structured, goal-oriented therapeutic approach that utilizes cognitive restructuring and behavioral activation to modify dysfunctional thoughts and behaviors [5]. Mindfulness, on the other hand, involves cultivating a non-judgmental awareness of the present moment, which can enhance emotional regulation and reduce psychological distress.
Research has shown that the integration of CBT and mindfulness can lead to improvements in depressive symptoms, anxiety, stress, and QoL, conditions that are prevalent among individuals undergoing haemodialysis. This combined approach not only empowers patients to develop coping strategies for managing their treatment and the associated lifestyle changes but also serves to enhance their engagement with their healthcare, potentially leading to better clinical outcomes. Moreover, systematic reviews indicate that CBT, particularly when augmented with mindfulness techniques, can positively impact both depressive symptoms and QoL among patients on maintenance haemodialysis. There are research results that show that after the group CBT with mindfulness in ESRD hemodialysis patients, ESRD patients undergoing Haemodialysis showed significant improvements in QoL, mood, anxiety, and perceived stress after 12 weeks of group CBT [5]. The growing body of evidence supports the assertion that such psychological interventions are crucial in addressing the emotional and psychosocial aspects of chronic illness management.
Understanding the relationship between haemodialysis prevalence, resultant decreases in QoL, and clinical parameters, such as Hb, Hct, and erythrocyte levels, is vital in formulating comprehensive treatment strategies. Decreased clinical outcomes can lead to anaemia. Anaemia is the most frequent complication in patients undergoing chronic haemodialysis, which can affect QoL. HRQoL is a factor that correlates with patient morbidity, mortality, and cost of care. One of the therapies that can be utilized in the improvement of the QoL of ESRD patients is CBT. The implementation of integrative psychological approaches, such as Group CBT with mindfulness, holds significant potential for improving both clinical outcomes and the emotional health of haemodialysis patients. The current study has been conducted to assess the effect of group CBT combined with mindfulness on QoL and clinical outcome improvement in haemodialysis patients. This study addresses a significant gap in the literature by exploring the combined effects of CBT and mindfulness in a group setting specifically for hemodialysis patients. This population is often underrepresented in mental health research.
Methods
Study design and setting
This study utilized a quasi-experimental design featuring pre and post-tests alongside a control group. Questionnaires were administered both prior to and following the intervention to collect responses from respondents, who were divided into two groups: the control group and the intervention group. The intervention group was given group CBT with mindfulness, meanwhile, the control group received standard care. Only the respondents do not know which treatment they are receiving, while the researchers do. This design helps to reduce bias in participants’ responses, as they do not know whether they are receiving experimental treatment or standard care. Instead, the researchers knew the treatment assignment, which allowed them to effectively monitor the study. Comprehensive blood laboratory tests were conducted to evaluate clinical outcomes before and after the group CBT with mindfulness intervention.
Population and sample
This research was conducted in the hemodialysis room at Jendral Ahmad Yani Hospital, Lampung, from the first week of November 2023 to January 2024. The study respondents were chosen from the patients registered at the haemodialysis room of the Jendral Ahmad Yani Hospital who met the inclusion criteria of the study. The inclusion criteria are kidney disease qol short form-36 (KDQOL-SF) score <50, age >18, and >3 months of haemodialysis. A total of 66 respondents were chosen through purposive sampling, with 33 in the intervention group and 33 in the control group.
Research instrument
The independent variable in this study was the group CBT combined with mindfulness, while the dependent variables included the QoL and clinical outcomes. The KDQOL SF-36 questionnaire served as the tool for assessing patient QoL. The KDQOL-SF 36 scale produces scores ranging from 0 to 100, with 0 indicating the worst QoL and 100 indicating the best QoL.
The SF-36 component consists of eight subscales assessing physical functioning, role limitations due to physical health, bodily pain, general health perception, vitality, social functioning, role limitations due to emotional problems, and mental health [11]. Content validity was calculated using the content validity index (CVI) formula. The KDQOL-36 instrument was tested by six experts who provided input and comments on the content of the instrument, which was easy to understand and adapted to the culture and customs of Indonesians. The validity test results yielded a value of 1.00, indicating that the Indonesian version of the KDQOL-36 has very high accuracy or validity. The reliability of the Indonesian version of the KDQOL-36 was tested using Cronbach’s α coefficient. The Cronbach’s α coefficient for the Indonesian version of the KDQOL-36 was 0.708, indicating that the Indonesian version of the KDQOL-36 is reliable [12].
In this study, it was found that the KDQOL-SF had a Cronbach’s α coefficient of 0.94 for the overall scale, reflecting excellent internal consistency. The subscales included in the analysis, such as the physical health and mental health components, showed high reliability coefficients. The physical function subscale had a Cronbach’s α coefficient of 0.88, while the mental health subscale yielded a coefficient of 0.90. The reliability of each subscale reinforces the accuracy of this tool in measuring various dimensions of QoL relevant to patients undergoing haemodialysis. Three mL EDTA venous blood samples were collected, and a complete blood count examination was performed using the Sysmex XN-1000. Clinical outcomes were measured both before and after the group CBT with mindfulness intervention. A total of 33 respondents participated in the CBT intervention.
The theoretical foundations of CBT are predominantly anchored in the work of Aaron T. Beck, who originally developed cognitive therapy in the 1960s and 1970s. Beck’s framework posits that cognitive distortions contribute to emotional distress and maladaptive behaviors. At its core, CBT is built upon several key theoretical constructs. One fundamental concept is the cognitive triad, which consists of negative views about the self, the world, and the future [13]. Beck’s later work, particularly the introduction of the concept of “modes,” further expanded the CBT framework. Modes are observed as sub-organizations within an individual’s personality that comprise relevant cognitive, emotional, motivational, and behavioral patterns developed through experiences. Each mode represents a distinct way of responding to situations, especially those perceived as threatening [14].
This therapy was developed by researchers based on existing CBT modules, namely Cognitive Behavioural Therapy for Depression in Veterans and Military Servicemembers: Therapist Manual. Washington, DC: U.S. Department of Veterans Affairs [15], Manual for Group Cognitive-Behavioural Therapy of Major Depression from University of California [16], San Francisco, and Cognitive-Behavioural Therapy Group from University of Michigan [17]. Seven sessions were held for this therapy, with an explanation of each session detailed in the Table 1.
The researcher was the one, who conducted the therapy on the intervention group who is a trained psychiatric nurse specialist and trained in CBT. The researcher has a Master’s background in psychiatry nursing and has a degree as a specialist in mental health nursing. The researcher conducted therapy based on the CBT module that had been created. The therapy consisted of 7 sessions that were completed in 12 meetings as some sessions required more than one meeting. Two meetings are held every week. A total of 33 respondents were divided into 3 small groups. The therapy was conducted at different times for each small group. Follow up is done 1 month after treatment. In addition, respondents in the intervention group received a workbook that was filled in at each session. The sessions in the respondent’s workbook were the same as the sessions in the CBT module used by the therapist.
Statistical analysis
Data were cleaned, processed, and analyzed using computer software (SPSS software, version 24). All variables underwent univariate analysis to get a typical description. The effect of group CBT on patients’ QoL and clinical outcome, and the difference in QoL and clinical outcome scores before and after intervention were analyzed using bivariate analysis. The normality test of Shapiro-Wilk is effective and valid for small samples. For quality-of-life data before and after the intervention, the P=0.117 (P>0.05) so that the data is normally distributed and uses a paired t-test. While for clinical outcomes, the data is not normally distributed, therefore, it uses the Wilcoxon test. The independent t-test has been used to compare post-test scores between intervention and control groups, whereas the Mann-Whitney test has been used for clinical outcomes (Hct, Hb, erythrocyte) (Tables 2 and 3).
Results
The results of QoL in the intervention group using the paired t-test (P<0.05); therefore, it can be concluded that there are changes in QoL pre (Mean±SD, 7.15±1.906) and post (Mean±SD, 9.36±2.059) given therapy in patients undergoing haemodialysis in the intervention group. Analysis of changes in erythrocytes, Hct, and Hb before and after therapy using the Wilcoxon test obtained a P =0.000 (P<0.05); therefore, it can be concluded that there are changes in clinical outcomes.
The results of QoL in the control group using the paired t-test (P<0.05); therefore, it can be concluded that there are changes in QoL pre (Mean±SD, 6.21±1.949) and post (Mean±SD, 7.18±1.845) in the control group. Analysis of changes in clinical outcomes was tested using the Wilcoxon test, Erythrocytes (P=0.899), Hb (P=0.672), Hct (P=0.080), all P>0.05; therefore, there was no change in clinical outcomes in the control group.
Table 4 presents an analysis of the differences in changes in QoL and clinical outcomes between the groups that received group CBT with mindfulness and those that received standard care in hemodialysis patients. The results of the statistical trial using the independent t-test obtained a P=0.000 (mean=-16.00, MD=2.726, SD=7.40, 95% CI, 0.697%, 1.787%); therefore, there is a difference in QoL between the two groups. While the clinical outcome variation between the groups that received and those that did not receive CBT in hemodialysis patients was tested using the Mann-Whitney trial, the P=0.000 (P<0.05); therefore, there is a difference in the change in the level of the clinical outcome between the two groups.
Discussion
The results showed that the QoL of haemodialysis patients was very low (mean=6.09). Some of the main factors contributing to this low QoL include family support, medication adherence, psychological state, and the patient’s experience with the disease and treatment itself. One factor that is synonymous with low QoL among haemodialysis patients is family support. The study by Titusman et al. [6] showed that patients who received good family support had higher levels of adherence to haemodialysis schedules, and this adherence was directly related to improved QoL. Patients who are not adherent to the schedule and nutritional restrictions are more at risk of experiencing poor QoL, about 4.7 times higher than those who are adherent to treatment [6].
The psychological condition of patients also has a major influence on QoL. Increased anxiety, depression, and sleep disturbances are often experienced by patients undergoing haemodialysis therapy. Several studies have shown that these psychological disorders contribute significantly to the decline in QoL [18]. In addition, the lack of supportive psychosocial approaches may also exacerbate the situation because some patients do not receive enough help to cope with the mental burden they experience [19].
Another factor that contributes to low QoL is the patient’s experience of haemodialysis itself. The time-consuming method of haemodialysis that limits patients’ physical activity can have a negative impact on QoL. Research by Mathew et al. showed that patients undergoing haemodialysis experienced a significant reduction in QoL scores compared to patients receiving other therapies [20]. These limitations can include a reduction in the ability to undertake daily activities and social participation, as well as increased feelings of dependence on healthcare facilities. Changes in living habits, dietary and activity restrictions, can also worsen patients’ QoL, especially in physical and social terms. Haemodialysis patients often experience physical complaints and unpleasant symptoms, which further lead to increased anxiety and depression, as well as reduced motivation to participate in daily activities that they previously enjoyed [21].
Clinical outcome before therapy also showed low values (erythrocytes: mean=3.13, Hb: mean=9.28, Htc: mean=28.26). Several studies have established that HRQoL is inversely correlated with erythrocyte levels. For instance, patients experiencing lower QoL often exhibit higher instances of anemia, characterized by reduced Hb levels. These reduced Hb levels correlate with poorer functional outcomes and increased fatigue, affecting patients’ ability to engage in daily activities and adhere to treatment protocols [20]. Additionally, patients undergoing hemodialysis frequently experience nutrient deficiencies that can further exacerbate anemia, thereby contributing to a reduction in their overall QoL.
Moreover, HRQoL is closely linked with laboratory markers, including Hb and Hct. They reported that impairments in QoL were found to predict poor outcomes in CKD patients, signifying that those with lower Hb levels consistently reported worse QoL outcomes [20]. This aligns with findings from Anderson et al. which indicated that adverse clinical outcomes, such as reduced Hb concentrations, were associated with a decline in QoL among dialysis patients, impacting both their physical and psychological well-being.
Furthermore, the research conducted by Dmitrieva et al. supports the premise that frailty, a contributing factor to reduced QoL also correlates significantly with lower Hb levels in hemodialysis patients. They observed that frail patients often exhibit not only diminished QoL but also laboratory results indicating inadequate erythropoiesis [8]. This interrelatedness suggests that improving patients’ QoL might have beneficial effects on their clinical parameters, including Hb and Hct levels. In connection with psychosocial factors, Celik et al. noted that perceived social support improved QoL in hemodialysis patients, leading to better adherence to treatment regimens and consequently more favorable laboratory outcomes, including higher erythrocyte, haemoglobin, and Hct levels [4]. This highlights the complex interplay between emotional well-being, social factors, and clinical outcomes, underscoring the significance of holistic patient management in improving both QoL and clinical metrics.
The negative impact of low QoL on clinical outcomes such as Hb and Hct in hemodialysis patients is well-documented. Interventions aimed at enhancing QoL, whether through psychosocial support or adequate medical management, can have far-reaching implications for clinical outcomes and patient well-being.
In this study, Group CBT therapy combined with mindfulness was shown to improve the QoL of patients and can also improve clinical outcomes of haemodialysis patients (P=0.000). CBT, developed in the 1960s by Aaron T. Beck, was initially designed to treat depression through a structured approach that challenges and modifies dysfunctional thought patterns. Beck’s approach was grounded in the cognitive model of emotional response, which posits that feelings and behaviors are governed by one’s thoughts. As he and others expanded the principles of CBT, it became a method used to address various mental health concerns, including anxiety disorders and symptoms of post-traumatic stress disorder (PTSD) [5].
The therapy emphasizes a collaborative effort between therapist and patient, focusing on identifying and restructuring cognitive distortions that contribute to emotional distress. Over the years, it has become widely researched and validated, with meta-analyses demonstrating its effectiveness in treating a range of psychological issues [5]. CBT techniques, such as cognitive restructuring and behavioral activation, allow patients to develop practical skills that can be utilized beyond the therapy sessions, thereby fostering long-lasting behavioral change. The mechanisms of mindfulness operate primarily through the frameworks of monitoring and acceptance, as described by Lindsay and Creswell in their exploration of mindfulness craving theory. Through the ongoing monitoring of present experiences, individuals become attuned to their internal states and external environments, which cultivates an awareness that fosters acceptance of thoughts and feelings rather than avoidance. This capacity to observe without judgment allows individuals to develop greater emotional regulation, thereby reducing psychological distress and enhancing well-being [22].
Group CBT combined with mindfulness therapy joins the list of treatments aimed at improving the QoL among patients undergoing hemodialysis. The unpleasant scenario is that individuals undergoing hemodialysis are prone to depression, which has been shown to be highly detrimental to their QoL and compliance with treatment regimens. A variety of research studies indicate that chronic physiologic stressors and treatments alongside the lifestyle changes they need to adopt lead patients on hemodialysis to experience distress on a mammoth scale [23, 24]. As people begin taking renal replacement therapy, there is a drop in the social roles occupied and an increase in stress levels, thereby affecting the QoL [23].
Meta-analysis, which explains the benefits of CBT in patients undergoing dialysis therapy points out that group CBT helps to reduce levels of depression and anxiety among these patients [23, 25]. Additionally, CBT is further supplemented by mindfulness techniques aimed at focusing and accepting the moment, where patients are guided towards regulating their emotional reactions to the triggers of the condition [24]. According to Sohn et al., ESRD patients who participated in a structured group CBT program that included elements of mindfulness meditation significantly improved in their QoL, mood states, and stress perception [26]. It concurs with findings from a small number of randomized control trials to suggest that mindfulness-based therapies help patients reduce anxiety and depressive symptoms thereby raising their overall heath [27].
Apart from the psychological symptoms, the integration of CBT and mindfulness cultivates a sense of community among the participants. A study demonstrated that patients who took part in group CBT recorded greater life satisfaction improvement compared with their counterparts receiving standard treatment [28]. Furthermore, mindfulness techniques have been found to impact the body positively in terms of minimising inflammation and enhancing sleep, which is important for patients on hemodialysis [29]. Such individuals suffer from various levels of cognitive impairment, but recovery of both cognitive and emotional functions using integrative treatment might help improve their health conditions in general [30, 31]. As a result of the recovery of cognitive function as well as emotional health, people tend to take a more active part in self-care measures that improve their QoL [32].
The implementation of mindfulness in CBT is more effective because it fosters a greater sense of control and acceptance among patients. It can improve the focus of individuals, which may reduce anxiety about one’s condition or treatment. In addition, mindfulness-based cognitive therapy has been found to be effective in the prevention of depressive relapses in previously depressed individuals, and this is likely to be the case for other chronic diseases, such as ESRD, as well [33]. The enhancement of QoL through these interventions is reasoned to be beneficial to the clinical outcomes. In addition, there is also a better chance of adhering to treatment, which is important in patients on hemodialysis because of improved psychological wellbeing. For instance, better adherence will help in ameliorating anemia as shown by the increased Hb and Hct levels [34]. Furthermore, it has been found that better mental status is a determinant of improved nutritional and general health status, which is vital in the care of dialysis patients [35], that may affect clinical outcomes.
It is possible that group CBT combined with mindfulness not only increases the mental health of patients receiving hemodialysis but also targets the improvement of other clinical aspects. Since these aspects are concerned with the mental state of the patient and compliance with the treatment, thus possibilities of these techniques increasing the life and health standards of such a disadvantaged group are high.
Conclusion
In summary, combining CBT with mindfulness techniques presents a novel approach to effectively improve QoL and improve clinical outcomes, especially in patients undergoing haemodialysis. Improved QoL leads patients to adhere to all treatment regimens set for them, including compliance with diets and fluids, which will affect clinical outcomes, especially Hb, Hct, and erythrocytes. This therapeutic integration utilises the strengths of both methodologies, addressing cognitive distortions while improving emotion regulation through mindfulness practice. The findings of this study could pave the way for the development of integrated psychosocial interventions in the routine care of hemodialysis patients, potentially leading to widespread adoption of such therapies in clinical settings. The results could influence healthcare policy by highlighting the importance of incorporating mental health interventions into the standard care regimen for chronic illness patients, particularly those undergoing hemodialysis.
Although the present quasi-experimental study provides valuable insights, it is important to underscore that its limited sample size constrains the generalizability of findings. Future research should include larger, more diverse populations with controlled experimental designs to mitigate biases and enhance the reliability of results. Randomized clinical trials could also explore the specific mechanisms through which CBT and mindfulness impact physiological parameters. For instance, studies might investigate if improvements in QoL as a result of successful therapy correspond with measurable changes in erythrocytes, Hb, or Hct, potentially using longitudinal designs to track these changes over time.
Ethical Considerations
Compliance with ethical guidelines
This study adhered to the ethical principles of research. It underwent ethical review at Jendral Ahmad Yani Hospital (Code: 370/367KEPK-LE/LL-02/2023).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Uswatun Hasanah; Data collection, data analysis, and final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank the people who contributed to this research.
References
- Cao T, An R, Wang Y, Lei J, Liang J, Wan Q. Risk factors and prevalence of cognitive impairment in maintenance haemodialysis patients: A systematic review and meta-analysis of observational studies. Journal of Advanced Nursing. 2023; 79(10):3691-706. [DOI:10.1111/jan.15746] [PMID]
- Kementerian Kesehatan RI. Riskendas 2018. Lap Nas Riskesdas. 2018; 44(8):181-222. [Link]
- Hasegawa S, Nakamura S, Sugiura T, Tsuka Y, Takahashi N, Matsumura K, et al. Evaluation of recombinant human erythropoietin responsiveness by measuring erythrocyte creatine content in haemodialysis patients. BMC Nephrology. 2021; 22(1):413. [DOI:10.1186/s12882-021-02623-4] [PMID]
- Celik G, Yöntem M, Bilge M, Cilo M, Ünaldi M. The relationship between the antioxidant system and anaemia in haemodialysis patients. Journal of International Medical Research. 2011; 39(5):1954-60. [DOI:10.1177/147323001103900541] [PMID]
- Ling C, Evans D, Zhang Y, Luo J, Hu Y, Ouyang Y, et al. The effects of cognitive behavioural therapy on depression and quality of life in patients with maintenance haemodialysis: A systematic review. BMC Psychiatry. 2020; 20(1):369. [DOI:10.1186/s12888-020-02754-2] [PMID]
- Titusman T, Guyatt A, Einarson G, Lima P. TiImpact of anemia on quality of life in patients receiving hemodialysis: A systematic review. American Journal of Kidney Diseases. 2021; 77(6): 887-95.
- Moreno F, Sanz-Guajardo D, López-Gómez JM, Jofre R, Valderrábano F. Increasing the hematocrit has a beneficial effect on quality of life and is safe in selected hemodialysis patients. Spanish Cooperative Renal Patients Quality of Life Study Group of the Spanish Society of Nephrology. Journal of the American Society of Nephrology. 2000; 11(2):335-42. [DOI:10.1681/ASN.V112335] [PMID]
- Dmitrieva O, de Lusignan S, Macdougall IC, Gallagher H, Tomson C, Harris K, et al. Association of anaemia in primary care patients with chronic kidney disease: Cross sectional study of quality improvement in chronic kidney disease (QICKD) trial data. BMC Nephrology. 2013; 14:24. [DOI:10.1186/1471-2369-14-24] [PMID]
- Sandeep A, Elumalai K, Williams H, Salkapuram S, Anandakumar S, Srinivasan S. Prevalence, prescription patterns, and quality of life of anaemia in adults with chronic renal disease. European Journal of Clinical and Experimental Medicine. 2023; 21(4):785-92. [DOI:10.15584/ejcem.2023.4.20]
- Eriksson D, Goldsmith D, Teitsson S, Jackson J, van Nooten F. Cross-sectional survey in CKD patients across Europe describing the association between quality of life and anaemia. BMC nephrology. 2016; 17(1):97. [DOI:10.1186/s12882-016-0312-9] [PMID]
- Arora S, Katz P, Nika A, Sequeira W, Block JA, Yazdany J, et al. Does higher quality of care in systemic lupus erythematosus improve quality of life? Arthritis Care & Research. 2023; 75(6):1198-205. [DOI:10.1002/acr.24979] [PMID]
- Hudoyo MCT, Perdana M, Setiyarini S. [Validity and reliability of the Kidney Disease Quality of Life-36 (KDQOL-36) in patients undergoing hemodialysis at Gadjah Mada University academic hospital, Yogyakarta (Indonesian)]. Clinical and Community Nursing Journal. 2021; 5(1). [Link]
- Beck AT, Haigh EA. Advances in cognitive theory and therapy: The generic cognitive model. Annual Review of Clinical Psychology. 2014; 10:1-24. [DOI:10.1146/annurev-clinpsy-032813-153734] [PMID]
- Apsche JA, Bass CK, Siv AM. A review and empirical comparison of three treatments for adolescent males with conduct and personality disorder: Mode deactivation therapy, cognitive behavior therapy and social skills training. International Journal of Behavioral Consultation and Therapy. 2005; 1(4):371-81. [DOI:10.1037/h0100759]
- Wenzel A, Brown GK, Karlin BE. Cognitive behavioral therapy for depression in veterans and military servicemembers therapist manual.
- Muñoz RF, Ippen CG, Rao S, Le HN, Dwyer EV. Manual for group cognitive behavioral therapy of major depression: A Reality management approach. San Francisco: San Francisco General Hospital Depression Clinic; 2000. [Link]
- DeSena D, Miner K, Tischler S, Rimer J. Cognitive-behavioral therapy (CBT) group program for depression: Adult patient manual. Michigan: University of Michigan; 2024. [Link]
- Hosseini ZM, Kafashpoor SA. The impact of psychological distress on quality of life in patients undergoing hemodialysis: A cross-sectional study. Journal of Nephrology Therapy. 2023; 13(1):12-9.
- Kang K, Lee EC, Han JH. The role of psychosocial support in managing quality of life and mental health in patients on hemodialysis. Patient Preference Adherence. 2015; 9:593-601.
- Mathew L, Tso A, Lim M, Lee H. Quality of life in patients with chronic kidney disease: A systematic review comparing treatment modalities Health and Disease. Canadian Journal of Kidney Health Disease. 2022; 9:1-12.
- Jesus JM, Coelho TS, Bittencourt CL. Impact of dialysis treatment on quality of life and social participation in chronic kidney disease patients. Journal of Nephrology. 32(4):589-96.
- Lindsay EK, Creswell JD. Mechanisms of mindfulness training: Monitor and Acceptance Theory (MAT). Clinical Psychology Review. 2017; 51:48-59. [DOI:10.1016/j.cpr.2016.10.011] [PMID]
- Ibrahim K, Taboonpong S, Nilmanat K. Coping and quality of life among Indonesians undergoing hemodialysis. Pacific Rim International Journal of Nursing Research. 2009; 13(2):109-17. [Link]
- Somvanshi S, Khan NZ, Ahmad M. Anemia in chronic kidney disease patients. Clinical Queries: Nephrology. 2012; 1(3):198-204. [DOI:10.1016/j.cqn.2012.06.003]
- Sanjaya AA, Santhi DG, Lestari AA. [Picture of anemia in chronic kidney disease patients at Sanglah general hospital in 2016 (Indonesian)]. Jurnal Medika Udayana. 2019; 8(6):1-6.[Link]
- Sohn BK, Oh YK, Choi JS, Song J, Lim A, Lee JP, et al. Effectiveness of group cognitive behavioral therapy with mindfulness in end-stage renal disease hemodialysis patients. Kidney Research and Clinical Practice. 2018; 37(1):77-84. [DOI:10.23876/j.krcp.2018.37.1.77] [PMID]
- Senduk CR, Palar S, Rotty LWA. [The relationship between anemia and the quality of life of chronic kidney disease patients undergoing regular hemodialysis (Indonesian)]. Jurnal e-Clinic. 2016; 4(1):105-10. [DOI:10.35790/ecl.4.1.2016.10941]
- Ruskovska T, Bennett SJ, Brown CR, Dimitrov S, Kamcev N, Griffiths HR. Ankyrin is the major oxidised protein in erythrocyte membranes from end-stage renal disease patients on chronic haemodialysis and oxidation is decreased by dialysis and vitamin C supplementation. Free Radical Research. 2015; 49(2):175-85. [DOI:10.3109/10715762.2014.991725] [PMID]
- Hayashi T, Joki N, Tanaka Y, Hase H. Anaemia and early phase cardiovascular events on haemodialysis. Nephrology. 2015; 20(S 4):1-6. [DOI:10.1111/nep.12642.] [PMID]
- Meghraoui M, Meddah AK, Diaf M, Diaf M. Gender effect on some blood parameters in patients undergoing haemodialysis in north western Algeria. Advanced Journal of Graduate Research. 2020; 8(1):115-20. [DOI:10.21467/ajgr.8.1.115-120]
- Hanna RM, Streja E, Kalantar-Zadeh K. Burden of anemia in chronic kidney disease: beyond erythropoietin. Advances in therapy. 2021; 38(1):52-75. [DOI:10.1007/s12325-020-01524-6] [PMID]
- Perrone V, Veronesi C, Dovizio M, Ancona DD, Bartolini F, Ferrante F, et al. The influence of Iron-Deficiency Anaemia (IDA) therapy on clinical outcomes and healthcare resource consumptions in chronic kidney disease patients affected by IDA: A real-word evidence study among the Italian population. Journal of Clinical Medicine. 2022; 11(19):5820.[DOI:10.3390/jcm11195820] [PMID]
- Koibuchi K, Miyagi M, Arai T, Aoki T, Aikawa A, Sakai K. Comparing the efficacy of continuous erythropoietin receptor activator and darbepoetin Alfa treatments in Japanese patients with chronic kidney disease during the predialysis period: A propensity-matched analysis. Nephrology. 2015; 20(S 4):22-8. [DOI:10.1111/nep.12641.] [PMID]
- Dai S, Chen Y, Hao C, Ge X, Xie Q, Shang D, et al. Addition of roxadustat to erythropoiesis-stimulating agent (ESA) effectively corrects ESA-hyporesponsive anaemia in patients on peritoneal dialysis. Journal of Clinical Pharmacy and Therapeutics. 2022; 47(10):1525-30. [DOI:10.1111/jcpt.13696.] [PMID]
- Sariati S, Sholikhah DU, Narendri CM, Sari GM, Qoidah Yahya QN. Music therapy and aromatherapy interventions in patients undergoing hemodialysis: A systematic review.Jurnal Ners. 2019; 14(S 3):81-5. [DOI:10.20473/jn.v14i3.16990]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2025/06/7 | Accepted: 2025/09/20 | Published: 2026/03/1
Received: 2025/06/7 | Accepted: 2025/09/20 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
