

Volume 16, Issue 3 (May & June 2026)
J Research Health 2026, 16(3): 295-304 |
Back to browse issues page


Ethics code: LB.02.01.I/KE/L/287/2023
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Saefurrohim M Z, Ariyanti R, Rahayu E P, Rahayu A P. Prevalence and Risk Factors of Depression Among Indonesian Adolescents. J Research Health 2026; 16 (3) :295-304
URL: http://jrh.gmu.ac.ir/article-1-2835-en.html
URL: http://jrh.gmu.ac.ir/article-1-2835-en.html



1- Department of Epidemiology, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia. , saefurrohim@fkm.unmul.ac.id
2- Department of Biostatistics, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia.
3- Department of Health Policy and Administration, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia.
4- Department of Health Promotion and Behavioral Sciences, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia.
2- Department of Biostatistics, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia.
3- Department of Health Policy and Administration, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia.
4- Department of Health Promotion and Behavioral Sciences, Faculty of Public Health, Universitas Mulawarman, Samarinda, Indonesia.
Full-Text [PDF 759 kb]
(152 Downloads)
| Abstract (HTML) (445 Views)
Full-Text: (42 Views)
Introduction
Depression is one of the leading causes of disability worldwide and contributes significantly to the global burden of disease (GBD) [1]. It should not be confused with the momentary sadness that many people experience or the distress that comes with life’s challenges. Rather, depression is a serious mental health disorder, characterized by profound and prolonged emotional suffering, and potentially leading to premature death from physical illness or suicide [2]. The impact not only burdens the individual but also has far-reaching effects on families and communities, through disruption of social functioning and reduced economic productivity [3].
Depression represents a major public health concern, ranking as the leading cause of non-fatal health loss globally [4]. According to the latest GBD Study, depressive disorders account for approximately 7.5% of all years lived with disability (YLDs), surpassing both anxiety and bipolar disorders in burden [5, 6]. In 2021, depressive disorders were responsible for 56.3 million disability-adjusted life years (DALYs), constituting 1.9% of total global DALYs [7]. Within the broader category of mental and substance use disorders, major depressive disorder contributes the largest share of YLDs [8, 6]. The burden of depression has escalated significantly since 1990, with notable increases in both prevalence and DALYs [7, 9]. In low- and middle-income countries, depressive disorders consistently rank among the top two causes of disability [6, 10].
Approximately 4.7% of the world’s population experienced a depressive episode in the past 12-month period [2]. Among adolescents, the prevalence of depression shows alarming figures. World Health Organization (WHO) estimates that 1.1% of adolescents aged 10-14 years and 2.8% of those aged 15-19 years experience the disorder [11]. National data from the Indonesian health survey (IHS) in 2023 showed a depression prevalence of 1.4%, with the 15-24 age group recording the highest rate of around 2% [12]. One of the main symptoms of depression is a persistent depressed mood (feelings of sadness, irritability, or emptiness), accompanied by a loss of interest or pleasure in daily activities [11].
Depression in Indonesia shows significant variation across provinces, with reported prevalence ranging from 1.2% in Papua Barat to over 14% in Java Island, though actual rates may be higher in underserved rural and eastern regions [13, 14]. Limited access to psychiatric care and weak health reporting systems contribute to underdiagnosis in these areas. Cultural stigma and a lack of mental health awareness further discourage individuals from seeking help, especially outside urban centers [15]. Structural barriers such as travel distance and treatment costs are particularly severe in provinces, such as Papua, Nusa Tenggara Timur, and Papua Barat. In contrast, higher reported rates in Java likely reflect better access to diagnosis rather than a true increase in cases [14, 16].
The biopsychosocial framework explains adolescent depression as resulting from the interaction of biological, psychological, and social factors. Biologically, genetic vulnerability, neurochemical imbalances, and HPA axis sensitivity increase risk [17, 18]. Psychologically, adolescents may develop maladaptive thinking patterns, such as rumination and low self-esteem, which heighten susceptibility to depression [19, 20]. Social contributors include parental neglect, bullying, isolation, and economic hardship, which can both trigger and sustain depressive symptoms [21].
In Indonesian, a range of sociodemographic and behavioral variables has been linked to heightened depressive symptoms among youth. Specifically, female adolescents, those living with biological fathers only, or with non-parent guardians, and individuals without biological siblings are reported to be more susceptible to depression. This susceptibility is notably higher in cases where the mother is either unemployed or engaged in informal employment. Moreover, behavioral patterns, such as irregular sleep duration, tobacco use, frequent intake of sugar-sweetened beverages, and the presence of chronic health conditions necessitating continuous medical care further exacerbates the risk of depressive disorders in this population [22].
Recent studies suggest that psychological interventions, such as self-affirmation, can effectively reduce depressive symptoms, especially in youth with subclinical depression. In India, self-affirmation exercises led to immediate and lasting improvements in well-being, likely by enhancing self-worth and social connection [23]. A second study involving the same population confirmed both preventive and therapeutic benefits, with sustained symptom reduction even post-intervention [24]. These effects appear linked to strengthened internal coping mechanisms and personal meaning-making. Self-affirmation thus shows promise as a low-cost, scalable tool to support adolescent mental health in low-resource settings.
Although previous studies have examined the determinants of adolescent depression in Indonesia, there remains a notable absence of research specifically targeting individuals aged 15–19 years using nationally representative data from the 2023 IHS. To address this critical gap in the literature, the present study aims to investigate the prevalence and key determinants of depression among Indonesian adolescents within this specific age group. The findings from this research are expected to offer significant scientific contributions to the field of public health, particularly in the development of evidence-based strategies for mental health promotion and depression prevention. Furthermore, these insights may serve as a foundational resource for policymakers in designing agespecific screening programs, educational initiatives, and psychosocial interventions tailored to adolescents across familial, educational, and community settings.
Methods
Design and sample
This research utilized a cross-sectional approach, drawing on secondary data from the 2023 IHS (Survei Kesehatan Indonesia [SKI]), a nationally representative survey conducted by the Ministry of Health. Data were collected through structured interviews by trained enumerators. The IHS 2023 applied a multistage stratified cluster sampling design, with stratification by province and urban–rural classification. Clustering occurred at the census block level using the 2020 population census as the sampling frame. Households were then randomly selected within each block, and sampling weights were computed based on the inverse probability of selection and adjusted for non-response and post-stratification. This approach ensures national representativeness and minimizes selection bias. A sub-sample of adolescents aged 15–19 years was extracted from the full dataset using age-based filters to focus the analysis on this target group. Individuals with incomplete data on key variables were excluded, yielding a final sample of 52,531 respondents. Further details on IHS 2023 sampling methods, stratification procedures, and weighting can be accessed in the official technical report available [12].
Data collection and instrument
The dependent variable in this research was adolescent depression, assessed using the mini international neuropsychiatric interview (MINI), a brief, structured diagnostic tool developed by psychiatrists in the U.S. and Europe for mental health screening. The MINI, which consists of 10 binary-response (‘yes’ or ‘no’) items, was translated into Bahasa Indonesia and culturally adapted to ensure semantic and conceptual equivalence for local contexts [25]. Respondents were asked questions, such as: “In the past two weeks, have you been consistently sad, depressed or down, most of the day, nearly every day?”, “Have you been less interested in most things or less able to enjoy the things you used to enjoy?”, and “Did you feel tired or without energy, most of the time?” Youth aged 15–19 were classified as having depression if they responded ‘yes’ to at least two of the first three core items and at least two of the remaining seven items. The Indonesian version of the MINI has been psychometrically validated, showing sensitivity above 85% and specificity above 90%. It has been validated among adolescents and has been used previously in national surveys [26]; all interviewers underwent standardized training, and quality control measures, such as spot-checks and re-interviews, were applied to ensure diagnostic accuracy.
Independent variables encompassed a comprehensive set of sociodemographic and health-related indicators, each defined using standardized operational criteria. Sociodemographic variables included age (15–19 years, based on self-reported date of birth), sex (male or female), marital status (never married, married, or divorced), educational attainment (less than tertiary vs. tertiary education or higher, based on the highest level completed), employment status (student/unemployed vs. employed), and health insurance coverage (insured, uninsured, or unknown). These data were collected via structured self-report during face-to-face interviews. Health-related indicators included having a family member with a diagnosed mental disorder (based on the respondent’s report of a formal medical diagnosis), a personal history of asthma (self-reported physician diagnosis), and the presence of at least one non-communicable disease (NCD). NCD status was determined using a series of standardized questions: “Have you ever been diagnosed by a doctor with cancer, diabetes, heart disease, hypertension/high blood pressure, stroke, or chronic kidney failure (defined as kidney disease lasting at least three consecutive months)?” Respondents were classified as having a chronic disease if they answered “yes” to at least one of these six conditions. The same criteria were applied to assess parental history of chronic disease, based on the adolescent’s report. Self-reported impairments in vision and hearing were assessed by asking whether respondents had difficulty seeing or hearing even with aids such as glasses or hearing devices. Smoking status referred to current use of tobacco products (yes/no), and alcohol use was defined as any alcohol consumption within the past 30 days. Physical activity was assessed using modified questions from the WHO global physical activity questionnaire within the WHO STEPS instrument, capturing the frequency and duration of moderate and vigorous activities across work, leisure, and transport domains. Activity volume was calculated using metabolic equivalent of task (MET-minutes/week), where vigorous activity (MET=8) was defined as ≥3 days/week with ≥1,500 MET-minutes/week, and moderate activity (MET=4) was defined as ≥5 days/week with ≥150 minutes/week [12].
Statistical analysis
Descriptive analysis was conducted to summarize the characteristics of all study variables. The chi-square test was used to assess the bivariate association between independent variables and depression, followed by multivariable logistic regression to identify significant predictors of depression among adolescents aged 15–19 years. Results were presented as adjusted odds ratios (aOR) with corresponding confidence interval (CI). Given the large sample size (n=52,531) and the exploratory nature of this analysis, a conventional significance threshold of α<0.05 was used to balance statistical sensitivity and control for type II error. However, to reduce the risk of type I error due to multiple hypothesis testing across independent variables, a Bonferroni correction was applied by adjusting the significance threshold based on the number of comparisons. All estimates, including P and 95% CIs, were calculated using survey-adjusted procedures that incorporated sampling weights to account for the complex survey design and ensure national representativeness in accordance with the IHS sampling structure. All statistical analyses were conducted using RStudio.
Results
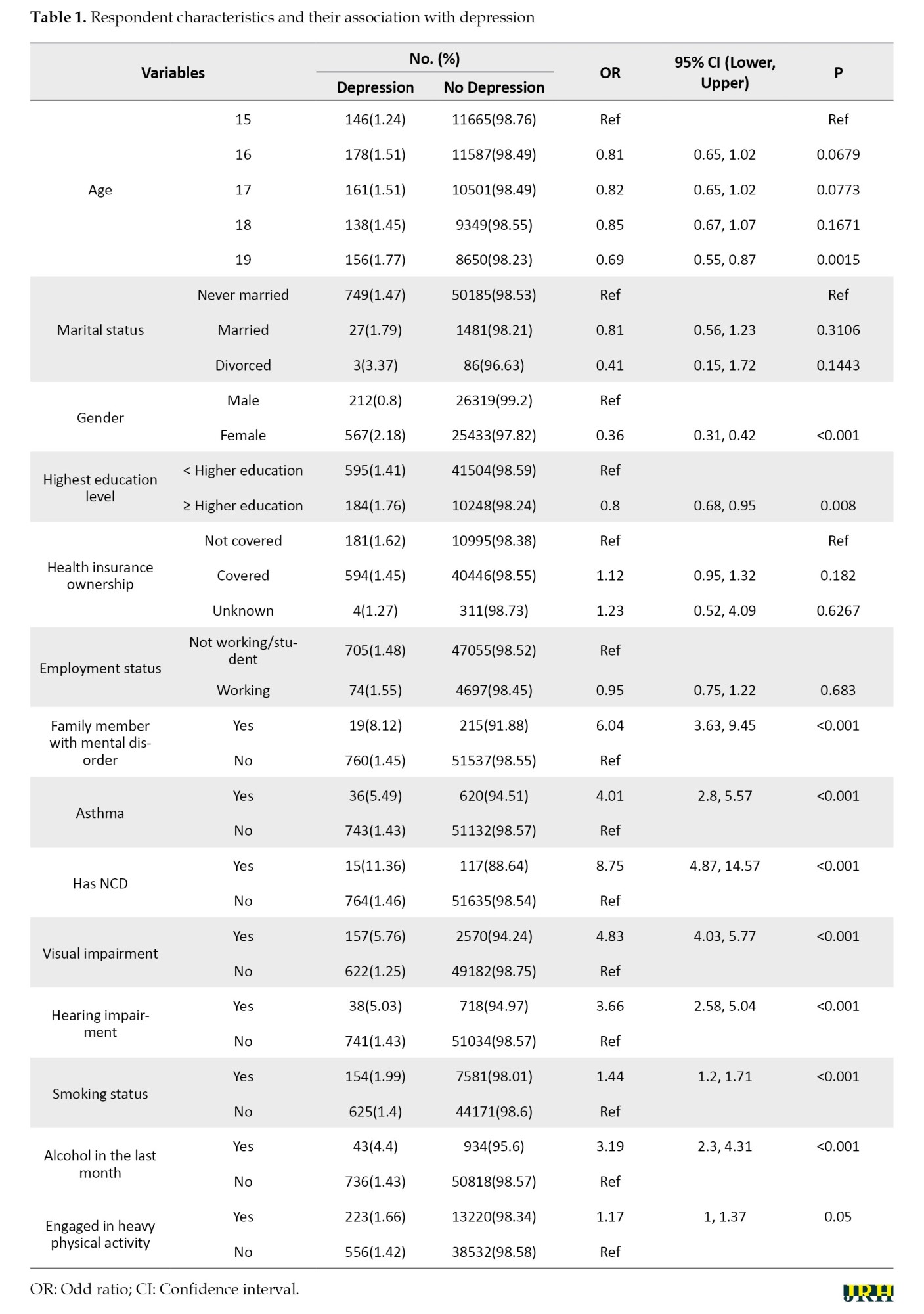
The analysis revealed several key predictors of depression among adolescents aged 15 to 19 years, with notable patterns across sociodemographic, health, and behavioral variables. Females had a higher prevalence of depression (2.18%) than males (0.80%); however, the multivariable model showed lower odds of depression among females compared with males (OR=0.36; 95% CI, 0.31%, 0.42%; P<0.001). Adolescents aged 19 had a lower odds of depression than those aged 15 (OR=0.69; 95% CI, 0.55%, 0.87%; P=0.0015), while higher educational attainment was associated with reduced risk (OR=0.8; 95% CI, 0.68%, 0.95%; P=0.008). Health-related factors showed the strongest associations: having a family member with mental illness (OR=6.04), a history of asthma (OR=4.01), having a NCD (OR=8.75), visual impairment (OR=4.83), and hearing impairment (OR=3.66), all significantly increased the odds of depression (all P<0.001). Smoking (OR=1.44; 95% CI, 1.2%, 1.71%; P<0.001) and alcohol use in the past month (OR=3.19; 95% CI, 2.3%, 4.31%; P<0.001) were also associated with higher odds of depression. Vigorous physical activity was linked to a slight increase in the odds of depression (OR=1.17; 95% CI, 1%, 1.37%; P=0.05). In contrast, marital status, employment, and health insurance ownership showed no significant association with depression (Table 1).
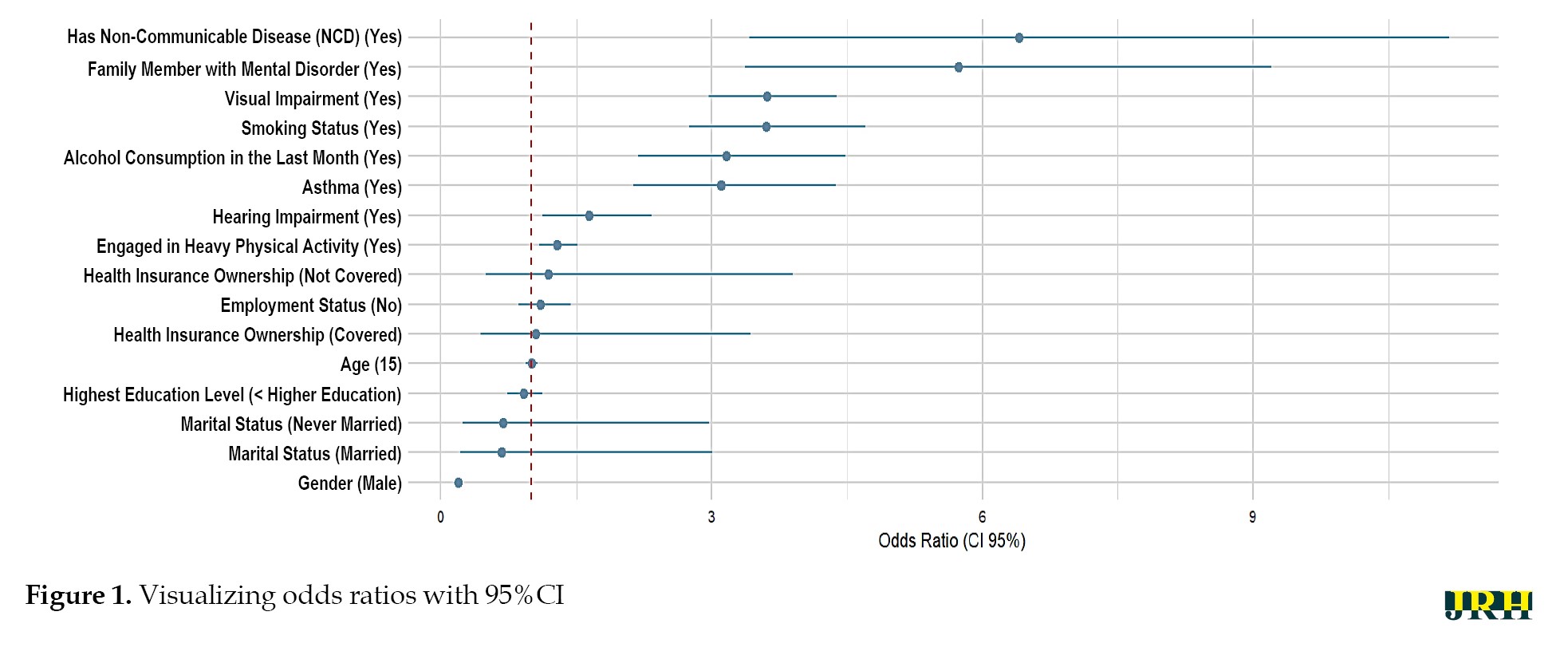
The results of multivariable logistic regression analysis identified several key predictors of depression among adolescents aged 15-19 years, with health-related and behavioral factors showing the strongest associations. Adolescents with a family member diagnosed with a mental disorder had significantly higher odds of experiencing depression (aOR=5.74; 95% CI, 3.37%, 9.21%; P<0.001), while those with a NCD such as cancer, diabetes, or chronic kidney failure were also at higher odds of depression (aOR=6.41; 95% CI, 3.42%, 11.17%; P<0.001). Visual impairment (aOR=3.61; 95% CI, 2.96%, 4.38%), asthma (aOR=3.11; 95% CI, 2.13%, 4.38%), and hearing impairment (aOR=1.64; 95% CI, 1.13%, 2.33%) further increased the odds of depression, highlighting the burden of chronic and sensory health conditions. Among behavioral factors, smoking was associated with over threefold increased odds of depression (aOR=3.6; 95% CI, 2.75%, 4.71%; P<0.001), and alcohol consumption in the past month was also strongly linked (aOR=3.16; 95% CI, 2.18%, 4.48%; P<0.001). Notably, adolescents who engaged in vigorous physical activity—defined as at least three days per week and ≥1,500 MET-minutes—also had a modest but significant increase in odds of depression (aOR=1.29; 95% CI, 1.09%, 1.51%; P=0.003), a finding that may reflect coping mechanisms or unmeasured stressors. In contrast, sociodemographic variables such as age, gender, marital status, education level, employment status, and health insurance ownership did not show significant associations with depression (all P>0.05) (Table 2).
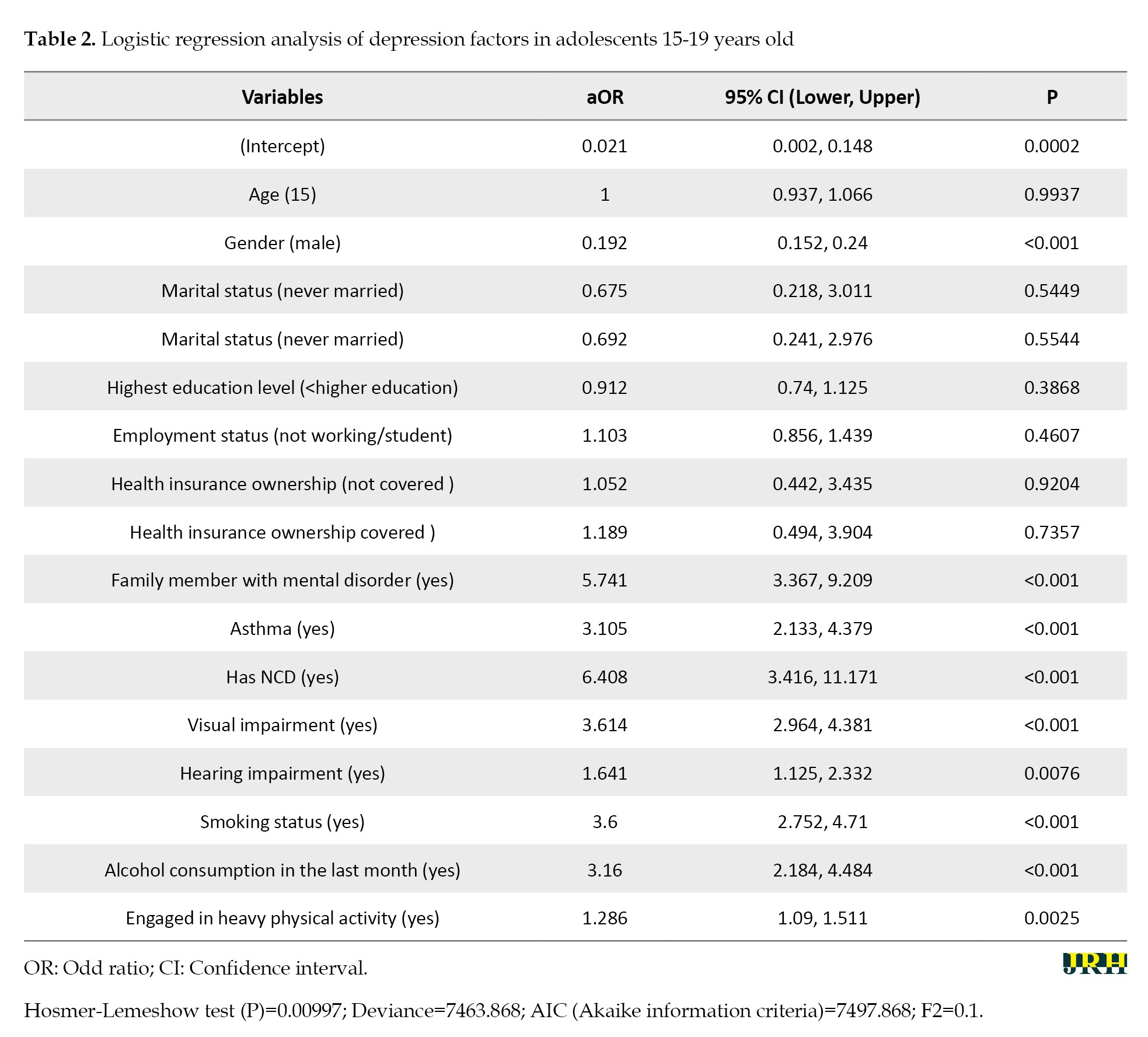
These results emphasize that health and behavioral vulnerabilities are more critical determinants of adolescent depression than demographic characteristics within this age group. Model performance was assessed using several statistical indicators. The Hosmer–Lemeshow test produced a P=0.00997, indicating poor model fit, which may result from model misspecification, omitted variables, or unaddressed nonlinear relationships. The Akaike information criterion (AIC) was 7497.868, suggesting moderate model quality, though this value is most useful when comparing alternative models. The deviance value of 7463.868 indicates room for improvement in explaining variability in the outcome. The F2 score was 0.1, reflecting limited predictive ability, particularly in identifying true cases of depression. These results suggest that although key predictors were statistically significant, the model’s overall predictive performance remains limited and may benefit from refinement.
Discussion
The main finding of this study is that the prevalence of depression among Indonesian adolescents aged 15-19 years in Indonesia is 1.77%. Figure 1 is slightly lower than the 2% depression prevalence reported among adolescents aged 5–24 years in the 2023 IHS.
Depression is one of the leading causes of disability worldwide and contributes significantly to the global burden of disease (GBD) [1]. It should not be confused with the momentary sadness that many people experience or the distress that comes with life’s challenges. Rather, depression is a serious mental health disorder, characterized by profound and prolonged emotional suffering, and potentially leading to premature death from physical illness or suicide [2]. The impact not only burdens the individual but also has far-reaching effects on families and communities, through disruption of social functioning and reduced economic productivity [3].
Depression represents a major public health concern, ranking as the leading cause of non-fatal health loss globally [4]. According to the latest GBD Study, depressive disorders account for approximately 7.5% of all years lived with disability (YLDs), surpassing both anxiety and bipolar disorders in burden [5, 6]. In 2021, depressive disorders were responsible for 56.3 million disability-adjusted life years (DALYs), constituting 1.9% of total global DALYs [7]. Within the broader category of mental and substance use disorders, major depressive disorder contributes the largest share of YLDs [8, 6]. The burden of depression has escalated significantly since 1990, with notable increases in both prevalence and DALYs [7, 9]. In low- and middle-income countries, depressive disorders consistently rank among the top two causes of disability [6, 10].
Approximately 4.7% of the world’s population experienced a depressive episode in the past 12-month period [2]. Among adolescents, the prevalence of depression shows alarming figures. World Health Organization (WHO) estimates that 1.1% of adolescents aged 10-14 years and 2.8% of those aged 15-19 years experience the disorder [11]. National data from the Indonesian health survey (IHS) in 2023 showed a depression prevalence of 1.4%, with the 15-24 age group recording the highest rate of around 2% [12]. One of the main symptoms of depression is a persistent depressed mood (feelings of sadness, irritability, or emptiness), accompanied by a loss of interest or pleasure in daily activities [11].
Depression in Indonesia shows significant variation across provinces, with reported prevalence ranging from 1.2% in Papua Barat to over 14% in Java Island, though actual rates may be higher in underserved rural and eastern regions [13, 14]. Limited access to psychiatric care and weak health reporting systems contribute to underdiagnosis in these areas. Cultural stigma and a lack of mental health awareness further discourage individuals from seeking help, especially outside urban centers [15]. Structural barriers such as travel distance and treatment costs are particularly severe in provinces, such as Papua, Nusa Tenggara Timur, and Papua Barat. In contrast, higher reported rates in Java likely reflect better access to diagnosis rather than a true increase in cases [14, 16].
The biopsychosocial framework explains adolescent depression as resulting from the interaction of biological, psychological, and social factors. Biologically, genetic vulnerability, neurochemical imbalances, and HPA axis sensitivity increase risk [17, 18]. Psychologically, adolescents may develop maladaptive thinking patterns, such as rumination and low self-esteem, which heighten susceptibility to depression [19, 20]. Social contributors include parental neglect, bullying, isolation, and economic hardship, which can both trigger and sustain depressive symptoms [21].
In Indonesian, a range of sociodemographic and behavioral variables has been linked to heightened depressive symptoms among youth. Specifically, female adolescents, those living with biological fathers only, or with non-parent guardians, and individuals without biological siblings are reported to be more susceptible to depression. This susceptibility is notably higher in cases where the mother is either unemployed or engaged in informal employment. Moreover, behavioral patterns, such as irregular sleep duration, tobacco use, frequent intake of sugar-sweetened beverages, and the presence of chronic health conditions necessitating continuous medical care further exacerbates the risk of depressive disorders in this population [22].
Recent studies suggest that psychological interventions, such as self-affirmation, can effectively reduce depressive symptoms, especially in youth with subclinical depression. In India, self-affirmation exercises led to immediate and lasting improvements in well-being, likely by enhancing self-worth and social connection [23]. A second study involving the same population confirmed both preventive and therapeutic benefits, with sustained symptom reduction even post-intervention [24]. These effects appear linked to strengthened internal coping mechanisms and personal meaning-making. Self-affirmation thus shows promise as a low-cost, scalable tool to support adolescent mental health in low-resource settings.
Although previous studies have examined the determinants of adolescent depression in Indonesia, there remains a notable absence of research specifically targeting individuals aged 15–19 years using nationally representative data from the 2023 IHS. To address this critical gap in the literature, the present study aims to investigate the prevalence and key determinants of depression among Indonesian adolescents within this specific age group. The findings from this research are expected to offer significant scientific contributions to the field of public health, particularly in the development of evidence-based strategies for mental health promotion and depression prevention. Furthermore, these insights may serve as a foundational resource for policymakers in designing agespecific screening programs, educational initiatives, and psychosocial interventions tailored to adolescents across familial, educational, and community settings.
Methods
Design and sample
This research utilized a cross-sectional approach, drawing on secondary data from the 2023 IHS (Survei Kesehatan Indonesia [SKI]), a nationally representative survey conducted by the Ministry of Health. Data were collected through structured interviews by trained enumerators. The IHS 2023 applied a multistage stratified cluster sampling design, with stratification by province and urban–rural classification. Clustering occurred at the census block level using the 2020 population census as the sampling frame. Households were then randomly selected within each block, and sampling weights were computed based on the inverse probability of selection and adjusted for non-response and post-stratification. This approach ensures national representativeness and minimizes selection bias. A sub-sample of adolescents aged 15–19 years was extracted from the full dataset using age-based filters to focus the analysis on this target group. Individuals with incomplete data on key variables were excluded, yielding a final sample of 52,531 respondents. Further details on IHS 2023 sampling methods, stratification procedures, and weighting can be accessed in the official technical report available [12].
Data collection and instrument
The dependent variable in this research was adolescent depression, assessed using the mini international neuropsychiatric interview (MINI), a brief, structured diagnostic tool developed by psychiatrists in the U.S. and Europe for mental health screening. The MINI, which consists of 10 binary-response (‘yes’ or ‘no’) items, was translated into Bahasa Indonesia and culturally adapted to ensure semantic and conceptual equivalence for local contexts [25]. Respondents were asked questions, such as: “In the past two weeks, have you been consistently sad, depressed or down, most of the day, nearly every day?”, “Have you been less interested in most things or less able to enjoy the things you used to enjoy?”, and “Did you feel tired or without energy, most of the time?” Youth aged 15–19 were classified as having depression if they responded ‘yes’ to at least two of the first three core items and at least two of the remaining seven items. The Indonesian version of the MINI has been psychometrically validated, showing sensitivity above 85% and specificity above 90%. It has been validated among adolescents and has been used previously in national surveys [26]; all interviewers underwent standardized training, and quality control measures, such as spot-checks and re-interviews, were applied to ensure diagnostic accuracy.
Independent variables encompassed a comprehensive set of sociodemographic and health-related indicators, each defined using standardized operational criteria. Sociodemographic variables included age (15–19 years, based on self-reported date of birth), sex (male or female), marital status (never married, married, or divorced), educational attainment (less than tertiary vs. tertiary education or higher, based on the highest level completed), employment status (student/unemployed vs. employed), and health insurance coverage (insured, uninsured, or unknown). These data were collected via structured self-report during face-to-face interviews. Health-related indicators included having a family member with a diagnosed mental disorder (based on the respondent’s report of a formal medical diagnosis), a personal history of asthma (self-reported physician diagnosis), and the presence of at least one non-communicable disease (NCD). NCD status was determined using a series of standardized questions: “Have you ever been diagnosed by a doctor with cancer, diabetes, heart disease, hypertension/high blood pressure, stroke, or chronic kidney failure (defined as kidney disease lasting at least three consecutive months)?” Respondents were classified as having a chronic disease if they answered “yes” to at least one of these six conditions. The same criteria were applied to assess parental history of chronic disease, based on the adolescent’s report. Self-reported impairments in vision and hearing were assessed by asking whether respondents had difficulty seeing or hearing even with aids such as glasses or hearing devices. Smoking status referred to current use of tobacco products (yes/no), and alcohol use was defined as any alcohol consumption within the past 30 days. Physical activity was assessed using modified questions from the WHO global physical activity questionnaire within the WHO STEPS instrument, capturing the frequency and duration of moderate and vigorous activities across work, leisure, and transport domains. Activity volume was calculated using metabolic equivalent of task (MET-minutes/week), where vigorous activity (MET=8) was defined as ≥3 days/week with ≥1,500 MET-minutes/week, and moderate activity (MET=4) was defined as ≥5 days/week with ≥150 minutes/week [12].
Statistical analysis
Descriptive analysis was conducted to summarize the characteristics of all study variables. The chi-square test was used to assess the bivariate association between independent variables and depression, followed by multivariable logistic regression to identify significant predictors of depression among adolescents aged 15–19 years. Results were presented as adjusted odds ratios (aOR) with corresponding confidence interval (CI). Given the large sample size (n=52,531) and the exploratory nature of this analysis, a conventional significance threshold of α<0.05 was used to balance statistical sensitivity and control for type II error. However, to reduce the risk of type I error due to multiple hypothesis testing across independent variables, a Bonferroni correction was applied by adjusting the significance threshold based on the number of comparisons. All estimates, including P and 95% CIs, were calculated using survey-adjusted procedures that incorporated sampling weights to account for the complex survey design and ensure national representativeness in accordance with the IHS sampling structure. All statistical analyses were conducted using RStudio.
Results
The analysis revealed several key predictors of depression among adolescents aged 15 to 19 years, with notable patterns across sociodemographic, health, and behavioral variables. Females had a higher prevalence of depression (2.18%) than males (0.80%); however, the multivariable model showed lower odds of depression among females compared with males (OR=0.36; 95% CI, 0.31%, 0.42%; P<0.001). Adolescents aged 19 had a lower odds of depression than those aged 15 (OR=0.69; 95% CI, 0.55%, 0.87%; P=0.0015), while higher educational attainment was associated with reduced risk (OR=0.8; 95% CI, 0.68%, 0.95%; P=0.008). Health-related factors showed the strongest associations: having a family member with mental illness (OR=6.04), a history of asthma (OR=4.01), having a NCD (OR=8.75), visual impairment (OR=4.83), and hearing impairment (OR=3.66), all significantly increased the odds of depression (all P<0.001). Smoking (OR=1.44; 95% CI, 1.2%, 1.71%; P<0.001) and alcohol use in the past month (OR=3.19; 95% CI, 2.3%, 4.31%; P<0.001) were also associated with higher odds of depression. Vigorous physical activity was linked to a slight increase in the odds of depression (OR=1.17; 95% CI, 1%, 1.37%; P=0.05). In contrast, marital status, employment, and health insurance ownership showed no significant association with depression (Table 1).
The results of multivariable logistic regression analysis identified several key predictors of depression among adolescents aged 15-19 years, with health-related and behavioral factors showing the strongest associations. Adolescents with a family member diagnosed with a mental disorder had significantly higher odds of experiencing depression (aOR=5.74; 95% CI, 3.37%, 9.21%; P<0.001), while those with a NCD such as cancer, diabetes, or chronic kidney failure were also at higher odds of depression (aOR=6.41; 95% CI, 3.42%, 11.17%; P<0.001). Visual impairment (aOR=3.61; 95% CI, 2.96%, 4.38%), asthma (aOR=3.11; 95% CI, 2.13%, 4.38%), and hearing impairment (aOR=1.64; 95% CI, 1.13%, 2.33%) further increased the odds of depression, highlighting the burden of chronic and sensory health conditions. Among behavioral factors, smoking was associated with over threefold increased odds of depression (aOR=3.6; 95% CI, 2.75%, 4.71%; P<0.001), and alcohol consumption in the past month was also strongly linked (aOR=3.16; 95% CI, 2.18%, 4.48%; P<0.001). Notably, adolescents who engaged in vigorous physical activity—defined as at least three days per week and ≥1,500 MET-minutes—also had a modest but significant increase in odds of depression (aOR=1.29; 95% CI, 1.09%, 1.51%; P=0.003), a finding that may reflect coping mechanisms or unmeasured stressors. In contrast, sociodemographic variables such as age, gender, marital status, education level, employment status, and health insurance ownership did not show significant associations with depression (all P>0.05) (Table 2).
These results emphasize that health and behavioral vulnerabilities are more critical determinants of adolescent depression than demographic characteristics within this age group. Model performance was assessed using several statistical indicators. The Hosmer–Lemeshow test produced a P=0.00997, indicating poor model fit, which may result from model misspecification, omitted variables, or unaddressed nonlinear relationships. The Akaike information criterion (AIC) was 7497.868, suggesting moderate model quality, though this value is most useful when comparing alternative models. The deviance value of 7463.868 indicates room for improvement in explaining variability in the outcome. The F2 score was 0.1, reflecting limited predictive ability, particularly in identifying true cases of depression. These results suggest that although key predictors were statistically significant, the model’s overall predictive performance remains limited and may benefit from refinement.
Discussion
The main finding of this study is that the prevalence of depression among Indonesian adolescents aged 15-19 years in Indonesia is 1.77%. Figure 1 is slightly lower than the 2% depression prevalence reported among adolescents aged 5–24 years in the 2023 IHS.
The results of logistic regression analysis showed that the main determinants of depression incidence in this study were family member with mental disorder, NCD, visual impairment, asthma, smoking status, alcohol consumption in the last month, hearing impairment, and engaged in heavy physical activity. These determinants can increase the risk of depression, whereas male gender serves as a protective factor that reduces the likelihood of depression. Meanwhile, age, marital status (never married), education level ( The association observed in this study between having a family member with a mental disorder and adolescent depression is consistent with previous research reports which say that a family history of psychiatric disorders, including in grandparents, increases the risk of depression across generations due to a combination of genetic predisposition and maladaptive parenting patterns [27]. Adolescents whose parents have mental health disorders are at increased risk of developing depression due to complex interactions among genetic, psychosocial, and environmental factors [27]. For instance, daughters of depressed mothers are more likely to experience depression themselves, whereas sons of depressed mothers tend to have lower educational attainment [28]. Paternal depression is also associated with increased family conflict, particularly when both parents are affected. Moreover, paternal psychopathology independently predicts depressive symptoms in adolescents, suggesting both biological and psychosocial pathways of transmission [29].
These findings align with studies from both Western and Asian contexts. In China, intergenerational transmission of depression risk has been shown to occur, particularly through maternal depression and adolescent stress reactivity. A study involving 738 adolescents found that maternal and paternal depressive symptoms can be transmitted through rejecting parenting behaviors, with adolescent perceptual sensitivity moderating the effect in mother-child dyads—supporting a diathesis-stress model [30]. Longitudinal evidence further indicates that fluctuations in maternal depression predict corresponding changes in adolescent depressive symptoms, highlighting the role of negative parenting and stressful family environments in this transmission process [31].
Adolescents with diabetes have been shown to have depression rates 2–3 times higher than their healthy peers [32]. Similarly, approximately 11% of children and adolescents with chronic kidney disease (CKD) exhibit depressive symptoms, triggered by treatment burdens (e.g. dialysis), social isolation, and family stress [33]. The prevalence of psychiatric disorders in pediatric CKD patients ranges from 10% to 35%, depending on disease stage (e.g. post-transplantation, on dialysis, or pre-end-stage renal disease) and patient age (child or adolescent). Studies report that 7% of children and adolescents with CKD meet diagnostic criteria for depression, with an additional 5% reporting elevated depressive symptoms [34].
A systematic review and meta-analysis of 13 studies involving 822 participants estimated the pooled prevalence of depression among children and adolescents with visual impairment at 14% [35]. Increased depression risk among visually impaired adolescents is linked to social isolation, stigma, and reduced independence [36]. In addition to visual impairments, adolescents with severe to profound hearing loss also demonstrate higher levels of depression and anxiety [37]. This study also found that while high-intensity physical activity was associated with an increased risk of depression, physical inactivity carried an even higher risk for mental health issues, including a six-fold increase in anxiety, more than a five-fold increase in depression, and over an eight-fold increase in other mental disorders compared to physically active adolescents [38].
There is also a strong link between asthma and depression among adolescents, particularly when asthma is poorly controlled, as this can impede disease management and create a reinforcing cycle between physical and mental health problems. Adolescents with asthma experiencing high levels of stress are up to nine times more likely to develop depression compared to those with lower stress levels [39]. Unhealthy behaviors, such as smoking and alcohol consumption, further elevate depression risk. The bidirectional relationship between depression and these unhealthy behaviors becomes especially pronounced among adolescents with chronic conditions, such as asthma. These complex interactions highlight the need for a holistic approach to adolescent physical and mental healthcare [40]. While these associations are well-documented globally, their manifestation in Indonesia may be shaped by cultural and systemic factors. For example, access to mental health care remains limited in rural areas, and societal stigma often prevents adolescents from seeking help. Moreover, Indonesia’s collectivist family structures may function as either support systems or sources of pressure, depending on household mental health literacy. These cultural dynamics could mediate how risk factors influencemental health outcomes.
Based on the analysis, no significant relationship was found between marital status, education level, employment status, or health insurance ownership and the incidence of depression in adolescents. This finding contrasts with several international studies that suggest lower educational attainment and lack of employment increase depression risk [41, 42]. The discrepancy may be due to the homogeneous characteristics of the study population (most being students) or unmeasured confounders such as parental education, family income, or neighborhood environment.
In light of these findings, psychological interventions such as self-affirmation may serve as a complementary strategy to reduce depressive symptoms, particularly among adolescents at subclinical risk. Two experimental studies conducted in India demonstrated the curative and preventive benefits of self-affirmation among young adults with subclinical depression. Participants who received the intervention showed significantly lower depression scores both immediately post-intervention and at follow-up, suggesting sustained mental health improvements. The mechanism of action is thought to involve enhancement of self-worth, inner strengths, and positive social relationships, which may buffer against relapse even after the intervention ends. These findings support the potential for scalable, low-cost psychological tools to complement broader mental health strategies targeting youth populations [23, 24].
A limitation of this study lies in the dichotomous classification of depression—categorized only as depressed or not depressed—which restricts further analysis. Ideally, depression status could be analyzed as a continuous variable or score, allowing for more nuanced multivariate analyses of common mental health disorders in Indonesian adolescents, especially since both variables are available in the IHS dataset. This binary approach may mask variations in depression severity, hindering efforts to identify early or subclinical symptoms. In addition, the reliance on self-reported data introduces the possibility of reporting bias, especially considering cultural stigma that may lead adolescents to underreport emotional symptoms. Another important limitation is the potential influence of unmeasured confounders such as household income, parental education, or exposure to trauma, which were not available in the dataset but may significantly affect depression outcomes. Finally, the cross-sectional design limits causal inference, making it impossible to determine temporal relationships between risk factors and depression. Future research should consider using longitudinal designs and incorporating standardized psychological instruments to improve diagnostic accuracy and causal analysis.
Conclusion
The results suggest that adolescents with risk factors, such as having a family member with a mental disorder, NCD, visual impairments, asthma, smoking habits, alcohol consumption, hearing impairments, and high-intensity physical activity, are at greater risk of developing depression. Therefore, targeted preventive interventions are essential for these groups, including comprehensive mental health programs, effective management of chronic diseases, and public health campaigns to reduce smoking and alcohol use among adolescents. Incorporating culturally sensitive mental health education, improving access to adolescent-friendly mental health services, and addressing stigma are also crucial for effective implementation in the Indonesian context. Longitudinal studies are necessary to establish causal relationships between risk factors and depression outcomes. In addition, further exploration of unmeasured social determinants—such as socioeconomic status, parental education, and trauma exposure—is essential to provide a more comprehensive understanding of depression risk in this population.
Ethical Considerations
Compliance with ethical guidelines
All research procedures complied with ethical standards and were approved by the Research Ethics Committee of Universitas Dian Nuswantoro, Semarang, Indonesia (Code: 003369/Universitas Dian Nuswantoro/2025). Permission to use the data was granted by the Ministry of Health of the Republic of Indonesia (authorization No.: 2412B889773C1309).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study design, and data collection: Muhamad Zakki Saefurrohim, Rea Ariyanti, and Eka Putri Rahayu; Data analysis and interpretation: Muhamad Zakki Saefurrohim, Eka Putri Rahayu, and Agustin Putri Rahayu; Initial draft preparation: Muhamad Zakki Saefurrohim, Rea Ariyanti, and Agustin Putri Rahayu; Administrative, technical, and material support: Rea Ariyanti, Eka Putri Rahayu, and Agustin Putri Rahayu; Supervision: Agustin Putri Rahayu and Eka Putri Rahayu; Statistical analyses: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the Health Policy and Development Agency, Ministry of Health, Republic of Indonesia, for providing access to the 2023 Indonesian Health Survey (IHS) data
These findings align with studies from both Western and Asian contexts. In China, intergenerational transmission of depression risk has been shown to occur, particularly through maternal depression and adolescent stress reactivity. A study involving 738 adolescents found that maternal and paternal depressive symptoms can be transmitted through rejecting parenting behaviors, with adolescent perceptual sensitivity moderating the effect in mother-child dyads—supporting a diathesis-stress model [30]. Longitudinal evidence further indicates that fluctuations in maternal depression predict corresponding changes in adolescent depressive symptoms, highlighting the role of negative parenting and stressful family environments in this transmission process [31].
Adolescents with diabetes have been shown to have depression rates 2–3 times higher than their healthy peers [32]. Similarly, approximately 11% of children and adolescents with chronic kidney disease (CKD) exhibit depressive symptoms, triggered by treatment burdens (e.g. dialysis), social isolation, and family stress [33]. The prevalence of psychiatric disorders in pediatric CKD patients ranges from 10% to 35%, depending on disease stage (e.g. post-transplantation, on dialysis, or pre-end-stage renal disease) and patient age (child or adolescent). Studies report that 7% of children and adolescents with CKD meet diagnostic criteria for depression, with an additional 5% reporting elevated depressive symptoms [34].
A systematic review and meta-analysis of 13 studies involving 822 participants estimated the pooled prevalence of depression among children and adolescents with visual impairment at 14% [35]. Increased depression risk among visually impaired adolescents is linked to social isolation, stigma, and reduced independence [36]. In addition to visual impairments, adolescents with severe to profound hearing loss also demonstrate higher levels of depression and anxiety [37]. This study also found that while high-intensity physical activity was associated with an increased risk of depression, physical inactivity carried an even higher risk for mental health issues, including a six-fold increase in anxiety, more than a five-fold increase in depression, and over an eight-fold increase in other mental disorders compared to physically active adolescents [38].
There is also a strong link between asthma and depression among adolescents, particularly when asthma is poorly controlled, as this can impede disease management and create a reinforcing cycle between physical and mental health problems. Adolescents with asthma experiencing high levels of stress are up to nine times more likely to develop depression compared to those with lower stress levels [39]. Unhealthy behaviors, such as smoking and alcohol consumption, further elevate depression risk. The bidirectional relationship between depression and these unhealthy behaviors becomes especially pronounced among adolescents with chronic conditions, such as asthma. These complex interactions highlight the need for a holistic approach to adolescent physical and mental healthcare [40]. While these associations are well-documented globally, their manifestation in Indonesia may be shaped by cultural and systemic factors. For example, access to mental health care remains limited in rural areas, and societal stigma often prevents adolescents from seeking help. Moreover, Indonesia’s collectivist family structures may function as either support systems or sources of pressure, depending on household mental health literacy. These cultural dynamics could mediate how risk factors influencemental health outcomes.
Based on the analysis, no significant relationship was found between marital status, education level, employment status, or health insurance ownership and the incidence of depression in adolescents. This finding contrasts with several international studies that suggest lower educational attainment and lack of employment increase depression risk [41, 42]. The discrepancy may be due to the homogeneous characteristics of the study population (most being students) or unmeasured confounders such as parental education, family income, or neighborhood environment.
In light of these findings, psychological interventions such as self-affirmation may serve as a complementary strategy to reduce depressive symptoms, particularly among adolescents at subclinical risk. Two experimental studies conducted in India demonstrated the curative and preventive benefits of self-affirmation among young adults with subclinical depression. Participants who received the intervention showed significantly lower depression scores both immediately post-intervention and at follow-up, suggesting sustained mental health improvements. The mechanism of action is thought to involve enhancement of self-worth, inner strengths, and positive social relationships, which may buffer against relapse even after the intervention ends. These findings support the potential for scalable, low-cost psychological tools to complement broader mental health strategies targeting youth populations [23, 24].
A limitation of this study lies in the dichotomous classification of depression—categorized only as depressed or not depressed—which restricts further analysis. Ideally, depression status could be analyzed as a continuous variable or score, allowing for more nuanced multivariate analyses of common mental health disorders in Indonesian adolescents, especially since both variables are available in the IHS dataset. This binary approach may mask variations in depression severity, hindering efforts to identify early or subclinical symptoms. In addition, the reliance on self-reported data introduces the possibility of reporting bias, especially considering cultural stigma that may lead adolescents to underreport emotional symptoms. Another important limitation is the potential influence of unmeasured confounders such as household income, parental education, or exposure to trauma, which were not available in the dataset but may significantly affect depression outcomes. Finally, the cross-sectional design limits causal inference, making it impossible to determine temporal relationships between risk factors and depression. Future research should consider using longitudinal designs and incorporating standardized psychological instruments to improve diagnostic accuracy and causal analysis.
Conclusion
The results suggest that adolescents with risk factors, such as having a family member with a mental disorder, NCD, visual impairments, asthma, smoking habits, alcohol consumption, hearing impairments, and high-intensity physical activity, are at greater risk of developing depression. Therefore, targeted preventive interventions are essential for these groups, including comprehensive mental health programs, effective management of chronic diseases, and public health campaigns to reduce smoking and alcohol use among adolescents. Incorporating culturally sensitive mental health education, improving access to adolescent-friendly mental health services, and addressing stigma are also crucial for effective implementation in the Indonesian context. Longitudinal studies are necessary to establish causal relationships between risk factors and depression outcomes. In addition, further exploration of unmeasured social determinants—such as socioeconomic status, parental education, and trauma exposure—is essential to provide a more comprehensive understanding of depression risk in this population.
Ethical Considerations
Compliance with ethical guidelines
All research procedures complied with ethical standards and were approved by the Research Ethics Committee of Universitas Dian Nuswantoro, Semarang, Indonesia (Code: 003369/Universitas Dian Nuswantoro/2025). Permission to use the data was granted by the Ministry of Health of the Republic of Indonesia (authorization No.: 2412B889773C1309).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study design, and data collection: Muhamad Zakki Saefurrohim, Rea Ariyanti, and Eka Putri Rahayu; Data analysis and interpretation: Muhamad Zakki Saefurrohim, Eka Putri Rahayu, and Agustin Putri Rahayu; Initial draft preparation: Muhamad Zakki Saefurrohim, Rea Ariyanti, and Agustin Putri Rahayu; Administrative, technical, and material support: Rea Ariyanti, Eka Putri Rahayu, and Agustin Putri Rahayu; Supervision: Agustin Putri Rahayu and Eka Putri Rahayu; Statistical analyses: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledge the Health Policy and Development Agency, Ministry of Health, Republic of Indonesia, for providing access to the 2023 Indonesian Health Survey (IHS) data
References
- Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: Meta-analysis of longitudinal studies. The British Journal of Psychiatry. 2018; 212(5):279–86. [DOI:10.1192/bjp.2018.27] [PMID]
- Herrman H, Patel V, Kieling C, Berk M, Buchweitz C, Cuijpers P, et al. Time for united action on depression: A Lancet–world psychiatric association commission. The Lancet. 2022; 399(10328):957–1022. [DOI:10.1016/s0140-6736(21)02141-3] [PMID]
- Dwyer JB, Stringaris A, Brent DA, Bloch MH. Annual Research Review: Defining and treating pediatric treatment-resistant depression. Journal of Child Psychology and Psychiatry. 2020; 61(3):312–32. [DOI:10.1111/jcpp.13202] [PMID]
- Krause KR, Chung S, Adewuya AO, Albano AM, Babins-Wagner R, Birkinshaw L, et al. International consensus on a standard set of outcome measures for child and youth anxiety, depression, obsessive-compulsive disorder, and post-traumatic stress disorder. Lancet Psychiatry. 2021; 8(1):76–86. [DOI:10.1016/s2215-0366(20)30356-4] [PMID]
- Australian Institute of Health and Welfare. Australian burden of disease study: Impact and causes of illness and death in Australia 2018. Canberra: Australian Institute of Health and Welfare; 2021. [Link]
- World Health Organisation. Depression and other common mental disorders: Global health estimates. Geneva: World Health Organization; 2017. [Link]
- Rong J, Wang X, Cheng P, Li D, Zhao D. Global, regional and national burden of depressive disorders and attributable risk factors, from 1990 to 2021: Results from the 2021 global burden of disease study. The British Journal of Psychiatry. 2025; 227(4):688-97. [DOI:10.1192/bjp.2024.266] [PMID]
- Yan G, Zhang Y, Wang S, Yan Y, Liu M, Tian M, et al. Global, regional, and national temporal trend in burden of major depressive disorder from 1990 to 2019: An analysis of the global burden of disease study. Psychiatry Research. 2024; 337:115958. [Link]
- Chen XD, Li F, Zuo H, Zhu F. Trends in prevalent cases and disability-adjusted life-years of depressive disorders worldwide: Findings from the global burden of disease study from 1990 to 2021. Depress Anxiety. 2025; 2025:5553491. [Link]
- Rathod S, Pinninti N, Irfan M, Gorczynski P, Rathod P, Gega L, et al. Mental health service provision in low- and middle-income countries. Health Services Insights. 2017; 10:1178632917694350. [Link]
- WHO. Depressive disorder (depression). Geneva: World Health Organization; 2023. [Link]
- Health Development Policy Agency. Results of the 2023 Indonesian health survey (IHS). Jakarta: Ministry of Health Republic of Indonesia; 2023. [Link]
- Putri A, Hartono R, Nabila S. Examining health disparities in access to mental health services in urban and rural areas. International Journal of Health and Social Behavior. 2024; 1(1):06–10. [Link]
- Agustin WS, Prastika HA, Kendrasti GK, Fajriyah R, Le-Quy V. Clustering the depression prevalence in Indonesia provinces through natural breaks Jenks method. Clinical Practice and Epidemiology in Mental Health. 2025; 21(1):e17450179375982. [Link]
- Hartini N, Fardana NA, Ariana AD, Wardana ND. Stigma toward people with mental health problems in Indonesia. Psychology Research and Behavior Management. 2018; 11:535–41. [Link]
- Munira L, Liamputtong P, Viwattanakulvanid P. Barriers and facilitators to access mental health services among people with mental disorders in Indonesia: A qualitative study. Belitung Nursing Journal. 2023; 9(2):110. [Link]
- Eiland L, Romeo RD. Stress and the developing adolescent brain. Neuroscience. 2012; 249:162. [Link]
- Bingham B, McFadden K, Zhang X, Bhatnagar S, Beck S, Valentino R. Early adolescence as a critical window during which social stress distinctly alters behavior and brain norepinephrine activity. Neuropsychopharmacology. 2011; 36(4):896–909. [PMID]
- Depboylu GY, Fındık BE. Relationships among alexithymia, psychological distress, and disordered eating behaviors in adolescents. Appetite. 2024; 200:107536. [Link]
- Merino M, Tornero-Aguilera JF, Rubio-Zarapuz A, Villanueva-Tobaldo CV, Martín-Rodríguez A, Clemente-Suárez VJ. Body perceptions and psychological well-being: A review of the impact of social media and physical measurements on self-esteem and mental health with a focus on body image satisfaction and its relationship with cultural and gender factors. Healthcare (Basel). 2024; 12(14):1396. [DOI:10.3390/healthcare12141396] [PMID]
- Liu Y.The role of peer relationships in adolescents’ psychological well-being. Paper presented at: International Conference on Education, Psychology and Cultural Communication (ICEPCC 2023). 15 December 2023; Singapore. [Link]
- Candrarukmi D, Hartanto F, Wibowo T, Nugroho HW, Anam MS, Indraswari BW, et al. Risk factors for depression symptoms in adolescents: A population-based study. Saudi Medical Journal. 2025; 46(2):190. [Link]
- Pandey R, Tiwari GK, Rai PK. Restoring and preserving capacity of self-affirmation for well-being in Indian adults with non-clinical depressive tendencies. Current Issues in Personality Psychology. 2021; 9(2):135–47. [Link]
- Pandey R, Tiwari GK, Rai PK. Understanding the efficacy of self-affirmation intervention for subclinical depression among young adults. Practice in Clinical Psychology. 2023; 11(1):23–34. [Link]
- Idaiani S, Mubasyiroh R, Isfandari S. Validity and reliability of depression, anxiety and psychosis questionnaire of mini international neuropsychiatric interview (MINI) in Indonesia. ASEAN Journal of Psychiatry. 2020; 21(1):1. [Link]
- Tran TD, Kaligis F, Wiguna T, Willenberg L, Nguyen HTM, Luchters S, et al. Screening for depressive and anxiety disorders among adolescents in Indonesia: Formal validation of the centre for epidemiologic studies depression scale – revised and the Kessler psychological distress scale. Journal of Affective Disorders. 2019; 246:189–94. [DOI:10.1016/j.jad.2018.12.042] [PMID]
- Wang E, Zhang J, Peng S, Zeng B. The association between family function and Adolescents’ depressive symptoms in China: a longitudinal cross-lagged analysis. Frontiers in Psychiatry. 2021; 12:744976. [DOI:10.3389/fpsyt.2021.744976]
- Sander JB, McCarty CA. Youth depression in the family context: Familial risk factors and models of treatment. Clinical Child and Family Psychology Review. 2005; 8(3):203–19. [DOI:10.1007/s10567-005-6666-3] [PMID]
- Huang X, Hu N, Yao Z, Peng B. Family functioning and adolescent depression: A moderated mediation model of self-esteem and peer relationships. Frontiers in Psychology. 2022; 13:962147. [DOI:10.3389/fpsyg.2022.962147] [PMID]
- Sun K, Zhang X, Li P, Cao C. Intergenerational Transmission of Depressive Symptoms in Chinese Families: The Role of Mothers versus Fathers and Adolescent Perceptual Sensitivity. Psychology Research and Behavior Management. 2025; 18:1481. [Link]
- Zhai R, Yang S. How parental depression influences the development of adolescent depression: Based on data from China family panel studies. Frontiers in Psychology. 2025; 16:1514024. [Link]
- Bădescu SV, Tătaru C, Kobylinska L, Georgescu EL, Zahiu DM, Zăgrean AM, et al. The association between Diabetes mellitus and Depression. Journal of Medicine and Life. 2016; 9(2):120-5. [PMID]
- Kiliś-Pstrusińska K, Medyńska A, Adamczyk P, Leszczyńska B, Szczepańska M, Tkaczyk M, et al. Depressive disorders in children with chronic kidney disease treated conservatively. Advances in Clinical and Experimental Medicine. 2024; 33(11):1189-99. [DOI:10.17219/acem/175236] [PMID]
- Dryjańska N, Kiliś-Pstrusińska K. Depression in children and adolescents with chronic kidney disease-review of available literature. Journal of Clinical Medicine. 2023; 12(10):3554. [DOI:10.3390/jcm12103554] [PMID]
- Bakhla AK, Pallavi P, Kisku RR, Goyal N, Kumar A, Prasad K. Prevalence of depression in visually impaired children and adolescents: A systematic review and meta-analysis. Indian Journal of Psychiatry. 2023; 65(4):396-403. [PMID]
- Rafeyan R. Study reinforces link between visual impairment and suicide risk. The Journal of Clinical Psychiatry. 2024. [Link]
- Cejas I, Coto J, Sanchez C, Holcomb M, Lorenzo NE. Prevalence of depression and anxiety in adolescents with hearing loss. Otology & Neurotology. 2021; 42(4):e470-5. [DOI:10.1097/mao.0000000000003006] [PMID]
- Denche-Zamorano Á, Franco-García JM, Carlos-Vivas J, Mendoza-Muñoz M, Pereira-Payo D, Pastor-Cisneros R, et al. Increased risks of mental disorders: Youth with inactive physical activity. Healthcare (Basel). 2022; 10(2):237. [DOI:10.3390/healthcare10020237] [PMID]
- Leonard SI, Turi ER, Powell JS, Usseglio J, MacDonell KK, Bruzzese JM. Associations of asthma self-management and mental health in adolescents: A scoping review. Respiratory Medicine. 2022; 200:106897. [DOI:10.1016/j.rmed.2022.106897] [PMID]
- Park JH, Kim MJ. A study on depression among adolescents with asthma in South Korea using the 15th Korea Youth risk behaviour web-based survey. Child Health Nursing Research. 2021; 27(3):276-85. [DOI:10.4094/chnr.2021.27.3.276] [PMID]
- Patria B. The longitudinal effects of education on depression: Finding from the Indonesian national survey. Frontiers in Public Health. 2022; 10:1017995. [DOI:10.3389/fpubh.2022.1017995] [PMID]
- Yang Y, Niu L, Amin S, Yasin I. Unemployment and mental health: a global study of unemployment’s influence on diverse mental disorders. Frontiers in Public Health. 2024; 12:1440403. [Link]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2025/07/2 | Accepted: 2025/09/20 | Published: 2026/03/14
Received: 2025/07/2 | Accepted: 2025/09/20 | Published: 2026/03/14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
