

Volume 15, Issue 6 And S7 (Artificial Intelligence 2025)
J Research Health 2025, 15(6 And S7): 641-660 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Afkhami Teimouri G, Amadeh Taheri A, Moeinipour Y, Adineh Fathabadi M, Bagheri F. The Impact of AI-based Nursing Documentation on Time Management and Patient Safety: A Systematic Review. J Research Health 2025; 15 (6) :641-660
URL: http://jrh.gmu.ac.ir/article-1-2940-en.html
URL: http://jrh.gmu.ac.ir/article-1-2940-en.html
Ghazaleh Afkhami Teimouri1 

 , Arash Amadeh Taheri1 , Yasamin Moeinipour2 , Malihe Adineh Fathabadi1 , Fatemeh Bagheri3
, Arash Amadeh Taheri1 , Yasamin Moeinipour2 , Malihe Adineh Fathabadi1 , Fatemeh Bagheri3
, Arash Amadeh Taheri1 , Yasamin Moeinipour2 , Malihe Adineh Fathabadi1 , Fatemeh Bagheri3
1- Department of Nursing and Midwifery, MMS.C. Islamic Azad University, Mashhad, Iran.
2- Department of Cardiothoracic Surgery, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Nursing and Midwifery, MMS.C. Islamic Azad University, Mashhad, Iran. ,bagherifatemeh59@yahoo.com
2- Department of Cardiothoracic Surgery, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Nursing and Midwifery, MMS.C. Islamic Azad University, Mashhad, Iran. ,
Keywords: Artificial intelligence (AI), Nursing documentation, Documentation burden, Patient safety, Systematic review
Full-Text [PDF 1334 kb]
(272 Downloads)
| Abstract (HTML) (1968 Views)
Full-Text: (442 Views)
Introduction
The documentation of uniform nursing practices is characterized by prompt, accurate, and consistent documentation of evaluation, diagnosis, treatment strategies, interventions, and outcomes throughout the nursing process. Empirical evidence suggests that, in addition to continuity of care, there is a direct correlation between the caliber of such documentation and the overall quality and safety of care [1]. From a quality and safety point of view, the introduction of organized electronic frameworks increases the accuracy of the content and usability of the data, which is correlated with a reduction in document inaccuracies and a positive progress in patient safety indicators [2, 3]. The nursing dossier serves as a fundamental framework for patient-oriented, safe, and effective care, and dedicating resources to standardization, improving quality, and further utilizing its data significantly enhances both clinical and administrative outcomes [4].
Despite its foundational role, clinical documentation in practice has become a “hidden burden” for nurses. With the implementation of electronic health records (EHRs), the volume and complexity of documentation tasks have significantly increased, consuming a substantial portion of a nurse’s shift. Time allocation studies reveal that nurses spend between 25% and 35.3% of their work time on documentation [5, 6], time that could otherwise be dedicated to direct patient care, education, and support. In the health informatics literature, this phenomenon has been framed as the “documentation burden.” This added load is also linked to adverse psychological and professional outcomes. Research has demonstrated a correlation between high documentation volume and inefficient or unusable EHRs with factors, such as emotional exhaustion and depersonalization, which contribute to burnout [7, 8]. Furthermore, documentation processes are inherently susceptible to human errors from incomplete or incorrect medication records to omissions and delays in documenting vital signs that can lead to flawed clinical decision-making and adverse events [3].
In response to the dual challenges of the “documentation time burden” and associated “safety risks,” artificial intelligence (AI) has emerged as a transformative solution. Three key branches, automatic speech recognition (ASR), natural language processing (NLP), and machine learning (ML), can optimize the documentation loop from “clinical dialogue” to “structured note,” restoring time for direct patient interaction through intelligent automation. In the NLP domain, systematic and integrative reviews have shown that extracting critical components from unstructured nursing notes is reliable for decision support, trend identification, and predicting high-risk events, like patient falls [9, 10]. Moreover, combining emergency department nursing texts with structured data in ML models has facilitated the early detection of critical conditions, such as sepsis, and enhanced the efficacy of early warning systems [11]. At the same time, field experiences with ASR serve as a reminder that automated documentation without review may be prone to transcriptional and conceptual errors. Therefore, a “human-in-the-loop” approach and quality assurance procedures are vital for ensuring the safety and accuracy of records [12, 13]. Collectively, this body of evidence suggests that the targeted application of AI can significantly enhance documentation efficiency while also contributing to patient safety by reducing burnout and improving data quality, provided it is designed responsibly and its clinical outcomes are continuously evaluated [14-18].
In recent years, a growing number of studies have investigated the application of these technologies in clinical settings. Despite promising results, the existing evidence in this field is highly scattered, heterogeneous, and in the early stages of maturity. Many of these studies are small-scale, single-center, and employ quasi-experimental designs, which carry a high potential for bias and limit the generalizability of their findings. There is also considerable heterogeneity in the types of technology used, patient populations, clinical settings, and outcome measures evaluated. This diversity makes it difficult to synthesize the evidence and draw definitive conclusions about the overall effectiveness of these interventions.
Consequently, this systematic review aimed to address this evidence gap and the heterogeneity of existing results by synthesizing the effect of AI-driven interventions in nursing documentation on two key outcomes: time management and patient safety. This study will provide practical, evidence-based recommendations for administrators, policymakers, clinical nurses, and technology developers, an action that is of strategic importance given the increasing investments by healthcare systems in digital health and artificial intelligence.
Methods
Protocol and registration
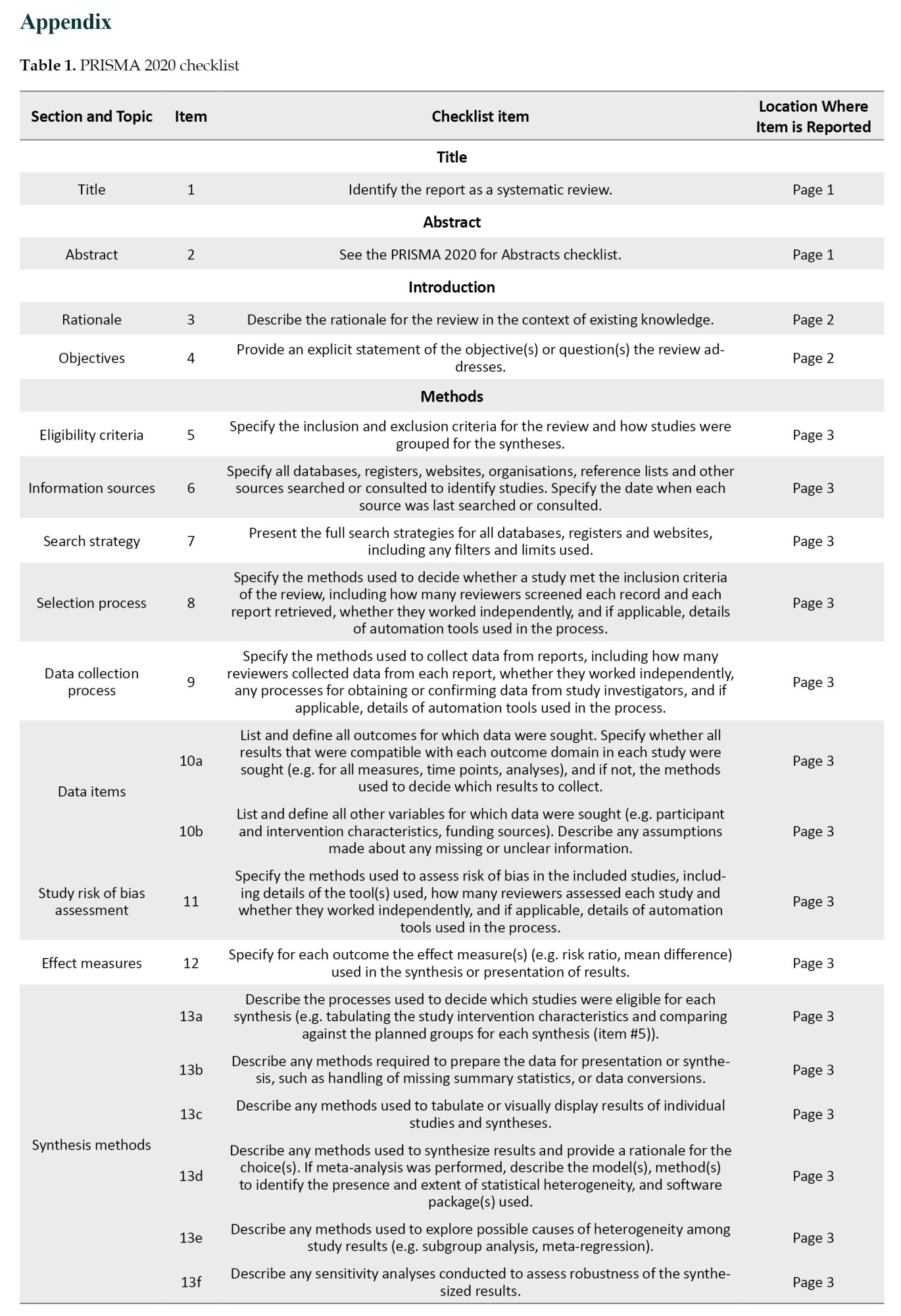
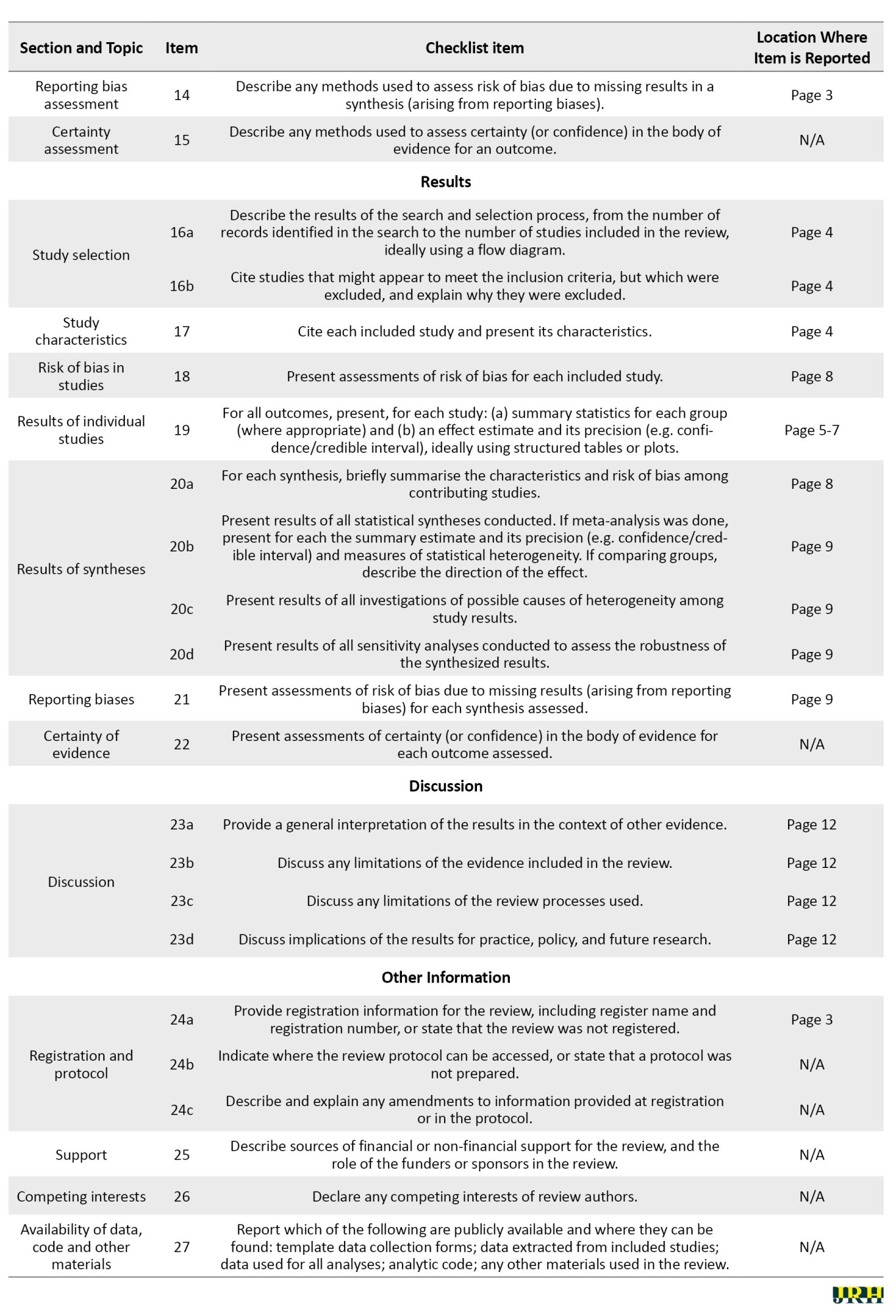
This systematic review was conducted and reported in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines (Appendix 1) [19].
Eligibility criteria
Studies were included based on the population, intervention, comparison, outcomes, and study design (PICOS) framework:
Population (P): Practicing nurses in any clinical setting. Intervention (I): Use of any AI-based tool (e.g. NLP, ML, and ASR) to support or automate nursing documentation. Comparison (C): Standard documentation workflows or pre-intervention conditions. Outcomes (O): Measures related to time management (e.g. documentation time, workload) and/or patient safety (e.g. documentation errors, quality metrics). Study Designs (S): Primary research studies, including randomized controlled trials (RCTs), non-randomized interventional studies, cohort studies, case-control studies, and cross-sectional studies.
Publications were excluded if they were reviews, editorials, conference abstracts, case reports, or non-empirical papers. Studies describing only the technical development of an AI tool without clinical evaluation were also excluded.
Information sources and search strategy
A systematic search was conducted in PubMed, Scopus, Web of Science, and Embase, with no date or language restrictions applied. To ensure comprehensive coverage, the search was supplemented by screening results from Google Scholar and by forward/backward citation tracking using Research Rabbit.
Study selection and data management
After removing duplicates using EndNote software, version 21, two authors independently screened all titles and abstracts on the Rayyan platform. The full texts of potentially eligible articles were subsequently reviewed for final inclusion. Disagreements at either stage were resolved through consensus discussion or, when necessary, adjudication by a third reviewer.
Data extraction and risk of bias assessment
Two reviewers independently extracted key data from included studies using a standardized form. Extracted fields included study characteristics, population, intervention details, and quantitative or qualitative outcomes relevant to the research questions. The risk of bias for each study was independently assessed by two reviewers using the appropriate Joanna Briggs institute (JBI) critical appraisal checklist for the study’s design [20].
Data synthesis
A quantitative meta-analysis was precluded by the significant heterogeneity observed across AI interventions, clinical settings, and outcome measures. Consequently, a narrative synthesis was employed to systematically integrate and interpret the findings from the included studies.
Results
Study selection
The initial database search yielded 2,052 records. After 826 duplicates were removed, the titles and abstracts of the remaining 1,226 records were screened. From this cohort, 1,003 records were excluded for not meeting the inclusion criteria. The full texts of the remaining 223 reports were searched for retrieval, of which 14 reports could not be found. Subsequently, the full texts of 209 reports were assessed for eligibility, and from this, 191 reports were excluded for reasons detailed in the PRISMA flow diagram (Figure 1).
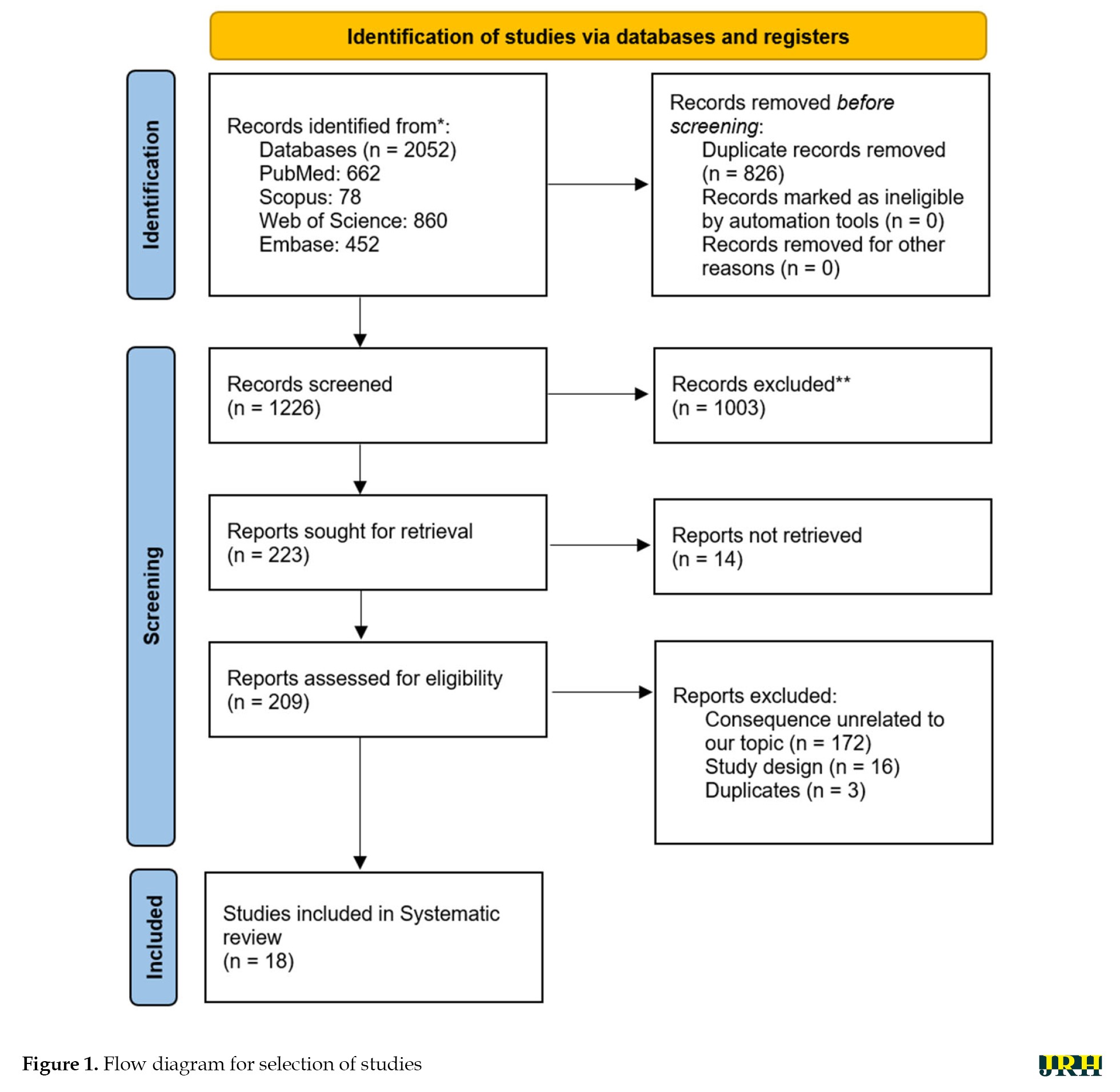 Ultimately, 18 studies met the eligibility criteria and were included in this narrative synthesis [16, 21-35].
Ultimately, 18 studies met the eligibility criteria and were included in this narrative synthesis [16, 21-35].
Characteristics of included studies
The 18 included studies, published between 2009 and 2025, represented a methodologically and geographically diverse body of evidence, as detailed in Table 1.
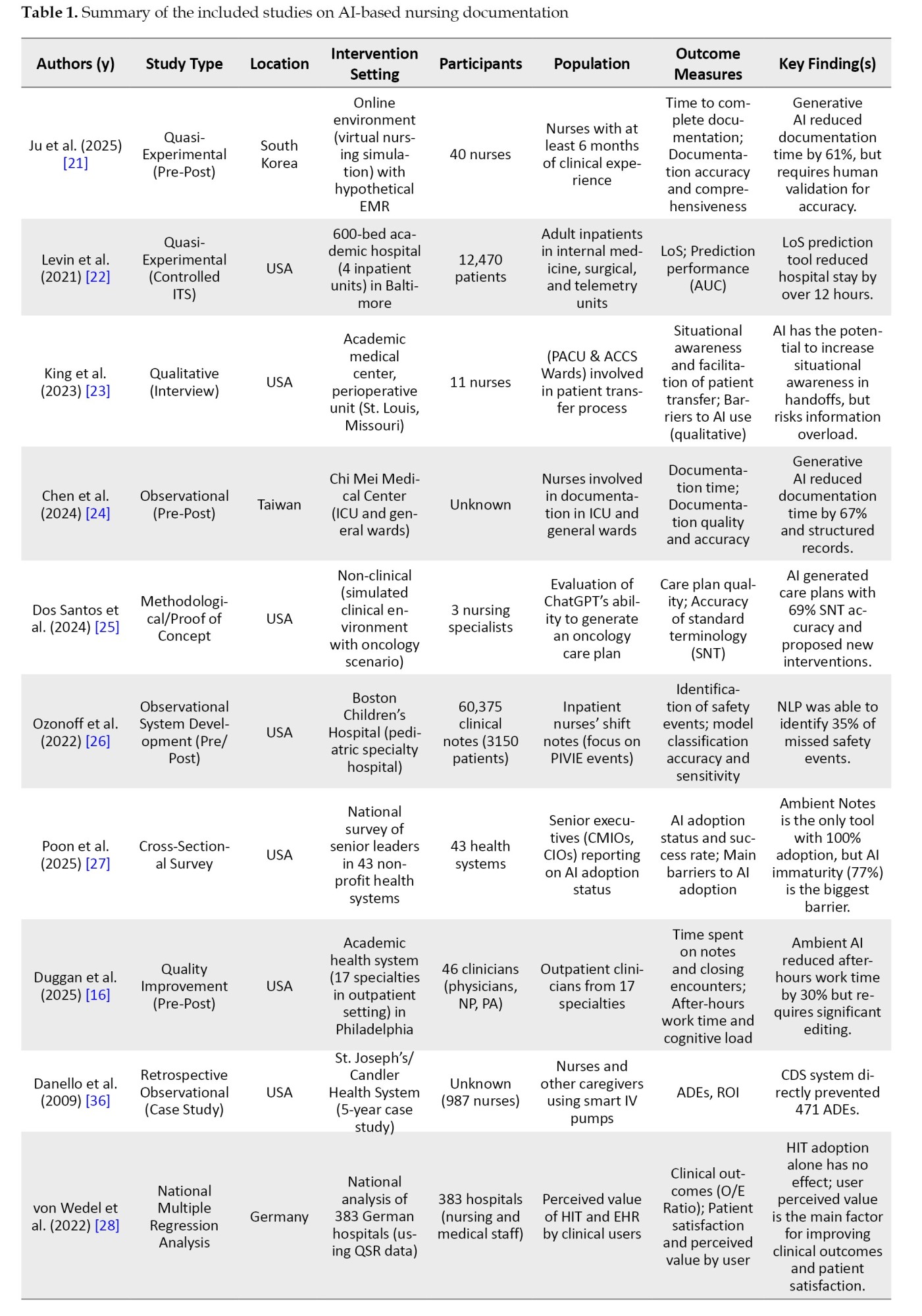
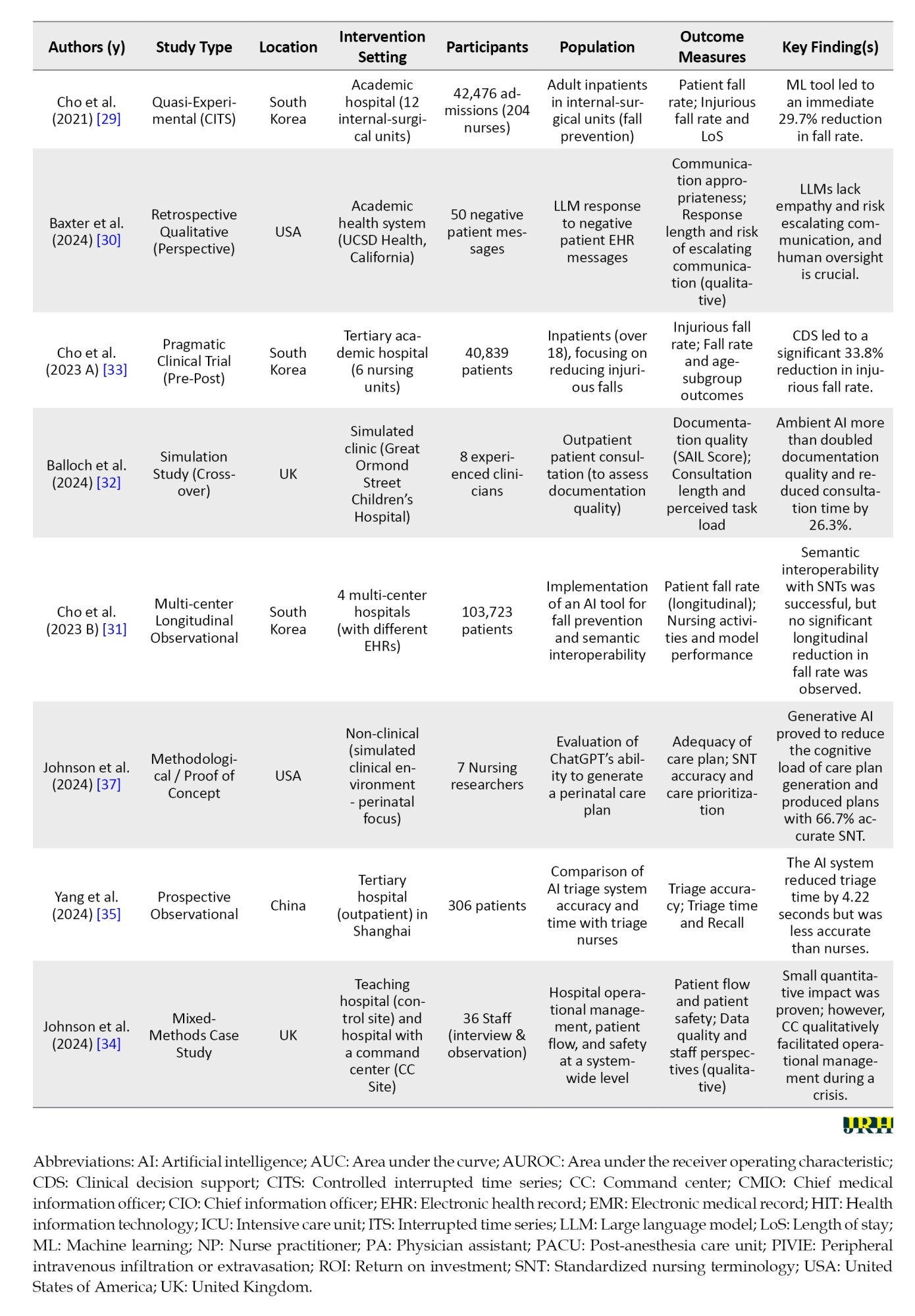
The studies were conducted across several countries, including the United States, South Korea, the United Kingdom, Germany, China, and Taiwan. Research designs were diverse, reflecting the nascent state of the field, and included quasi-experimental studies, practical trials, observational studies, qualitative studies, and proof-of-concept.
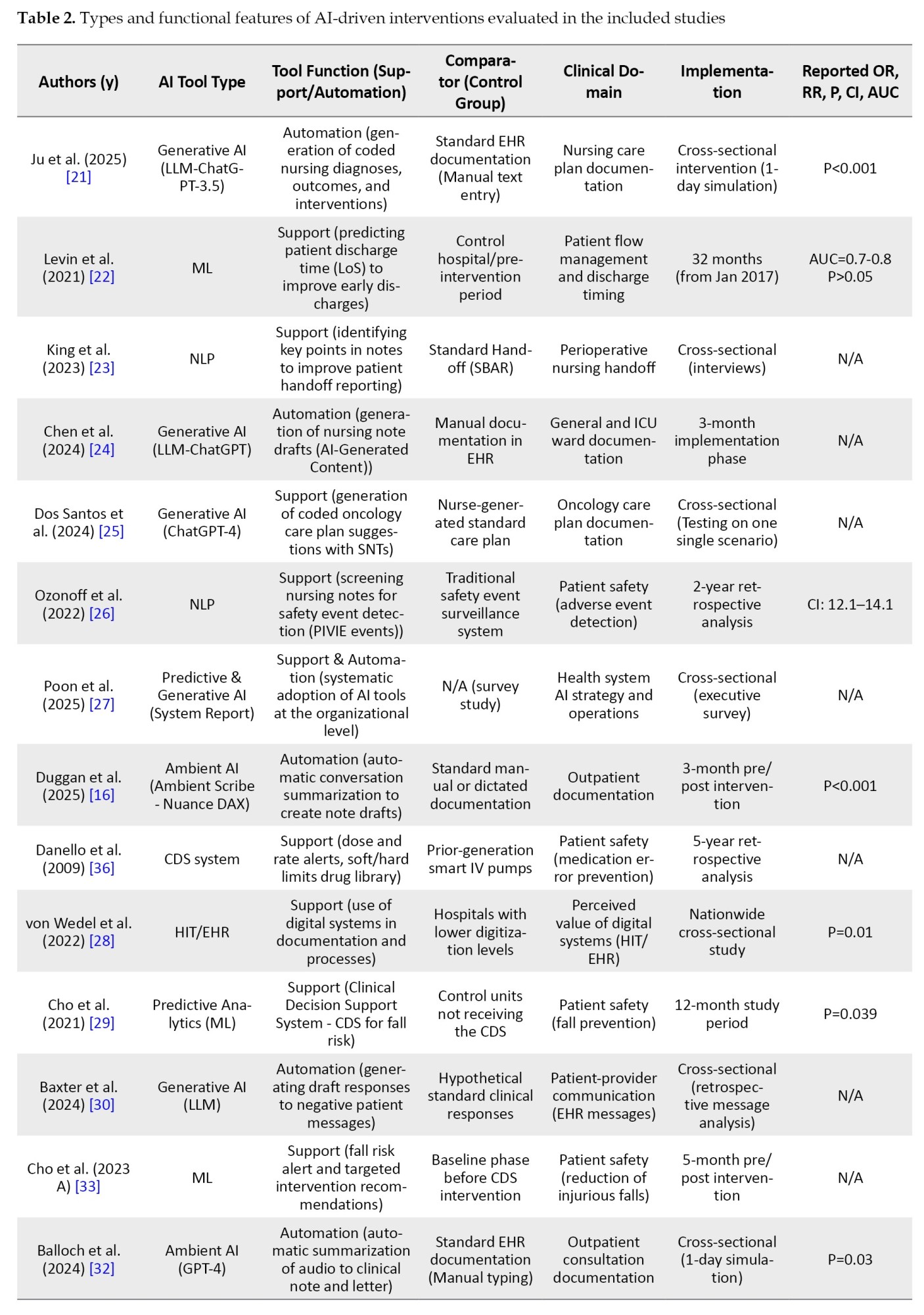
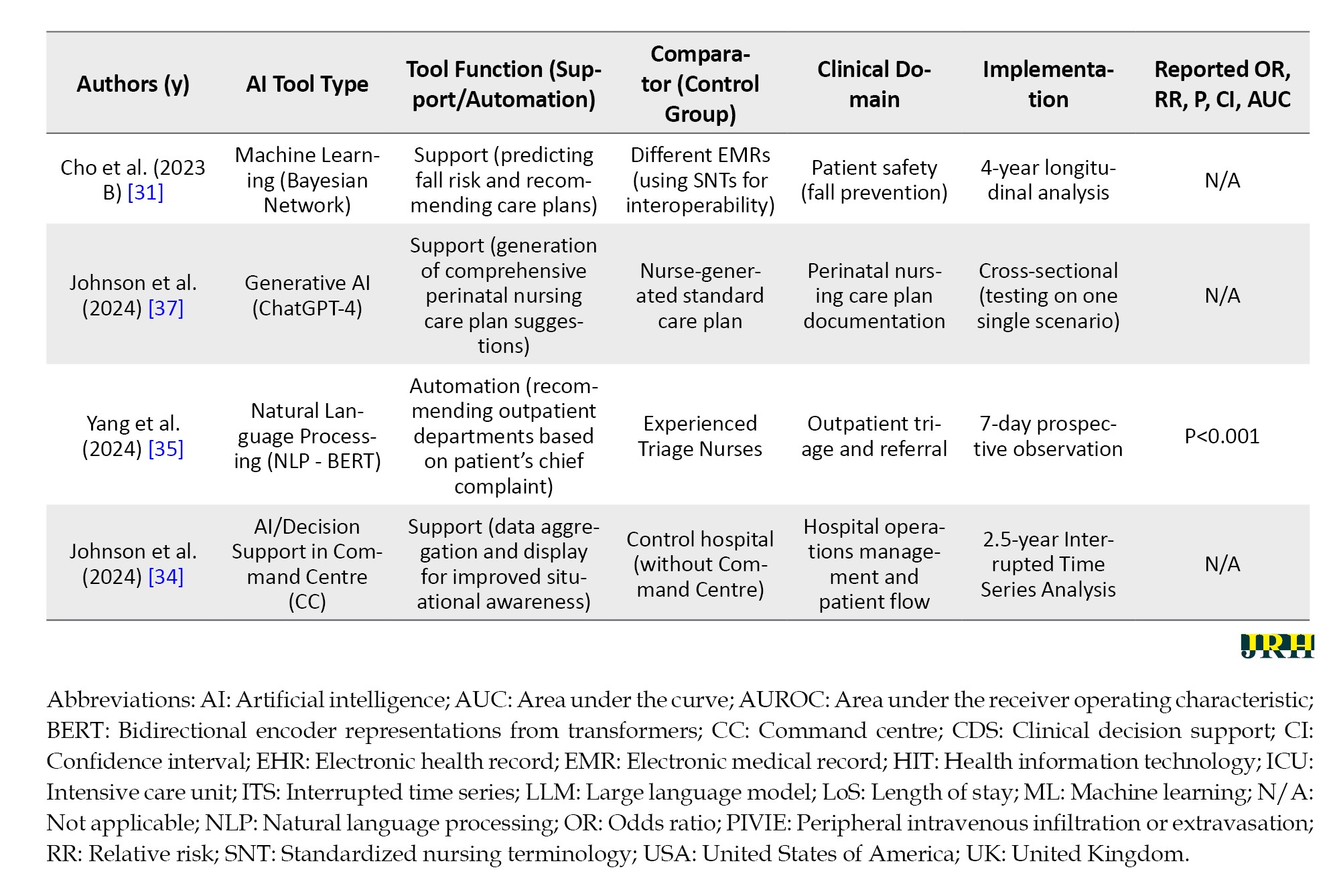
As shown in Table 1, study populations were heterogeneous, ranging from small, focused groups of nurses (e.g. n=11 in King, 2023 [23]) to large-scale analyses involving tens of thousands of patient records [22, 29]. The AI interventions examined were also diverse, spanning a spectrum from established decision support systems to cutting-edge generative AI, with the specific tool type for each study detailed in Table 2.
Risk of bias in the included studies
The methodological quality of the included studies was assessed to determine the risk of bias. Of the 18 studies included in this systematic review, 16 were critically appraised using the appropriate JBI critical appraisal checklist [20] corresponding to their respective study designs. For the remaining two studies, a suitable JBI checklist could not be identified; Consequently, their findings were reviewed with greater sensitivity and caution regarding their methodological limitations.
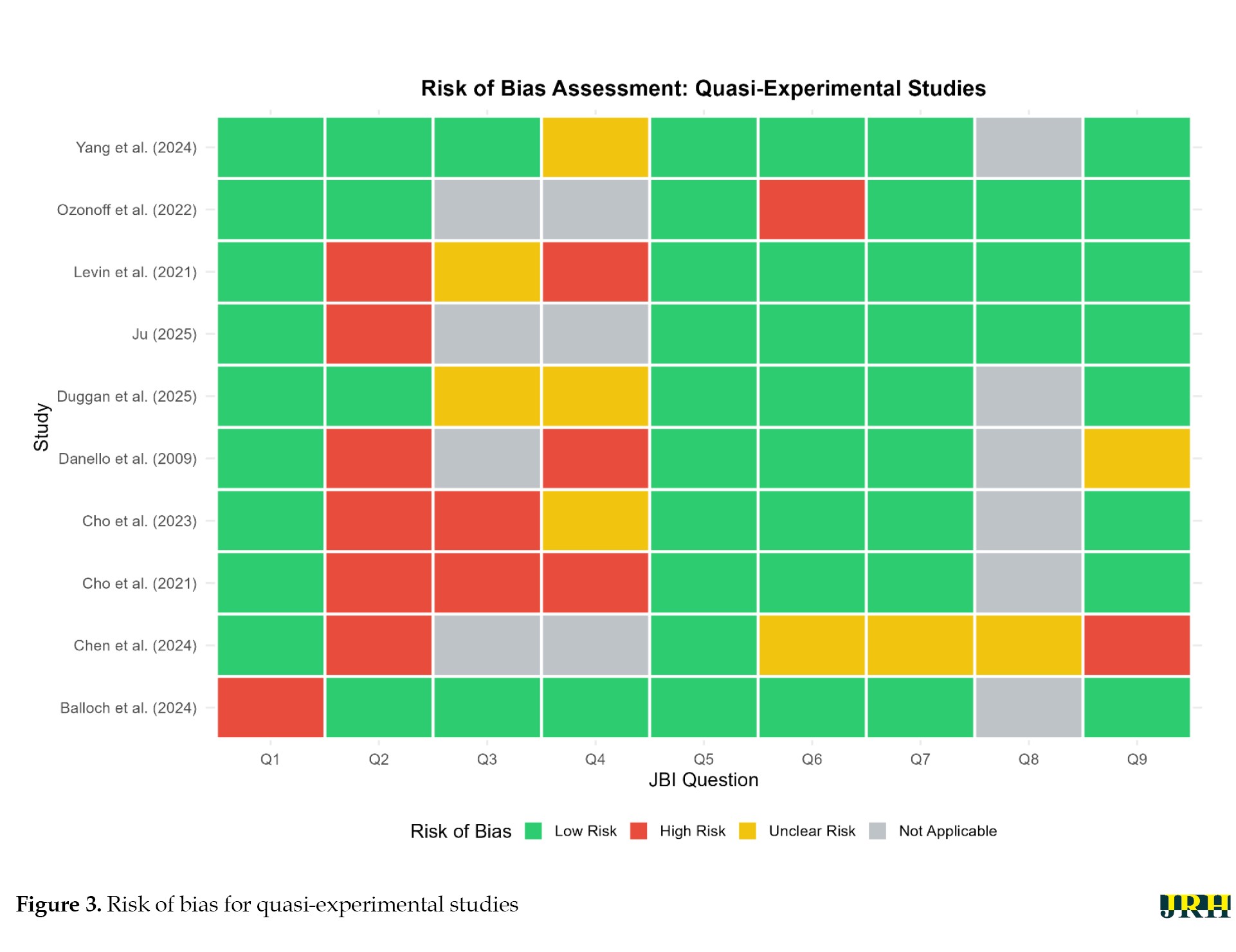
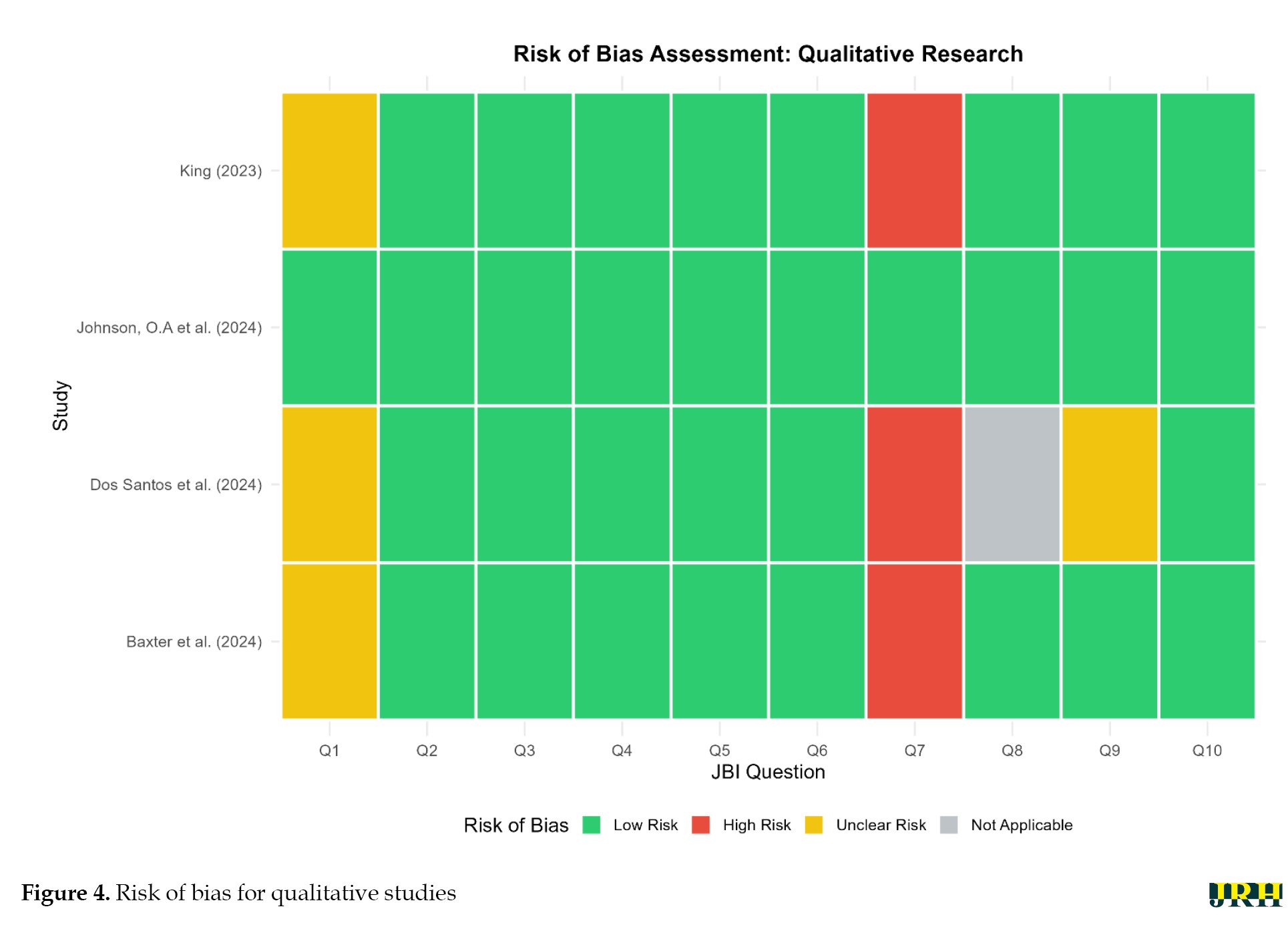
A summary of the risk of bias assessment for these studies, categorized by design, is presented in Figure 2 for cross-sectional, Figure 3 for quasi-experimental, and Figure 4 for qualitative studies.
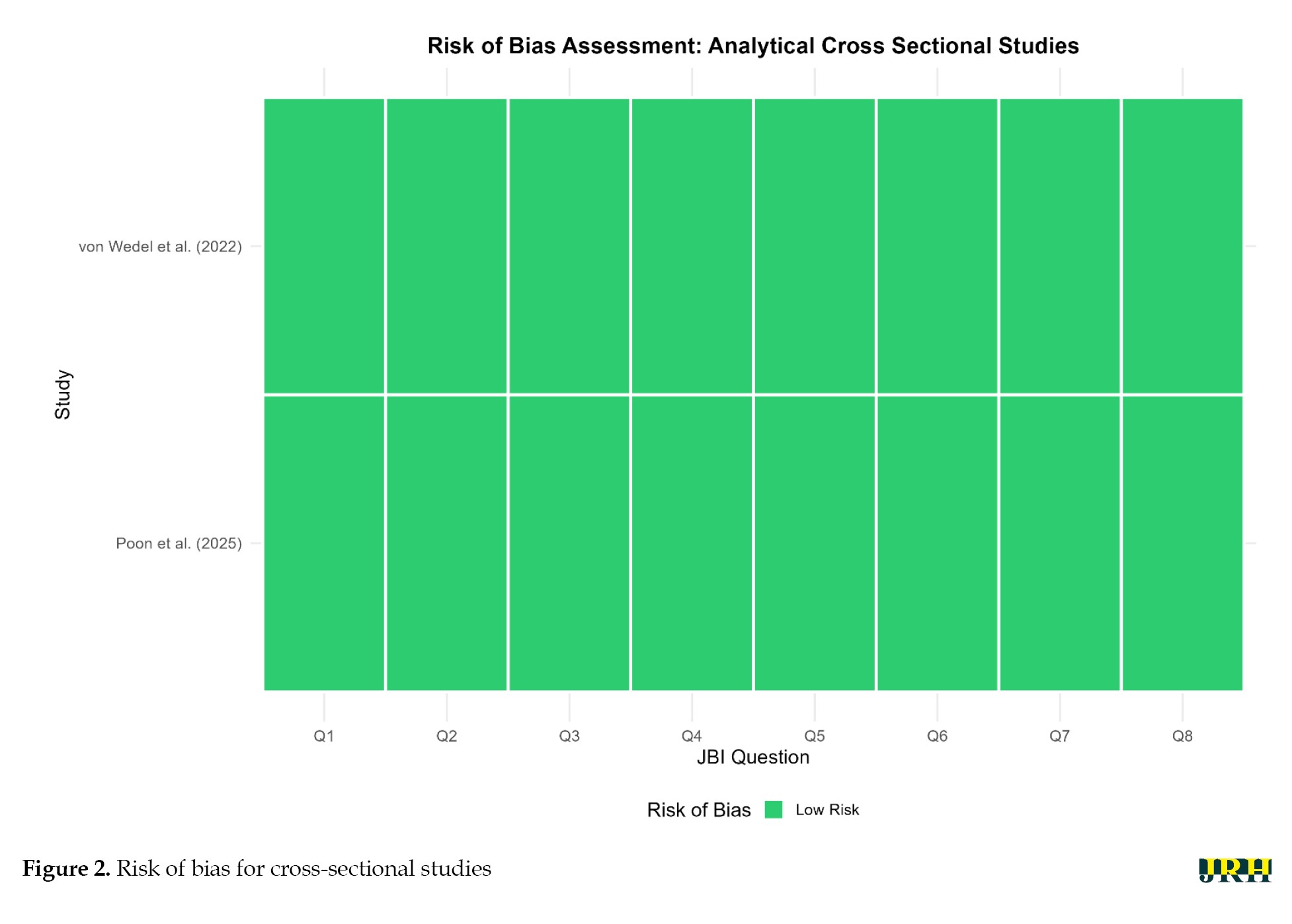
 A clear divergence in methodological rigor was observed across the different study designs. The two analytical cross-sectional studies [27, 28] were both assessed as having a low risk of bias across all applicable domains, indicating a high degree of methodological quality.
A clear divergence in methodological rigor was observed across the different study designs. The two analytical cross-sectional studies [27, 28] were both assessed as having a low risk of bias across all applicable domains, indicating a high degree of methodological quality.
The four qualitative studies demonstrated a generally low-to-moderate risk of bias. While strengths were noted, some domains presented potential for bias, with an unclear risk noted in Question 1 (Q1) and a high risk in Q7 for several studies [23, 25, 30].
The ten quasi-experimental studies represented the most methodologically heterogeneous group and contained the most significant potential for bias. High risks of bias were frequently identified in domains concerning participant allocation and control of confounding variables (notably Q2, Q3, and Q4). Furthermore, an unclear risk was common across domains related to follow-up and outcome measurement (Q6, Q7, and Q9). These limitations suggest that the evidence from this substantial portion of the included literature should be interpreted with considerable caution.
In summary, while the overall body of evidence provides valuable insights, the variable methodological quality, particularly within the quasi-experimental designs, underscores the need for careful consideration of the potential for bias when interpreting the findings of this review.
Synthesis of findings
The findings from the 18 included studies were synthesized into four main thematic areas: 1) impact on time management and efficiency, 2) impact on documentation quality, 3) impact on direct patient safety outcomes, and 4) the critical role of the human-in-the-loop and emergent risks.
Impact on time management and efficiency
One of the most consistent findings across the included literature was the potential for AI to significantly reduce the time spent on documentation and improve clinical efficiency. As synthesized in Table 3, studies utilizing generative AI or ambient scribe technology reported substantial time savings.
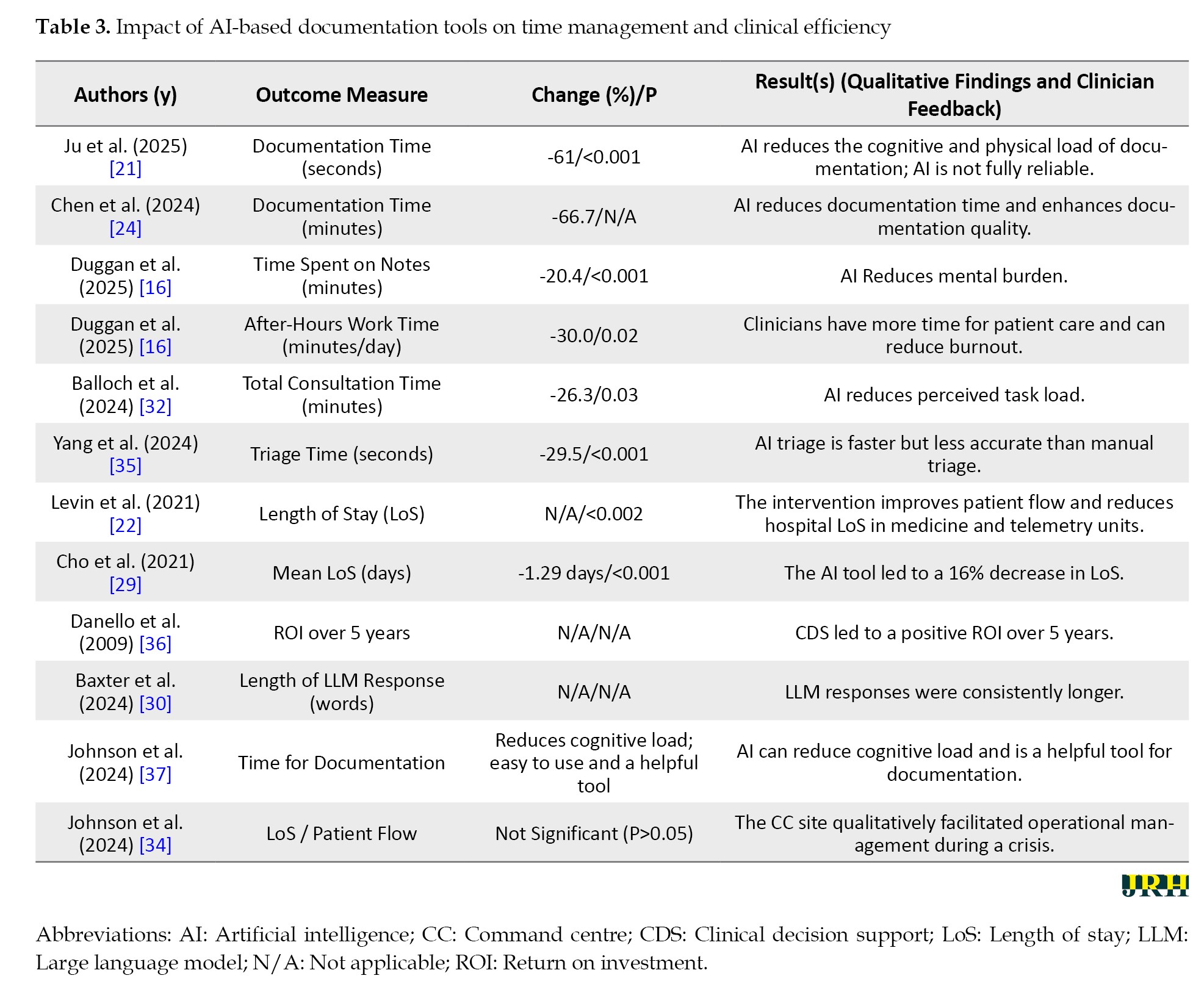
For instance, Ju et al. demonstrated an approximate 61% reduction in documentation time (from 467 to 183 seconds, P<0.001), while Chen et al. reduced this time from 15 to approximately 5 minutes per patient. Similarly, Duggan et al. observed a 20.4% decrease in time spent in notes and a 30% reduction in after-hours work (P=0.02), and Balloch et al. found that AI-assisted consultations were 26.3% shorter (P=0.03) [16, 21, 24, 32].
These benefits extended beyond note-writing to system-level efficiency. As shown in Table 3, predictive AI tools were associated with significant reductions in patient length of stay [22, 29] and expedited clinical processes, like outpatient triage [35]. However, this time-saving effect was not absolute. Qualitative findings from several studies [16, 30] revealed that the time saved in initial content generation was often reallocated to the critical task of reviewing and editing the AI output to ensure clinical accuracy and safety [16, 22, 29, 30, 35].
Impact on documentation quality
A second major theme was the capacity of AI to enhance the quality and completeness of clinical documentation. Evidence for this is summarized in Table 4.
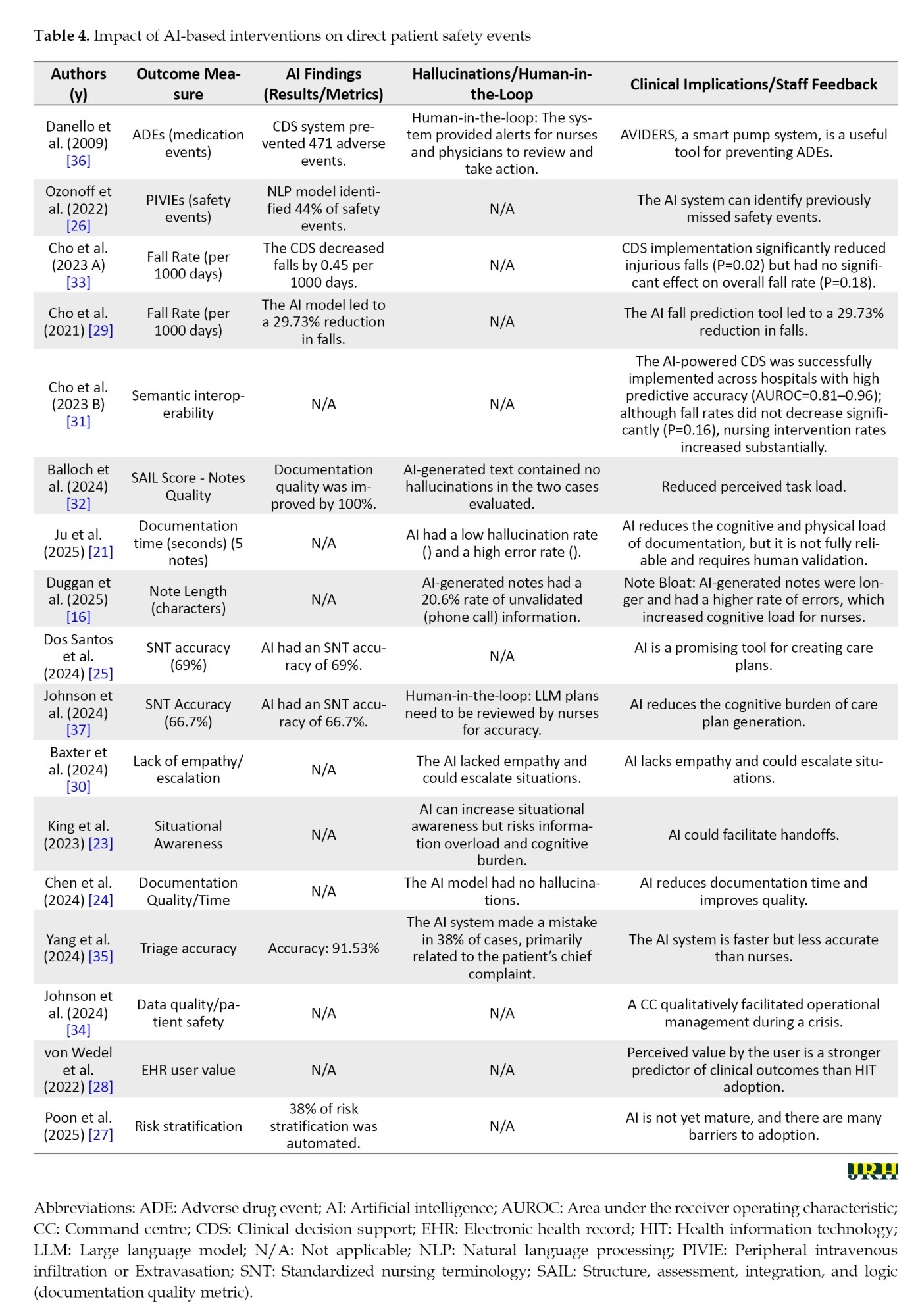
A simulation study by Balloch et al. provided compelling quantitative data, with 100% of AI-generated clinical notes receiving a “good/very good” score on the validated SAIL instrument, compared to only 43% of manually written notes (P=0.004) [32].
Proof-of-concept studies, also detailed in Table 4, demonstrated this potential as well. AI-generated care plans were found to be not only comparable to those created by expert nurses, but in some cases, enhanced them by providing additional relevant interventions [25, 34]. This was supported by findings of increased overall note length and completeness [16]. However, this improvement in structural quality was coupled with concerns about content accuracy. Both Dos Santos et al. and Johnson et al. found that AI correctly used standard nursing terminologies in only about two-thirds of instances. Qualitative feedback from clinicians consistently emphasized the need for significant editing to correct factual errors and refine clinical nuances [25, 37].
Impact on direct patient safety events
The direct impact of AI on patient safety events, detailed in Table 4, was complex and context-dependent. Decision support systems targeting specific risks showed clear benefits. The study by Danello et al. on smart IV pumps reported the prevention of at least 471 adverse drug events over five years. Similarly, an NLP-based tool developed by Ozonoff et al. was able to identify 44% of safety events that were missed by the hospital’s existing reporting systems [26, 36].
Conversely, evidence regarding patient fall prevention, a key nursing-sensitive indicator, was contradictory. An early controlled study showed an immediate 29.7% reduction in the overall fall rate after AI implementation [29], and a subsequent pragmatic trial reported a significant reduction in injurious falls (P=0.0171) even if the overall fall rate did not change [33]. However, a large, multi-center implementation study found no significant long-term change in fall rates [31]. Furthermore, a large study of an AI-powered hospital command center found no discernible impact on macro-level safety indicators, like mortality or readmission rates [34], suggesting that the effectiveness of AI is highly contingent on the clinical context and the specific safety outcome being measured.
The role of the human user and emerging risks
A critical theme that emerged from the synthesis is that AI in nursing documentation functions as a powerful tool, not an autonomous agent. This highlights both the irreplaceable role of the clinician and the new risks introduced by the technology itself. The study by Baxter et al. [30] provided a cautionary illustration of these risks. When a generative AI was used to draft responses to patient messages, it not only lacked empathy but dangerously suggested a patient file a formal complaint against their physician, revealing the potential to harm the therapeutic relationship and create medico-legal issues. As noted across multiple studies [24, 32], this risk of generating false or inappropriate content, often termed “hallucination,” underscores the non-negotiable need for human clinical judgment to review, edit, and validate all AI-generated outputs before they enter the official patient record.
Finally, the effectiveness of any AI tool was intrinsically linked to its integration into the clinical workflow and its acceptance by end-users. A large national study in Germany by von Wedel et al. concluded that positive clinical outcomes did not correlate with the mere adoption of technology, but rather with its “user-perceived value.” This finding underscores the paramount importance of user-centered design and ensuring that AI tools support, rather than disrupt, the complex cognitive work of nurses [28].
Discussion
This systematic review synthesized evidence from 18 included studies on the impact of diverse AI technologies on nursing documentation, focusing on the dual outcomes of time management and patient safety. Our findings revealed a rapidly innovating field with promising initial results, yet one simultaneously marked by significant methodological heterogeneity and the emergence of critical socio-technical challenges. The principal findings of this review can be organized into four core themes:
Efficiency and time management: A paradigm shift from creation to curation
AI interventions, particularly generative and ambient scribe technologies, consistently demonstrate the potential to alleviate the clinical administrative burden. Our synthesis quantitatively confirms that AI can substantially reduce time spent on documentation, with simulation studies reporting reductions exceeding 60% [21]. Furthermore, in real-world outpatient settings, time spent in notes decreased by 20.4%, and significant relief was found in “after-hours work time” (Pajama Time), which saw a reduction of 30.0% [16]. These findings strongly support the primary hypothesis that AI can liberate nursing time for direct patient interaction and theoretically mitigate clinician burnout.
However, a crucial finding is that this time-saving is not absolute. The “raw output” generated by AI consistently requires meticulous human review, editing, and clinical validation. Qualitative feedback indicates that time reallocated to editing inaccuracies, correcting factual errors, and adding clinical nuance can sometimes equate to or even outweigh the time initially saved in content generation [16]. This mandates a reframing of the net impact on time: AI drives a strategic shift in clinical workload from content creation to content curation.
Patient safety: Bifurcated impact and the emergence of new risks
The impact of AI on patient safety is complex and multifactorial, lacking uniform positivity. Our analysis identified three distinct pathways of influence:
Direct safety improvement (hard outcomes): Certain AI tools designed to target specific, measurable risks demonstrated clear, quantifiable safety gains. This includes decision support systems (CDS), like smart IV pumps, which objectively averted ≥471 preventable adverse drug events (ADEs) over five years [36]. Similarly, NLP successfully identified 35% of safety events, potentially identifiable and preventable inpatient safety events (PIVIEs) missed by conventional hospital reporting systems [26].
Indirect safety improvement via documentation quality: Studies involving generative AI often linked potential safety improvements to enhancements in documentation quality. AI tools demonstrated an ability to generate notes that were more structured, comprehensive [24], and adhered better to standardized nursing terminologies (SNTs), albeit imperfectly [25, 34]. The implicit mechanism is that better data quality supports clearer communication and safer care.
Emergence of novel safety risks: Critically, our review highlights that AI introduces new vectors for patient harm. The risk of AI “hallucinations” (factual inaccuracies) was noted even in controlled environments [21, 32]. More concerningly, LLMs demonstrated potential for severe socio-technical harm, generating responses to patient messages that lacked empathy and carried the risk of escalation, even suggesting filing formal complaints [30]. This complexity strongly reinforces the non-negotiable need for robust “human-in-the-loop” protocols to manage the intersection of AI capabilities and clinical responsibility.
Methodological landscape: The critical need for rigor
The evidence base supporting AI in nursing documentation remains nascent. The included studies were predominantly limited to quasi-experimental pre-post designs or simulation/qualitative approaches. While valuable for initial evaluation and hypothesis generation [23], this heterogeneity prevented a quantitative meta-analysis on efficiency outcomes and limits the ability to draw firm causal conclusions.
A key limitation is the inconsistency in findings regarding the strongest clinical outcome, fall prevention. While some studies reported immediate success [29]. Cho et al. reported a 29.7% immediate fall reduction, a larger longitudinal implementation failed to detect a sustained, significant decrease in the overall fall rate [31]. This lack of definitive evidence underscores a critical need for more methodologically rigorous designs, particularly well-executed controlled interrupted time series (CITS) and RCTs, to confidently attribute observed gains to the intervention rather than confounding factors.
Implementation success: The socio-technical imperative
Our findings suggest that the successful integration of AI is not purely a technical exercise but a socio-technical challenge. The national analysis by von Wedel et al. was particularly insightful, concluding that clinical benefits were correlated not merely with technology adoption, but strongly with the “user-perceived value” of the installed systems (β=−0.138) [28].
This reinforces the importance of human factors. Qualitative data highlighted that poor system design can lead to alarm fatigue [23] or create a negative organizational culture where front-line staff feel “monitored” [34]. Therefore, effective AI integration must prioritize user-centered design and maintain the centrality of human clinical judgment and professional autonomy. The transition of the nurse’s role from content creator to critical curator demands comprehensive training and a governance framework that empowers clinicians to support, not override, AI-generated recommendations.
Conclusion
The collective evidence demonstrates that AI-based documentation tools markedly improve time efficiency and workflow optimization across multiple clinical contexts. Most studies reported substantial reductions in documentation time, ranging from 20 % to over 60 %, as well as meaningful decreases in after-hours work and clinician cognitive burden. These time savings translate into improved patient flow, shorter length of stay, and enhanced opportunities for direct patient interaction. However, qualitative findings consistently emphasize that while AI systems significantly reduce the physical and mental load of documentation, they are not yet fully reliable for unsupervised clinical use. Therefore, the optimal integration of such systems requires human oversight and post-AI editing to ensure clinical accuracy, contextual relevance, and patient safety. In summary, AI holds clear potential to transform documentation efficiency and mitigate burnout, but sustained clinician engagement and rigorous validation are essential to achieve trustworthy, safe, and equitable implementation in healthcare settings.
Limitations
This systematic review is subject to several methodological and practical limitations that should be considered when interpreting the findings. First, the primary constraint was the methodological immaturity and inherent heterogeneity across the included studies. The predominance of quasi-experimental (pre-post) designs, single-center trials, and simulation-based studies limits the ability to draw firm causal conclusions regarding the net impact of AI on patient care. Specifically, the high variability in AI technologies, patient populations, and inconsistent reporting of quantitative outcomes precluded a formal statistical meta-analysis of time-related endpoints.
Second, the generalizability (external validity) of the findings is constrained. Many of the studies evaluating efficiency gains were conducted at a single site or focused on niche populations, often relying on institution-specific EHR configurations. Furthermore, the reliance on simulation and proof-of-concept designs means that the full spectrum of operational and socio-technical challenges encountered in real-world clinical deployment may be underestimated.
Third, the review’s scope was limited to formally published literature, meaning that relevant “grey literature” (e.g. technical reports, internal health system evaluations, or conference proceedings) that might contain valuable early evidence or operational insights could have been inadvertently missed.
Finally, the rapid pace of AI development, particularly within generative and ambient technologies, means that the evidence base is constantly and quickly evolving. The findings represent a snapshot in time and should be continuously evaluated against emerging technological capabilities and new implementation data.
Challenges and future works
Despite the accelerating integration of AI into nursing documentation, several challenges remain unresolved. Data heterogeneity, limited interoperability across EHR systems, and inconsistent use of SNTs continue to constrain model performance and generalizability. Future research should prioritize the development of unified data frameworks and advanced natural language processing pipelines capable of handling multilingual and context-dependent nursing language. Another critical challenge is ensuring clinical validity and trustworthiness: AI-generated documentation must be continuously validated through rigorous human-in-the-loop evaluation and transparent auditing to prevent misinformation and safeguard patient safety. The ethical and legal dimensions of AI use, particularly data privacy, algorithmic bias, and accountability, demand clear governance policies and interdisciplinary oversight. Finally, large, multi-center pragmatic trials are needed to evaluate the long-term impact of AI-assisted documentation on efficiency, patient outcomes, and clinician well-being, with special emphasis on user-centered design and real-world implementation science. Only through addressing these challenges can AI tools move from promising prototypes to reliable clinical companions in nursing practice.
Ethical Considerations
Compliance with ethical guidelines
This systematic review was conducted in accordance with established academic and ethical standards. As the work synthesized data solely from publicly available published studies and did not involve new data collection or patient/clinical interventions, Institutional Review Board (IRB) approval and participant consent were not required. The review protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) (Code: CRD420251089257). Reporting followed the PRISMA 2020 Statement to ensure clarity, reproducibility, and full disclosure of the review process.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, investigation and writing of the original draft: Arash Amadeh Taheri and Ghazaleh Afkhami Teimouri; Methodology: Yasamin Moeinipour and Arash Amadeh Taheri; Data collection: Yasamin Moeinipour, Arash Amadeh Taheri and Ghazaleh Afkhami Teimouri; Review, and editing: Yasamin Moeinipour and Fatemeh Bagheri; Supervision: Malihe Adineh Fathabadi; Project Administration: Arash Amadeh Taheri.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all individuals who contributed to this study through informal discussions or technical support but did not meet the criteria for authorship.
References
The documentation of uniform nursing practices is characterized by prompt, accurate, and consistent documentation of evaluation, diagnosis, treatment strategies, interventions, and outcomes throughout the nursing process. Empirical evidence suggests that, in addition to continuity of care, there is a direct correlation between the caliber of such documentation and the overall quality and safety of care [1]. From a quality and safety point of view, the introduction of organized electronic frameworks increases the accuracy of the content and usability of the data, which is correlated with a reduction in document inaccuracies and a positive progress in patient safety indicators [2, 3]. The nursing dossier serves as a fundamental framework for patient-oriented, safe, and effective care, and dedicating resources to standardization, improving quality, and further utilizing its data significantly enhances both clinical and administrative outcomes [4].
Despite its foundational role, clinical documentation in practice has become a “hidden burden” for nurses. With the implementation of electronic health records (EHRs), the volume and complexity of documentation tasks have significantly increased, consuming a substantial portion of a nurse’s shift. Time allocation studies reveal that nurses spend between 25% and 35.3% of their work time on documentation [5, 6], time that could otherwise be dedicated to direct patient care, education, and support. In the health informatics literature, this phenomenon has been framed as the “documentation burden.” This added load is also linked to adverse psychological and professional outcomes. Research has demonstrated a correlation between high documentation volume and inefficient or unusable EHRs with factors, such as emotional exhaustion and depersonalization, which contribute to burnout [7, 8]. Furthermore, documentation processes are inherently susceptible to human errors from incomplete or incorrect medication records to omissions and delays in documenting vital signs that can lead to flawed clinical decision-making and adverse events [3].
In response to the dual challenges of the “documentation time burden” and associated “safety risks,” artificial intelligence (AI) has emerged as a transformative solution. Three key branches, automatic speech recognition (ASR), natural language processing (NLP), and machine learning (ML), can optimize the documentation loop from “clinical dialogue” to “structured note,” restoring time for direct patient interaction through intelligent automation. In the NLP domain, systematic and integrative reviews have shown that extracting critical components from unstructured nursing notes is reliable for decision support, trend identification, and predicting high-risk events, like patient falls [9, 10]. Moreover, combining emergency department nursing texts with structured data in ML models has facilitated the early detection of critical conditions, such as sepsis, and enhanced the efficacy of early warning systems [11]. At the same time, field experiences with ASR serve as a reminder that automated documentation without review may be prone to transcriptional and conceptual errors. Therefore, a “human-in-the-loop” approach and quality assurance procedures are vital for ensuring the safety and accuracy of records [12, 13]. Collectively, this body of evidence suggests that the targeted application of AI can significantly enhance documentation efficiency while also contributing to patient safety by reducing burnout and improving data quality, provided it is designed responsibly and its clinical outcomes are continuously evaluated [14-18].
In recent years, a growing number of studies have investigated the application of these technologies in clinical settings. Despite promising results, the existing evidence in this field is highly scattered, heterogeneous, and in the early stages of maturity. Many of these studies are small-scale, single-center, and employ quasi-experimental designs, which carry a high potential for bias and limit the generalizability of their findings. There is also considerable heterogeneity in the types of technology used, patient populations, clinical settings, and outcome measures evaluated. This diversity makes it difficult to synthesize the evidence and draw definitive conclusions about the overall effectiveness of these interventions.
Consequently, this systematic review aimed to address this evidence gap and the heterogeneity of existing results by synthesizing the effect of AI-driven interventions in nursing documentation on two key outcomes: time management and patient safety. This study will provide practical, evidence-based recommendations for administrators, policymakers, clinical nurses, and technology developers, an action that is of strategic importance given the increasing investments by healthcare systems in digital health and artificial intelligence.
Methods
Protocol and registration
This systematic review was conducted and reported in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines (Appendix 1) [19].
Eligibility criteria
Studies were included based on the population, intervention, comparison, outcomes, and study design (PICOS) framework:
Population (P): Practicing nurses in any clinical setting. Intervention (I): Use of any AI-based tool (e.g. NLP, ML, and ASR) to support or automate nursing documentation. Comparison (C): Standard documentation workflows or pre-intervention conditions. Outcomes (O): Measures related to time management (e.g. documentation time, workload) and/or patient safety (e.g. documentation errors, quality metrics). Study Designs (S): Primary research studies, including randomized controlled trials (RCTs), non-randomized interventional studies, cohort studies, case-control studies, and cross-sectional studies.
Publications were excluded if they were reviews, editorials, conference abstracts, case reports, or non-empirical papers. Studies describing only the technical development of an AI tool without clinical evaluation were also excluded.
Information sources and search strategy
A systematic search was conducted in PubMed, Scopus, Web of Science, and Embase, with no date or language restrictions applied. To ensure comprehensive coverage, the search was supplemented by screening results from Google Scholar and by forward/backward citation tracking using Research Rabbit.
Study selection and data management
After removing duplicates using EndNote software, version 21, two authors independently screened all titles and abstracts on the Rayyan platform. The full texts of potentially eligible articles were subsequently reviewed for final inclusion. Disagreements at either stage were resolved through consensus discussion or, when necessary, adjudication by a third reviewer.
Data extraction and risk of bias assessment
Two reviewers independently extracted key data from included studies using a standardized form. Extracted fields included study characteristics, population, intervention details, and quantitative or qualitative outcomes relevant to the research questions. The risk of bias for each study was independently assessed by two reviewers using the appropriate Joanna Briggs institute (JBI) critical appraisal checklist for the study’s design [20].
Data synthesis
A quantitative meta-analysis was precluded by the significant heterogeneity observed across AI interventions, clinical settings, and outcome measures. Consequently, a narrative synthesis was employed to systematically integrate and interpret the findings from the included studies.
Results
Study selection
The initial database search yielded 2,052 records. After 826 duplicates were removed, the titles and abstracts of the remaining 1,226 records were screened. From this cohort, 1,003 records were excluded for not meeting the inclusion criteria. The full texts of the remaining 223 reports were searched for retrieval, of which 14 reports could not be found. Subsequently, the full texts of 209 reports were assessed for eligibility, and from this, 191 reports were excluded for reasons detailed in the PRISMA flow diagram (Figure 1).
Characteristics of included studies
The 18 included studies, published between 2009 and 2025, represented a methodologically and geographically diverse body of evidence, as detailed in Table 1.
The studies were conducted across several countries, including the United States, South Korea, the United Kingdom, Germany, China, and Taiwan. Research designs were diverse, reflecting the nascent state of the field, and included quasi-experimental studies, practical trials, observational studies, qualitative studies, and proof-of-concept.
As shown in Table 1, study populations were heterogeneous, ranging from small, focused groups of nurses (e.g. n=11 in King, 2023 [23]) to large-scale analyses involving tens of thousands of patient records [22, 29]. The AI interventions examined were also diverse, spanning a spectrum from established decision support systems to cutting-edge generative AI, with the specific tool type for each study detailed in Table 2.
Risk of bias in the included studies
The methodological quality of the included studies was assessed to determine the risk of bias. Of the 18 studies included in this systematic review, 16 were critically appraised using the appropriate JBI critical appraisal checklist [20] corresponding to their respective study designs. For the remaining two studies, a suitable JBI checklist could not be identified; Consequently, their findings were reviewed with greater sensitivity and caution regarding their methodological limitations.
A summary of the risk of bias assessment for these studies, categorized by design, is presented in Figure 2 for cross-sectional, Figure 3 for quasi-experimental, and Figure 4 for qualitative studies.
The four qualitative studies demonstrated a generally low-to-moderate risk of bias. While strengths were noted, some domains presented potential for bias, with an unclear risk noted in Question 1 (Q1) and a high risk in Q7 for several studies [23, 25, 30].
The ten quasi-experimental studies represented the most methodologically heterogeneous group and contained the most significant potential for bias. High risks of bias were frequently identified in domains concerning participant allocation and control of confounding variables (notably Q2, Q3, and Q4). Furthermore, an unclear risk was common across domains related to follow-up and outcome measurement (Q6, Q7, and Q9). These limitations suggest that the evidence from this substantial portion of the included literature should be interpreted with considerable caution.
In summary, while the overall body of evidence provides valuable insights, the variable methodological quality, particularly within the quasi-experimental designs, underscores the need for careful consideration of the potential for bias when interpreting the findings of this review.
Synthesis of findings
The findings from the 18 included studies were synthesized into four main thematic areas: 1) impact on time management and efficiency, 2) impact on documentation quality, 3) impact on direct patient safety outcomes, and 4) the critical role of the human-in-the-loop and emergent risks.
Impact on time management and efficiency
One of the most consistent findings across the included literature was the potential for AI to significantly reduce the time spent on documentation and improve clinical efficiency. As synthesized in Table 3, studies utilizing generative AI or ambient scribe technology reported substantial time savings.
For instance, Ju et al. demonstrated an approximate 61% reduction in documentation time (from 467 to 183 seconds, P<0.001), while Chen et al. reduced this time from 15 to approximately 5 minutes per patient. Similarly, Duggan et al. observed a 20.4% decrease in time spent in notes and a 30% reduction in after-hours work (P=0.02), and Balloch et al. found that AI-assisted consultations were 26.3% shorter (P=0.03) [16, 21, 24, 32].
These benefits extended beyond note-writing to system-level efficiency. As shown in Table 3, predictive AI tools were associated with significant reductions in patient length of stay [22, 29] and expedited clinical processes, like outpatient triage [35]. However, this time-saving effect was not absolute. Qualitative findings from several studies [16, 30] revealed that the time saved in initial content generation was often reallocated to the critical task of reviewing and editing the AI output to ensure clinical accuracy and safety [16, 22, 29, 30, 35].
Impact on documentation quality
A second major theme was the capacity of AI to enhance the quality and completeness of clinical documentation. Evidence for this is summarized in Table 4.
A simulation study by Balloch et al. provided compelling quantitative data, with 100% of AI-generated clinical notes receiving a “good/very good” score on the validated SAIL instrument, compared to only 43% of manually written notes (P=0.004) [32].
Proof-of-concept studies, also detailed in Table 4, demonstrated this potential as well. AI-generated care plans were found to be not only comparable to those created by expert nurses, but in some cases, enhanced them by providing additional relevant interventions [25, 34]. This was supported by findings of increased overall note length and completeness [16]. However, this improvement in structural quality was coupled with concerns about content accuracy. Both Dos Santos et al. and Johnson et al. found that AI correctly used standard nursing terminologies in only about two-thirds of instances. Qualitative feedback from clinicians consistently emphasized the need for significant editing to correct factual errors and refine clinical nuances [25, 37].
Impact on direct patient safety events
The direct impact of AI on patient safety events, detailed in Table 4, was complex and context-dependent. Decision support systems targeting specific risks showed clear benefits. The study by Danello et al. on smart IV pumps reported the prevention of at least 471 adverse drug events over five years. Similarly, an NLP-based tool developed by Ozonoff et al. was able to identify 44% of safety events that were missed by the hospital’s existing reporting systems [26, 36].
Conversely, evidence regarding patient fall prevention, a key nursing-sensitive indicator, was contradictory. An early controlled study showed an immediate 29.7% reduction in the overall fall rate after AI implementation [29], and a subsequent pragmatic trial reported a significant reduction in injurious falls (P=0.0171) even if the overall fall rate did not change [33]. However, a large, multi-center implementation study found no significant long-term change in fall rates [31]. Furthermore, a large study of an AI-powered hospital command center found no discernible impact on macro-level safety indicators, like mortality or readmission rates [34], suggesting that the effectiveness of AI is highly contingent on the clinical context and the specific safety outcome being measured.
The role of the human user and emerging risks
A critical theme that emerged from the synthesis is that AI in nursing documentation functions as a powerful tool, not an autonomous agent. This highlights both the irreplaceable role of the clinician and the new risks introduced by the technology itself. The study by Baxter et al. [30] provided a cautionary illustration of these risks. When a generative AI was used to draft responses to patient messages, it not only lacked empathy but dangerously suggested a patient file a formal complaint against their physician, revealing the potential to harm the therapeutic relationship and create medico-legal issues. As noted across multiple studies [24, 32], this risk of generating false or inappropriate content, often termed “hallucination,” underscores the non-negotiable need for human clinical judgment to review, edit, and validate all AI-generated outputs before they enter the official patient record.
Finally, the effectiveness of any AI tool was intrinsically linked to its integration into the clinical workflow and its acceptance by end-users. A large national study in Germany by von Wedel et al. concluded that positive clinical outcomes did not correlate with the mere adoption of technology, but rather with its “user-perceived value.” This finding underscores the paramount importance of user-centered design and ensuring that AI tools support, rather than disrupt, the complex cognitive work of nurses [28].
Discussion
This systematic review synthesized evidence from 18 included studies on the impact of diverse AI technologies on nursing documentation, focusing on the dual outcomes of time management and patient safety. Our findings revealed a rapidly innovating field with promising initial results, yet one simultaneously marked by significant methodological heterogeneity and the emergence of critical socio-technical challenges. The principal findings of this review can be organized into four core themes:
Efficiency and time management: A paradigm shift from creation to curation
AI interventions, particularly generative and ambient scribe technologies, consistently demonstrate the potential to alleviate the clinical administrative burden. Our synthesis quantitatively confirms that AI can substantially reduce time spent on documentation, with simulation studies reporting reductions exceeding 60% [21]. Furthermore, in real-world outpatient settings, time spent in notes decreased by 20.4%, and significant relief was found in “after-hours work time” (Pajama Time), which saw a reduction of 30.0% [16]. These findings strongly support the primary hypothesis that AI can liberate nursing time for direct patient interaction and theoretically mitigate clinician burnout.
However, a crucial finding is that this time-saving is not absolute. The “raw output” generated by AI consistently requires meticulous human review, editing, and clinical validation. Qualitative feedback indicates that time reallocated to editing inaccuracies, correcting factual errors, and adding clinical nuance can sometimes equate to or even outweigh the time initially saved in content generation [16]. This mandates a reframing of the net impact on time: AI drives a strategic shift in clinical workload from content creation to content curation.
Patient safety: Bifurcated impact and the emergence of new risks
The impact of AI on patient safety is complex and multifactorial, lacking uniform positivity. Our analysis identified three distinct pathways of influence:
Direct safety improvement (hard outcomes): Certain AI tools designed to target specific, measurable risks demonstrated clear, quantifiable safety gains. This includes decision support systems (CDS), like smart IV pumps, which objectively averted ≥471 preventable adverse drug events (ADEs) over five years [36]. Similarly, NLP successfully identified 35% of safety events, potentially identifiable and preventable inpatient safety events (PIVIEs) missed by conventional hospital reporting systems [26].
Indirect safety improvement via documentation quality: Studies involving generative AI often linked potential safety improvements to enhancements in documentation quality. AI tools demonstrated an ability to generate notes that were more structured, comprehensive [24], and adhered better to standardized nursing terminologies (SNTs), albeit imperfectly [25, 34]. The implicit mechanism is that better data quality supports clearer communication and safer care.
Emergence of novel safety risks: Critically, our review highlights that AI introduces new vectors for patient harm. The risk of AI “hallucinations” (factual inaccuracies) was noted even in controlled environments [21, 32]. More concerningly, LLMs demonstrated potential for severe socio-technical harm, generating responses to patient messages that lacked empathy and carried the risk of escalation, even suggesting filing formal complaints [30]. This complexity strongly reinforces the non-negotiable need for robust “human-in-the-loop” protocols to manage the intersection of AI capabilities and clinical responsibility.
Methodological landscape: The critical need for rigor
The evidence base supporting AI in nursing documentation remains nascent. The included studies were predominantly limited to quasi-experimental pre-post designs or simulation/qualitative approaches. While valuable for initial evaluation and hypothesis generation [23], this heterogeneity prevented a quantitative meta-analysis on efficiency outcomes and limits the ability to draw firm causal conclusions.
A key limitation is the inconsistency in findings regarding the strongest clinical outcome, fall prevention. While some studies reported immediate success [29]. Cho et al. reported a 29.7% immediate fall reduction, a larger longitudinal implementation failed to detect a sustained, significant decrease in the overall fall rate [31]. This lack of definitive evidence underscores a critical need for more methodologically rigorous designs, particularly well-executed controlled interrupted time series (CITS) and RCTs, to confidently attribute observed gains to the intervention rather than confounding factors.
Implementation success: The socio-technical imperative
Our findings suggest that the successful integration of AI is not purely a technical exercise but a socio-technical challenge. The national analysis by von Wedel et al. was particularly insightful, concluding that clinical benefits were correlated not merely with technology adoption, but strongly with the “user-perceived value” of the installed systems (β=−0.138) [28].
This reinforces the importance of human factors. Qualitative data highlighted that poor system design can lead to alarm fatigue [23] or create a negative organizational culture where front-line staff feel “monitored” [34]. Therefore, effective AI integration must prioritize user-centered design and maintain the centrality of human clinical judgment and professional autonomy. The transition of the nurse’s role from content creator to critical curator demands comprehensive training and a governance framework that empowers clinicians to support, not override, AI-generated recommendations.
Conclusion
The collective evidence demonstrates that AI-based documentation tools markedly improve time efficiency and workflow optimization across multiple clinical contexts. Most studies reported substantial reductions in documentation time, ranging from 20 % to over 60 %, as well as meaningful decreases in after-hours work and clinician cognitive burden. These time savings translate into improved patient flow, shorter length of stay, and enhanced opportunities for direct patient interaction. However, qualitative findings consistently emphasize that while AI systems significantly reduce the physical and mental load of documentation, they are not yet fully reliable for unsupervised clinical use. Therefore, the optimal integration of such systems requires human oversight and post-AI editing to ensure clinical accuracy, contextual relevance, and patient safety. In summary, AI holds clear potential to transform documentation efficiency and mitigate burnout, but sustained clinician engagement and rigorous validation are essential to achieve trustworthy, safe, and equitable implementation in healthcare settings.
Limitations
This systematic review is subject to several methodological and practical limitations that should be considered when interpreting the findings. First, the primary constraint was the methodological immaturity and inherent heterogeneity across the included studies. The predominance of quasi-experimental (pre-post) designs, single-center trials, and simulation-based studies limits the ability to draw firm causal conclusions regarding the net impact of AI on patient care. Specifically, the high variability in AI technologies, patient populations, and inconsistent reporting of quantitative outcomes precluded a formal statistical meta-analysis of time-related endpoints.
Second, the generalizability (external validity) of the findings is constrained. Many of the studies evaluating efficiency gains were conducted at a single site or focused on niche populations, often relying on institution-specific EHR configurations. Furthermore, the reliance on simulation and proof-of-concept designs means that the full spectrum of operational and socio-technical challenges encountered in real-world clinical deployment may be underestimated.
Third, the review’s scope was limited to formally published literature, meaning that relevant “grey literature” (e.g. technical reports, internal health system evaluations, or conference proceedings) that might contain valuable early evidence or operational insights could have been inadvertently missed.
Finally, the rapid pace of AI development, particularly within generative and ambient technologies, means that the evidence base is constantly and quickly evolving. The findings represent a snapshot in time and should be continuously evaluated against emerging technological capabilities and new implementation data.
Challenges and future works
Despite the accelerating integration of AI into nursing documentation, several challenges remain unresolved. Data heterogeneity, limited interoperability across EHR systems, and inconsistent use of SNTs continue to constrain model performance and generalizability. Future research should prioritize the development of unified data frameworks and advanced natural language processing pipelines capable of handling multilingual and context-dependent nursing language. Another critical challenge is ensuring clinical validity and trustworthiness: AI-generated documentation must be continuously validated through rigorous human-in-the-loop evaluation and transparent auditing to prevent misinformation and safeguard patient safety. The ethical and legal dimensions of AI use, particularly data privacy, algorithmic bias, and accountability, demand clear governance policies and interdisciplinary oversight. Finally, large, multi-center pragmatic trials are needed to evaluate the long-term impact of AI-assisted documentation on efficiency, patient outcomes, and clinician well-being, with special emphasis on user-centered design and real-world implementation science. Only through addressing these challenges can AI tools move from promising prototypes to reliable clinical companions in nursing practice.
Ethical Considerations
Compliance with ethical guidelines
This systematic review was conducted in accordance with established academic and ethical standards. As the work synthesized data solely from publicly available published studies and did not involve new data collection or patient/clinical interventions, Institutional Review Board (IRB) approval and participant consent were not required. The review protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) (Code: CRD420251089257). Reporting followed the PRISMA 2020 Statement to ensure clarity, reproducibility, and full disclosure of the review process.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, investigation and writing of the original draft: Arash Amadeh Taheri and Ghazaleh Afkhami Teimouri; Methodology: Yasamin Moeinipour and Arash Amadeh Taheri; Data collection: Yasamin Moeinipour, Arash Amadeh Taheri and Ghazaleh Afkhami Teimouri; Review, and editing: Yasamin Moeinipour and Fatemeh Bagheri; Supervision: Malihe Adineh Fathabadi; Project Administration: Arash Amadeh Taheri.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all individuals who contributed to this study through informal discussions or technical support but did not meet the criteria for authorship.
References
- De Groot K, De Veer AJE, Munster AM, Francke AL, Paans W. Nursing documentation and its relationship with perceived nursing workload: A mixed-methods study among community nurses. BMC Nursing. 2022; 21(1):34. [DOI:10.1186/s12912-022-00811-7] [PMID]
- Ebbers T, Kool RB, Smeele LE, Dirven R, Den Besten CA, Karssemakers LHE, et al. The Impact of Structured and Standardized Documentation on Documentation Quality; a Multicenter, Retrospective Study. Journal of Medical Systems. 2022; 46(7):46. [DOI:10.1007/s10916-022-01837-9] [PMID]
- Wahyuni ED, Nursalam N, Dewi YS, Arifin H, Benjamin LS. Electronic nursing documentation for patient safety, quality of nursing care, and documentation: A systematic review. The Journal of the Pakistan Medical Association. 2024; 74(9):1669-77. [DOI:10.47391/JPMA.9996] [PMID]
- Shi Q, Wotherspoon R, Morphet J. Nursing informatics and patient safety outcomes in critical care settings: A systematic review. BMC Nursing. 2025; 24(1):546. [DOI:10.1186/s12912-025-03195-6] [PMID]
- Bakhoum N, Gerhart C, Schremp E, Jeffrey AD, Anders S, France D, et al. A Time and Motion Analysis of Nursing Workload and Electronic Health Record Use in the Emergency Department. Journal of Emergency Nursing. 2021; 47(5):733-41. [DOI:10.1016/j.jen.2021.03.007] [PMID]
- Moore EC, Tolley CL, Bates DW, Slight SP. A systematic review of the impact of health information technology on nurses’ time. Journal of The American Medical Informatics Association. 2020; 27(5):798-807. [DOI:10.1093/jamia/ocz231] [PMID]
- Gesner E, Dykes PC, Zhang L, Gazarian P. Documentation Burden in Nursing and Its Role in Clinician Burnout Syndrome. Applied Clinical Informatics. 2022; 13(05):983-90. [DOI:10.1055/s-0042-1757157] [PMID]
- Nguyen OT, Shah S, Gartland AJ, Parekh A, Turner K, Feldman SS, et al. Factors associated with nurse well-being in relation to electronic health record use: A systematic review. Journal of the American Medical Informatics Association. 2021; 28(6):1288-97. [DOI:10.1093/jamia/ocaa289] [PMID]
- Mitha S, Schwartz J, Hobensack M, Cato K, Woo K, Smaldone A, et al. Natural Language Processing of Nursing Notes: An Integrative Review. CIN: Computers, Informatics, Nursing. 2023; 41(6):377-84. [DOI:10.1097/CIN.0000000000000967] [PMID]
- Trinh VQN, Zhang S, Kovoor J, Gupta A, Chan WO, Gilbert T, et al. The use of natural language processing in detecting and predicting falls within the healthcare setting: A systematic review. International Journal for Quality in Health Care. 2023; 35(4):mzad077. [DOI:10.1093/intqhc/mzad077] [PMID]
- Brann F, Sterling NW, Frisch SO, Schrager JD. Sepsis prediction at emergency department triage using natural language processing: Retrospective cohort study. Journal of Medical Internet Research Artificial Intelligence. 2024; 3:e49784. [DOI:10.2196/49784] [PMID]
- Peivandi S, Ahmadian L, Farokhzadian J, Jahani Y. Evaluation and comparison of errors on nursing notes created by online and offline speech recognition technology and handwritten: An interventional study. BMC Medical Informatics and Decision Making. 2022; 22(1):96. [DOI:10.1186/s12911-022-01835-4] [PMID]
- Hou SY, Wu YL, Chen KC, Chang TA, Hsu YM, Chuang SJ, et al. Code-switching automatic speech recognition for nursing record documentation: System development and evaluation. JMIR Nursing. 2022; 5(1):e37562. [DOI:10.2196/37562] [PMID] []
- Tierney AA, Gayre G, Hoberman B, Mattern B, Ballesca M, Kipnis P, et al. Ambient Artificial Intelligence Scribes to Alleviate the Burden of Clinical Documentation. NEJM Catalyst. 2024; 5(3). [DOI:10.1056/CAT.23.0404]
- Wendt SJ, Dinh CT, Sutcliffe M, Jones K, Scanlan JM, Smitherman JS. Deploying ambient clinical intelligence to improve care: A research article assessing the impact of nuance DAX on documentation burden and burnout. Future Healthcare Journal. 2025; 12(3):100450. [DOI:10.1016/j.fhj.2025.100450] [PMID]
- Duggan MJ, Gervase J, Schoenbaum A, Hanson W, Howell JT, Sheinberg M, et al. Clinician Experiences With Ambient Scribe Technology to Assist With Documentation Burden and Efficiency. JAMA Network Open. 2025; 8(2):e2460637. [DOI:10.1001/jamanetworkopen.2024.60637] [PMID]
- Liu TL, Hetherington TC, Dharod A, Carroll T, Bundy R, Nguyen H, et al. Does AI-Powered Clinical Documentation Enhance Clinician Efficiency? A Longitudinal Study. New England Journal of Medicine – Artificial Intelligence. 2024; 1(12). [DOI:10.1056/AIoa2400659]
- Haberle T, Cleveland C, Snow GL, Barber C, Stookey N, Thornock C, et al. The impact of nuance DAX ambient listening AI documentation: A cohort study. Journal of The American Medical Informatics Association. 2024; 31(4):975-9. [DOI:10.1093/jamia/ocae022] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. [DOI:10.1136/bmj.n71] [PMID]
- Lockwood C, Porrit K, Munn Z, Rittenmeyer L, Salmond S, Bjerrum M, et al. Systematic reviews of qualitative evidence. Jbi Manual for Evidence Synthesis. 2020; 46658:1-4. [Link]
- Ju H, Park M, Jeong H, Lee Y, Kim H, Seong M, et al. Generative AI-Based Nursing Diagnosis and Documentation Recommendation Using Virtual Patient Electronic Nursing Record Data. Healthcare Informatics Research. 2025; 31(2):156-65. [DOI:10.4258/hir.2025.31.2.156] [PMID]
- Levin S, Barnes S, Toerper M, Debraine A, DeAngelo A, Hamrock E, et al. Machine-learning-based hospital discharge predictions can support multidisciplinary rounds and decrease hospital length-of-stay. BMJ Innovations. 2021; 7(2). [DOI:10.1136/bmjinnov-2020-000420]
- King CR, Shambe A, Abraham J. Potential uses of AI for perioperative nursing handoffs: A qualitative study. JAMIA Open. 2023; 6(1):ooad015. [DOI:10.1093/jamiaopen/ooad015] [PMID]
- Chen CJ, Liao CT, Tung YC, Liu CF. Enhancing healthcare efficiency: Integrating ChatGPT in nursing documentation. Studies in Health Technology and Informatics. 2024; 316:851-2. [Link]
- Dos Santos FC, Johnson LG, Madandola OO, Priola KJB, Yao Y, Macieira TGR, et al. An example of leveraging AI for documentation: ChatGPT-generated nursing care plan for an older adult with lung cancer. Journal of the American Medical Informatics Association. 2024; 31(9):2089-96. [DOI:10.1093/jamia/ocae116] [PMID]
- Ozonoff A, Milliren CE, Fournier K, Welcher J, Landschaft A, Samnaliev M, et al. Electronic surveillance of patient safety events using natural language processing. Health Informatics Journal. 2022; 28(4):14604582221132429. [DOI:10.1177/14604582221132429] [PMID]
- Poon EG, Lemak CH, Rojas JC, Guptill J, Classen D. Adoption of artificial intelligence in healthcare: survey of health system priorities, successes, and challenges. Journal of The American Medical Informatics Association. 2025; 32(7):1093-100. [DOI:10.1093/jamia/ocaf065] [PMID]
- von Wedel P, Hagist C, Liebe JD, Esdar M, Hübner U, Pross C. Effects of Hospital Digitization on Clinical Outcomes and Patient Satisfaction: Nationwide Multiple Regression Analysis Across German Hospitals. Journal of Medical Internet Research. 2022; 24(11):e40124. [DOI:10.2196/40124] [PMID]
- Cho I, Jin IS, Park H, Dykes PC. Clinical Impact of an Analytic Tool for Predicting the Fall Risk in Inpatients: Controlled Interrupted Time Series. JMIR Medical Informatics. 2021; 9(11):e26456. [DOI:10.2196/26456] [PMID]
- Baxter SL, Longhurst CA, Millen M, Sitapati AM, Tai-Seale M. Generative artificial intelligence responses to patient messages in the electronic health record: Early lessons learned. JAMIA Open. 2024; 7(2):ooae028. [DOI:10.1093/jamiaopen/ooae028] [PMID]
- Cho I, Cho J, Hong JH, Choe WS, Shin H. Utilizing standardized nursing terminologies in implementing an AI-powered fall-prevention tool to improve patient outcomes: A multihospital study. Journal of The American Medical Informatics Association. 2023; 30(11):1826-36. [DOI:10.1093/jamia/ocad145] [PMID]
- Balloch J, Sridharan S, Oldham G, Wray J, Gough P, Robinson R, et al. Use of an ambient artificial intelligence tool to improve quality of clinical documentation. Future Healthcare Journal. 2024; 11(3):100157. [DOI:10.1016/j.fhj.2024.100157] [PMID]
- Cho I, Kim M, Song MR, Dykes PC. Evaluation of an approach to clinical decision support for preventing inpatient falls: A pragmatic trial. JAMIA Open. 2023; 6(2):ooad019. [DOI:10.1093/jamiaopen/ooad019] [PMID]
- Johnson OA, McCrorie C, McInerney C, Mebrahtu TF, Granger J, Sheikh N, et al. Implementing an artificial intelligence command centre in the NHS: A mixed-methods study. Health and Social Care Delivery Research. 2024; 12(41):1-108. [DOI:10.3310/TATM3277]
- Yang L, Pang J, Zuo S, Xu J, Jin W, Zuo F, et al. Evolution of the “Internet Plus Health Care” Mode Enabled by Artificial Intelligence: Development and Application of an Outpatient Triage System. Journal of Medical Internet Research. 2024; 26:e51711. [DOI:10.2196/51711] [PMID]
- Danello SH, Maddox RR, Schaack GJ. Intravenous Infusion Safety Technology: Return on Investment. Hospital Pharmacy. 2009; 44(8):680-8. [DOI:10.1310/hpj4408-680]
- Johnson LG, Madandola OO, Dos Santos FC, Priola KJB, Yao Y, Macieira TGR, et al. Creating perinatal nursing care plans using ChatGPT: A pathway to improve nursing care plans and reduce documentation burden. The Journal of Perinatal & Neonatal Nursing. 2025; 39(1):10-9. [Link]
Type of Study: Review Article |
Subject:
● Artificial Intelligence
Received: 2025/10/13 | Accepted: 2025/11/8 | Published: 2025/12/31
Received: 2025/10/13 | Accepted: 2025/11/8 | Published: 2025/12/31
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
