

Volume 11, Issue 3 (May & Jun 2021)
J Research Health 2021, 11(3): 191-202 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shahabi A, Ehteshamzadeh P, Asgari P, Makvandi B. Effectiveness of ACT vs Guided Imagery on Emotional Regulation of Cardiac Patients. J Research Health 2021; 11 (3) :191-202
URL: http://jrh.gmu.ac.ir/article-1-1826-en.html
URL: http://jrh.gmu.ac.ir/article-1-1826-en.html



1- Department of Health Psychology, Khorramshahr-Persian Gulf International Branch, Islamic Azad University, Khorramshahr, Iran.
2- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran. ,ehtesham@iauahvaz.ac.ir
3- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran.
2- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran. ,
3- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran.
Full-Text [PDF 739 kb]
(772 Downloads)
| Abstract (HTML) (2592 Views)
Full-Text: (886 Views)
1. Introduction
Currently, cardiovascular disease is recognized as the most important cause of death worldwide. In Western countries, such diseases generate more deaths than any other disease. In the United States, more than half of all death cases over the age of 45 years belong to cardiovascular diseases. In Iran, cardiovascular disease is the first cause of death in individuals aged over 35 years. Additionally, according to the Isfahan cohort research, the incidence of heart disease equals 19.4% in Iran [1]. The leading cause of death in Iran is cardiovascular diseases involving 39.3% of all deaths. Of this percentage, 19.5% is related to myocardial infarction, 9.3% to brain stroke, and 3.1% to hypertension; the rest is related to other cardiovascular diseases [2].
Various physical, social, and personal characteristics increase both the risk of cardiovascular disease and its complications and mortality and affect the recovery process of these patients [3]. In cardiovascular diseases, emotion or emotion suppression is among the effective psychological factors that may impact the occurrence or exacerbation of these conditions. Studies indicate that the chronic effects of the inhibition of negative emotions increase the activity of the sympathetic function of the cardiovascular system [4]. The main finding shows that the enhanced level of negative emotions is associated with aggravated cardiovascular diseases. These findings led researchers to suspect that Emotion Regulation (ER) affected the outcome of this disease [5]. With the advent of psychosomatic illnesses, ER became central to physical health features [6]. Emotions are biological reactions that appear in critical challenges and life situations to coordinate our reactions and responses. Yarmohammadian et al. argued that intense emotions and acute stress could accelerate cardiac arrhythmias. Furthermore, the presence of the symptoms of anxiety and depression in individuals with myocardial infarction delays the recovery process and increases mortality in patients [7].
Emotion is a transient and continuous confusion in the mind, generated because of the difference between perceived reality and the individual’s desires. Emotions help individuals to cope with the problems and opportunities they face in life. However, emotions are not always helpful and can be harmful and lead to emotional problems [8]. Although emotions have a biological basis, individuals can influence emotions and how they are expressed; this notion is called ER [9]. The ER concept refers to the processes that individuals consciously or unconsciously use to respond to environmental demands appropriately [10]. The ER also acts as a mediator in coping with stress; individuals who use maladaptive cognitive strategies experience higher stress than those engaging in adaptive strategies [11].
One of the most novel psychological approaches is Acceptance and Commitment Therapy (ACT). This method is part of a clinical psychology approach committed to providing scientific treatment methods. Moreover, this new psychotherapy model is part of the so-called third wave of cognitive-behavioral therapy [12]. The ACT does not aim to create direct changes in clients, instead, it attempts to improve psychological and behavioral flexibility in areas where experiential avoidance prevails and prevents the individual of fundamental life aspects. Psychological flexibility increases the individual’s ability to make practical and the most appropriate choices between different options [13]. Psychological flexibility in the ACT is achieved through six main processes of acceptance, defusion, self as context, being present, valuing, and committed action [12]. Recent research on ACT has nominated this method as a suitable treatment for depression [10], posttraumatic stress disorder [14], panic disorder [15], chronic pain [16], job stress [6], obsessive-compulsive disorder [12], breast cancer [17], multiple sclerosis [18], diabetes [19, 20], and atypical grief [5].
Another treatment method is Guided Imagery (GI). As a mind-body technique, GI is based on the fact that mind and body are interconnected and can interact and reinforce each other in treating diseases and improving health. The GI activates the same area of the brain as the experience of an event does. In other words, people precisely create a stream of thought in themselves where they can see, hear, feel, or smell what they desire to feel at that time and can visualize it in their imagination [21]. Besides, GI creates a sense of power and relaxation by emphasizing focusing and using images, landscapes, sounds, music, and words [4]. In GI, individuals are encouraged to take deep abdominal and diaphragmatic breaths, and then, release muscles and imagine sceneries, like forest, beach, and pilgrimage sites, and pay attention to surrounding sounds and smells. Studies demonstrated that focusing on positive imagery can improve and balance mood. Creating a competitive focus and visualization can reduce pain, tension, anxiety, and depression and increase the feeling of health [22]. Abolghasemi and Saedi [22] stated that GI and gradual stress relief along with biofeedback are effective and sustainable in reducing migraine headaches in patients with migraines.
The main factor in preventing cardiovascular diseases is controlling behaviors and emotions in different life situations. Numerous factors, including characteristics, a history of mental health disorders, and family and work environments affect ER; they may also impair ER in chronic and acute illnesses, indicating the need for psychological treatment in these individuals [23]. Sheibani et al. investigated the effects of ACT on emotional intelligence and control in patients with cardiovascular diseases. These authors concluded that ACT significantly affected negative and positive ER in the studied patients [24]. Also, Yijing et al. reported the positive impact of GI on the heart rate of individuals encountering stressful environments [25]. However, no study has compared the effects of these methods on emotional intelligence in patients with cardiovascular diseases. Thus, the present study aimed to compare the impact of ACT and GI on positive and negative ER in patients with cardiovascular diseases referring to the cardiac rehabilitation department.
2. Methods
Study design
This was an experimental study with a pre-test, post-test design, a control group, and a 45-day follow-up. Among the patients referred to the cardiac rehabilitation department of Imam Reza Hospital, Mashhad City, Iran, in 2017, 45 patients with cardiovascular diseases were selected based on a clinical interview and the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition criteria. Accordingly, they received the treatment sessions after meeting the inclusion criteria and providing consent to participate in the study. Next, the study subjects were assigned into groups using the random sampling method. The mean age of the study subjects in the ACT, GI, and control groups was 55, 54, and 55 years, respectively.
The ER was measured using the Garnefski et al. scale in 2001. Besides, the experimental groups received separate 90-minute therapeutic intervention sessions. The first experimental group underwent eight sessions of ACT per the Sahebi therapy package (2012). The second group received 10 sessions of GI using the Simonton training package (2000). However, the control group received no psychological intervention. After completing the intervention sessions, the research variables were assessed in all study groups, in the post-test phase. Besides, the follow-up evaluation was conducted 45 days after the completion of the sessions.
The inclusion criteria of the study included having a cardiac problem, admission to the cardiac rehabilitation department, having a minimum literacy level (junior high) to understand the concepts of treatment sessions, and an age range of 35 to 75 years. Also, the exclusion criteria consisted of severe mental health disorders or neurological-induced illnesses, such as epilepsy and Alzheimer disease; drug or alcohol dependence; and the concurrent use of psychotropic medications.
Study measures
Demographic Characteristics Questionnaire: This researcher-made scale was designed to collect the personal information of the study subjects and included age, gender, educational level, marital status, and the history of heart surgery.
Cognitive Emotion Regulation Questionnaire (CERQ): The CERQ is a multidimensional self-report inventory. The main version of CERQ includes seven subscales and 36 questions that fall into two groups: negative strategies (self-blame, rumination, catastrophizing, and other-blame) and positive strategies (acceptance, positive reappraisal, refocus on planning, and positive refocusing). The questions are scored on a 5-point Likert scale, ranging from score one (almost never) to five (almost always). The total score of each subscale is calculated based on the algebraic sum of the questions’ values.
The reliability of CERQ was reported using the Cronbach alpha coefficient for positive and negative ER strategies and the whole questionnaire as 0.91, 0.86, and 0.93, respectively [26]. In Iran, Aminehabadi examined the construct validity of the questionnaire through exploratory factor analysis, using principal component analysis; this author reported a validity coefficient of 0.70 for the whole questionnaire [27]. The CERQ components include negative ER strategies that consist of the subcategories of self-blame, other-blame, rumination, and catastrophizing, as well as positive ER strategies, including acceptance, positive reappraisal, refocus on planning, putting into perspective, and positive refocusing.
Regarding reliability and validity, this questionnaire includes 36 5-point Likert-type questions (ranging from always to never). Every four questions evaluate one characteristic and a total of nine factors of self-blame, other-blame, rumination, catastrophizing, acceptance, positive reappraisal, refocus on planning, putting into perspective, and positive refocusing. The Persian version of CERQ has been validated by Samani and Jokar [28]. The reliability of this questionnaire was assessed using the Cronbach alpha coefficient; the relevant values for the subscales of the questionnaire have been reported by Granfski et al. to range from 0.71 to 0.81 [23].
To evaluate the convergent and divergent validity of this questionnaire in Iran, we used the Depression Anxiety Stress Scales that includes 21 4-point Likert-type items (from completely like me, to completely unlike me). This tool evaluates three factors of depression, stress, and anxiety and also addresses the cause of the emotional disturbances. To assess the psychometric properties of the ER questionnaire, this tool was first explored by factor analysis (to review and evaluate the construct validity). Before conducting factor analysis, the Kaiser-Meyer-Olkin ratio index was examined and the Bartlett-test was conducted. After confirming these indices, the cognitive ER questionnaire was assessed using the factor analysis and principal components methods.
Procedures
To conduct the research process, 45 individuals were selected and randomly assigned into the study groups, after the initial interview with patients based on the inclusion and exclusion criteria and providing complete explanations about the research and the related questionnaires. Then, the ACT and GI groups received eight and ten 90-minute intervention sessions, respectively. The first experimental group underwent eight sessions of ACT using the Sahebi therapy package (2012) and the second group received 10 sessions of GI using the Simonton training package (2000). All sessions were performed in groups, however, two study participants from the ACT group received four individual sessions because of their heart conditions. Initially, all study groups underwent the pre-test evaluation and completed the demographic characteristics questionnaire and the CERQ. After the treatment intervention, the post-test was performed in all three groups. After 45 days, the CERQ was recompleted by the research groups in the follow-up phase. Table 1 provides the content of ACT (Sahebi, 2012) and GI intervention (Simonten, 2000), respectively [2].
.PNG)
.PNG)
After collecting questionnaires and coding, the obtained data were analyzed using descriptive statistics related to the assumptions of the multivariate analysis of covariance to check the normality of variables in the samples and the equality of variances, in SPSS v. 22. Also, the inferential statistics, including the repeated-measures ANCOVA and Bonferroni post hoc test were used to compare the effectiveness of the two intervention methods; the relevant results were presented in tables and graphs.
3. Results
The demographic data of the study samples were compared between the two groups of intervention and control, also, the homogeneity of each variable was examined in the two groups (Table 2). In total, 93.3% and 53.3% of the study subjects were male in the GI and ACT groups, respectively. The Chi-squared test data indicated a significant difference in the frequency of gender between the two groups (P=0.034). Thus, the two groups were not homogeneous in terms of gender.
.PNG)
Moreover, the Mean±SD age of the study participants in the GI and ACT groups was 57.9±10.2 and 53.3±10.3 years, respectively. However, the age difference was not significant (P=0.187), based on the Mann-Whitney U test, and the two groups were homogeneous in terms of age.
In total, 33.3% and 53.3% of the subjects in the GI and ACT groups had a diploma, respectively. The Mann-Whitney U test revealed no significant difference concerning educational level between the two groups (P=0.436), thus, the two groups were homogeneous in terms of education (Table 2).
As per Table 3, the pre-test and post-test scores of the ACT group are much higher than that of the GI group. The independent samples t-test and MANCOVA were applied to investigate the differences in the effectiveness of these approaches in improving the positive and negative ER strategies in the explored patients (P=0.165 and P=0.101). The independent samples t-test results suggested a significant difference between the study groups, concerning positive ER, with the GI to be more efficient in this regard. Besides, the detected changes in negative ER significantly differed between the two therapies; GI was more effective than ACT in this aspect (P=0.003, t=2.3). Since no significant relationship was observed between gender and positive and negative ER, this variable was not confounding (P>0.05).
.PNG)
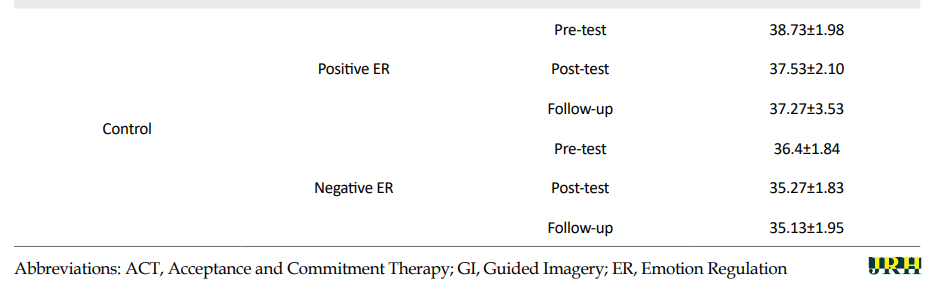
The effectiveness of ACT was studied in the positive and negative ER of cardiac patients referred to the cardiac rehabilitation department. The repeated-measures ANOVA reflected changes in the ER by controlling the pre-test scores between the ACT and control groups. Considering the level of significance and the eta-squared (89%), ACT was effective on positive and negative ER in the studied patients (P<0.001) (Table 4).
.PNG)
The effectiveness of GI was studied in the positive and negative ER of cardiac patients referred to the cardiac rehabilitation department. The results indicated that (after controlling the pre-test data) the GI group presented higher effects on positive ER, compared with the control group (eta-squared, 81%; P<0.001). However, GI was ineffective on negative ER (P=0.103) (Table 4).
At each stage of the measurement, the effectiveness of ACT and GI were examined in positive ER in the studied patients. The Bonferroni post hoc test revealed a significant increase in the positive ER post-test values of the ACT group, compared with the GI and control groups (P<0.001). Besides, the differences between the two groups’ mean scores highlighted the higher effects of ACT, compared with the GI approach. Additionally, compared with the GI group, the ACT group presented significant differences in all assessment phases (P<0.001). The ACT group members achieved higher scores on positive ER (Table 5).


At each stage of the measurement, the effectiveness of ACT and GI were examined in negative ER in the studied patients. The Bonferroni post hoc test revealed a significant decrease in the negative ER post-test values of the ACT group, compared with the GI and control groups (P<0.001). Besides, the differences between the mean scores of the two groups reflected the higher effects of ACT, compared with the GI approach. Additionally, compared with the GI program, the ACT group presented significant differences in the follow-up step (P<0.001).
4. Discussion
The current findings indicated that ACT was effective on positive and negative ER in patients with cardiovascular conditions. These results are consistent with the results of Moghadamfar et al. [29] and Darvish Baseri et al. [30]. The obtained results reflected that experiential avoidance, which is the main component of psychological inflexibility in ACT, is significantly and negatively correlated with adaptive ER strategies. Therefore, the primary purpose of ACT is to reduce avoidance. Accordingly, this treatment can improve adaptive ER strategies in individuals.
Another useful process of ACT is introducing an alternative to control, namely, acceptance. The acceptance component allows the individual to accept unpleasant inner emotional experiences without trying to control them. Subsequently, such emotional experiences seem less threatening and impact less on the individual’s life. Besides, the mindfulness processes used in this treatment cause dramatic changes in the way clients use mindfulness. In other words, these processes generate attention bias in the individual and cause fostering a viewpoint of mental events, which allows the person to observe better mental events instead of considering those as part of their existence. Thus, ACT can effectively regulate an individual’s emotions owing to its emphasis on accepting experiences and performing voluntary actions [31].
Furthermore, GI was effective on positive ER in the studied patients. In this regard, Smucker et al. in 1995 and Aachen Bach in 2004 believed that individuals with incurable diseases often experience negative self-evaluation and consider themselves as the victims of difficult life situations. Such a negative evaluation, which is accompanied by mental rumination over time, leads to cognitive distortions and irrational beliefs about oneself, the world, and the future. Accordingly, these people not only encounter emotional and interpersonal problems but also experience numerous mental health symptoms, such as depression, anxiety, helplessness, insomnia, nightmares, and even suicidal ideation. By participating in GI sessions, negative thoughts, maladaptive schemas, and the traumatic mental images of their illness are first redisplayed, cognitively visualized, and reviewed with details. Then, with the changes generated in its meanings, positive thoughts and mental images are replaced by previous negative thoughts and mental images.
In such situations, on the one hand, their tolerance for sorrow, desire, and life expectancy increases, and on the other hand, their inner conflict, negative emotions, and annoying thoughts decrease. Eventually, they overcome negative thoughts and images that have taken over their level of consciousness. This process not only improves their interpersonal relationships but also reduces many of their mental health conditions, such as anxiety, negative automatic thoughts, and emotions [32]. Hackmann and Holmes and Arntz et al. investigated patients with cancer and suggested GI as an effective treatment for them. This result is because GI causes the expression, visualization, and cognitive reprocessing of negative thoughts and stressful memories. It plays an essential role in controlling psychological symptoms, such as negative automatic thoughts, mental rumination, and insomnia in different patients [4, 33].
Some limitations of the present study included the small sample size and the study restriction to one hospital in Mashhad City; these limitations should be considered in generalizing the obtained results. Besides, the interval between the post-test and follow-up phase was short. Thus, future studies could consider a continuous follow-up period to achieve more accurate data.
5. Conclusion
The present study suggested the effectiveness of ACT in positive and negative ER among patients with cardiovascular conditions. In the ACT, the purpose of emphasizing individuals’ desire for inner experiences is to assist them in coping with their disturbing thoughts, experiencing them as thoughts, becoming aware of the ineffective nature of their current plan, dealing with what is important to them in life instead of responding to the thoughts, and matching with their values. The ACT is a behavioral therapy that uses mindfulness, acceptance, and cognitive defusion skills to increase psychological flexibility.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Ahvaz Branch, Islamic Azad University (Code: IR.IAU.AHVAZ.REC.1398.012).Moreover, it received the Iranian Clinical Trials code (IRCT20190727044345N1).All ethical principles are considered in this article. The participants were informed about the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This study was extracted from PhD. dissertation of the first author at the Department of Health Psychology, Khorramshahr-Persian Gulf International Branch, Islamic Azad University, Khorramshahr.
Authors' contributions
Conceptualization and supervision: Parvin Ehteshamzade; Methodology: Abbasali Shahabi; Investigation, writing – original draft, and writing – review & editing: All authors; Data collection, data analysis, funding acquisition and resources: Abbsali Shahabi.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
We want to appreciate All patients and the staff of the Cardiac Rehabilitation Department of Imam Reza (AS) Hospital in Mashhad.
Currently, cardiovascular disease is recognized as the most important cause of death worldwide. In Western countries, such diseases generate more deaths than any other disease. In the United States, more than half of all death cases over the age of 45 years belong to cardiovascular diseases. In Iran, cardiovascular disease is the first cause of death in individuals aged over 35 years. Additionally, according to the Isfahan cohort research, the incidence of heart disease equals 19.4% in Iran [1]. The leading cause of death in Iran is cardiovascular diseases involving 39.3% of all deaths. Of this percentage, 19.5% is related to myocardial infarction, 9.3% to brain stroke, and 3.1% to hypertension; the rest is related to other cardiovascular diseases [2].
Various physical, social, and personal characteristics increase both the risk of cardiovascular disease and its complications and mortality and affect the recovery process of these patients [3]. In cardiovascular diseases, emotion or emotion suppression is among the effective psychological factors that may impact the occurrence or exacerbation of these conditions. Studies indicate that the chronic effects of the inhibition of negative emotions increase the activity of the sympathetic function of the cardiovascular system [4]. The main finding shows that the enhanced level of negative emotions is associated with aggravated cardiovascular diseases. These findings led researchers to suspect that Emotion Regulation (ER) affected the outcome of this disease [5]. With the advent of psychosomatic illnesses, ER became central to physical health features [6]. Emotions are biological reactions that appear in critical challenges and life situations to coordinate our reactions and responses. Yarmohammadian et al. argued that intense emotions and acute stress could accelerate cardiac arrhythmias. Furthermore, the presence of the symptoms of anxiety and depression in individuals with myocardial infarction delays the recovery process and increases mortality in patients [7].
Emotion is a transient and continuous confusion in the mind, generated because of the difference between perceived reality and the individual’s desires. Emotions help individuals to cope with the problems and opportunities they face in life. However, emotions are not always helpful and can be harmful and lead to emotional problems [8]. Although emotions have a biological basis, individuals can influence emotions and how they are expressed; this notion is called ER [9]. The ER concept refers to the processes that individuals consciously or unconsciously use to respond to environmental demands appropriately [10]. The ER also acts as a mediator in coping with stress; individuals who use maladaptive cognitive strategies experience higher stress than those engaging in adaptive strategies [11].
One of the most novel psychological approaches is Acceptance and Commitment Therapy (ACT). This method is part of a clinical psychology approach committed to providing scientific treatment methods. Moreover, this new psychotherapy model is part of the so-called third wave of cognitive-behavioral therapy [12]. The ACT does not aim to create direct changes in clients, instead, it attempts to improve psychological and behavioral flexibility in areas where experiential avoidance prevails and prevents the individual of fundamental life aspects. Psychological flexibility increases the individual’s ability to make practical and the most appropriate choices between different options [13]. Psychological flexibility in the ACT is achieved through six main processes of acceptance, defusion, self as context, being present, valuing, and committed action [12]. Recent research on ACT has nominated this method as a suitable treatment for depression [10], posttraumatic stress disorder [14], panic disorder [15], chronic pain [16], job stress [6], obsessive-compulsive disorder [12], breast cancer [17], multiple sclerosis [18], diabetes [19, 20], and atypical grief [5].
Another treatment method is Guided Imagery (GI). As a mind-body technique, GI is based on the fact that mind and body are interconnected and can interact and reinforce each other in treating diseases and improving health. The GI activates the same area of the brain as the experience of an event does. In other words, people precisely create a stream of thought in themselves where they can see, hear, feel, or smell what they desire to feel at that time and can visualize it in their imagination [21]. Besides, GI creates a sense of power and relaxation by emphasizing focusing and using images, landscapes, sounds, music, and words [4]. In GI, individuals are encouraged to take deep abdominal and diaphragmatic breaths, and then, release muscles and imagine sceneries, like forest, beach, and pilgrimage sites, and pay attention to surrounding sounds and smells. Studies demonstrated that focusing on positive imagery can improve and balance mood. Creating a competitive focus and visualization can reduce pain, tension, anxiety, and depression and increase the feeling of health [22]. Abolghasemi and Saedi [22] stated that GI and gradual stress relief along with biofeedback are effective and sustainable in reducing migraine headaches in patients with migraines.
The main factor in preventing cardiovascular diseases is controlling behaviors and emotions in different life situations. Numerous factors, including characteristics, a history of mental health disorders, and family and work environments affect ER; they may also impair ER in chronic and acute illnesses, indicating the need for psychological treatment in these individuals [23]. Sheibani et al. investigated the effects of ACT on emotional intelligence and control in patients with cardiovascular diseases. These authors concluded that ACT significantly affected negative and positive ER in the studied patients [24]. Also, Yijing et al. reported the positive impact of GI on the heart rate of individuals encountering stressful environments [25]. However, no study has compared the effects of these methods on emotional intelligence in patients with cardiovascular diseases. Thus, the present study aimed to compare the impact of ACT and GI on positive and negative ER in patients with cardiovascular diseases referring to the cardiac rehabilitation department.
2. Methods
Study design
This was an experimental study with a pre-test, post-test design, a control group, and a 45-day follow-up. Among the patients referred to the cardiac rehabilitation department of Imam Reza Hospital, Mashhad City, Iran, in 2017, 45 patients with cardiovascular diseases were selected based on a clinical interview and the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition criteria. Accordingly, they received the treatment sessions after meeting the inclusion criteria and providing consent to participate in the study. Next, the study subjects were assigned into groups using the random sampling method. The mean age of the study subjects in the ACT, GI, and control groups was 55, 54, and 55 years, respectively.
The ER was measured using the Garnefski et al. scale in 2001. Besides, the experimental groups received separate 90-minute therapeutic intervention sessions. The first experimental group underwent eight sessions of ACT per the Sahebi therapy package (2012). The second group received 10 sessions of GI using the Simonton training package (2000). However, the control group received no psychological intervention. After completing the intervention sessions, the research variables were assessed in all study groups, in the post-test phase. Besides, the follow-up evaluation was conducted 45 days after the completion of the sessions.
The inclusion criteria of the study included having a cardiac problem, admission to the cardiac rehabilitation department, having a minimum literacy level (junior high) to understand the concepts of treatment sessions, and an age range of 35 to 75 years. Also, the exclusion criteria consisted of severe mental health disorders or neurological-induced illnesses, such as epilepsy and Alzheimer disease; drug or alcohol dependence; and the concurrent use of psychotropic medications.
Study measures
Demographic Characteristics Questionnaire: This researcher-made scale was designed to collect the personal information of the study subjects and included age, gender, educational level, marital status, and the history of heart surgery.
Cognitive Emotion Regulation Questionnaire (CERQ): The CERQ is a multidimensional self-report inventory. The main version of CERQ includes seven subscales and 36 questions that fall into two groups: negative strategies (self-blame, rumination, catastrophizing, and other-blame) and positive strategies (acceptance, positive reappraisal, refocus on planning, and positive refocusing). The questions are scored on a 5-point Likert scale, ranging from score one (almost never) to five (almost always). The total score of each subscale is calculated based on the algebraic sum of the questions’ values.
The reliability of CERQ was reported using the Cronbach alpha coefficient for positive and negative ER strategies and the whole questionnaire as 0.91, 0.86, and 0.93, respectively [26]. In Iran, Aminehabadi examined the construct validity of the questionnaire through exploratory factor analysis, using principal component analysis; this author reported a validity coefficient of 0.70 for the whole questionnaire [27]. The CERQ components include negative ER strategies that consist of the subcategories of self-blame, other-blame, rumination, and catastrophizing, as well as positive ER strategies, including acceptance, positive reappraisal, refocus on planning, putting into perspective, and positive refocusing.
Regarding reliability and validity, this questionnaire includes 36 5-point Likert-type questions (ranging from always to never). Every four questions evaluate one characteristic and a total of nine factors of self-blame, other-blame, rumination, catastrophizing, acceptance, positive reappraisal, refocus on planning, putting into perspective, and positive refocusing. The Persian version of CERQ has been validated by Samani and Jokar [28]. The reliability of this questionnaire was assessed using the Cronbach alpha coefficient; the relevant values for the subscales of the questionnaire have been reported by Granfski et al. to range from 0.71 to 0.81 [23].
To evaluate the convergent and divergent validity of this questionnaire in Iran, we used the Depression Anxiety Stress Scales that includes 21 4-point Likert-type items (from completely like me, to completely unlike me). This tool evaluates three factors of depression, stress, and anxiety and also addresses the cause of the emotional disturbances. To assess the psychometric properties of the ER questionnaire, this tool was first explored by factor analysis (to review and evaluate the construct validity). Before conducting factor analysis, the Kaiser-Meyer-Olkin ratio index was examined and the Bartlett-test was conducted. After confirming these indices, the cognitive ER questionnaire was assessed using the factor analysis and principal components methods.
Procedures
To conduct the research process, 45 individuals were selected and randomly assigned into the study groups, after the initial interview with patients based on the inclusion and exclusion criteria and providing complete explanations about the research and the related questionnaires. Then, the ACT and GI groups received eight and ten 90-minute intervention sessions, respectively. The first experimental group underwent eight sessions of ACT using the Sahebi therapy package (2012) and the second group received 10 sessions of GI using the Simonton training package (2000). All sessions were performed in groups, however, two study participants from the ACT group received four individual sessions because of their heart conditions. Initially, all study groups underwent the pre-test evaluation and completed the demographic characteristics questionnaire and the CERQ. After the treatment intervention, the post-test was performed in all three groups. After 45 days, the CERQ was recompleted by the research groups in the follow-up phase. Table 1 provides the content of ACT (Sahebi, 2012) and GI intervention (Simonten, 2000), respectively [2].
After collecting questionnaires and coding, the obtained data were analyzed using descriptive statistics related to the assumptions of the multivariate analysis of covariance to check the normality of variables in the samples and the equality of variances, in SPSS v. 22. Also, the inferential statistics, including the repeated-measures ANCOVA and Bonferroni post hoc test were used to compare the effectiveness of the two intervention methods; the relevant results were presented in tables and graphs.
3. Results
The demographic data of the study samples were compared between the two groups of intervention and control, also, the homogeneity of each variable was examined in the two groups (Table 2). In total, 93.3% and 53.3% of the study subjects were male in the GI and ACT groups, respectively. The Chi-squared test data indicated a significant difference in the frequency of gender between the two groups (P=0.034). Thus, the two groups were not homogeneous in terms of gender.
Moreover, the Mean±SD age of the study participants in the GI and ACT groups was 57.9±10.2 and 53.3±10.3 years, respectively. However, the age difference was not significant (P=0.187), based on the Mann-Whitney U test, and the two groups were homogeneous in terms of age.
In total, 33.3% and 53.3% of the subjects in the GI and ACT groups had a diploma, respectively. The Mann-Whitney U test revealed no significant difference concerning educational level between the two groups (P=0.436), thus, the two groups were homogeneous in terms of education (Table 2).
As per Table 3, the pre-test and post-test scores of the ACT group are much higher than that of the GI group. The independent samples t-test and MANCOVA were applied to investigate the differences in the effectiveness of these approaches in improving the positive and negative ER strategies in the explored patients (P=0.165 and P=0.101). The independent samples t-test results suggested a significant difference between the study groups, concerning positive ER, with the GI to be more efficient in this regard. Besides, the detected changes in negative ER significantly differed between the two therapies; GI was more effective than ACT in this aspect (P=0.003, t=2.3). Since no significant relationship was observed between gender and positive and negative ER, this variable was not confounding (P>0.05).
The effectiveness of ACT was studied in the positive and negative ER of cardiac patients referred to the cardiac rehabilitation department. The repeated-measures ANOVA reflected changes in the ER by controlling the pre-test scores between the ACT and control groups. Considering the level of significance and the eta-squared (89%), ACT was effective on positive and negative ER in the studied patients (P<0.001) (Table 4).
The effectiveness of GI was studied in the positive and negative ER of cardiac patients referred to the cardiac rehabilitation department. The results indicated that (after controlling the pre-test data) the GI group presented higher effects on positive ER, compared with the control group (eta-squared, 81%; P<0.001). However, GI was ineffective on negative ER (P=0.103) (Table 4).
At each stage of the measurement, the effectiveness of ACT and GI were examined in positive ER in the studied patients. The Bonferroni post hoc test revealed a significant increase in the positive ER post-test values of the ACT group, compared with the GI and control groups (P<0.001). Besides, the differences between the two groups’ mean scores highlighted the higher effects of ACT, compared with the GI approach. Additionally, compared with the GI group, the ACT group presented significant differences in all assessment phases (P<0.001). The ACT group members achieved higher scores on positive ER (Table 5).
At each stage of the measurement, the effectiveness of ACT and GI were examined in negative ER in the studied patients. The Bonferroni post hoc test revealed a significant decrease in the negative ER post-test values of the ACT group, compared with the GI and control groups (P<0.001). Besides, the differences between the mean scores of the two groups reflected the higher effects of ACT, compared with the GI approach. Additionally, compared with the GI program, the ACT group presented significant differences in the follow-up step (P<0.001).
4. Discussion
The current findings indicated that ACT was effective on positive and negative ER in patients with cardiovascular conditions. These results are consistent with the results of Moghadamfar et al. [29] and Darvish Baseri et al. [30]. The obtained results reflected that experiential avoidance, which is the main component of psychological inflexibility in ACT, is significantly and negatively correlated with adaptive ER strategies. Therefore, the primary purpose of ACT is to reduce avoidance. Accordingly, this treatment can improve adaptive ER strategies in individuals.
Another useful process of ACT is introducing an alternative to control, namely, acceptance. The acceptance component allows the individual to accept unpleasant inner emotional experiences without trying to control them. Subsequently, such emotional experiences seem less threatening and impact less on the individual’s life. Besides, the mindfulness processes used in this treatment cause dramatic changes in the way clients use mindfulness. In other words, these processes generate attention bias in the individual and cause fostering a viewpoint of mental events, which allows the person to observe better mental events instead of considering those as part of their existence. Thus, ACT can effectively regulate an individual’s emotions owing to its emphasis on accepting experiences and performing voluntary actions [31].
Furthermore, GI was effective on positive ER in the studied patients. In this regard, Smucker et al. in 1995 and Aachen Bach in 2004 believed that individuals with incurable diseases often experience negative self-evaluation and consider themselves as the victims of difficult life situations. Such a negative evaluation, which is accompanied by mental rumination over time, leads to cognitive distortions and irrational beliefs about oneself, the world, and the future. Accordingly, these people not only encounter emotional and interpersonal problems but also experience numerous mental health symptoms, such as depression, anxiety, helplessness, insomnia, nightmares, and even suicidal ideation. By participating in GI sessions, negative thoughts, maladaptive schemas, and the traumatic mental images of their illness are first redisplayed, cognitively visualized, and reviewed with details. Then, with the changes generated in its meanings, positive thoughts and mental images are replaced by previous negative thoughts and mental images.
In such situations, on the one hand, their tolerance for sorrow, desire, and life expectancy increases, and on the other hand, their inner conflict, negative emotions, and annoying thoughts decrease. Eventually, they overcome negative thoughts and images that have taken over their level of consciousness. This process not only improves their interpersonal relationships but also reduces many of their mental health conditions, such as anxiety, negative automatic thoughts, and emotions [32]. Hackmann and Holmes and Arntz et al. investigated patients with cancer and suggested GI as an effective treatment for them. This result is because GI causes the expression, visualization, and cognitive reprocessing of negative thoughts and stressful memories. It plays an essential role in controlling psychological symptoms, such as negative automatic thoughts, mental rumination, and insomnia in different patients [4, 33].
Some limitations of the present study included the small sample size and the study restriction to one hospital in Mashhad City; these limitations should be considered in generalizing the obtained results. Besides, the interval between the post-test and follow-up phase was short. Thus, future studies could consider a continuous follow-up period to achieve more accurate data.
5. Conclusion
The present study suggested the effectiveness of ACT in positive and negative ER among patients with cardiovascular conditions. In the ACT, the purpose of emphasizing individuals’ desire for inner experiences is to assist them in coping with their disturbing thoughts, experiencing them as thoughts, becoming aware of the ineffective nature of their current plan, dealing with what is important to them in life instead of responding to the thoughts, and matching with their values. The ACT is a behavioral therapy that uses mindfulness, acceptance, and cognitive defusion skills to increase psychological flexibility.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Ahvaz Branch, Islamic Azad University (Code: IR.IAU.AHVAZ.REC.1398.012).Moreover, it received the Iranian Clinical Trials code (IRCT20190727044345N1).All ethical principles are considered in this article. The participants were informed about the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This study was extracted from PhD. dissertation of the first author at the Department of Health Psychology, Khorramshahr-Persian Gulf International Branch, Islamic Azad University, Khorramshahr.
Authors' contributions
Conceptualization and supervision: Parvin Ehteshamzade; Methodology: Abbasali Shahabi; Investigation, writing – original draft, and writing – review & editing: All authors; Data collection, data analysis, funding acquisition and resources: Abbsali Shahabi.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
We want to appreciate All patients and the staff of the Cardiac Rehabilitation Department of Imam Reza (AS) Hospital in Mashhad.
- Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin Psychol Rev. 2010; 30(2):217-37. [DOI:10.1016/j.cpr.2009.11.004] [PMID]
- Tayyari-Kalajahi B, Panah-Ali A. The effectiveness of mental imaging training on reducing anxiety and increasing happiness among heart surgery patients. Depict Health. 2016; 6(4):40-8. https://doh.tbzmed.ac.ir/Article/doh-138
- Antall GF, Kresevic D. The use of guided imagery to manage pain in an elderly orthopedic population. Orthop Nurs. 2004; 23(5):335-40. [DOI:10.1097/00006416-200409000-00012] [PMID]
- Arntz A, Tiesema M, Kindt M. Treatment of PTSD: A comparison of imaginal exposure with and without imagery rescripting. J Behav Ther Exp Psychiatry. 2007; 38(4):345-70. [DOI:10.1016/j.jbtep.2007.10.006] [PMID]
- Behrouz B. [The effectiveness of group-based acceptance and commitment therapy on post-traumatic stress disorder, coping styles, and self-efficacy in girls with abnormal grief (Persian)]. J Clin Psychol. 2016; 7(4):81-91. [DOI:10.22075/JCP.2017.2220]
- Brinkborg H, Michanek J, Hesser H, Berglund G. Acceptance and commitment therapy for the treatment of stress among social workers: A randomized controlled trial. Behav Res Ther. 2011; 49(6-7):389-98. [DOI:10.1016/j.brat.2011.03.009] [PMID]
- Yarmohammadian A, Massoumeh B, Khanbani M. The role of anxiety in patients with coronary heart disease and its relationship with personality type a behaviors. J Med Sci. 2006; 5:18. https://scholar.google.com/scholar?hl=en&as_sdt=2005&sciodt=0%2C5&cites=3861224658810895878&scipsc=&q=The+role+of+anxiety+in+patients+with+coronary+heart+disease+and+its+relationship+with+personality+type+A+behaviors&btnG=
- Issazadegan A, Aghayanzade H, Shiekhy S. [Comparison of cognitive emotion regulation strategies, optimism and life atisfaction among people with gastrointestinal and cardiovascular disease (Persian)]. Nurs Midwifery J. 2015; 13(5):440-50. http://unmf.umsu.ac.ir/browse.php?a_id=2271&sid=1&slc_lang=fa
- Dehdari T, Heidarnia A, Ramezankhani A, Sadeghian S, Ghofranipour F. Effects of progressive muscular relaxation training on quality of life in anxious patients after coronary artery bypass graft surgery. Indian J Med Res. 2009; 129(5):603-8. [PMID]
- Folke F, Parling T. Melin L. Acceptance and commitment therapy for depression: A preliminary randomized clinical trial for unemployed on long-term sick leave. Cog behav pract. 2012; 19(4):583-94. [DOI:10.1016/j.cbpra.2012.01.002]
- Foxwell R, Morley C, Frizelle D. Illness perceptions, mood and quality of life: A systematic review of coronary heart disease patients. J Psychosom Res. 2013; 75(3):211-22. [DOI:10.1016/j.jpsychores.2013.05.003] [PMID]
- Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: Model, processes and outcomes. Behaviour research and therapy. 2006; 44(1):1-25. https://www.sciencedirect.com/science/article/abs/pii/S0005796705002147
- Forman EM, Herbert JD. New directions in cognitive behavior therapy: Acceptance-based therapies. In: O’Donohue WT, Fisher JE editors. General Principles and Empirically Supported Techniques of Cognitive Behavior Therapy. New Jersey: John Wiley & Sons. 2009. https://books.google.com/books?id=W1rLL2BYPqgC&printsec=frontcover&dq
- Orsillo SM, Batten SV. Acceptance and Commitment Therapy in the treatment of posttraumatic stress disorder. Behav Modif. 2005; 29(1):95-129. [DOI:10.1177/0145445504270876] [PMID]
- Pourfaraj Omran M. [The effectiveness of acceptance and commitment group therapy in social phobia of students (Persian)]. Knowl Health. 2011; 6(2):1-5. [DOI:10.22100/jkh.v6i2.100]
- Irandoost F, Neshat-Doost HT, Nadi MA, Safary S. [The effectiveness of Acceptance and Commitment Therapy (ACT) on the rate of pain intensity in women with chronic low back pain (Persian)]. J Clin Psychol. 2014; 6(2):75-84. [DOI:10.22075/JCP.2017.2165]
- Hulbert-Williams NJ, Storey L, Wilson KG. Psychological interventions for patients with cancer: Psychological flexibility and the potential utility of Acceptance and Commitment Therapy. Eur J Cancer Care (Engl). 2015; 24(1):15-27. [DOI:10.1111/ecc.12223] [PMID]
- Rajabi S, Yazdkhasti F. [The effectiveness of acceptance and commitment group therapy on anxiety and depression in women with MS who were referred to the MS association (Persian)]. J Clin Psycol. 2014; 6(1):29-38. [DOI:10.22075/JCP.2017.2152]
- Hor M, Aghaei A, Abedi A, Attari A. [The effectiveness of acceptance and commitment therapy on depression in patients with type 2 diabetes (Persian)]. J Res Behav Sci. 2013; 11(2):121-8. https://www.sid.ir/fa/journal/ViewPaper.aspx?id=202124
- Tavakolizadeh J, Kianmehr M, Basiri Moghadam M, Pahlavan M. [Effect of guided visualization on anxiety of patients with acute coronary syndrome admitted to the cardiac intensive care unit (Persian)]. Horizon Med Sci. 2015; 21(3):147-53. [DOI:10.18869/acadpub.hms.21.3.147]
- Rees BL. Effect of relaxation with guided imagery on anxiety, depression, and self-esteem in primiparas. J Holist Nurs. 1995; 13(3):255-67. [DOI:10.1177/089801019501300307] [PMID]
- Abolghasemi SH, Saedi S. [Comparison of the efficacy of pharmacotherapy, mental imagery and gradual de-stressing with biofeedback on headache in migraine patients in Ahvaz (Persian)]. J Soc Psychol. 2010; 5(16):97-110. https://www.sid.ir/fa/journal/ViewPaper.aspx?id=145533
- Etebaryan A, Poorvali Z. [Determining the relationship between self-control and conflict resolution strategies among administrative staff of Khorasgan Azad University (Isfahan) (Persian)]. J New Approaches Educ Admi. 2008; 1(2):113-33. https://www.sid.ir/fa/journal/ViewPaper.aspx?id=114095
- Sheibani H, Sheibani KA, Amreei NN, Masrour MJ. An investigation of the effects of the acceptance and commitment therapy in groups on the cognitive strategies of emotion regulation and self-control in coronary heart disease patients. J Med Life. 2019; 12(4):361-7. [PMID] [PMCID]
- Yijing Z, Xiaoping D, Fang L, Xiaolu J, Bin W. The effects of guided imagery on heart rate variability in simulated spaceflight emergency tasks performers. Biomed Res Int. 2015; 2015:687020. [DOI:10.1155/2015/687020] [PMID] [PMCID]
- Garnefski N, Van Den kommer T, Kraaij V, Teerds J, Legerstee J, Onstein E. The relationship between cognitive emotion regulation strategies and emotional problems: Comparison between a clinical and a non-clinical sample. Eur J Pers. 2002; 16(5):403-20. [DOI:10.1002/per.458]
- Aminabadi Z, Dehghani M, Khodapanahi MK. [Factor structure and validation of the Cognitive Emotion Regulation Questionnaire (Persian)]. Int J Behav Sci. 2012; 5(4):365-71. http://www.behavsci.ir/article_67755.html
- Samani S, Jokar B, Sahragard N. [Effects of resilience on mental health and life satisfaction (Persian)]. Iran J Psychiatry Clin Psychol. 2007; 13(3):290-5. http://ijpcp.iums.ac.ir/article-1-275-en.html
- Moghadamfar N, Amraei R, Asadi F, Amani O. [The efficacy of Acceptance and Commitment Therapy (ACT) on hope and psychological well-being in women with breast cancer under chemotherapy (Persian)]. Iran J Psychiatr Nurs. 2018; 6(5):1-7. https://ijpn.ir/browse.php?a_id=1155&sid=1&slc_lang=fa&ftxt=1
- Darvish Baseri L, DashtBozorgi Z. [Effectiveness of group therapy based on acceptance and commitment on cognitive emotion regulation and alexithymia of patients with type 2 diabetes (Persian)]. Iran J Psychiatric Nurs. 2017; 5(1):7-14. [DOI:10.21859/ijpn-05012]
- Jahangiri A, Shirdal M, Gharachoorlou S. [The effectiveness of Acceptance and Commitment (Act) Therapy on cognitive-emotional regulation and self-efficacy in struggling with problems in people with substance abuse treated with methadone (Persian)]. North Khorasan J Med Sci. 2018; 10(2):41-9. http://journal.nkums.ac.ir/browse.php?a_id=1517&sid=1&slc_lang=en
- Smucker MR, Dancu C, Foa EB, Niederee JL. Imagery rescripting: A new treatment for survivors of childhood sexual abuse suffering from posttrumatic stress. J Cogn Psychother. 1995; 9(1):3-17. [DOI:10.1891/0889-8391.9.1.3]
- Hackmann, A. Holmes EA. Reflecting on imagery: A clinical perspective and overview of the special issue of memory on mental imagery and memory in psychopathology. Memory. 2004; 12(4):389-402. [DOI:10.1080/09658210444000133] [PMID]
Type of Study: Orginal Article |
Subject:
● International Health
Received: 2019/07/16 | Accepted: 2020/07/20 | Published: 2021/06/1
Received: 2019/07/16 | Accepted: 2020/07/20 | Published: 2021/06/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
