

Volume 14, Issue 6 (Nov & Dec 2024)
J Research Health 2024, 14(6): 593-598 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Faramarzizadeh F, Ramezankhani A, Ghaffari M, Namdari M. Effect of Food Traffic Light Training on Mother’s Knowledge, Attitude and Practice. J Research Health 2024; 14 (6) :593-598
URL: http://jrh.gmu.ac.ir/article-1-2415-en.html
URL: http://jrh.gmu.ac.ir/article-1-2415-en.html



1- Department of Public Health, School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran. , Fereshteh.faramarzi@sbmu.ac.ir
2- Department of Public Health, School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Department of Oral Health Community, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Public Health, School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Department of Oral Health Community, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 775 kb]
(831 Downloads)
| Abstract (HTML) (3555 Views)
Full-Text: (986 Views)
Introduction
Noncommunicable diseases (NCDs) associated with premature mortality are one of the major concerns for health supervising organizations worldwide [1]. An unhealthy diet is one of the five modifiable behavioral risk factors for NCDs. The World Health Organization (WHO) has issued a global action plan with nine distinct action targets to prevent and control NCDs. Accordingly, a comprehensive program, which includes 13 goals, was developed for NCD management in Iran. Among these goals, examples of food-related milestones in the Iranian national action plan for the period from 2015 to 2025 include a “4.30% relative reduction in the average salt intake,” “zero trans fatty acids in oily products,” and “a halt to the rising rates of diabetes and obesity” [2]. To promote a healthy diet, providing point-of-choice information is a potentially effective strategy [3]. Various forms of point-of-choice information have been implemented in food service [4], with the most widely recognized and applied approaches including nutrition facts labeling [5] and calorie labeling [6, 7]. The complex information found on nutrition fact labels poses challenges for consumers when selecting healthier foods [8, 9]. Despite its simplicity, calorie labeling has not shown significant effects on consumer food choices and caloric intake, according to a recent review and meta-analysis [6, 7]. Another simplified food-labeling method uses colors to inform customers and facilitate healthy food choices. This system uses the red, yellow, and green labels of traffic light (TL) colors to represent ‘unhealthy food/stop’, ‘moderately unhealthy food/wait and watch’, and ‘healthy food/go’, respectively (Figure 1), [10].
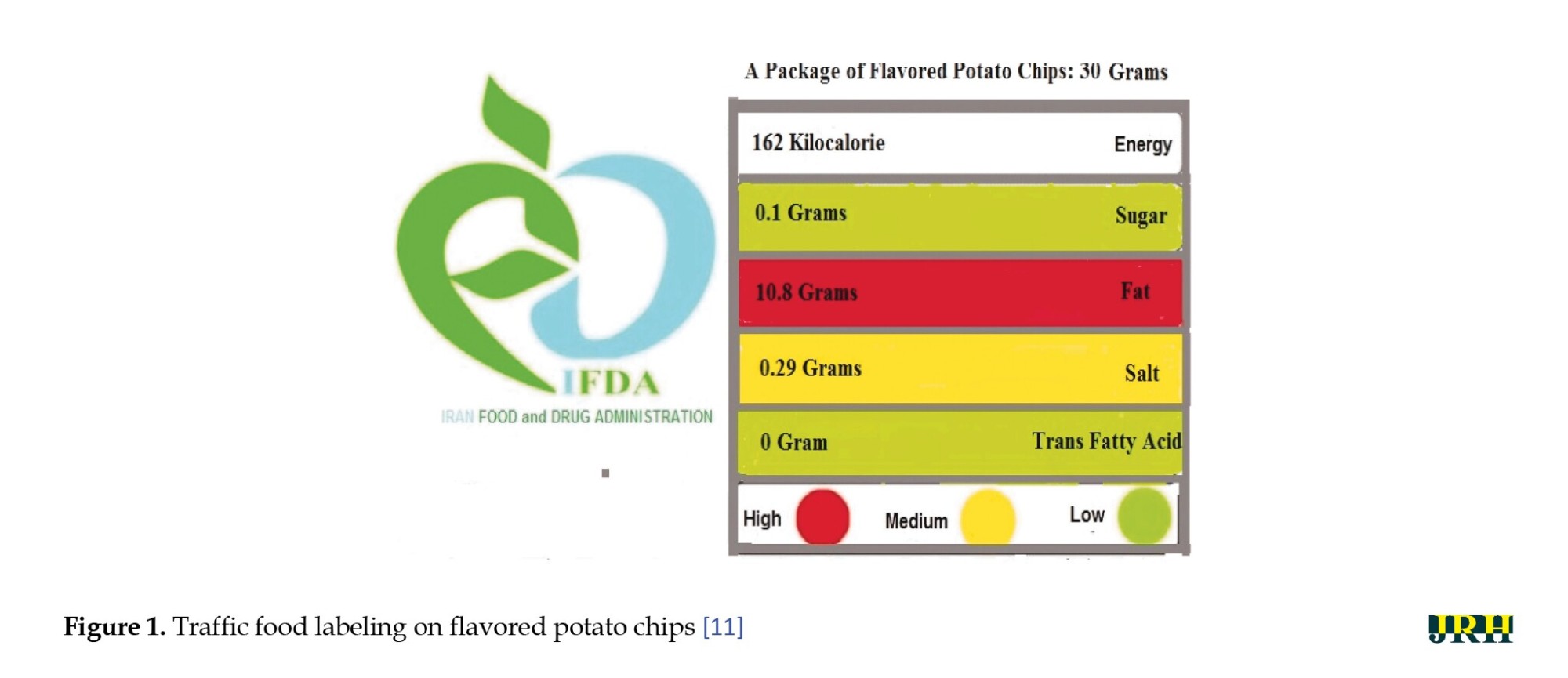
In Iran, TL application in food labeling has become commonplace, as mandated by the Iran Food and Drug Administration (IFDA) in collaboration with food manufacturers since 2015. The use of TL on food labeling has become compulsory for every industrially produced food item [11]. Behavioral trials have revealed that the use of colors effectively guides consumers in making informed decisions for healthier food choices [12]. This study aimed to investigate the effect of education through WhatsApp on mother’s knowledge, attitude, and practice about healthy food choices in Tehran, Iran.
Methods
Study design and subjects
In this interventional semi-experimental study, 84 mothers covered by the health centers of Shahid Beheshti University of Medical Sciences, Tehran, Iran, participated. They were randomly divided into the intervention and control groups (42 participants in each group). The research community consisted of three regions of the Shemiranat health networks: Tehran North and Tehran East, which were selected using a cluster sampling method. Two health centers were randomly selected as sampling centers from each network. The difference between the two groups was measured with the maximum type 1 and type 2 errors of 5% and 10%, respectively. Also, considering the amount of difference between the two methods, d was 5 and the standard deviation (SD) was 6. According to the Equation 1:

, the number of samples in each group was calculated to be 31, accounting for a 25% probability of loss. Ultimately, 42 participants were included in each group, resulting in a total of 84 mothers in the study (n=42 in each group). Also, the allocation of samples to the intervention and control groups was done by generating random blocks using Excel software [12].
A WhatsApp group was then created for information exchange, and educational messages were forwarded through text, images, videos, and a researcher-made booklet titled “food TL: A way to choose a healthy life.” The training sessions were held for six weeks, consisting of 12 sessions held on Monday and Wednesday mornings at 10 AM, from June 15 to August 15, 2022. Then, the research purpose, methods, and importance were explained to the mothers and written consent was collected after receiving ethical approval from the Shahid Beheshti University of Medical Sciences. The inclusion criterion included the provision of consent to participate. Exclusion criteria were reluctance to participate in the research, absence from sessions, failure to study the content and incomplete questionnaires.
Data collection
Data were collected through a demographic questionnaire and a standard questionnaire measuring knowledge, attitude, and practice, whose validity was affirmed by Esfandiari et al. [13]. To measure the questionnaire’s reliability, it was completed by 24 mothers who were not part of the intervention and control groups, yielding a Cronbach’s α between 0.64 and 0.76. In addition, the validity of the questionnaire was evaluated by faculty members from the School of Public Health and Safety and the School of Nutrition at Shahid Beheshti University of Medical Sciences.
The questionnaire was designed in three sections, including knowledge, attitude, and practice, along with the demographic characteristics of the respondents. The demographic section included general information, such as age, weight, employment status, educational level and marital status.
In the knowledge section, there were 11 questions focused on NCDs, TL labeling and its colors, and the relationship between risk factors. This section assessed knowledge regarding TL and NCDs. Each question had two possible answers: True or false, assigned scores of 1 and 0, respectively. For example, one of the questions was, “Does the color green in TL food labeling visually indicate a healthy food choice?” Participants answered either “yes” or “no” to this question.
The next part of the questionnaire addressed the attitudes of the respondents about the significance of TL food labeling. For example, a question was asked about the attitude toward TL labeling, such as whether the inappropriate choice of food can significantly impact health conditions and lead to high medical treatment expenditures, or whether paying attention to the amount of energy in TL food labeling plays an important role in preventing overweight and obesity. In total, five statements were given, and each respondent was requested to indicate her level of agreement using a five-point rating scale (i.e. strongly disagree, disagree, uncertain, agree, and strongly agree), with scores ranging between 0 and 20. The practices of respondents were evaluated by their self-reported purchasing behaviors in the last section of the questionnaire. For instance, we asked participants if they chose a food product based on the amount of energy in TL food labeling when making food purchases. This section included six questions, scored from 0 to 24, using a 5-point rating scale (never, seldom, sometimes, often and always).
Statistical analysis
To assess the normal distribution of the data, we used the Kolmogorov-Smirnov test, while the chi-square test and t-test were employed to evaluate demographic and independent variables. Data were collected using a questionnaire at three stages: Pre-test, first post-test (a week after the intervention) and second post-test (a month after the intervention) and analyzed by repeated measures ANOVA across the three different time points of the study. SPSS software, version 21 was utilized for data analysis and a P<0.05 was considered significant for the analysis.
Results
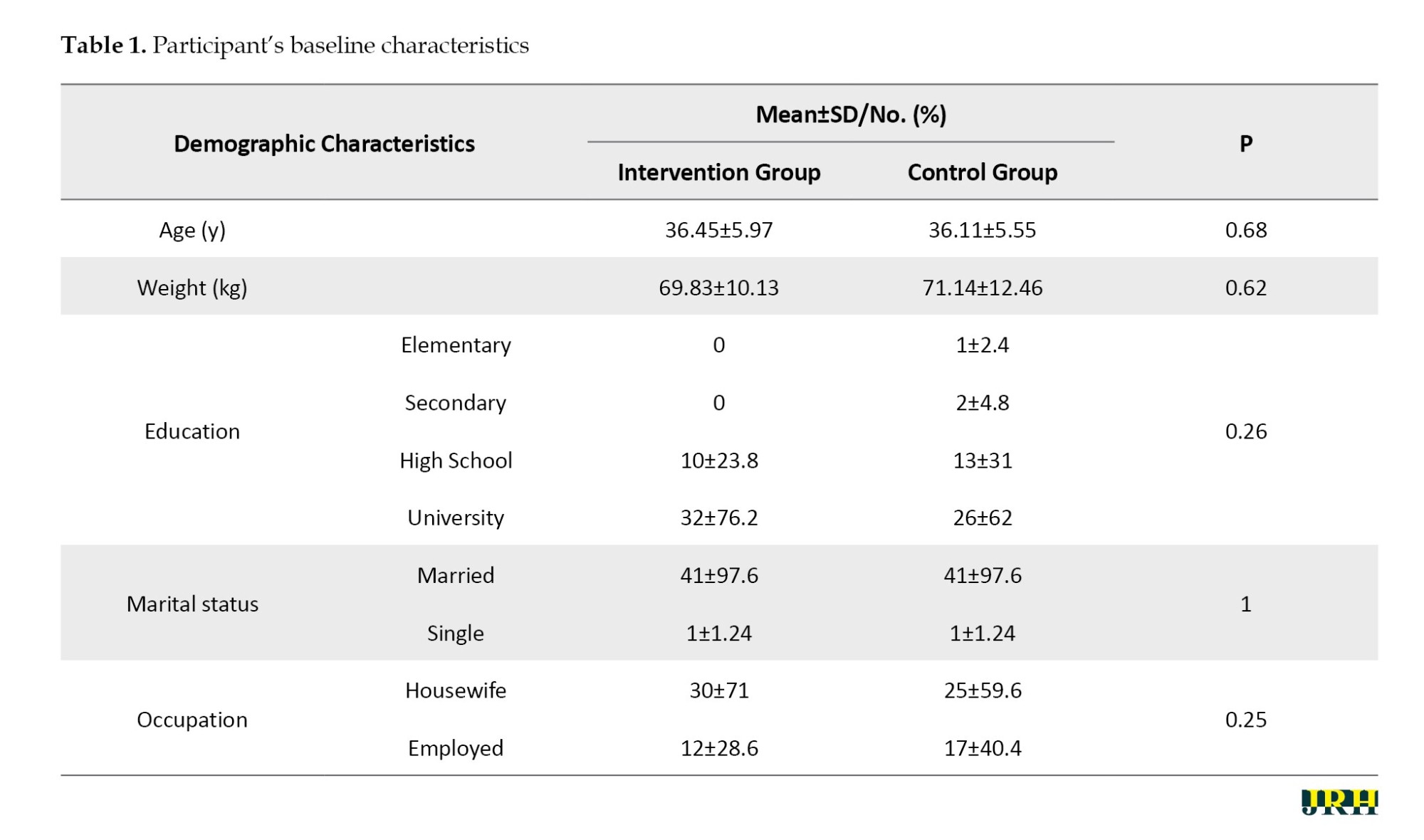
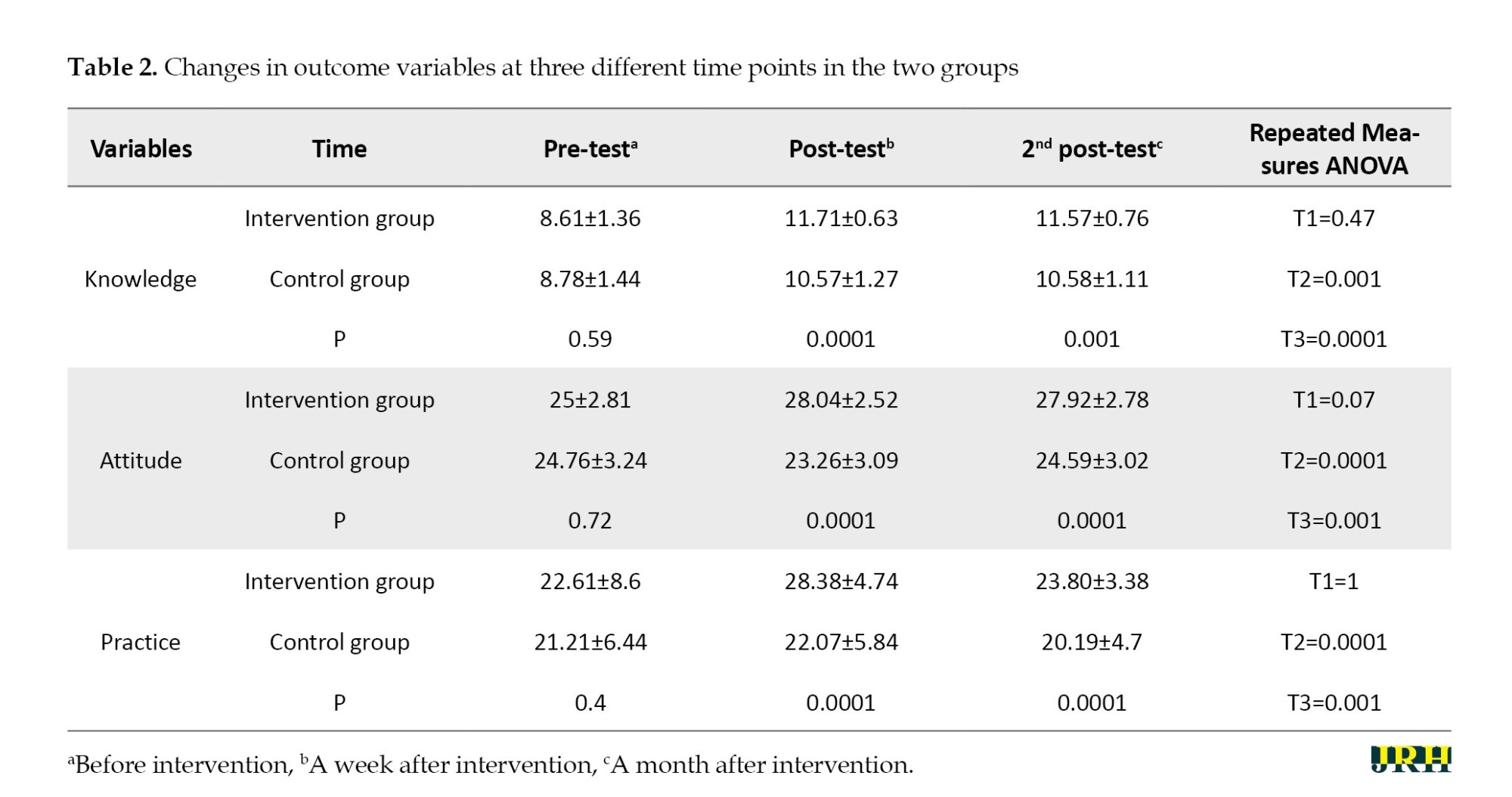
There was no significant relationship between age, weight, marital status and educational and employment status in the two groups (P<0.05; Table 1). Table 2 shows the changes in the main three variables across three different testing times for both groups. The repeated measures ANOVA results and the scores from participants’ responses to questions assessing their knowledge of dietary risk factors for NCDs and the corresponding colors in TL labeling are presented. Despite a high percentage of general information on diet dependency, respondents had very limited understanding of dietary risk factors for NCDs, as well as information about color and the five indicators affecting health, before the intervention (knowledge pre-test score=0.59). However, after the educational intervention, mothers’ knowledge about the colors of the TL and the five indicators affecting health (energy, sugar, fat, salt and trans fatty acids) increased significantly (P=0.0001). In the second post-test, the repeated measures ANOVA results illustrated a considerable change (P=0.001).
The results of the attitude assessment indicated that, before education, the majority agreed that an unhealthy diet resulted in medical expenses (pre-test P=0.72; Table 2). Also, the level of awareness regarding the importance of food TL labeling and the amounts of energy, sugar, fat, salt, and trans-fatty acids contained in food was low, but this increased significantly after the educational intervention (P=0.0001; Table 2).
The same trend in attitude was observed when respondents were asked whether TL literacy affects NCD prevention in the second post-test (P=0.0001). Regarding practice questions about choosing a food product based on the TL food label, before, considerable changes were noted before the intervention, one week after and one month after the intervention. The repeated measures ANOVA results for the three different tests were respectively as follows: Pre-test P=0.40, post-test P=0.0001, and second post-test P=0.0001; Table 2).
Discussion
The present study was conducted to investigate the effect of food TL training on mother’s knowledge, attitude, and practice. According to the results, education significantly affected the knowledge, attitude, and practice of mothers after intervention. In nutrition education, familiarization with and usage of information on food labeling, specifically TL labeling, is important. This study is the first of its kind in Iran, examining mothers’ knowledge, attitude, and practice toward TL food labeling and whether TL education positively affects consumer understanding and behavior. According to the WHO, Iran has been ranked first for developing and implementing the NCD national action plan, which has led to desired prevention and control outcomes [14, 15].
However, the previously provided information did not independently address TL literacy. Several studies have shown that most food consumers tend to include nutritional considerations in their choices, but they struggle to evaluate and understand nutritional information carefully. Obstacles, such as insufficient consumer knowledge and the features that a food product offers, along with the complex information on nutrition fact labels, make it challenging for consumers to choose healthier foods [8, 9]. Despite its simplicity, calorie labeling did not have significant effects on consumer food choices and caloric intake, according to a recent review and meta-analysis [6, 7]. In an online project, a fairly high rate (5.9 out of 7) of understandability of the TL labeling was indicated by German undergraduate students [16]. Also, it was found that the TL model may provide supplementary knowledge by improving consumers’ interpretation of nutritional information in a study performed in the UK [17]. In a study by Graham et al. in the United States, which examined nutrition label use through an online survey among university students, it was shown that using food labels could change healthy eating attitudes and overall dietary quality [18]. On the other hand, the literature shows that the cues from red and green labels may have different effects on customer’s food choices. A UK study has shown that, although red labels directed shoppers away from an item, green labels did not encourage shoppers to an item [19]. It is evident from the results of this intervention that respondents with a high degree of knowledge and attitudes acted appropriately in choosing healthier food products and healthy behavior.
This revealed that TL information may serve as a positive approach to nutrition education for Iranian mothers to help them choose healthy foods. In a recent study with a small population focused on Iranian university students, it was observed that education on TL labeling played a significant role in improving knowledge and attitudes, and to some extent, enhanced participants’ practices for selecting healthier food [13].
Conclusion
The results of the present study showed that the knowledge, attitude, and practice of mothers about food TLs on food products were low before the intervention, indicating that food labels were not a decision-making factor for purchasing food products prior to education. After the educational intervention, an improvement was observed in the scores of knowledge, attitude, and practice, which depicts a significant positive association between the educational intervention and the knowledge, attitude, and practice of the studied population. This suggests that TL labeling may influence consumers who choose to adopt a healthier lifestyle to purchase healthier food. In the second post-test, the results also depicted considerable changes, reflecting the effects of the intervention, which indicates that the training has remained effective. This study had no limitations other than unrestricted access to the internet. Furthermore, despite the general knowledge about the risk factors for NCDs, a nationwide awareness campaign is needed to promote the utilization of TL labeling and food label information as decision-making tools for choosing a healthier diet among consumers in Iran. In addition, it is recommended to conduct further studies on how to achieve full acceptance of food labels among Iranian consumers in the long term.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (Code: IR.SBMU.PHNS.REC.1400.148).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All the authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely extend their appreciation to the individuals who contributed to the realization and development of this study, particularly the Department of School Health and Safety at Shahid Beheshti University of Medical Sciences in Tehran, Iran.
References
Noncommunicable diseases (NCDs) associated with premature mortality are one of the major concerns for health supervising organizations worldwide [1]. An unhealthy diet is one of the five modifiable behavioral risk factors for NCDs. The World Health Organization (WHO) has issued a global action plan with nine distinct action targets to prevent and control NCDs. Accordingly, a comprehensive program, which includes 13 goals, was developed for NCD management in Iran. Among these goals, examples of food-related milestones in the Iranian national action plan for the period from 2015 to 2025 include a “4.30% relative reduction in the average salt intake,” “zero trans fatty acids in oily products,” and “a halt to the rising rates of diabetes and obesity” [2]. To promote a healthy diet, providing point-of-choice information is a potentially effective strategy [3]. Various forms of point-of-choice information have been implemented in food service [4], with the most widely recognized and applied approaches including nutrition facts labeling [5] and calorie labeling [6, 7]. The complex information found on nutrition fact labels poses challenges for consumers when selecting healthier foods [8, 9]. Despite its simplicity, calorie labeling has not shown significant effects on consumer food choices and caloric intake, according to a recent review and meta-analysis [6, 7]. Another simplified food-labeling method uses colors to inform customers and facilitate healthy food choices. This system uses the red, yellow, and green labels of traffic light (TL) colors to represent ‘unhealthy food/stop’, ‘moderately unhealthy food/wait and watch’, and ‘healthy food/go’, respectively (Figure 1), [10].
In Iran, TL application in food labeling has become commonplace, as mandated by the Iran Food and Drug Administration (IFDA) in collaboration with food manufacturers since 2015. The use of TL on food labeling has become compulsory for every industrially produced food item [11]. Behavioral trials have revealed that the use of colors effectively guides consumers in making informed decisions for healthier food choices [12]. This study aimed to investigate the effect of education through WhatsApp on mother’s knowledge, attitude, and practice about healthy food choices in Tehran, Iran.
Methods
Study design and subjects
In this interventional semi-experimental study, 84 mothers covered by the health centers of Shahid Beheshti University of Medical Sciences, Tehran, Iran, participated. They were randomly divided into the intervention and control groups (42 participants in each group). The research community consisted of three regions of the Shemiranat health networks: Tehran North and Tehran East, which were selected using a cluster sampling method. Two health centers were randomly selected as sampling centers from each network. The difference between the two groups was measured with the maximum type 1 and type 2 errors of 5% and 10%, respectively. Also, considering the amount of difference between the two methods, d was 5 and the standard deviation (SD) was 6. According to the Equation 1:
, the number of samples in each group was calculated to be 31, accounting for a 25% probability of loss. Ultimately, 42 participants were included in each group, resulting in a total of 84 mothers in the study (n=42 in each group). Also, the allocation of samples to the intervention and control groups was done by generating random blocks using Excel software [12].
A WhatsApp group was then created for information exchange, and educational messages were forwarded through text, images, videos, and a researcher-made booklet titled “food TL: A way to choose a healthy life.” The training sessions were held for six weeks, consisting of 12 sessions held on Monday and Wednesday mornings at 10 AM, from June 15 to August 15, 2022. Then, the research purpose, methods, and importance were explained to the mothers and written consent was collected after receiving ethical approval from the Shahid Beheshti University of Medical Sciences. The inclusion criterion included the provision of consent to participate. Exclusion criteria were reluctance to participate in the research, absence from sessions, failure to study the content and incomplete questionnaires.
Data collection
Data were collected through a demographic questionnaire and a standard questionnaire measuring knowledge, attitude, and practice, whose validity was affirmed by Esfandiari et al. [13]. To measure the questionnaire’s reliability, it was completed by 24 mothers who were not part of the intervention and control groups, yielding a Cronbach’s α between 0.64 and 0.76. In addition, the validity of the questionnaire was evaluated by faculty members from the School of Public Health and Safety and the School of Nutrition at Shahid Beheshti University of Medical Sciences.
The questionnaire was designed in three sections, including knowledge, attitude, and practice, along with the demographic characteristics of the respondents. The demographic section included general information, such as age, weight, employment status, educational level and marital status.
In the knowledge section, there were 11 questions focused on NCDs, TL labeling and its colors, and the relationship between risk factors. This section assessed knowledge regarding TL and NCDs. Each question had two possible answers: True or false, assigned scores of 1 and 0, respectively. For example, one of the questions was, “Does the color green in TL food labeling visually indicate a healthy food choice?” Participants answered either “yes” or “no” to this question.
The next part of the questionnaire addressed the attitudes of the respondents about the significance of TL food labeling. For example, a question was asked about the attitude toward TL labeling, such as whether the inappropriate choice of food can significantly impact health conditions and lead to high medical treatment expenditures, or whether paying attention to the amount of energy in TL food labeling plays an important role in preventing overweight and obesity. In total, five statements were given, and each respondent was requested to indicate her level of agreement using a five-point rating scale (i.e. strongly disagree, disagree, uncertain, agree, and strongly agree), with scores ranging between 0 and 20. The practices of respondents were evaluated by their self-reported purchasing behaviors in the last section of the questionnaire. For instance, we asked participants if they chose a food product based on the amount of energy in TL food labeling when making food purchases. This section included six questions, scored from 0 to 24, using a 5-point rating scale (never, seldom, sometimes, often and always).
Statistical analysis
To assess the normal distribution of the data, we used the Kolmogorov-Smirnov test, while the chi-square test and t-test were employed to evaluate demographic and independent variables. Data were collected using a questionnaire at three stages: Pre-test, first post-test (a week after the intervention) and second post-test (a month after the intervention) and analyzed by repeated measures ANOVA across the three different time points of the study. SPSS software, version 21 was utilized for data analysis and a P<0.05 was considered significant for the analysis.
Results
There was no significant relationship between age, weight, marital status and educational and employment status in the two groups (P<0.05; Table 1). Table 2 shows the changes in the main three variables across three different testing times for both groups. The repeated measures ANOVA results and the scores from participants’ responses to questions assessing their knowledge of dietary risk factors for NCDs and the corresponding colors in TL labeling are presented. Despite a high percentage of general information on diet dependency, respondents had very limited understanding of dietary risk factors for NCDs, as well as information about color and the five indicators affecting health, before the intervention (knowledge pre-test score=0.59). However, after the educational intervention, mothers’ knowledge about the colors of the TL and the five indicators affecting health (energy, sugar, fat, salt and trans fatty acids) increased significantly (P=0.0001). In the second post-test, the repeated measures ANOVA results illustrated a considerable change (P=0.001).
The results of the attitude assessment indicated that, before education, the majority agreed that an unhealthy diet resulted in medical expenses (pre-test P=0.72; Table 2). Also, the level of awareness regarding the importance of food TL labeling and the amounts of energy, sugar, fat, salt, and trans-fatty acids contained in food was low, but this increased significantly after the educational intervention (P=0.0001; Table 2).
The same trend in attitude was observed when respondents were asked whether TL literacy affects NCD prevention in the second post-test (P=0.0001). Regarding practice questions about choosing a food product based on the TL food label, before, considerable changes were noted before the intervention, one week after and one month after the intervention. The repeated measures ANOVA results for the three different tests were respectively as follows: Pre-test P=0.40, post-test P=0.0001, and second post-test P=0.0001; Table 2).
Discussion
The present study was conducted to investigate the effect of food TL training on mother’s knowledge, attitude, and practice. According to the results, education significantly affected the knowledge, attitude, and practice of mothers after intervention. In nutrition education, familiarization with and usage of information on food labeling, specifically TL labeling, is important. This study is the first of its kind in Iran, examining mothers’ knowledge, attitude, and practice toward TL food labeling and whether TL education positively affects consumer understanding and behavior. According to the WHO, Iran has been ranked first for developing and implementing the NCD national action plan, which has led to desired prevention and control outcomes [14, 15].
However, the previously provided information did not independently address TL literacy. Several studies have shown that most food consumers tend to include nutritional considerations in their choices, but they struggle to evaluate and understand nutritional information carefully. Obstacles, such as insufficient consumer knowledge and the features that a food product offers, along with the complex information on nutrition fact labels, make it challenging for consumers to choose healthier foods [8, 9]. Despite its simplicity, calorie labeling did not have significant effects on consumer food choices and caloric intake, according to a recent review and meta-analysis [6, 7]. In an online project, a fairly high rate (5.9 out of 7) of understandability of the TL labeling was indicated by German undergraduate students [16]. Also, it was found that the TL model may provide supplementary knowledge by improving consumers’ interpretation of nutritional information in a study performed in the UK [17]. In a study by Graham et al. in the United States, which examined nutrition label use through an online survey among university students, it was shown that using food labels could change healthy eating attitudes and overall dietary quality [18]. On the other hand, the literature shows that the cues from red and green labels may have different effects on customer’s food choices. A UK study has shown that, although red labels directed shoppers away from an item, green labels did not encourage shoppers to an item [19]. It is evident from the results of this intervention that respondents with a high degree of knowledge and attitudes acted appropriately in choosing healthier food products and healthy behavior.
This revealed that TL information may serve as a positive approach to nutrition education for Iranian mothers to help them choose healthy foods. In a recent study with a small population focused on Iranian university students, it was observed that education on TL labeling played a significant role in improving knowledge and attitudes, and to some extent, enhanced participants’ practices for selecting healthier food [13].
Conclusion
The results of the present study showed that the knowledge, attitude, and practice of mothers about food TLs on food products were low before the intervention, indicating that food labels were not a decision-making factor for purchasing food products prior to education. After the educational intervention, an improvement was observed in the scores of knowledge, attitude, and practice, which depicts a significant positive association between the educational intervention and the knowledge, attitude, and practice of the studied population. This suggests that TL labeling may influence consumers who choose to adopt a healthier lifestyle to purchase healthier food. In the second post-test, the results also depicted considerable changes, reflecting the effects of the intervention, which indicates that the training has remained effective. This study had no limitations other than unrestricted access to the internet. Furthermore, despite the general knowledge about the risk factors for NCDs, a nationwide awareness campaign is needed to promote the utilization of TL labeling and food label information as decision-making tools for choosing a healthier diet among consumers in Iran. In addition, it is recommended to conduct further studies on how to achieve full acceptance of food labels among Iranian consumers in the long term.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (Code: IR.SBMU.PHNS.REC.1400.148).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All the authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely extend their appreciation to the individuals who contributed to the realization and development of this study, particularly the Department of School Health and Safety at Shahid Beheshti University of Medical Sciences in Tehran, Iran.
References
- World Health Organization (WHO). Global status report on non-communicable diseases. Geneva: World Health Organization; 2014. [Link]
- Peykari N, Hashemi H, Dinarvand R, Haji-Aghajani M, Malekzadeh R, Sadrolsadat A, et al. National action plan for non-communicable diseases prevention and control in Iran; a response to emerging epidemic. Journal of Diabetes & Metabolic Disorders. 2017; 16(3):1-7. [DOI:10.1186/s40200-017-0288-4]
- Zhang X, Ouyang Y, Yin X, Bai J, Zhang R, Zhang J, et al. Consumers’ Perceptions of the design of front-of-package warning labels-a qualitative study in China. Nutrients. 2023; 15(2):415. [DOI:10.3390/nu15020415]
- Gittelsohn J, Lee-Kwan SH, Batorsky B. Community-based interventions in prepared-food sources: A systematic review. Preventing Chronic Disease. 2013; 10:E180. [DOI:10.5888/pcd10.130073]
- World Health Organization (WHO). Global nutrition policy review: What does it take to scale up nutrition action? Geneva: World Health Organization; 2013. [Link]
- Kiszko KM, Martinez OD, Abrams C, Elbel B. The influence of calorie labeling on food orders and consumption: A review of the literature. Journal of Community Health. 2014; 39(6):1248-69. [DOI:10.1007/s10900-014-9876-0]
- Long MW, Tobias DK, Cradock AL, Batchelder H, Gortmaker SL. Systematic review and meta-analysis of the impact of restaurant menu calorie labeling. American Journal of Public Health. 2015; 105(5):e11e24. [DOI:10.2105/AJPH.2015.302570]
- Graham DJ, Roberto CA. Evaluating the impact of U.S. Food and Drug Administration-proposed nutrition facts label changes on young adults’ visual attention and purchase intentions. Health Education & Behavior. 2016; 43(4):389e98. [DOI:10.1177/1090198116651082]
- Nelson D, Graham D, Harnack L. An objective measure of nutrition facts panel usage and nutrient quality of food choice. Journal of Nutrition Education and Behavior. 2014; 46(6):589e94. [DOI:10.1016/j.jneb.2014.04.296]
- Trudel R, Murray KB, Kim S, Chen S. The impact of traffic light color-coding on food health perceptions and choice. Journal of Experimental Psychology. 2015; 21(3):255e75. [DOI:10.1037/xap0000049]
- Iran Food and Drug Administration. [Act for a traffic light on food labeling with No. 688/479/dated 13 June 2015 technical and legal committee of the general directorate of monitoring and evaluation of edible, cosmetic and health products of the food and drug organization. Tehran: Iran Food and Drug Administration; 2015. [Link]
- Chan YH. Biostatistics 301. Repeated measurement analysis. Singapore Medical Journal. 2004; 45(8):354-68. [PMID]
- Esfandiari Z, Mirlohi M, Tanha JM, Hadian M, Mossavi SI, Ansariyan A, et al. Effect of face-to-face education on knowledge, attitudes, and practices toward "traffic light" food labeling in Isfahan society, Iran. Community Health Equity Research & Policy. 2021; 41(3):275-84. [DOI: 10.1177/0272684X20916612] [PMID]
- Khosravi Shadmani F, Farzadfar F, Larijani B, Mirzaei M, Haghdoost AA. Trend and projection of mortality rate due to NCDs in Iran: A modeling study. Plos One. 2019; 14:2. [DOI:10.1371/journal.pone.0211622]
- Chien TY, Chien YW, Chang JS, Chen YC. Influence of mothers’ nutrition knowledge and attitudes on their purchase intention for infant cereal with no added sugar claim. Nutrients. 2018; 10(4):435. [DOI:10.3390/nu10040435]
- Hieke S, Wilczynski P. Colour me in-an empirical study on consumer responses to the traffic light signposting system in nutrition labeling. Public Health Nutrition. 2012; 15(5):773-82. [DOI:10.1017/S1368980011002874]
- Jones G, Richardson M. An objective examination of consumer perception of nutrition information based on healthiness rating and eye movements. Public Health Nutrition. 2007; 10(3):238-44. [DOI:10.1017/S1368980007258513]
- Graham DJ, Laska MN. Nutrition label use partially mediated the relationship between attitudes toward healthy eating and overall dietary quality among college students. Journal of the Academy of Nutrition and Dietetics. 2012; 112(3):414-8. [DOI:10.1016/j.jada.2011.08.047]
- Scarborough P, Matthews A, Eyles H, Kaur A, Hodgkins C, Raats MM, et al. Reds are more important than greens: how UK supermarket shoppers use the different information on a traffic light nutrition label in a choice experiment. International Journal of Behavioral Nutrition and Physical Activity. 2015; 12:151. [DOI:10.1186/s12966-015-0319-9]
Type of Study: Short Communication |
Subject:
● Health Education
Received: 2023/09/1 | Accepted: 2023/12/31 | Published: 2024/10/28
Received: 2023/09/1 | Accepted: 2023/12/31 | Published: 2024/10/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
