

Volume 14, Issue 6 (Nov & Dec 2024)
J Research Health 2024, 14(6): 555-566 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yazdanpanah F, Nasirzadeh M, Ahmadinia H, Abdolkarimi M, Askari F. Effectiveness of Educational Intervention Based on the Extended Theory of Planned Behavior on Exclusive Breastfeeding. J Research Health 2024; 14 (6) :555-566
URL: http://jrh.gmu.ac.ir/article-1-2449-en.html
URL: http://jrh.gmu.ac.ir/article-1-2449-en.html
Farahnaz Yazdanpanah1 

 , Mostafa Nasirzadeh2 , Hassan Ahmadinia3 , Mahdi Abdolkarimi4 , Fatemeh Askari5
, Mostafa Nasirzadeh2 , Hassan Ahmadinia3 , Mahdi Abdolkarimi4 , Fatemeh Askari5
, Mostafa Nasirzadeh2 , Hassan Ahmadinia3 , Mahdi Abdolkarimi4 , Fatemeh Askari5
1- Student Research Committee, Department of Health Education and Health Promotion, School of Health, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
2- Department of Health Education and Health Promotion, Occupational Health and Safety Research Center, School of Health, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
3- Department of Epidemiology and Biostatics, School of Medicine, Rafsanjani University of Medical Sciences, Rafsanjan, Iran.
4- Department of Health Education and Health Promotion, Geriatric Care Research Center, School of Health, Rafsanjan University of Medical Sciences, Rafsanjan, Iran. ,Mahdi_13581@yahoo.com
5- Niknafs Maternity Hospital, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
2- Department of Health Education and Health Promotion, Occupational Health and Safety Research Center, School of Health, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
3- Department of Epidemiology and Biostatics, School of Medicine, Rafsanjani University of Medical Sciences, Rafsanjan, Iran.
4- Department of Health Education and Health Promotion, Geriatric Care Research Center, School of Health, Rafsanjan University of Medical Sciences, Rafsanjan, Iran. ,
5- Niknafs Maternity Hospital, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
Full-Text [PDF 939 kb]
(1452 Downloads)
| Abstract (HTML) (3860 Views)
Full-Text: (1076 Views)
Introduction
The World Health Organization (WHO) defines exclusive breastfeeding (EBF) as breastfeeding an infant exclusively, without the introduction of other foods or even water, except for medication, oral rehydration solutions, vitamins and supplements [1]. In addition to providing the most appropriate physical growth for the baby and meeting the emotional needs of the infant and mother, breast milk plays a vital role in preventing gastrointestinal and respiratory infections [2]. It also provides maternal health and well-being by affecting gestational age and reducing the risk of breast and ovarian cancer [3]. However, even in developed countries, the rate of EBF has been reported to be low [4]. At the 65th meeting of the WHO, it was decided to increase the rate of EBF to 50% by 2025. This figure differs significantly in developing countries, ranging from 13% to 77% in Iran [5]. A study in Riyadh showed that despite the start of breastfeeding, only 20.9% continue to be exclusively breastfed [6]. The results of the latest studies conducted in a review study on EBF showed that despite the emphasis of Iran Ministry of Health and Medical Education and the concern of health policymakers to increase this index, only about half of women adhere to EBF [7]. Therefore, it is necessary to determine effective interventions to promote this behavior for the health of mothers and babies.
Early cessation of breastfeeding causes physical, psychological, and socio-economic damage to the child and society [8]. Subjective norms among lactating and postpartum women, including the views of significant individuals, such as peers and social networks and important family members, such as spouses, parents, or siblings, are important factors in breastfeeding [9].
One of the theories that influence behavior change in response to social norms is the theory of planned behavior (TPB), which was developed in 1991 by Ajzen and Fishbein [10]. The TPB includes the following constructs: Behavioral intention, attitude toward behavior, subjective norms and perceived behavioral control (PBC) [10]. The TPB is a behavioral theory in social psychology that analyzes the factors affecting behavioral goals and explains the behavior. It points out that the main predictor of behavior is a change in behavior intention that depends on individuals’ attitudes, subjective norms, and PBC [11]. This theory, which has been applied to many health behaviors, explains, on average, about 40% of the relationship between intention and health behaviors [12]. One of the criticisms of the TPB is the lack of attention to social factors affecting behavior. Numerous studies have emphasized the role of social support, especially the spouse’s involvement, in initiating and continuing EBF [13, 14]. Breastfeeding is a behavior that requires the knowledge, skills, support, and confidence of the mother [15]. Social factors, including the support of social groups, significantly affect breastfeeding mothers [16].
On the other hand, some researchers believe that self-efficacy predicts the behavior’s occurrence better than the PBC for some behaviors, such as successful breastfeeding. Breastfeeding self-efficacy is a social cognitive theory that was developed by Dennis. Breastfeeding self-efficacy reflects how a mother perceives her ability to breastfeed rather than her true ability to succeed in breastfeeding. Mothers with high self-efficacy often can overcome the exhausting barriers of mothers with low self-efficacy [17]. Breastfeeding self-efficacy can predict breastfeeding outcomes at one and two months postpartum in mothers with term infants, and this is a modifiable factor that can affect breastfeeding success [18].
Considering the criticisms of the TPB and the results of studies on factors affecting EBF behavior, especially the prominent role of social support and breastfeeding self-efficacy, interventions based on a model that incorporates these constructs seem necessary. Few studies have been conducted to examine the intention and behavior of breastfeeding by combining the constructs of the TPB with breastfeeding self-efficacy and social breastfeeding support. Yazdanpanah et al. showed that the use of the extended TPB, along with social support structures and breastfeeding self-efficacy, can predict the intention and behavior of EBF [19].
In this study, the answers to three hypotheses were evaluated: 1) Can an educational intervention based on the TPB improve the intention and behavior of EBF? 2) Can an intervention that combines social support for breastfeeding and breastfeeding self-efficacy with interventions based on the constructs of the TPB improve the intention and behavior of EBF? 3) Is the effect of the intervention based on the extended TPB on the intention and behavior of EBF greater than the effect of the intervention based on the constructs of the TPB?
Methods
Design
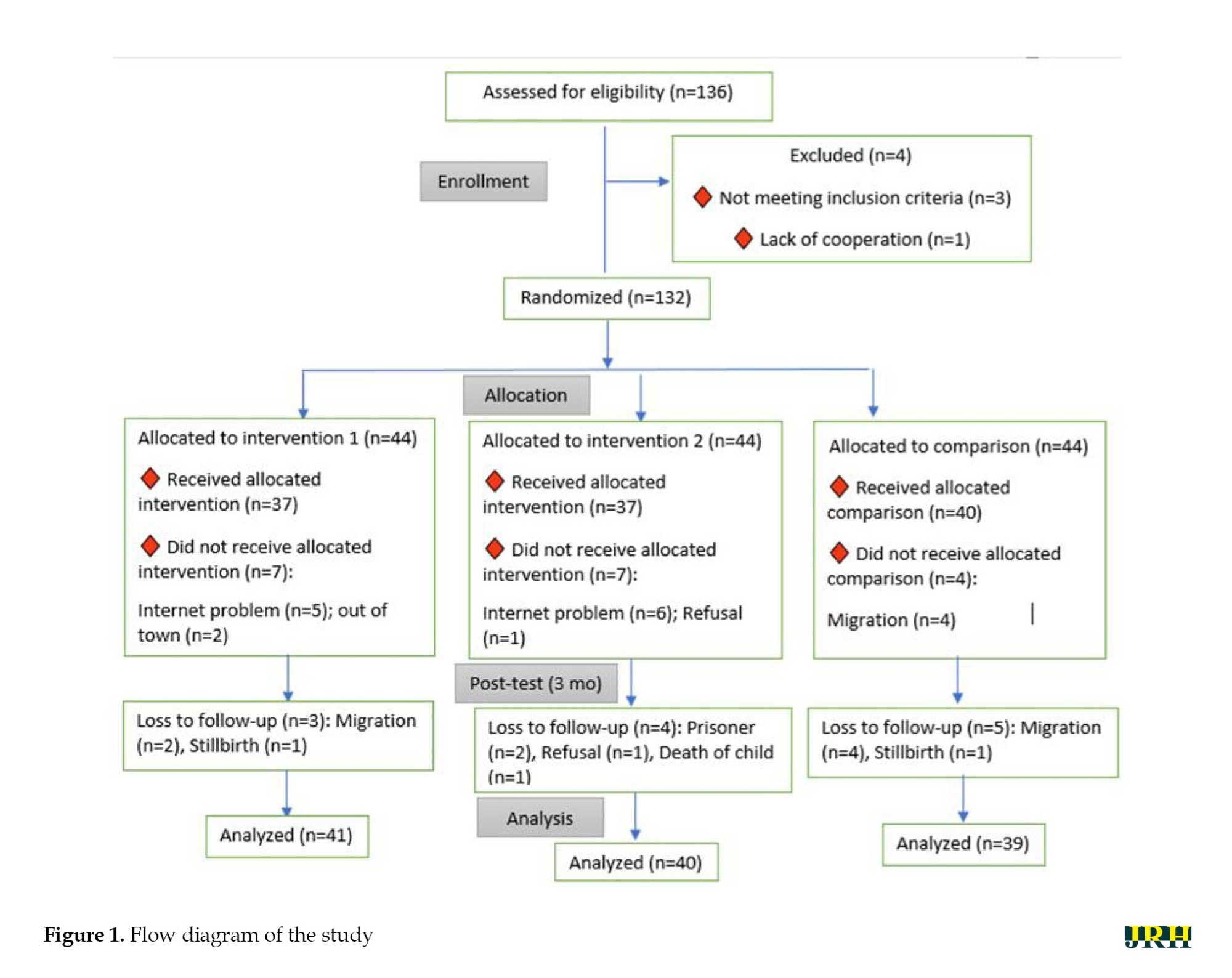
This study was a randomized controlled educational trial, in which 132 primiparous pregnant women who were referred to comprehensive public health service centers in Kerman between December 2019 and January 2020 were included.
One hundred thirty-six people were evaluated according to the study’s inclusion criteria, and four people were excluded from the study. Finally, the results of the second stage were analyzed in the intervention group based on the extended theory, which included 41 participants; the intervention based on the TPB, which included 40 participants and the control group, which included 39 participants (Figure 1).
Participants
The sample size calculation formula (Equation 1) applied in interventional studies (comparing the averages of two groups before and after the intervention) was used to determine the sample size.
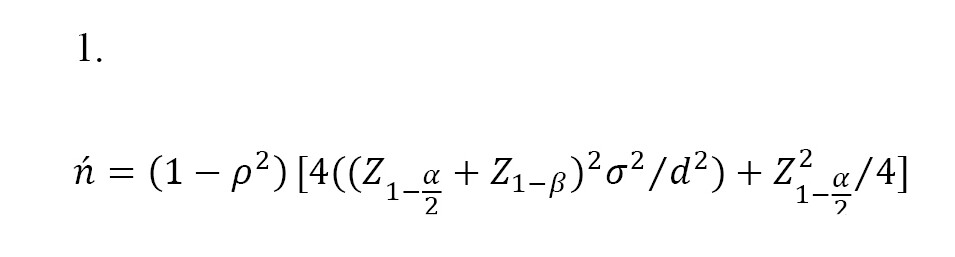
Due to the presence of three groups in the study, the correction formula n=√kn ́was used, where k is equal to the number of groups minus one and ρ is the correlation coefficient between the measurements before and after the intervention, which was considered equal to 0.76 based on similar studies. Also, considering a confidence level of 95% and the statistical power of 90%, and according to similar studies [20], the minimum difference in the average attitude score o between the two groups is 1.68, with a variance of 2.2, Consequently, the required sample size for each of the three groups was calculated to be 44 participants.
Randomization
The sampling method was multi-stage random sampling. After coordinating with officials from Kerman health centers, the first two areas in the city, categorized by economic, social, and cultural status, were excluded. Then, out of the remaining eight comprehensive health service centers, three centers were selected by lottery using a multi-stage random sampling method. In the second stage, a health center was selected from each center by lottery. Then, one center was randomly assigned to the first intervention group, one center to the second intervention group and one center to the control group through a drawing. In each center, samples were randomly entered into the study based on the electronic records of pregnant women and according to the inclusion and exclusion criteria.
Inclusion criteria
Primiparous women with singleton pregnancies were enrolled in the study.
Exclusion criteria
Pregnant women who did not fully participate in the sessions, as well as women who experienced an abortion or did not cooperate in completing the questionnaire after the intervention, were excluded from the study.
Educational intervention
In order to investigate the effectiveness of TPB by combining the two constructs of self-efficacy and breastfeeding social support, two intervention groups were considered.
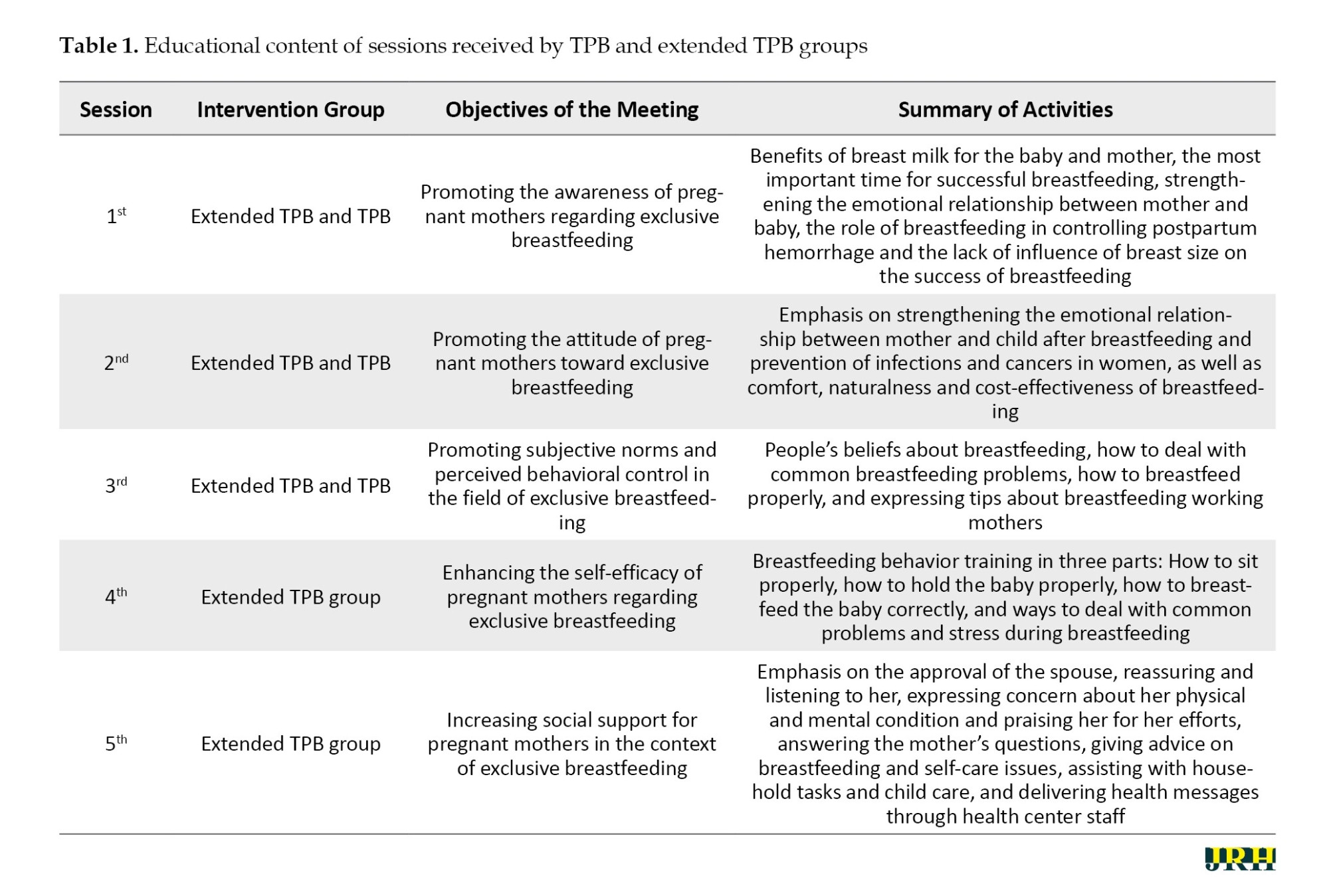
In both intervention groups, educational sessions were conducted to improve the TPB constructs. Interventions were planned in order to create a positive attitude, improve PBC, and modify subjective norms for EBF. The educational program consisted of three online sessions, each one hour long and scheduled one week apart. In the extended intervention group, one 45 minute training session was also provided to improve social support, and one 45-minute training session was also provided to improve breastfeeding self-efficacy based on the strategies recommended by Bandura [21]. The training intervention was presented in the 32nd week of pregnancy. The questionnaire was completed before the intervention and again in the second month after delivery. The control group received routine training at health centers. The educational intervention lasted for five weeks, employing various methods such as presentations, discussions, exchanges of ideas, and sharing of successful experiences (Table 1).
Data collection tool
The tool used in the research was a standard questionnaire consisting of five sections that included demographic characteristics, including age, level of education, occupation, and income. The knowledge assessment questionnaire, adopted from Faridvand et al.’s study [22], consisted of 14 questions, where a score of 2 was assigned for a correct answer, a score of 0 was assigned for a wrong answer, and a score of 1 was assigned for those who did not know the answer. The validity of this tool has been confirmed through content validation and its reliability through test re-test [22]. Reliability was determined by calculating the internal correlation coefficient (ICC). Twenty people who were randomly selected from the studied samples were asked to complete the questionnaire again one week later and the correlation coefficient between the scores obtained from the two tests was calculated. The reliability of the instrument was confirmed with an ICC=0.71, which was significant at the P<0.05 level (95% confidence interval [CI]).
The part related to the constructs of the TPB included attitude, measured through 11 questions; subjective norms, measured through seven questions; PBC, measured through four questions and behavioral intention, measured through three questions. These constructs were adopted from the Alami et al.’ study [23]. The questions were measured using a five-point Likert scale, where a score of five was assigned for complete agreement, and a score of one was assigned for complete disagreement. The materials related to the model constructs demonstrated acceptable content validity (ranging from 0.66 to 0.99) (with <0.5 considered poor, between 0.5 and 0.75 considered average, between 0.75 and 0.9 considered good and >0.9 considered excellent). Additionally, Cronbach’s α and intra-class correlation coefficients were 0.79 and 0.81, respectively (with <0.5 considered unacceptable, between 0.5 and 0.6 considered poor, between 0.6 and 0.7 considered questionable, between 0.7 and 0.8 considered acceptable, between 0.8 and 0.9 considered good and >0.9 considered excellent).
The Dennis lactation behavior self-efficacy questionnaire (adopted from the Araban et al.’s study) [24] consisted of 13 questions. The answers were provided on a five-point likert scale. In examining the differential validity, the questionnaire demonstrated a significant correlation with the scales of general self-efficacy and perceived stress. The Cronbach’s α for the questionnaire was evaluated at 0.91 [24]. In the present study, the Cronbach’s α coefficient was recalculated to be 0.85. This questionnaire includes 13 questions, each scored from zero to four, with a maximum score of 52. No specific cut-off point has been established for the tool.
The social support questionnaire adopted from Boateng et al.’s study [25] consisted of 16 questions. The answers to the questions were categorized into three options: 1) Receive no help at all or much less than you would like, 2) Less than what you would like and 3) As much as you would like. The validity of this questionnaire was examined qualitatively, as well as through expert opinions and the determination of the content validity ratio (CVR) and content validity index (CVI). In the reliability analysis, Cronbach’s α coefficient for the scale was calculated to be 0.84 (with <0.5 considered unacceptable, between 0.5 and 0.6 considered poor, between 0.6 and 0.7 considered questionable, between 0.7 and 0.8 considered acceptable, between 0.8 and 0.9 considered good and >0.9 considered excellent).
Questionnaires related to the constructs of the TPB, social support and breastfeeding self-efficacy were completed by all three groups in the last month of pregnancy and again three months after the intervention, when the child was two months old. Two months after delivery, EBF behavior was also investigated and compared among all three groups.
The tool for examining the performance of EBF also included five questions scored from zero to three, which were adapted from the breastfeeding checklist of the ministry of health [24]. The questionnaire was completed before the intervention and again in the second month after delivery
Statistical analysis
Finally, the data were entered into SPSS software, version 22 (IBM, Armonk, NY, USA). The significance level for the tests was set at P<0.05. Means and frequencies were calculated for all demographic variables. Analysis of covariance, one-way analysis of variance, paired t-test, chi-square tests and Bonferroni tests were used to analyze the data.
Results
Demographic characteristics of the participants
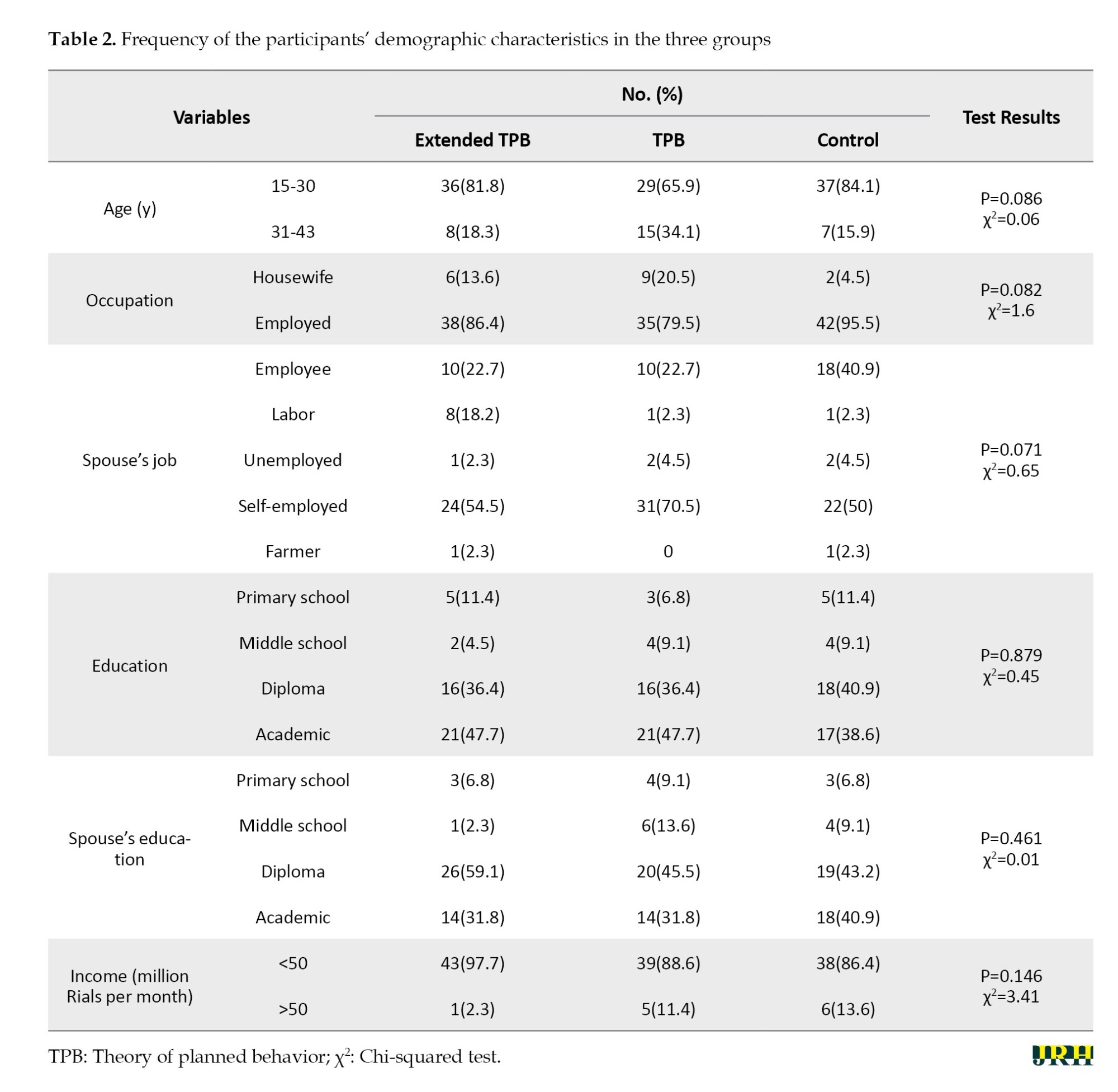
Regarding age, 77.2% of the samples were in the age group of 15-30 years. The majority (87.12%) of the samples were housewives and had a university education (44.6%). Most spouses were self-employed (58.3%) and had diplomas (49.2%). Also, 90.9% of households had a monthly income of fewer than one million Tomans. The results based on the chi-square test conducted before the educational intervention on 132 participants, showed that no significant difference in any of the demographic characteristics among the three groups (P<0.05) (Table 2).
A paired t-test was used to compare the changes in the scores of the TPB constructs, as well as the scores of social support and breastfeeding self-efficacy and the intention to exclusively breastfeed before and after the intervention in the three groups (Table 3). The scores of TPB constructs in both groups increased compared to before the study, while no such difference was observed in the control group. Based on the paired t-test, the mean score of breastfeeding self-efficacy construct significantly increased before the intervention and three months after the intervention in the extended TPB group. However, regarding the social support construct, no significant increase was observed in the extended theory group, even with the intervention.

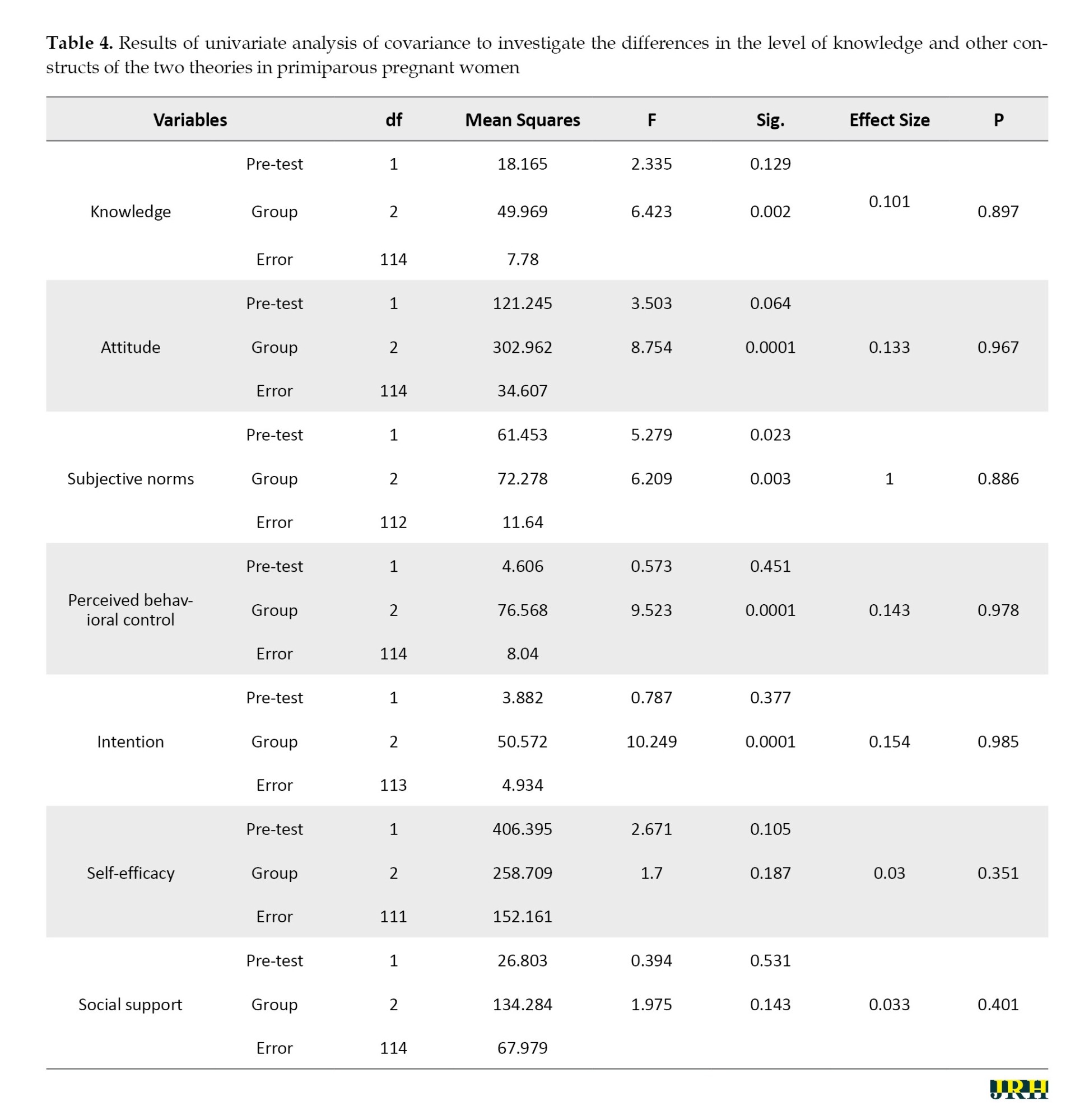
The analysis of covariance was used to compare the three groups in terms of the constructs of the TPB, as well as the constructs of self-efficacy and social support related to breastfeeding. In order to eliminate possible confounding factors, the group was considered as a covariance (Table 4). The F statistic for the TPB constructs in the post-test, with P<0.05, indicates that there is a significant difference between the groups in their scores. However, the F statistic for self-efficacy and social support in the post-test, with P>0.05, was not significant and showed no significant difference between the groups in the changes in these constructs.
According to the analysis of variance, the scores of the intention and the behavior of EBF showed a significant difference among the three groups (P=0.0001). However, the post hoc Bonferroni test showed that the scores of intention and behavior in both intervention groups were significantly higher than in the control group; however, was not significant (P>0.05).
Discussion
The present study was a randomized controlled educational trial to investigate the effect of combining social support and self-efficacy constructs with TPB on promoting the intention and behavior of EBF in primiparous pregnant women in Kerman. Considering that the mothers participating in this study were primiparous, the majority were under 30 years old (77.2%), which is similar to the findings of Arshad et al. and Jamehei et al. [20, 26]. Although most mothers had a university education, they were not employed. The majority of the studied population reported their income level as below average, while in some similar studies, the majority reported an average income [27].
The majority of women had a high level of awareness, which is consistent with the results of Mansour Ghanaei et al. [28]. However, there are contradictory results in this regard. For example, Haghighi and Varzandeh in Shiraz [29] showed that 69.2% of mothers, despite most having a bachelor’s degree, had low knowledge in this area. Ihudiebube-Splendor et al. [30] found that most women learn about breastfeeding from midwifery visits during pregnancy. Therefore, one reason for the difference between the results of Haghighi and Varzandeh and the present study could be the difference in the level of education during pregnancy in the two populations. In analyzing the questions in the knowledge section of the questionnaire, the greatest weakness was the knowledge about the benefits of breastfeeding for the mother. In Mansour Ghanaei et al.’s study [28], the most incorrect answer was related to the relationship between proper maternal nutrition and the quality of breast milk.
The results showed that the mean attitude score three months after the intervention was significantly increased in the intervention groups, which is consistent with the findings of Arshad et al. [20]. Also, the results of the present study are consistent with those of Zhang et al. who showed that the attitude toward EBF improved after the intervention [31]. Attitude toward behavior refers to the desirability of that behavior from an individual’s perspective [10]. The stronger the attitude toward performing a positive behavior, the more likely it is that the intention to perform that behavior will be formed [32]. Walingo and Mutuli [33] and Jalambadani et al. [34] also showed that attitude significantly affects the intention of breastfeeding behavior. This contrasts with the results of Bajoulvand et al. [35], who showed that PBC can explain 60% of the intention to exclusively breastfeed.
Regarding the construct of subjective norms, it can be said that, as in the study by Arshad et al. [20] and the study by Rahmanian et al. [36], the educational intervention increased subjective norms in the intervention groups of pregnant women. In contrast, in the study by Jalambadani et al. [34], the construct of subjective norms did not change after the educational intervention; one reason could be cultural and social differences in different regions. Some studies have shown that the recommendations given by friends, healthcare teams, grandmothers, and even the spouses of pregnant women play a significant role as subjective norms influencing the behavior of EBF [37]. Considering the influence of these people and the compliance of pregnant mothers, especially primiparous women who lack experience in EBF, these individuals should be considered as secondary target groups in the intervention programs.
In the present study, the perceived behavioral control score improved in both intervention groups. The interventions were designed to enhance self-efficacy, fostering a sense of empowerment to overcome barriers to breastfeeding and the belief that EBF is manageable and not difficult. For this purpose, group discussions and the expression of successful experiences and examples from similar people were used to promote this construct. In this regard, our results are consistent with those of Arshad et al. [20] and Jalambadani et al. [34]. Therefore, due to issues, such as maternal and infant diseases, as well as misconception that EBF is impossible and challenging, interventions in this area appear to be necessary.
Breastfeeding self-efficacy score improved in the extended group. This finding is supported by previous studies worldwide [38]. According to this finding, it can be concluded that the educational intervention program based on the extended model for the behavior of EBF increased the level of breastfeeding self-efficacy in the extended intervention group. In a review study [9] on factors affecting EBF, Lau et al. found self-efficacy as an important predictor for the duration of breastfeeding. However, Temple Newhook et al. [39] and Senghore et al. [40] considered attitude the most important predictor for intention. This difference can be related to the differences in the social structural elements that shape mothers’ lives. Budiati et al. showed that one of the factors influencing the attitude toward breastfeeding is the culture and level of social support provided by the mother [41].
Regarding social support, it can be said that the educational intervention based on the extended model for the EBF behavior did not increase the levels of social support in the intervention groups. It appears that education provided only before childbirth was insufficient. It would be more effective to conduct interventions in two stages: During pregnancy and postpartum. Although training on social support for EBF during pregnancy can prepare the people around the pregnant mother to offer support during the postpartum period, it seems that the continuation of this training and support after delivery, especially in the face of real and unforeseen challenges, can strengthen this support. Additionally, it is possible that the circumstances of virtual education and the restrictions imposed by COVID-19 played a role in this lack of effect. In contrast to the findings of the present study, Wilson et al. demonstrated that breastfeeding social support improved through the formation of a social support group [42]. It seems that the strength and scope of these support networks are influential factors in the difference in results.
Regarding the construct of intention, it can be said that educational intervention increased the levels of intentional behavior in both intervention groups. Although the difference in the mean score of behavior intention in the extended intervention group was greater than in the TPB group, this difference was not significant between the two intervention groups. In this study, the highest mean score of behavior was seen in the extended intervention group. However, according to the Bonferroni test, this difference was not significant between the extended TPB and TPB groups.
It can be concluded that the constructs of both theories independently contribute to increasing the intention and behavior of breastfeeding. In the context of comparing the effect of the intervention on the TPB and extended theory, along with the constructs of breastfeeding self-efficacy and breastfeeding social support on EBF, no completely similar studies were found in the literature. Some studies show that the constructs added to the model have been effective in promoting EBF behavior. Ismail et al. in a prospective cohort study, showed that postpartum social support for breast-feeding problems could increase the explained variance of behavior by 6% [43]. Lau et al. found breastfeeding self-efficacy to be an important predictor for breastfeeding duration [9].
In justifying the lack of a significant difference between in behavior between the two intervention groups, it can be pointed out that in this study, the levels of breastfeeding social support and self-efficacy did not change significantly compared to the TPB group, which could be due to the limitations in the implementation of the study. Among the limitations of this study was the delivery of courses in a virtual format and during the COVID-19 pandemic, which may have affected the quality of the interventions. Therefore, further research is suggested to address the limitations of the current study to develop a comprehensive model to encourage EBF behavior and improve the health of mothers and babies.
Conclusion
The present study showed improvement in EBF behavior in both interventional groups compared to the control group. Although the behavior score was higher in the extended group, this difference was insignificant. It can be concluded that the extended theory, combined with the constructs of breastfeeding self-efficacy and social support, can effectively promote EBF behavior. Therefore, it is suggested to implement interventions based on the developed theory, with an emphasis on social support and breastfeeding self-efficacy for primiparous pregnant mothers.
Limitations
In the present study, the implementation of training was conducted solely online, which has several disadvantages, including a lack of visual communication (such as eye contact and non-verbal cues), hindering the establishment of effective communication with learners. Also, the sample size was relatively small, and it would be beneficial to include a larger sample in future studies. Participants were selected only from pregnant women who visited health centers in Kerman City, excluding those who sought care at private clinics, which may limit the generalizability of the results to the entire population of pregnant women.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Rafsanjan University of Medical Sciences (Code: IR.RUMS.REC.1399.102) and ethically in accordance with the World Medical Association Declaration of Helsinki. Mothers provided their written informed consent to participate.
Funding
This study was financially supported by the Vice Deputy Chancellor for Research and Technology at Rafsanjan University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Mahdi Abdolkarimi and Farahnaz Yazdanpanah; Methodology: Hassan Ahmadinia; Data collection: Farahnaz Yazdanpanah; Funding acquisition and writing the original draft: Farahnaz Yazdanpanah, Mostafa Nasirzadeh, Mahdi Abdolkarimi and Hassan Ahmadinia; Review and editing: Mostafa Nasirzadeh; Mahdi Abdolkarimi and Farahnaz Yazdanpanah; Resources: Farahnaz Yazdanpanah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all who assisted in implementing this research, especially the pregnant women participating in the study and the staff of the comprehensive health service centers involved in the project.
References
The World Health Organization (WHO) defines exclusive breastfeeding (EBF) as breastfeeding an infant exclusively, without the introduction of other foods or even water, except for medication, oral rehydration solutions, vitamins and supplements [1]. In addition to providing the most appropriate physical growth for the baby and meeting the emotional needs of the infant and mother, breast milk plays a vital role in preventing gastrointestinal and respiratory infections [2]. It also provides maternal health and well-being by affecting gestational age and reducing the risk of breast and ovarian cancer [3]. However, even in developed countries, the rate of EBF has been reported to be low [4]. At the 65th meeting of the WHO, it was decided to increase the rate of EBF to 50% by 2025. This figure differs significantly in developing countries, ranging from 13% to 77% in Iran [5]. A study in Riyadh showed that despite the start of breastfeeding, only 20.9% continue to be exclusively breastfed [6]. The results of the latest studies conducted in a review study on EBF showed that despite the emphasis of Iran Ministry of Health and Medical Education and the concern of health policymakers to increase this index, only about half of women adhere to EBF [7]. Therefore, it is necessary to determine effective interventions to promote this behavior for the health of mothers and babies.
Early cessation of breastfeeding causes physical, psychological, and socio-economic damage to the child and society [8]. Subjective norms among lactating and postpartum women, including the views of significant individuals, such as peers and social networks and important family members, such as spouses, parents, or siblings, are important factors in breastfeeding [9].
One of the theories that influence behavior change in response to social norms is the theory of planned behavior (TPB), which was developed in 1991 by Ajzen and Fishbein [10]. The TPB includes the following constructs: Behavioral intention, attitude toward behavior, subjective norms and perceived behavioral control (PBC) [10]. The TPB is a behavioral theory in social psychology that analyzes the factors affecting behavioral goals and explains the behavior. It points out that the main predictor of behavior is a change in behavior intention that depends on individuals’ attitudes, subjective norms, and PBC [11]. This theory, which has been applied to many health behaviors, explains, on average, about 40% of the relationship between intention and health behaviors [12]. One of the criticisms of the TPB is the lack of attention to social factors affecting behavior. Numerous studies have emphasized the role of social support, especially the spouse’s involvement, in initiating and continuing EBF [13, 14]. Breastfeeding is a behavior that requires the knowledge, skills, support, and confidence of the mother [15]. Social factors, including the support of social groups, significantly affect breastfeeding mothers [16].
On the other hand, some researchers believe that self-efficacy predicts the behavior’s occurrence better than the PBC for some behaviors, such as successful breastfeeding. Breastfeeding self-efficacy is a social cognitive theory that was developed by Dennis. Breastfeeding self-efficacy reflects how a mother perceives her ability to breastfeed rather than her true ability to succeed in breastfeeding. Mothers with high self-efficacy often can overcome the exhausting barriers of mothers with low self-efficacy [17]. Breastfeeding self-efficacy can predict breastfeeding outcomes at one and two months postpartum in mothers with term infants, and this is a modifiable factor that can affect breastfeeding success [18].
Considering the criticisms of the TPB and the results of studies on factors affecting EBF behavior, especially the prominent role of social support and breastfeeding self-efficacy, interventions based on a model that incorporates these constructs seem necessary. Few studies have been conducted to examine the intention and behavior of breastfeeding by combining the constructs of the TPB with breastfeeding self-efficacy and social breastfeeding support. Yazdanpanah et al. showed that the use of the extended TPB, along with social support structures and breastfeeding self-efficacy, can predict the intention and behavior of EBF [19].
In this study, the answers to three hypotheses were evaluated: 1) Can an educational intervention based on the TPB improve the intention and behavior of EBF? 2) Can an intervention that combines social support for breastfeeding and breastfeeding self-efficacy with interventions based on the constructs of the TPB improve the intention and behavior of EBF? 3) Is the effect of the intervention based on the extended TPB on the intention and behavior of EBF greater than the effect of the intervention based on the constructs of the TPB?
Methods
Design
This study was a randomized controlled educational trial, in which 132 primiparous pregnant women who were referred to comprehensive public health service centers in Kerman between December 2019 and January 2020 were included.
One hundred thirty-six people were evaluated according to the study’s inclusion criteria, and four people were excluded from the study. Finally, the results of the second stage were analyzed in the intervention group based on the extended theory, which included 41 participants; the intervention based on the TPB, which included 40 participants and the control group, which included 39 participants (Figure 1).
Participants
The sample size calculation formula (Equation 1) applied in interventional studies (comparing the averages of two groups before and after the intervention) was used to determine the sample size.
Due to the presence of three groups in the study, the correction formula n=√kn ́was used, where k is equal to the number of groups minus one and ρ is the correlation coefficient between the measurements before and after the intervention, which was considered equal to 0.76 based on similar studies. Also, considering a confidence level of 95% and the statistical power of 90%, and according to similar studies [20], the minimum difference in the average attitude score o between the two groups is 1.68, with a variance of 2.2, Consequently, the required sample size for each of the three groups was calculated to be 44 participants.
Randomization
The sampling method was multi-stage random sampling. After coordinating with officials from Kerman health centers, the first two areas in the city, categorized by economic, social, and cultural status, were excluded. Then, out of the remaining eight comprehensive health service centers, three centers were selected by lottery using a multi-stage random sampling method. In the second stage, a health center was selected from each center by lottery. Then, one center was randomly assigned to the first intervention group, one center to the second intervention group and one center to the control group through a drawing. In each center, samples were randomly entered into the study based on the electronic records of pregnant women and according to the inclusion and exclusion criteria.
Inclusion criteria
Primiparous women with singleton pregnancies were enrolled in the study.
Exclusion criteria
Pregnant women who did not fully participate in the sessions, as well as women who experienced an abortion or did not cooperate in completing the questionnaire after the intervention, were excluded from the study.
Educational intervention
In order to investigate the effectiveness of TPB by combining the two constructs of self-efficacy and breastfeeding social support, two intervention groups were considered.
In both intervention groups, educational sessions were conducted to improve the TPB constructs. Interventions were planned in order to create a positive attitude, improve PBC, and modify subjective norms for EBF. The educational program consisted of three online sessions, each one hour long and scheduled one week apart. In the extended intervention group, one 45 minute training session was also provided to improve social support, and one 45-minute training session was also provided to improve breastfeeding self-efficacy based on the strategies recommended by Bandura [21]. The training intervention was presented in the 32nd week of pregnancy. The questionnaire was completed before the intervention and again in the second month after delivery. The control group received routine training at health centers. The educational intervention lasted for five weeks, employing various methods such as presentations, discussions, exchanges of ideas, and sharing of successful experiences (Table 1).
Data collection tool
The tool used in the research was a standard questionnaire consisting of five sections that included demographic characteristics, including age, level of education, occupation, and income. The knowledge assessment questionnaire, adopted from Faridvand et al.’s study [22], consisted of 14 questions, where a score of 2 was assigned for a correct answer, a score of 0 was assigned for a wrong answer, and a score of 1 was assigned for those who did not know the answer. The validity of this tool has been confirmed through content validation and its reliability through test re-test [22]. Reliability was determined by calculating the internal correlation coefficient (ICC). Twenty people who were randomly selected from the studied samples were asked to complete the questionnaire again one week later and the correlation coefficient between the scores obtained from the two tests was calculated. The reliability of the instrument was confirmed with an ICC=0.71, which was significant at the P<0.05 level (95% confidence interval [CI]).
The part related to the constructs of the TPB included attitude, measured through 11 questions; subjective norms, measured through seven questions; PBC, measured through four questions and behavioral intention, measured through three questions. These constructs were adopted from the Alami et al.’ study [23]. The questions were measured using a five-point Likert scale, where a score of five was assigned for complete agreement, and a score of one was assigned for complete disagreement. The materials related to the model constructs demonstrated acceptable content validity (ranging from 0.66 to 0.99) (with <0.5 considered poor, between 0.5 and 0.75 considered average, between 0.75 and 0.9 considered good and >0.9 considered excellent). Additionally, Cronbach’s α and intra-class correlation coefficients were 0.79 and 0.81, respectively (with <0.5 considered unacceptable, between 0.5 and 0.6 considered poor, between 0.6 and 0.7 considered questionable, between 0.7 and 0.8 considered acceptable, between 0.8 and 0.9 considered good and >0.9 considered excellent).
The Dennis lactation behavior self-efficacy questionnaire (adopted from the Araban et al.’s study) [24] consisted of 13 questions. The answers were provided on a five-point likert scale. In examining the differential validity, the questionnaire demonstrated a significant correlation with the scales of general self-efficacy and perceived stress. The Cronbach’s α for the questionnaire was evaluated at 0.91 [24]. In the present study, the Cronbach’s α coefficient was recalculated to be 0.85. This questionnaire includes 13 questions, each scored from zero to four, with a maximum score of 52. No specific cut-off point has been established for the tool.
The social support questionnaire adopted from Boateng et al.’s study [25] consisted of 16 questions. The answers to the questions were categorized into three options: 1) Receive no help at all or much less than you would like, 2) Less than what you would like and 3) As much as you would like. The validity of this questionnaire was examined qualitatively, as well as through expert opinions and the determination of the content validity ratio (CVR) and content validity index (CVI). In the reliability analysis, Cronbach’s α coefficient for the scale was calculated to be 0.84 (with <0.5 considered unacceptable, between 0.5 and 0.6 considered poor, between 0.6 and 0.7 considered questionable, between 0.7 and 0.8 considered acceptable, between 0.8 and 0.9 considered good and >0.9 considered excellent).
Questionnaires related to the constructs of the TPB, social support and breastfeeding self-efficacy were completed by all three groups in the last month of pregnancy and again three months after the intervention, when the child was two months old. Two months after delivery, EBF behavior was also investigated and compared among all three groups.
The tool for examining the performance of EBF also included five questions scored from zero to three, which were adapted from the breastfeeding checklist of the ministry of health [24]. The questionnaire was completed before the intervention and again in the second month after delivery
Statistical analysis
Finally, the data were entered into SPSS software, version 22 (IBM, Armonk, NY, USA). The significance level for the tests was set at P<0.05. Means and frequencies were calculated for all demographic variables. Analysis of covariance, one-way analysis of variance, paired t-test, chi-square tests and Bonferroni tests were used to analyze the data.
Results
Demographic characteristics of the participants
Regarding age, 77.2% of the samples were in the age group of 15-30 years. The majority (87.12%) of the samples were housewives and had a university education (44.6%). Most spouses were self-employed (58.3%) and had diplomas (49.2%). Also, 90.9% of households had a monthly income of fewer than one million Tomans. The results based on the chi-square test conducted before the educational intervention on 132 participants, showed that no significant difference in any of the demographic characteristics among the three groups (P<0.05) (Table 2).
A paired t-test was used to compare the changes in the scores of the TPB constructs, as well as the scores of social support and breastfeeding self-efficacy and the intention to exclusively breastfeed before and after the intervention in the three groups (Table 3). The scores of TPB constructs in both groups increased compared to before the study, while no such difference was observed in the control group. Based on the paired t-test, the mean score of breastfeeding self-efficacy construct significantly increased before the intervention and three months after the intervention in the extended TPB group. However, regarding the social support construct, no significant increase was observed in the extended theory group, even with the intervention.
The analysis of covariance was used to compare the three groups in terms of the constructs of the TPB, as well as the constructs of self-efficacy and social support related to breastfeeding. In order to eliminate possible confounding factors, the group was considered as a covariance (Table 4). The F statistic for the TPB constructs in the post-test, with P<0.05, indicates that there is a significant difference between the groups in their scores. However, the F statistic for self-efficacy and social support in the post-test, with P>0.05, was not significant and showed no significant difference between the groups in the changes in these constructs.
According to the analysis of variance, the scores of the intention and the behavior of EBF showed a significant difference among the three groups (P=0.0001). However, the post hoc Bonferroni test showed that the scores of intention and behavior in both intervention groups were significantly higher than in the control group; however, was not significant (P>0.05).
Discussion
The present study was a randomized controlled educational trial to investigate the effect of combining social support and self-efficacy constructs with TPB on promoting the intention and behavior of EBF in primiparous pregnant women in Kerman. Considering that the mothers participating in this study were primiparous, the majority were under 30 years old (77.2%), which is similar to the findings of Arshad et al. and Jamehei et al. [20, 26]. Although most mothers had a university education, they were not employed. The majority of the studied population reported their income level as below average, while in some similar studies, the majority reported an average income [27].
The majority of women had a high level of awareness, which is consistent with the results of Mansour Ghanaei et al. [28]. However, there are contradictory results in this regard. For example, Haghighi and Varzandeh in Shiraz [29] showed that 69.2% of mothers, despite most having a bachelor’s degree, had low knowledge in this area. Ihudiebube-Splendor et al. [30] found that most women learn about breastfeeding from midwifery visits during pregnancy. Therefore, one reason for the difference between the results of Haghighi and Varzandeh and the present study could be the difference in the level of education during pregnancy in the two populations. In analyzing the questions in the knowledge section of the questionnaire, the greatest weakness was the knowledge about the benefits of breastfeeding for the mother. In Mansour Ghanaei et al.’s study [28], the most incorrect answer was related to the relationship between proper maternal nutrition and the quality of breast milk.
The results showed that the mean attitude score three months after the intervention was significantly increased in the intervention groups, which is consistent with the findings of Arshad et al. [20]. Also, the results of the present study are consistent with those of Zhang et al. who showed that the attitude toward EBF improved after the intervention [31]. Attitude toward behavior refers to the desirability of that behavior from an individual’s perspective [10]. The stronger the attitude toward performing a positive behavior, the more likely it is that the intention to perform that behavior will be formed [32]. Walingo and Mutuli [33] and Jalambadani et al. [34] also showed that attitude significantly affects the intention of breastfeeding behavior. This contrasts with the results of Bajoulvand et al. [35], who showed that PBC can explain 60% of the intention to exclusively breastfeed.
Regarding the construct of subjective norms, it can be said that, as in the study by Arshad et al. [20] and the study by Rahmanian et al. [36], the educational intervention increased subjective norms in the intervention groups of pregnant women. In contrast, in the study by Jalambadani et al. [34], the construct of subjective norms did not change after the educational intervention; one reason could be cultural and social differences in different regions. Some studies have shown that the recommendations given by friends, healthcare teams, grandmothers, and even the spouses of pregnant women play a significant role as subjective norms influencing the behavior of EBF [37]. Considering the influence of these people and the compliance of pregnant mothers, especially primiparous women who lack experience in EBF, these individuals should be considered as secondary target groups in the intervention programs.
In the present study, the perceived behavioral control score improved in both intervention groups. The interventions were designed to enhance self-efficacy, fostering a sense of empowerment to overcome barriers to breastfeeding and the belief that EBF is manageable and not difficult. For this purpose, group discussions and the expression of successful experiences and examples from similar people were used to promote this construct. In this regard, our results are consistent with those of Arshad et al. [20] and Jalambadani et al. [34]. Therefore, due to issues, such as maternal and infant diseases, as well as misconception that EBF is impossible and challenging, interventions in this area appear to be necessary.
Breastfeeding self-efficacy score improved in the extended group. This finding is supported by previous studies worldwide [38]. According to this finding, it can be concluded that the educational intervention program based on the extended model for the behavior of EBF increased the level of breastfeeding self-efficacy in the extended intervention group. In a review study [9] on factors affecting EBF, Lau et al. found self-efficacy as an important predictor for the duration of breastfeeding. However, Temple Newhook et al. [39] and Senghore et al. [40] considered attitude the most important predictor for intention. This difference can be related to the differences in the social structural elements that shape mothers’ lives. Budiati et al. showed that one of the factors influencing the attitude toward breastfeeding is the culture and level of social support provided by the mother [41].
Regarding social support, it can be said that the educational intervention based on the extended model for the EBF behavior did not increase the levels of social support in the intervention groups. It appears that education provided only before childbirth was insufficient. It would be more effective to conduct interventions in two stages: During pregnancy and postpartum. Although training on social support for EBF during pregnancy can prepare the people around the pregnant mother to offer support during the postpartum period, it seems that the continuation of this training and support after delivery, especially in the face of real and unforeseen challenges, can strengthen this support. Additionally, it is possible that the circumstances of virtual education and the restrictions imposed by COVID-19 played a role in this lack of effect. In contrast to the findings of the present study, Wilson et al. demonstrated that breastfeeding social support improved through the formation of a social support group [42]. It seems that the strength and scope of these support networks are influential factors in the difference in results.
Regarding the construct of intention, it can be said that educational intervention increased the levels of intentional behavior in both intervention groups. Although the difference in the mean score of behavior intention in the extended intervention group was greater than in the TPB group, this difference was not significant between the two intervention groups. In this study, the highest mean score of behavior was seen in the extended intervention group. However, according to the Bonferroni test, this difference was not significant between the extended TPB and TPB groups.
It can be concluded that the constructs of both theories independently contribute to increasing the intention and behavior of breastfeeding. In the context of comparing the effect of the intervention on the TPB and extended theory, along with the constructs of breastfeeding self-efficacy and breastfeeding social support on EBF, no completely similar studies were found in the literature. Some studies show that the constructs added to the model have been effective in promoting EBF behavior. Ismail et al. in a prospective cohort study, showed that postpartum social support for breast-feeding problems could increase the explained variance of behavior by 6% [43]. Lau et al. found breastfeeding self-efficacy to be an important predictor for breastfeeding duration [9].
In justifying the lack of a significant difference between in behavior between the two intervention groups, it can be pointed out that in this study, the levels of breastfeeding social support and self-efficacy did not change significantly compared to the TPB group, which could be due to the limitations in the implementation of the study. Among the limitations of this study was the delivery of courses in a virtual format and during the COVID-19 pandemic, which may have affected the quality of the interventions. Therefore, further research is suggested to address the limitations of the current study to develop a comprehensive model to encourage EBF behavior and improve the health of mothers and babies.
Conclusion
The present study showed improvement in EBF behavior in both interventional groups compared to the control group. Although the behavior score was higher in the extended group, this difference was insignificant. It can be concluded that the extended theory, combined with the constructs of breastfeeding self-efficacy and social support, can effectively promote EBF behavior. Therefore, it is suggested to implement interventions based on the developed theory, with an emphasis on social support and breastfeeding self-efficacy for primiparous pregnant mothers.
Limitations
In the present study, the implementation of training was conducted solely online, which has several disadvantages, including a lack of visual communication (such as eye contact and non-verbal cues), hindering the establishment of effective communication with learners. Also, the sample size was relatively small, and it would be beneficial to include a larger sample in future studies. Participants were selected only from pregnant women who visited health centers in Kerman City, excluding those who sought care at private clinics, which may limit the generalizability of the results to the entire population of pregnant women.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Rafsanjan University of Medical Sciences (Code: IR.RUMS.REC.1399.102) and ethically in accordance with the World Medical Association Declaration of Helsinki. Mothers provided their written informed consent to participate.
Funding
This study was financially supported by the Vice Deputy Chancellor for Research and Technology at Rafsanjan University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Mahdi Abdolkarimi and Farahnaz Yazdanpanah; Methodology: Hassan Ahmadinia; Data collection: Farahnaz Yazdanpanah; Funding acquisition and writing the original draft: Farahnaz Yazdanpanah, Mostafa Nasirzadeh, Mahdi Abdolkarimi and Hassan Ahmadinia; Review and editing: Mostafa Nasirzadeh; Mahdi Abdolkarimi and Farahnaz Yazdanpanah; Resources: Farahnaz Yazdanpanah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all who assisted in implementing this research, especially the pregnant women participating in the study and the staff of the comprehensive health service centers involved in the project.
References
- World Health Organization (WHO). Exclusive breastfeeding for optimal growth, development and health of infants [Internet]. 2019 [Updated 2023 August 9]. Available from: [Link]
- Mokhtarian T, Farhud D, Malmir M, Mokhtarian T. [Moral imperative of breastfeeding & commitment to the children’s rights (Persian)]. Ethics in Science and Technology. 2017; 12(1):1-9. [Link]
- Hashim S, Ishak A, Muhammad J. Unsuccessful exclusive breastfeeding and associated factors among the healthcare providers in East Coast, Malaysia. Korean Journal of family medicine. 2020; 41(6):416-21. [DOI:10.4082/kjfm.19.0060] [PMID]
- Bartle NC, Harvey K. Explaining infant feeding: The role of previous personal and vicarious experience on attitudes, subjective norms, self-efficacy, and breastfeeding outcomes. British Journal of Health Psychology. 2017; 22(4):763-85. [DOI:10.1111/bjhp.12254] [PMID]
- Taheri Z, Bakouei F. [The relationship between mothers’ empowerment in breastfeeding with exclusive breast feeding in infants (Persian)]. Journal of Babol University of Medical Sciences. 2019; 21(1):85-92. [DOI:10.22088/jbums.21.1.85]
- Saied H, Mohamed A, Suliman A, Al Anazi W. Breastfeeding knowledge, attitude and barriers among Saudi women in Riyadh. Journal of Natural Sciences Research. 2013; 3(12):6-13. [Link]
- Behzadifar M, Saki M, Behzadifar M, Mardani M, Yari F, Ebrahimzadeh F, et al. Prevalence of exclusive breastfeeding practice in the first six months of life and its determinants in Iran: A systematic review and meta-analysis. BMC Pediatrics. 2019; 19(1):1-10. [DOI:10.1186/s12887-019-1776-0]
- Pakpour A, Alijanzadeh M, Pouresmaeil M, Taherkhani F, Mohammadgholiha R, Jozi N. [Predictive factors associated with breastfeeding initiation and duration behaviors of 6-months postpartum mothers referred to health centers in the city of Qazvin based on theory of planned behavior (Persian)]. Iranian Journal of Health Education and Health Promotion. 2016; 4(1):20-30. [DOI:10.18869/acadpub.ihepsaj.4.1.20]
- Lau CY, Lok KY, Tarrant M. Breastfeeding duration and the theory of planned behavior and breastfeeding self-efficacy framework: A systematic review of observational studies. Maternal and Child Health Journal. 2018; 22:327-42. [DOI:10.1007/s10995-018-2453-x]
- Mahmudian H, Rezaei M. [Women and low childbearing action: The case study of Kurdish women (Persian)]. Women’s Strategic Studies. 2012; 14(55):173-225. [Link]
- Wang J, Liu W, Zhao Q, Xiao M, Peng D. An application of the theory of planned behavior to predict the intention and practice of nursing staff toward physical restraint use in long-term care facilities: Structural equation modeling. Psychology Research and Behavior Management. 2021; 2021:275-87. [DOI:10.2147/PRBM.S293759]
- Farzaneh Z, Asadollahi Z, Asadpour M, Rahaei Z, Sardari F, Rezaeaian M. [Predictors of oral health condition among pregnant mothers in rafsanjan city based on theory of planned behavior in 2016: A descriptive study (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2020; 19(1):65-80. [DOI:10.29252/jrums.19.1.65]
- Brown A, Raynor P, Lee M. Young mothers who choose to breast feed: the importance of being part of a supportive breast-feeding community. Midwifery. 2011; 27(1):53-9. [DOI:10.1016/j.midw.2009.09.004]
- Zareipour M, Abdolkarimi M, Moradi Z, Mahbubi M. Quality of life and self-efficacy in health care providers of rural health centers in Urmia. Caspian Journal of Health Research. 2020; 5(1):3-7. [DOI:10.29252/cjhr.5.1.3]
- Maleki-Saghooni N, Amel Barez M, Karimi FZ. Investigation of the relationship between social support and breastfeeding self-efficacy in primiparous breastfeeding mothers. The Journal of Maternal-Fetal & Neonatal Medicine. 2020; 33(18):3097-102. [DOI:10.1080/14767058.2019.1568986]
- Sanjari S, Mohammadi Soleimani M, Khanjani N, Mohseni M, Ahmadi Tabatabaei S. [The relationship between demographic factors, healthy family and social health with exclusive breastfeeding in women referred to Kashani hospital of Jiroft in 2014 (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2016; 15(2):165-78. [Link]
- Brockway M, Benzies KM, Carr E, Aziz K. Breastfeeding self-efficacy and breastmilk feeding for moderate and late preterm infants in the Family Integrated Care trial: A mixed methods protocol. International Breastfeeding Journal. 2018; 13(1):1-11. [DOI:10.1186/s13006-018-0168-7]
- Brockway M, Benzies K, Hayden KA. Interventions to improve breastfeeding self-efficacy and resultant breastfeeding rates: A systematic review and meta-analysis. Journal of Human Lactation. 2017; 33(3):486-99. [DOI:10.1177/0890334417707957]
- Yazdanpanah F, Nasirzadeh M, Ahmadinia H, Abdolkarimi M. Application of the extended theory of planned behavior to predict exclusive breastfeeding intention, in pregnant nulliparous women. A cross-sectional study. Investigación y Educación en Enfermería. 2022; 40(2):e04. [DOI:10.17533/udea.iee.v40n2e04] [PMID]
- Arshad SM, Khani-Jeihooni A, Moradi Z, Kouhpayeh SA, Kashfi SM, Dehghan A. Effect of theory of planned behavior-based educational intervention on breastfeeding behavior in pregnant women in Fasa city, Iran. Journal of Education and Community Health. 2017; 4(2):55-63. [DOI:10.21859/jech.4.2.55]
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977; 84(2):191. [DOI:10.1037//0033-295X.84.2.191]
- Faridvand F, Mirghafourvand M, Malakouti J, Mohammad-Alizadeh-Charandabi S. Relationship between social support and breastfeeding self-efficacy among women in Tabriz, Iran. British Journal of Midwifery. 2017; 25(2):103-9. [DOI:10.12968/bjom.2017.25.2.103]
- Alami A, Moshki M, Alimardani A. [Development and validation of theory of planned behavior questionnaire for exclusive breastfeeding (Persian)]. Journal of Neyshabur University of Medical Sciences. 2014; 2(4):45-53. [Link]
- Araban M, Mehrjardi FF, Shahry P, Montazeri A. [The Persian version of breastfeeding self-efficacy scale-short form (BSES-SF): Translation and psychometric assessment (Persian)]. Payesh. 2016; 15(1):87-93. [Link]
- Boateng GO, Martin SL, Collins SM, Natamba BK, Young SL. Measuring exclusive breastfeeding social support: Scale development and validation in Uganda. Maternal & Child Nutrition. 2018; 14(3):e12579. [DOI:10.1111/mcn.12579]
- Jamehei F, Ostovar A, Javadzade H. Predictors of exclusive breastfeeding among nulliparous Iranian mothers: Application of the theory of planned behavior. International Journal of Pediatrics. 2017; 5(3):4457-67. [DOI:10.22038/ijp.2016.20815.1748]
- Jalal M, Dolatian M, Mahmoodi Z, Aliyari R. The relationship between psychological factors and maternal social support to breastfeeding process. Electronic Physician. 2017; 9(1):3561. [DOI:10.19082/3561]
- Mansour Ghanaei M, Kazemnezhad Leili E, Amin A, Asgari ghalehbin S. [Mothers’ knowledge and attitude toward exclusive breastfeeding (Persian)]. Journal of Guilan University of Medical Sciences. 2020; 29(2):1-13. [Link]
- Haghighi M, Varzandeh R. Maternal knowledge and attitude toward exclusive breastfeeding in six months after birth in Shiraz, Iran. International Journal of Pediatrics. 2016; 4(11):3759-67. [DOI:10.22038/ijp.2016.7414]
- Ihudiebube-Splendor CN, Okafor CB, Anarado AN, Jisieike-Onuigbo NN, Chinweuba AU, Nwaneri AC, et al. Exclusive breastfeeding knowledge, intention to practice and predictors among primiparous women in Enugu South-East, Nigeria. Journal of Pregnancy. 2019; 2019:1-8. [DOI:10.1155/2019/9832075]
- Zhang Y, Yuan R, Ma H. Effect of the theory of planned behavior on primipara breastfeeding. Annals of Palliative Medicine. 2021; 10(4):4547-54. [DOI:10.21037/apm-21-255]
- Lagzian M, Hadadian A, Kafashan M, Doreh YA. [An investigation into students’ perception of electronic services in academic libraries: Based on azjens theory of planned behavi (Persian)]. Iranian Journal of Information Processing and Management. 2022; 29(2):333-50. [Link]
- Walingo MK, Mutuli LA. Influence of maternal beliefs, attitude, perceived behavior on breast-feeding among post partum mothers in Western Kenya. Pakistan Journal of Nutrition. 2014; 13(5):250-4. [DOI:10.3923/pjn.2014.250.254]
- Jalambadani Z, Shojaei Zadeh D, Hoseini M, Sadeghi R. [The effect of education for iron consumption based on the theory of planned behavior in pregnant women in Mashhad (Persian)]. Journal of Clinical Nursing and Midwifery. 2015; 4(2):59-68. [Link]
- Bajoulvand R, González-Jiménez E, Imani-Nasab MH, Ebrahimzadeh F. Predicting exclusive breastfeeding among Iranian mothers: application of the theory of planned behavior using structural equation modeling. Iranian Journal of Nursing and Midwifery Research. 2019; 24(5):323. [DOI:10.4103/ijnmr.ijnmr_164_18]
- Rahmanian V, Jahromi VK, Rastgoo F, Najafi F, Sharifi N. The effect of educational intervention based on the theory of planned behavior in pregnant women and individuals affecting their exclusive breastfeeding: A controlled trial. Journal of Education and Community Health. 2022; 9(1):60-8. [DOI:10.34172/jech.2022.10]
- Guo JL, Wang TF, Liao J, Huang C. Efficacy of the theory of planned behavior in predicting breastfeeding: Meta-analysis and structural equation modeling. Applied Nursing Research. 2016; 29:37-42. [DOI:10.1016/j.apnr.2015.03.016]
- Moafi F, Hajnasiri HH, Hosseini T, Alimoradi Z, Bajalan Z. Breastfeeding self-efficacy and its associated factors in women who gave birth in Kosar Hospital of Qazvin in 2016-2017: A descriptive study. Journal of Rafsanjan University of Medical Sciences. 2019;17(11):1003-16. [Link]
- Temple Newhook J, Newhook LA, Midodzi WK, Murphy Goodridge J, Burrage L, Gill N, et al. Poverty and breastfeeding: comparing determinants of early breastfeeding cessation incidence in socioeconomically marginalized and privileged populations in the FiNaL study. Health Equity. 2017; 1(1):96-102. [DOI:10.1089/heq.2016.0028]
- Senghore T, Omotosho TA, Ceesay O, Williams DCH. Predictors of exclusive breastfeeding knowledge and intention to or practice of exclusive breastfeeding among antenatal and postnatal women receiving routine care: A cross-sectional study. International Breastfeeding Journal. 2018; 13(9):1-8. [DOI:10.1186/s13006-018-0154-0]
- Budiati T, Setyowati. The influence culture and maternal care on exclusive breastfeeding practice in post caesarean section mothers. Enfermeria clinica. 2019; 29(Supplement 2):808-14. [DOI:10.1016/j.enfcli.2019.04.121]
- Wilson JC. Using social media for breastfeeding support. Nursing for Women’s Health. 2020; 24(5):332-43. [DOI:10.1016/j.nwh.2020.07.003]
- Ismail TAT, Muda WAMW, Bakar MI. The extended Theory of Planned Behavior in explaining exclusive breastfeeding intention and behavior among women in Kelantan, Malaysia. Nutrition Research and Practice. 2016; 10(1):49-55. [DOI:10.4162/nrp.2016.10.1.49]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2023/10/21 | Accepted: 2024/01/27 | Published: 2024/10/28
Received: 2023/10/21 | Accepted: 2024/01/27 | Published: 2024/10/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
