

Volume 15, Issue 3 (May & June 2025)
J Research Health 2025, 15(3): 227-236 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Charoghchian Khorasani E, Ahmadian M, Forghani T, Esmaily H, Gholian-aval M. Lifestyle Intervention of Iranian Medicine on Behavior of Older Adults in Reforming Nutritional Habits. J Research Health 2025; 15 (3) :227-236
URL: http://jrh.gmu.ac.ir/article-1-2520-en.html
URL: http://jrh.gmu.ac.ir/article-1-2520-en.html
Elham Charoghchian Khorasani1 

 , Mohammad Ahmadian2 , Toktam Forghani3 , Habibollah Esmaily4 , Mahdi Gholian-aval5
, Mohammad Ahmadian2 , Toktam Forghani3 , Habibollah Esmaily4 , Mahdi Gholian-aval5
, Mohammad Ahmadian2 , Toktam Forghani3 , Habibollah Esmaily4 , Mahdi Gholian-aval5
1- Department of Health Education and Promotion, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Persian Medicine, School of Persian and Complementary Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran.
4- Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. & Department of Biostatistics, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
5- Department of Health Education and Promotion, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,GholianAM@mums.ac.ir
2- Department of Persian Medicine, School of Persian and Complementary Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran.
4- Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. & Department of Biostatistics, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
5- Department of Health Education and Promotion, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,
Full-Text [PDF 1158 kb]
(725 Downloads)
| Abstract (HTML) (3522 Views)
Full-Text: (1009 Views)
Introduction
The world is aging. It is estimated that by 2050, more than two billion people worldwide will be over sixty years old, and 21% of the world’s population will be elderly [1, 2]. In Iran, the elderly population is expected to reach 21.7% by 2050 [3]. Thus, by 2050, a quarter of Iran’s population will be elderly [4]. This phenomenon is driven by improvements in health conditions and disease prevention, a decrease in the number of marriages, and declining birth rates, which will increase the number of elderly individuals relative to the entire population [5, 6]. Without proper planning, population aging will become a major challenge for society. Lifestyle changes include reduced physical activity, poor nutrition and food abuse, and increased stress [7].
World Health Organization (WHO) research shows that more than 50% of people’s quality of life and health depends on their lifestyle [8, 9]. A healthy lifestyle is a complex set of health-related activities [10], which includes following the principles of proper nutrition, sleep health, engaging in necessary movement during the day and night, not smoking, regular periodic examinations, having mental health and participating in social activities with family and the community [11]. One of the most important and influential of these cases is the modification of nutritional habits. Research has shown that the unfavorable nutritional status of the elderly causes an increase in mortality and a decrease in the quality of life, and by improving the nutritional conditions, a large share of the chronic diseases of the elderly can be prevented and treated [12, 13]. At the same time, traditional medical care is often simple, safe, affordable, and protective [14]. In this way, the WHO has prioritized the development strategy of traditional medicine [15]. There is evidence that traditional medicine is growing in popularity around the world [16, 17]. Traditional medicine, which encompasses a set of sciences and skills based on theories and experiences aligned with the cultures of different regions, can be utilized to protect individual health and to diagnose or treat diseases within societies [18, 19].
Iranian medicine is one of the oldest and richest branches of medicine with practical strategies and methods, one of which is the principle of nutrition [15, 20, 21].
Aging is a natural biological process. Based on the characteristics of temperament in Iranian medicine, the main temperament of the elderly is cold and dry; therefore, the food choices and all measures taken for the elderly should be designed to ensure that the body’s temperament is warm and humid [22]. Consequently, it is very important to provide nutrition education to the elderly, which should be carried out in a scientific way and in accordance with the interventions planned by health and treatment personnel [23, 24]. Although the results of a review study indicate that the health recommendations found in the sources of Iranian medicine appear useful for improving the quality of life of the elderly, there is a need to conduct clinical trials to fill the gap in knowledge [14]. Several nutritional interventions based on Iranian medicine have been performed on different groups [19, 25, 26], but to knowledge, no intervention based on Iranian medicine has been performed on the elderly. Considering that Iran is a country that will enter an aging population in the future, guidelines for educational intervention for the elderly should be developed. To the best of our knowledge, this study is the first to investigate the effects of lifestyle intervention on knowledge, attitudes, and behaviors related to improving nutritional habits among older Iranians. Therefore, the aim of this study was to determine the effects of lifestyle intervention of Iranian medicine on the knowledge, attitude and behavior of the elderly in the context of reforming nutritional habits in 2022.
Methods
Study design and sampling
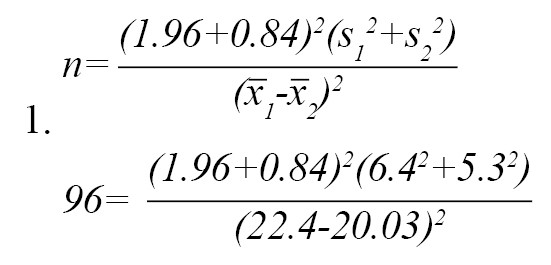
This research was an intervention study that was conducted in Fariman, Iran. Our statistical population was all the elderly of Fariman City. According to previous research [27], based on the changes related to performance and utilizing a 95% confidence and 80% power, it was calculated using the formula for comparing the averages in two groups that a sample size of 96 was needed for each group. To account for potential sample dropout, 10% was added to the calculated sample size, resulting in a minimum of 110 samples per group (Equation 1).
The sampling method used was random cluster sampling. From a total of eight comprehensive health service centers in Fariman City (four rural centers and four urban-rural centers), a total of four centers were selected by a simple random sampling method from among matched groups (two centers from rural centers and two centers from urban-rural centers). A total of 220 older adults were randomized into two groups: Control group (n=110) and intervention group (n=110) (Figure 1).
 The inclusion criteria were the age of 60 years and above and living in Fariman City. The exclusion criteria included having diseases, such as dementia and Alzheimer’s disease, as well as difficulty sitting for a long time. Additionally, participants who were absent from more than one training session were excluded from the study.
The inclusion criteria were the age of 60 years and above and living in Fariman City. The exclusion criteria included having diseases, such as dementia and Alzheimer’s disease, as well as difficulty sitting for a long time. Additionally, participants who were absent from more than one training session were excluded from the study.
Data collection tools
The tools used in this study were created by the researchers and consisted of a two-part questionnaire, which included demographic information and a questionnaire assessing knowledge, attitude, and behavior in the field of nutritional habit modification. The questionnaire was designed by reviewing the literature and studying standard questionnaires under the supervision of an Iranian medical expert and a health education expert, and its validity and reliability were confirmed.
To ensure that the most important and correct content (necessity of the item) was selected, the content validity ratio was used. Additionally, to confirm the items of the program are related to the desired topic, the CVI was used. In order to quantitatively determine the content validity ratio, 12 experts were invited to classify each item of the tool into three categories, including “necessary”, ”useful but not necessary” and “not necessary”. The content validity ratio was found to be 0.95 for all questionnaires. The content validity of the knowledge, attitude, and behavioral questionnaires was 0.88, 1, and 1, respectively.
To calculate the content validity index (CVI), evaluators commented on the three criteria of relevance or specificity, simplicity or fluency, and clarity or transparency based on a four-point scoring scale for each item. For this purpose, the respondents were asked to rate the relevance of each item on a 4-point scale: “Completely relevant =4”, “relevant but needs revision =3”, “requires serious revision =2”. and “not related =1”. A score of one was assigned to comments that did not meet the criteria in all questionnaires. The CVI was 1.00 for the knowledge questionnaire, 1.00 for the attitude questionnaire, and 1.00 for the behavior questionnaire.
Evaluators also commented on the clarity of each item using a four-point scale: “Completely clear =4”, “clear but needs revision =3”, “It needs serious revision =2” and “unclear =1”. The overall clarity score for the entire questionnaire was 0.99. The clarity score for the knowledge questionnaire was 0.99, the score for the attitude questionnaire was 1.00, and the score for the behavior questionnaire was 1.00.
Evaluators provided comments on the simplicity of each item using a 4-point scale: “Quite simple =4”, “simple but needs revision =3”, “needs serious revision =2” and “complicated =1”. The overall value for simplicity in the questionnaire was 0.99. The value for the knowledge questionnaire was 0.97, the value for the attitude questionnaire was 1.00, and the value for the behavior questionnaire was 1.00.
To measure the reliability of the questionnaire, it was completed by 30 elderly, and Cronbach’s α was calculated, yielding a reliability coefficient of 0.769 for all questionnaires.
In the knowledge questionnaire, this coefficient was 0.50; in the attitude questionnaire, it was 0.65; and in the behavior questionnaire, it was 0.73.
The questions related to knowledge included 15 items that were measured with “correct,” “incorrect,” or “I don’t know” (range: 0-15). The questions related to the attitude included 11 items that were rated from “completely disagree” to “completely agree” based on a five-point Likert scale (range: 11-55). Additionally, there were 15 questions related to the behavior of the elderly, which were evaluated using the options of “always,” “often,” “sometimes,” “rarely,” and “never” (range: 15-75).
Intervention
The intervention was conducted for the intervention group. The educational intervention consisted of four sessions presented to the intervention group using teaching aids such as slides and booklets. The outline, educational content, and method of educational intervention are given in Table 1.
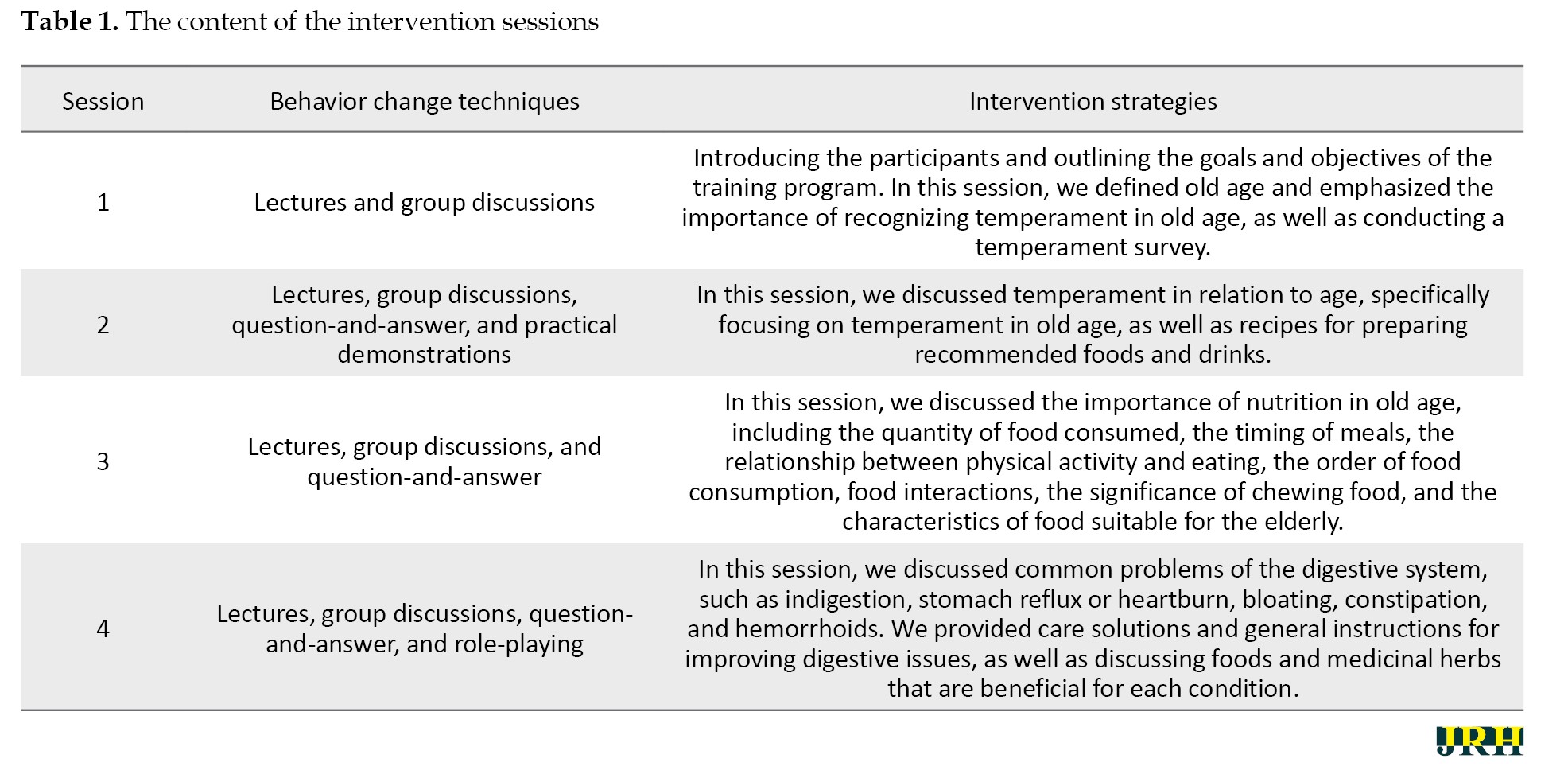
During the educational intervention, the intervention group was divided into ten groups, with 11 people in each group, and each group received four 90-minute training sessions (Table 1). The duration of the educational intervention was from October 2, 2022, to November 30, 2022.
The educational intervention was delivered through group face-to-face educational sessions, including lectures, group discussions, question and answer, practical demonstrations, role-playing, and the use of slides and blackboards. The source of information used for education was the guidelines for improving healthy lifestyles in the elderly, based on Iranian medical teaching (compiled by the vice-rector for health at Mashhad University of Medical Sciences) [28]. When introducing content, the language was kept concise and smooth, and the use of professional vocabulary.
Since our target group was the elderly, the speed of presenting the materials was intentionally slowed, and the educational materials were repeatedly summarized during the sessions. Feedback was gathered from the elderly in order to ensure their understanding of the material. In the training sessions, seniors who were successful in this field were used as role models in order to convey their successful experiences. At the beginning of the training sessions, the seniors were welcomed, then the goals of the training session were stated, and at the end, the seniors’ questions were asked, followed by a summary of the topics covered. Each training session lasted 90 minutes.
Data analysis
Data related to demographic and contextual observations of the participants were analyzed using SPSS software, version 23. We also conducted descriptive analyses (frequency, Mean±SD) and bivariate analyses (student’s t-test, chi-square test, repeated measures ANOVA, and independent t-test) to quantify the variation of different variables in the intervention and control groups. A P<0.05 was considered to be statistically significant.
Results
The results showed a statistically significant difference between the two groups in age, gender, source of income, employment status, education, and diabetes (P˂0.001) (Table 2).

According to Table 3, there was no significant difference in the baseline level of knowledge immediately after the intervention between the two groups; however, there was a significant difference in the level of knowledge at the 2-month follow-up (P=0.021).
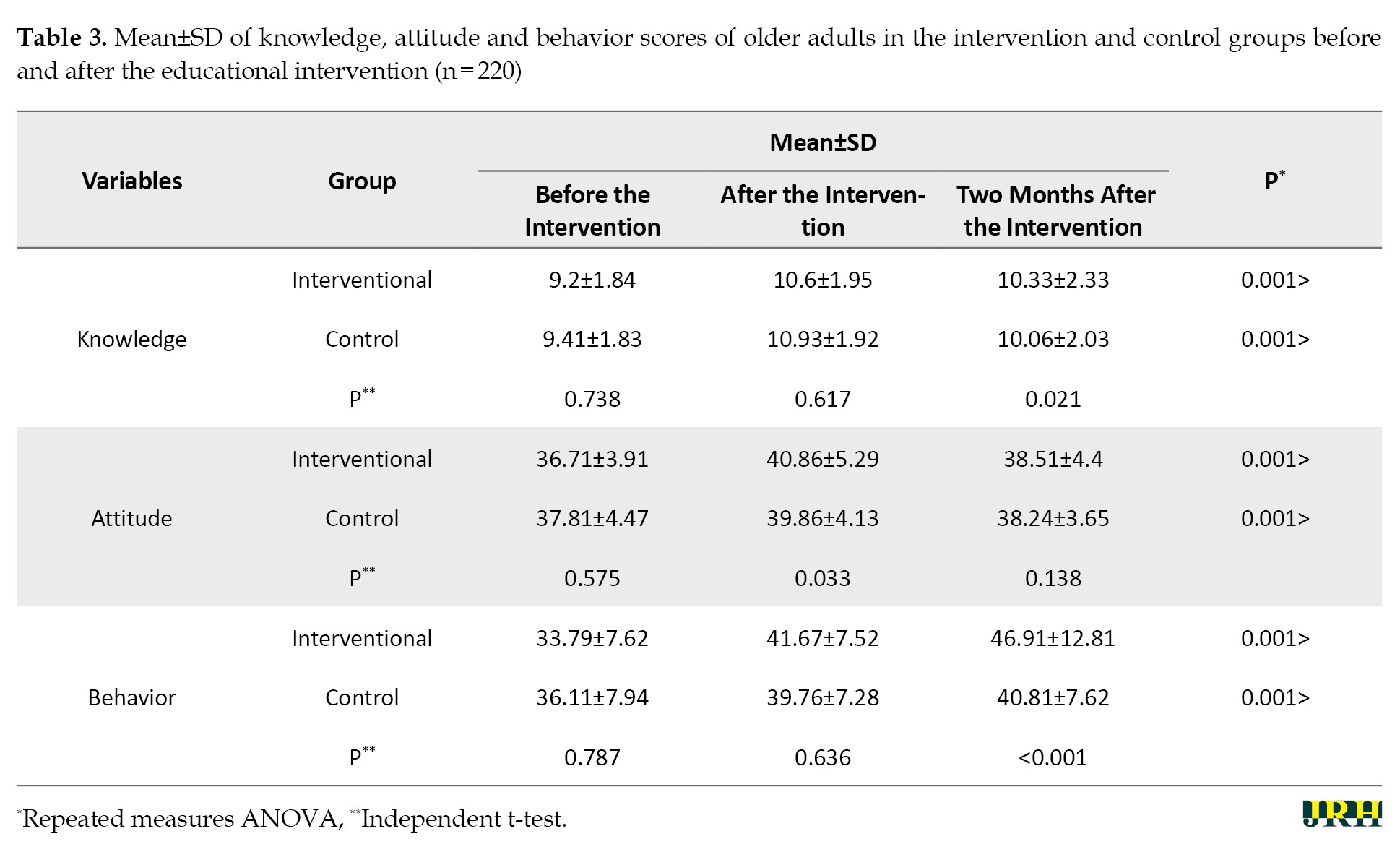
The changes in the intervention group immediately after the intervention increased by 0.131 compared to the control group, with a standard error of 0.283, but it was not significant (P=0.240). Additionally, at the 2-month follow-up, the knowledge score of the intervention group increased by 0.096 compared to the control group, with a standard error of 0.311, but this was also not significant (P=0.250) (Table 3).
As Table 3 shows, the baseline level of attitude and the 2-month follow-up were not significantly different between the two groups; however, the level of attitude immediately after the intervention was significantly different between the two groups (P=0.033). The results showed that the changes in the intervention group immediately after the intervention increased by 1.798 compared to the control group, with a standard error of 0.707, which was significant (P=0.012). However, at the 2-month follow-up, the attitude score of the intervention group increased by 0.384 compared to the control group, with a standard error of 0.599, but this was not significant (P=0.523) (Table 3).
There was no significant difference in the mean score of behavior at baseline and immediately after the intervention between the two groups; however, the behavior score at the 2-month follow-up showed a significant difference between the two groups (P≤0.001). Additionally, the results showed that the changes in the intervention group immediately after intervention increased by 0.269 compared to the control group, with a standard error of 1.083, but it was not significant (P=0.804). However, at the 2-month follow-up, the behavior score of the intervention group increased by 4.293 compared to the control group, with a standard error of 1.528, which was significant (P=0.005) (Table 3).
Discussion
We conducted this study in order to investigate the impact of lifestyle education in Iranian medicine on the knowledge, attitude, and behavior of older adults in the field of nutritional habits reform in 2022. This intervention was effective in improving older adults’ knowledge, attitude, and behavior. This study appears to be one of the few conducted in this field, as the researchers were unable to find any studies addressing the knowledge, attitude, and behavior of the elderly regarding nutritional habit reform within the context of Iranian medicine. Therefore, taking into account the similarity of the studies conducted, we will proceed to the discussion.
In different age groups, many studies have been conducted on people’s knowledge, attitude, and performance in the field of nutrition [29-31]. However, the target group of our study was the elderly, who faced many challenges [32]. Their educational interventions differ from those of other age groups; thus, only studies related to the older age group are examined here.
In our study, there was no significant difference in the knowledge level between the two groups before and immediately after the educational intervention. However, there was a significant difference between the two groups two months after the educational intervention. This may be attributed to the nature of the intervention, which was conducted once every two weeks for the elderly. After the educational intervention sessions, the questionnaires were completed and then the educational booklet was given to the elderly. Hence, the level of knowledge of the elderly immediately after the intervention did not differ significantly, likely due to forgetting the educational materials. However, two months later, after the elderly had read the booklet and implemented its content in their behavior, there was a significant difference in the level of knowledge.
In line with our study, Nanbakhsh et al. [33] in a semi-experimental study titled “The effect of elderly health education on the knowledge, attitude and performance of elderly women” showed that health education was effective in improving the level of knowledge of the elderly. However, there are differences between their study and ours [33]. In the study by Nanbakhsh et al. [33], the questionnaire was assessed before and six months after the intervention, and not immediately after the intervention in order to investigate changes that occurred immediately after the intervention. In line with the study by Nanbakhsh et al. [33], which did not investigate the level of knowledge immediately after the intervention, Alirezaei Shahraki et al. [34] did not complete the questionnaires immediately after the intervention, although they reported a significant improvement in the knowledge of elderly diabetic patients during the educational intervention.
In a study conducted by Gusty [35] to determine the effect of education on knowledge, attitude, and behavior in older adults with hypertension, the level of knowledge increased significantly in the intervention group, but the level of knowledge was not checked immediately after the intervention. Mirzaei et al. [36] also conducted an educational intervention on nutritional outcomes in two groups of elderly with sufficient and insufficient health literacy. The results showed that the average scores of knowledge in both intervention groups with sufficient or insufficient health literacy increased significantly. In this study, the questionnaires were not completed immediately after the intervention.
Regarding attitude, the attitude of the elderly before the training did not change significantly between the two groups, but immediately after the intervention, there was a significant change in the attitude of the elderly in the intervention group. However, this change in attitude was not stable and two months after the end of the intervention, there were no significant changes between the two groups. This non-sustainability of attitude change in the elderly is due to shortcomings in our educative intervention that should be considered and corrected in other studies. In the studies by Nanbakhsh et al. [33], Gusty [35], after the educational intervention, attitude changes were stable. It is important to note that the educational style, the number of sessions conducted, and the strategies and materials used in these studies differ from one another In the study by Mirzaei et al. [36], the attitude of the elderly who had sufficient health literacy increased significantly, and in the elderly who had insufficient health literacy, the attitude score did not show a significant increase after the intervention. This suggests that health literacy levels may play a role in changing attitude scores.
Regarding the behavior of the elderly adults, the results of the present study showed that there was no statistically significant difference in the behavior of the elderly between the two groups before and immediately after the educational intervention, but these changes were significant two months after the educational intervention. It is important to note that behaviors requiring investigation and improvement had not yet emerged immediately following the intervention, but over time, most of these changes can be reported. Malekafzali et al. [37] in Tehran showed that nine months after the intervention, women reduced the consumption of foods, such as meat and sweets, and increased the consumption of foods, such as vegetables. Notably, there was no significant difference in behavior before the intervention, which is consistent with our study. In our study, the elderly were not examined by gender, but in the study by Malekafzali et al. [37], the elderly were examined by gender. However, in the study by Malekafzali et al. [37], the elderly were assessed by gender, and within nine months, a significant change in behavior was noted among women, while no significant change was observed among men. In the study by Mirzaei et al. [36], there were no significant changes in performance two months after the educational intervention in the group with insufficient health literacy. In contrast, significant changes in the behavior of elderly individuals were observed in the group with sufficient health literacy two months after the educational intervention, although the questionnaires were not completed immediately after the intervention. In the studies by Nanbakhsh et al. [33] and Gusty [35], significant changes in the behavior of the elderly were noted after the educational intervention, but these changes were not evaluated immediately following the intervention.
Conclusion
The results of the study showed the effectiveness of the intervention in improving the nutritional knowledge, attitudes, and behaviors of the elderly based on Iranian medicine. This study focused on teaching nutritional topics related to Iranian medicine to older adults and, to our knowledge, was conducted for the first time. Although the changes in awareness were not significant immediately after the intervention, this may be attributed to the heavy educational content of Iranian medicine, such as temperament diagnosis. However, after two months of reading the provided booklet, the changes became significant. Attitude changes were significant immediately after the intervention, but were not significant two months later, suggesting that alternative educational styles should be employed to maintain these attitude changes. The behavioral changes among the elderly two months after the educational intervention were significant, which is the most important outcome of our intervention. In other words, changing behavior is the most important goal of our educational efforts. Therefore, it is suggested to perform such simple interventions for the elderly.
Strengths and limitations
Among the strengths of this study was the examination of knowledge, attitudes, and nutritional behaviors of the elderly based on Iranian medicine, which was done for the first time to our knowledge. The results showed that this intervention was effective in changing the behavior of the elderly. Therefore, it is recommended to carry out such low-cost interventions in health and treatment centers, cultural centers, parks, mosques, and other organizations for the elderly. Another strength of our study is that the intervention was conducted on 220 older adults divided into ten groups with 11 participants in each group, which is an appropriate sample size for an intervention study.
This study faced limitations. Some elderly did not participate in the 90-minute intervention sessions due to muscle problems; therefore, it is suggested to design training sessions with a greater number of shorter sessions. Another limitation was the investigation of the behavior of the elderly through self-reporting, which is not a suitable method for investigating behavior. Another limitation of this study is the lack of long-term follow-up of the educational intervention, which should be at least six months.
Ethical Considerations
Compliance with ethical guidelines
This study is based on a research project approved by the Mashhad University of Medical Sciences, Mashhad, Iran (Code: IR.MUMS.FHMPM.REC.1400.056). This study was conducted in accordance with the Helsinki Declaration throughout all phases. Confidentiality of data was ensured, and written informed consent was obtained from the participants.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Mahdi Gholian-aval; Methodology: Mohammad Ahmadian; Data collection: Toktam Forghani; Data analysis: Habibollah Esmaily; Investigation and writing: Elham Charoghchian Khorasani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the older adults who assisted the authors in conducting this research project.
References
The world is aging. It is estimated that by 2050, more than two billion people worldwide will be over sixty years old, and 21% of the world’s population will be elderly [1, 2]. In Iran, the elderly population is expected to reach 21.7% by 2050 [3]. Thus, by 2050, a quarter of Iran’s population will be elderly [4]. This phenomenon is driven by improvements in health conditions and disease prevention, a decrease in the number of marriages, and declining birth rates, which will increase the number of elderly individuals relative to the entire population [5, 6]. Without proper planning, population aging will become a major challenge for society. Lifestyle changes include reduced physical activity, poor nutrition and food abuse, and increased stress [7].
World Health Organization (WHO) research shows that more than 50% of people’s quality of life and health depends on their lifestyle [8, 9]. A healthy lifestyle is a complex set of health-related activities [10], which includes following the principles of proper nutrition, sleep health, engaging in necessary movement during the day and night, not smoking, regular periodic examinations, having mental health and participating in social activities with family and the community [11]. One of the most important and influential of these cases is the modification of nutritional habits. Research has shown that the unfavorable nutritional status of the elderly causes an increase in mortality and a decrease in the quality of life, and by improving the nutritional conditions, a large share of the chronic diseases of the elderly can be prevented and treated [12, 13]. At the same time, traditional medical care is often simple, safe, affordable, and protective [14]. In this way, the WHO has prioritized the development strategy of traditional medicine [15]. There is evidence that traditional medicine is growing in popularity around the world [16, 17]. Traditional medicine, which encompasses a set of sciences and skills based on theories and experiences aligned with the cultures of different regions, can be utilized to protect individual health and to diagnose or treat diseases within societies [18, 19].
Iranian medicine is one of the oldest and richest branches of medicine with practical strategies and methods, one of which is the principle of nutrition [15, 20, 21].
Aging is a natural biological process. Based on the characteristics of temperament in Iranian medicine, the main temperament of the elderly is cold and dry; therefore, the food choices and all measures taken for the elderly should be designed to ensure that the body’s temperament is warm and humid [22]. Consequently, it is very important to provide nutrition education to the elderly, which should be carried out in a scientific way and in accordance with the interventions planned by health and treatment personnel [23, 24]. Although the results of a review study indicate that the health recommendations found in the sources of Iranian medicine appear useful for improving the quality of life of the elderly, there is a need to conduct clinical trials to fill the gap in knowledge [14]. Several nutritional interventions based on Iranian medicine have been performed on different groups [19, 25, 26], but to knowledge, no intervention based on Iranian medicine has been performed on the elderly. Considering that Iran is a country that will enter an aging population in the future, guidelines for educational intervention for the elderly should be developed. To the best of our knowledge, this study is the first to investigate the effects of lifestyle intervention on knowledge, attitudes, and behaviors related to improving nutritional habits among older Iranians. Therefore, the aim of this study was to determine the effects of lifestyle intervention of Iranian medicine on the knowledge, attitude and behavior of the elderly in the context of reforming nutritional habits in 2022.
Methods
Study design and sampling
This research was an intervention study that was conducted in Fariman, Iran. Our statistical population was all the elderly of Fariman City. According to previous research [27], based on the changes related to performance and utilizing a 95% confidence and 80% power, it was calculated using the formula for comparing the averages in two groups that a sample size of 96 was needed for each group. To account for potential sample dropout, 10% was added to the calculated sample size, resulting in a minimum of 110 samples per group (Equation 1).
The sampling method used was random cluster sampling. From a total of eight comprehensive health service centers in Fariman City (four rural centers and four urban-rural centers), a total of four centers were selected by a simple random sampling method from among matched groups (two centers from rural centers and two centers from urban-rural centers). A total of 220 older adults were randomized into two groups: Control group (n=110) and intervention group (n=110) (Figure 1).
Data collection tools
The tools used in this study were created by the researchers and consisted of a two-part questionnaire, which included demographic information and a questionnaire assessing knowledge, attitude, and behavior in the field of nutritional habit modification. The questionnaire was designed by reviewing the literature and studying standard questionnaires under the supervision of an Iranian medical expert and a health education expert, and its validity and reliability were confirmed.
To ensure that the most important and correct content (necessity of the item) was selected, the content validity ratio was used. Additionally, to confirm the items of the program are related to the desired topic, the CVI was used. In order to quantitatively determine the content validity ratio, 12 experts were invited to classify each item of the tool into three categories, including “necessary”, ”useful but not necessary” and “not necessary”. The content validity ratio was found to be 0.95 for all questionnaires. The content validity of the knowledge, attitude, and behavioral questionnaires was 0.88, 1, and 1, respectively.
To calculate the content validity index (CVI), evaluators commented on the three criteria of relevance or specificity, simplicity or fluency, and clarity or transparency based on a four-point scoring scale for each item. For this purpose, the respondents were asked to rate the relevance of each item on a 4-point scale: “Completely relevant =4”, “relevant but needs revision =3”, “requires serious revision =2”. and “not related =1”. A score of one was assigned to comments that did not meet the criteria in all questionnaires. The CVI was 1.00 for the knowledge questionnaire, 1.00 for the attitude questionnaire, and 1.00 for the behavior questionnaire.
Evaluators also commented on the clarity of each item using a four-point scale: “Completely clear =4”, “clear but needs revision =3”, “It needs serious revision =2” and “unclear =1”. The overall clarity score for the entire questionnaire was 0.99. The clarity score for the knowledge questionnaire was 0.99, the score for the attitude questionnaire was 1.00, and the score for the behavior questionnaire was 1.00.
Evaluators provided comments on the simplicity of each item using a 4-point scale: “Quite simple =4”, “simple but needs revision =3”, “needs serious revision =2” and “complicated =1”. The overall value for simplicity in the questionnaire was 0.99. The value for the knowledge questionnaire was 0.97, the value for the attitude questionnaire was 1.00, and the value for the behavior questionnaire was 1.00.
To measure the reliability of the questionnaire, it was completed by 30 elderly, and Cronbach’s α was calculated, yielding a reliability coefficient of 0.769 for all questionnaires.
In the knowledge questionnaire, this coefficient was 0.50; in the attitude questionnaire, it was 0.65; and in the behavior questionnaire, it was 0.73.
The questions related to knowledge included 15 items that were measured with “correct,” “incorrect,” or “I don’t know” (range: 0-15). The questions related to the attitude included 11 items that were rated from “completely disagree” to “completely agree” based on a five-point Likert scale (range: 11-55). Additionally, there were 15 questions related to the behavior of the elderly, which were evaluated using the options of “always,” “often,” “sometimes,” “rarely,” and “never” (range: 15-75).
Intervention
The intervention was conducted for the intervention group. The educational intervention consisted of four sessions presented to the intervention group using teaching aids such as slides and booklets. The outline, educational content, and method of educational intervention are given in Table 1.
During the educational intervention, the intervention group was divided into ten groups, with 11 people in each group, and each group received four 90-minute training sessions (Table 1). The duration of the educational intervention was from October 2, 2022, to November 30, 2022.
The educational intervention was delivered through group face-to-face educational sessions, including lectures, group discussions, question and answer, practical demonstrations, role-playing, and the use of slides and blackboards. The source of information used for education was the guidelines for improving healthy lifestyles in the elderly, based on Iranian medical teaching (compiled by the vice-rector for health at Mashhad University of Medical Sciences) [28]. When introducing content, the language was kept concise and smooth, and the use of professional vocabulary.
Since our target group was the elderly, the speed of presenting the materials was intentionally slowed, and the educational materials were repeatedly summarized during the sessions. Feedback was gathered from the elderly in order to ensure their understanding of the material. In the training sessions, seniors who were successful in this field were used as role models in order to convey their successful experiences. At the beginning of the training sessions, the seniors were welcomed, then the goals of the training session were stated, and at the end, the seniors’ questions were asked, followed by a summary of the topics covered. Each training session lasted 90 minutes.
Data analysis
Data related to demographic and contextual observations of the participants were analyzed using SPSS software, version 23. We also conducted descriptive analyses (frequency, Mean±SD) and bivariate analyses (student’s t-test, chi-square test, repeated measures ANOVA, and independent t-test) to quantify the variation of different variables in the intervention and control groups. A P<0.05 was considered to be statistically significant.
Results
The results showed a statistically significant difference between the two groups in age, gender, source of income, employment status, education, and diabetes (P˂0.001) (Table 2).
According to Table 3, there was no significant difference in the baseline level of knowledge immediately after the intervention between the two groups; however, there was a significant difference in the level of knowledge at the 2-month follow-up (P=0.021).
The changes in the intervention group immediately after the intervention increased by 0.131 compared to the control group, with a standard error of 0.283, but it was not significant (P=0.240). Additionally, at the 2-month follow-up, the knowledge score of the intervention group increased by 0.096 compared to the control group, with a standard error of 0.311, but this was also not significant (P=0.250) (Table 3).
As Table 3 shows, the baseline level of attitude and the 2-month follow-up were not significantly different between the two groups; however, the level of attitude immediately after the intervention was significantly different between the two groups (P=0.033). The results showed that the changes in the intervention group immediately after the intervention increased by 1.798 compared to the control group, with a standard error of 0.707, which was significant (P=0.012). However, at the 2-month follow-up, the attitude score of the intervention group increased by 0.384 compared to the control group, with a standard error of 0.599, but this was not significant (P=0.523) (Table 3).
There was no significant difference in the mean score of behavior at baseline and immediately after the intervention between the two groups; however, the behavior score at the 2-month follow-up showed a significant difference between the two groups (P≤0.001). Additionally, the results showed that the changes in the intervention group immediately after intervention increased by 0.269 compared to the control group, with a standard error of 1.083, but it was not significant (P=0.804). However, at the 2-month follow-up, the behavior score of the intervention group increased by 4.293 compared to the control group, with a standard error of 1.528, which was significant (P=0.005) (Table 3).
Discussion
We conducted this study in order to investigate the impact of lifestyle education in Iranian medicine on the knowledge, attitude, and behavior of older adults in the field of nutritional habits reform in 2022. This intervention was effective in improving older adults’ knowledge, attitude, and behavior. This study appears to be one of the few conducted in this field, as the researchers were unable to find any studies addressing the knowledge, attitude, and behavior of the elderly regarding nutritional habit reform within the context of Iranian medicine. Therefore, taking into account the similarity of the studies conducted, we will proceed to the discussion.
In different age groups, many studies have been conducted on people’s knowledge, attitude, and performance in the field of nutrition [29-31]. However, the target group of our study was the elderly, who faced many challenges [32]. Their educational interventions differ from those of other age groups; thus, only studies related to the older age group are examined here.
In our study, there was no significant difference in the knowledge level between the two groups before and immediately after the educational intervention. However, there was a significant difference between the two groups two months after the educational intervention. This may be attributed to the nature of the intervention, which was conducted once every two weeks for the elderly. After the educational intervention sessions, the questionnaires were completed and then the educational booklet was given to the elderly. Hence, the level of knowledge of the elderly immediately after the intervention did not differ significantly, likely due to forgetting the educational materials. However, two months later, after the elderly had read the booklet and implemented its content in their behavior, there was a significant difference in the level of knowledge.
In line with our study, Nanbakhsh et al. [33] in a semi-experimental study titled “The effect of elderly health education on the knowledge, attitude and performance of elderly women” showed that health education was effective in improving the level of knowledge of the elderly. However, there are differences between their study and ours [33]. In the study by Nanbakhsh et al. [33], the questionnaire was assessed before and six months after the intervention, and not immediately after the intervention in order to investigate changes that occurred immediately after the intervention. In line with the study by Nanbakhsh et al. [33], which did not investigate the level of knowledge immediately after the intervention, Alirezaei Shahraki et al. [34] did not complete the questionnaires immediately after the intervention, although they reported a significant improvement in the knowledge of elderly diabetic patients during the educational intervention.
In a study conducted by Gusty [35] to determine the effect of education on knowledge, attitude, and behavior in older adults with hypertension, the level of knowledge increased significantly in the intervention group, but the level of knowledge was not checked immediately after the intervention. Mirzaei et al. [36] also conducted an educational intervention on nutritional outcomes in two groups of elderly with sufficient and insufficient health literacy. The results showed that the average scores of knowledge in both intervention groups with sufficient or insufficient health literacy increased significantly. In this study, the questionnaires were not completed immediately after the intervention.
Regarding attitude, the attitude of the elderly before the training did not change significantly between the two groups, but immediately after the intervention, there was a significant change in the attitude of the elderly in the intervention group. However, this change in attitude was not stable and two months after the end of the intervention, there were no significant changes between the two groups. This non-sustainability of attitude change in the elderly is due to shortcomings in our educative intervention that should be considered and corrected in other studies. In the studies by Nanbakhsh et al. [33], Gusty [35], after the educational intervention, attitude changes were stable. It is important to note that the educational style, the number of sessions conducted, and the strategies and materials used in these studies differ from one another In the study by Mirzaei et al. [36], the attitude of the elderly who had sufficient health literacy increased significantly, and in the elderly who had insufficient health literacy, the attitude score did not show a significant increase after the intervention. This suggests that health literacy levels may play a role in changing attitude scores.
Regarding the behavior of the elderly adults, the results of the present study showed that there was no statistically significant difference in the behavior of the elderly between the two groups before and immediately after the educational intervention, but these changes were significant two months after the educational intervention. It is important to note that behaviors requiring investigation and improvement had not yet emerged immediately following the intervention, but over time, most of these changes can be reported. Malekafzali et al. [37] in Tehran showed that nine months after the intervention, women reduced the consumption of foods, such as meat and sweets, and increased the consumption of foods, such as vegetables. Notably, there was no significant difference in behavior before the intervention, which is consistent with our study. In our study, the elderly were not examined by gender, but in the study by Malekafzali et al. [37], the elderly were examined by gender. However, in the study by Malekafzali et al. [37], the elderly were assessed by gender, and within nine months, a significant change in behavior was noted among women, while no significant change was observed among men. In the study by Mirzaei et al. [36], there were no significant changes in performance two months after the educational intervention in the group with insufficient health literacy. In contrast, significant changes in the behavior of elderly individuals were observed in the group with sufficient health literacy two months after the educational intervention, although the questionnaires were not completed immediately after the intervention. In the studies by Nanbakhsh et al. [33] and Gusty [35], significant changes in the behavior of the elderly were noted after the educational intervention, but these changes were not evaluated immediately following the intervention.
Conclusion
The results of the study showed the effectiveness of the intervention in improving the nutritional knowledge, attitudes, and behaviors of the elderly based on Iranian medicine. This study focused on teaching nutritional topics related to Iranian medicine to older adults and, to our knowledge, was conducted for the first time. Although the changes in awareness were not significant immediately after the intervention, this may be attributed to the heavy educational content of Iranian medicine, such as temperament diagnosis. However, after two months of reading the provided booklet, the changes became significant. Attitude changes were significant immediately after the intervention, but were not significant two months later, suggesting that alternative educational styles should be employed to maintain these attitude changes. The behavioral changes among the elderly two months after the educational intervention were significant, which is the most important outcome of our intervention. In other words, changing behavior is the most important goal of our educational efforts. Therefore, it is suggested to perform such simple interventions for the elderly.
Strengths and limitations
Among the strengths of this study was the examination of knowledge, attitudes, and nutritional behaviors of the elderly based on Iranian medicine, which was done for the first time to our knowledge. The results showed that this intervention was effective in changing the behavior of the elderly. Therefore, it is recommended to carry out such low-cost interventions in health and treatment centers, cultural centers, parks, mosques, and other organizations for the elderly. Another strength of our study is that the intervention was conducted on 220 older adults divided into ten groups with 11 participants in each group, which is an appropriate sample size for an intervention study.
This study faced limitations. Some elderly did not participate in the 90-minute intervention sessions due to muscle problems; therefore, it is suggested to design training sessions with a greater number of shorter sessions. Another limitation was the investigation of the behavior of the elderly through self-reporting, which is not a suitable method for investigating behavior. Another limitation of this study is the lack of long-term follow-up of the educational intervention, which should be at least six months.
Ethical Considerations
Compliance with ethical guidelines
This study is based on a research project approved by the Mashhad University of Medical Sciences, Mashhad, Iran (Code: IR.MUMS.FHMPM.REC.1400.056). This study was conducted in accordance with the Helsinki Declaration throughout all phases. Confidentiality of data was ensured, and written informed consent was obtained from the participants.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Mahdi Gholian-aval; Methodology: Mohammad Ahmadian; Data collection: Toktam Forghani; Data analysis: Habibollah Esmaily; Investigation and writing: Elham Charoghchian Khorasani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the older adults who assisted the authors in conducting this research project.
References
- Bahador F, Mahfoozpour S, Masoudiasl I, Vahdat S. [A systematic review of the management of preventive health care for the elderly in the world (Persian)]. Salmand. 2022; 16(4):592-607. [DOI:10.32598/sija.2021.3180.2]
- Karami -Agh Ghaleh H, Dehdari T, Hosseini AS. [Exploring the experience of loneliness in the older single women in Tehran City, Iran (Persian)]. Salmand. 2025; 19(4):544-57. [DOI:10.32598/sija.2024.3619.1]
- Manoochehry S, Rasouli HR. Iranian population policy and aging: New health concerns. International Journal of Travel Medicine and Global Health. 2017; 5(2):70-1. [DOI:10.15171/ijtmgh.2017.14]
- Sahebi MK. [The importance of new technologies in the great challenge of the country's aging (Persian)]. Journal of Gerontology. 2022; 7(1):1-2. [DOI:10.22034/JOGE.7.1.1]
- Zadehahmad Z, Abdollahi M, Sany SB, Khorasani EC. Tendency to childbearing and its relationship with spiritual health and health literacy in women referred to the healthcare centers of Torbat Heydarieh, Iran, in 2019. Razi Journal of Medical Sciences. 2020. 27(8):32-41. [Link]
- Tehrani H, Vali M, Nejatian M, Moshki M, Charoghchian Khorasani E, et al. The status of depression literacy and its relationship with quality of life among Iranian public population: A cross sectional study. BMC Psychiatry. 2022; 22(1):607. [DOI:10.1186/s12888-022-04251-0] [PMID] [PMCID]
- Keshavarznouroozpour R, Mahmoodinezhad H, Etesam I. [Investigating the impact of lifestyle changes (Persian)]. Political Sociology. 2023; 5(11):5679-95. [DOI:10.30510/psi.2022.290809.1826]
- Estebsari F, Taghdisi MH, Rahimi Foroushani A, Eftekhar Ardebili H, Shojaeizadeh D. An educational program based on the successful aging approach on health-promoting behaviors in the elderly: A clinical trial study. Iranian Red Crescent Medical Journal. 2014; 16(4):e16314. [DOI:10.5812/ircmj.16314] [PMID]
- Khorasani EC, Peyman N, Yaghobi F. Health promoting schools in Iran: Features and challenges. Journal of Education and Community Health. 2019; 6(3):127-9.[DOI:10.29252/jech.6.3.127]
- Al-Gimavi SM, Bakhshi M, Ghanbari Moghaddam A, Ghavami V, Al-Khalidi H. [A comparative study of healthy lifestyle of Iranian and Iraqi elderly and its predictors (Persian)]. Iranian Journal of Ageing. 2023; 18(1):118-33. [DOI:10.32598/sija.2022.3420.1]
- Wahlqvist ML, Saviage GS. Interventions aimed at dietary and lifestyle changes to promote healthy aging. European Journal of Clinical Nutrition. 2000; 54(Suppl 3):S148-56. [DOI:10.1038/sj.ejcn.1601037] [PMID]
- Lashkarboloki F, Aryaei M, Djazayery A, Eftekhar-Ardebily H, Minaei M. [Association of demographic, socio-economic features and some health problems with nutritional status in elderly (Persian)]. Iranian Journal of Nutrition Sciences and Food Technology. 2015; 9(4):27-34. [Link]
- Gholian-Aval M, Tehrani H, Salari M, Mohammadi M. [Related factors on the preventive behaviors of covid-19 in the elderly aged 60-75 years in Mashhad in 1400 (Persian)]. Journal of Gerontology. 2023; 8(3):46-55. [DOI:10.22034/JOGE.8.3.46]
- Parvizi MM, Nimrouzi M, Lankarani KB, Morteza S, Alorizi E, Hajimonfarednejad M. Health recommendations for the elderly in the viewpoint of traditional Persian medicine. Shiraz E-Medical Journal. 2018; 19(1):e14201. [DOI:10.5812/semj.14201]
- Moradi Dehnavi H, Pakzad A, Fakhari Zavare M. [Designing dietary measures based on persian medicine for individuals with cold and dry temperament (Persian)]. Qom University of Medical Sciences Journal. 2021; 14(11):61-8. [DOI:10.52547/qums.14.11.61]
- Tehrani H, Dadashi N, Movahedzadeh D, Khorasani EC, Jafari A. The predictors of the use of complementary and alternative medicine among type 2 diabetes patients based on the health belief model. Journal of Diabetes and Metabolic Disordersd. 2022; 21(1):285-92. [DOI:10.1007/s40200-022-00971-y] [PMID] [PMCID]
- Khorasani, E.C., Ardameh, M., Sany, S.B.T. et al. The influence of emotional intelligence on academic stress among medical students in Neyshabur, Iran. BMC Psychiatry 23, 848 (2023). [DOI: 10.1186/s12888-023-05344-0] [PMID]
- World Health Organization (WHO). The promotion and development of traditional medicine: Report of a WHO meeting. Geneva: World Health Organization, 1987. [Link]
- Shahraeini M, Shoorab NJ, Javan R, Shakeri MT. The effect of group counseling about the nutritional measures of Iranian traditional medicine on the vasomotor domain of quality of life in postmenopausal women. Hayat. 2020; 25(4):458-72. [Link]
- Ansaripour M, Naseri M, Esfahani MM, Nabipour I, Rakhshani F, Zargaran A, et al. Periconceptional care and offspring health at birth and long term, from the perspective of Avicenna. Journal of Integrative Medicine. 2019; 17(2):80-86. [DOI:10.1016/j.joim.2019.01.003] [PMID]
- Ferdosi M, Soltani F, Molavi Taleghani Y. [Status of traditional medicine in a healthy life style: Review study (Persian)]. Journal of Islamic and Iranian Traditional Medicine. 2016; 7(1):1-6. [Link]
- Beykverdi M, Yavari M. [Nutrition in different life periods: From Persian medicine to conventional medicine (Persian)]. Journal of Islamic and Iranian Traditional Medicine. 2017; 7(4):397-407. [Link]
- Michalczyk MM, Zajac-Gawlak I, Zając A, Pelclová J, Roczniok R, Langfort J. Influence of nutritional education on the diet and nutritional behaviors of elderly women at the university of the third age. International Journal of Environmental Research and Public Health. 2020; 17(3):696. [DOI:10.3390/ijerph17030696] [PMID] [PMCID]
- Tassi A. Elderly pationts knowledge and attitudes regarding Infulunza vaccination in Bekka. Health and Wellbeing. 2020; 3(1):1-8. [DOI:10.54729/2789-8288.1044]
- Sepehrirad M, Toozandehjani H. [Effectiveness of cognitive-behavioral group therapy training and nutritional strategies based on traditional medicine on Premenstrual Syndrome (Persian)]. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2015; 18(177):11-9. [DOI:10.22038/ijogi.2016.6453]
- Shahraeini M, Jahani Shourab N, Javan R, shakeri MT. [Effect of food-based strategies of Iranian traditional medicine on women's quality of life during menopause (Persian)]. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2021; 23(12):67-75. [DOI:10.22038/ijogi.2021.17828]
- Shamsi MO, Byati A. [The effect of education on knowledge, attitude and practice of pregnant woman referring to health centers about self-medication in Arak city (Persian)]. Internal Medicine Today. 2009; 15(3):27-35. [Link]
- Jafarinejad MM. Ahmadian M, Izadpanah M. [Educational set of health educators, a guide to improve healthy lifestyle in old age based on the teachings of Iranian medicine (Persian)]. Mashhad: Vice President of Health, Mashhad University of Medical Sciences; 2022.
- Charles Shapu R, Ismail S, Ahmad N, Lim PY, Abubakar Njodi I. Systematic review: Effect of health education intervention on improving knowledge, attitudes and practices of adolescents on malnutrition. Nutrients. 2020; 12(8):2426. [DOI:10.3390/nu12082426] [PMID] [PMCID]
- Teo CH, Chin YS, Lim PY, Masrom SAH, Shariff ZM. School-based intervention that integrates nutrition education and supportive healthy school food environment among Malaysian primary school children: A study protocol. BMC Public Health. 2019; 19(1):1427. [DOI:10.1186/s12889-019-7708-y] [PMID] [PMCID]
- Moitra P, Madan J, Verma P. Impact of a behaviourally focused nutrition education intervention on attitudes and practices related to eating habits and activity levels in Indian adolescents. Public Health Nutrition. 2021; 24(9):2715-26. [DOI:10.1017/S1368980021000203] [PMID] [PMCID]
- al-Zeer F, Kilani H. Improving the quality of movement biomechanically by knowledge of results and knowledge of performance of some elderly women in Palestine. Dirasat. 2021; 48(3). [Link]
- Nanbakhsh F, Mohaddesi H, Amirai A, Broomand F, Bahadori F, Gol Mohamadlo S. [The effect of health education on elderly weomen life quality (Persian)]. Payavard Salamat. 2011; 5(1):47-57. [Link]
- Alirezaei Shahraki R, Aliakbari Kamrani A, Sahaf R, Abolfathi Momtaz Y. [Effects of nationwide program for prevention and control of diabetes initiated by the ministry of health on elderly diabetic patients’ knowledge, attitude and practice in Isfahan (Persian)]. Salmand. 2019. 14(1):84-95. [DOI:10.32598/SIJA.14.1.84]
- Gusty RP. Health education model for elderly hypertension on knowledge, attitudes, and adherence to following the dietary approaches to stop hypertension. Jurnal Aisyah. 2023, 2023. 8(2):955–62. [DOI:10.30604/jika.v8i3.2093]
- Mirzaei A, Ramezankhani A, Taheri Tanjani P, Ghaffari M, Jorvand R, Bazyar M, et al. [The effectiveness of health literacy based educational intervention on nutritional outcomes of elderly (Persian)]. Salmand. 2020. 15(3):324-37. [DOI:10.32598/sija.15.3.2569.1]
- Malekafzali H, Baradaran Eftekhari M, Hejazi F, Khojasteh T, Noot RH, Falahat K, et al. The effectiveness of educational intervention in the health promotion in elderly people. Iranian Journal of Public Health. 2010; 39(2):18-23.] [PMID]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2024/03/10 | Accepted: 2024/07/13 | Published: 2025/05/30
Received: 2024/03/10 | Accepted: 2024/07/13 | Published: 2025/05/30
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
