

Volume 15, Issue 1 (Jan & Feb 2025)
J Research Health 2025, 15(1): 41-50 |
Back to browse issues page



Ethics code: NA
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mishra A, Gaurav A, Kumar S. Mental Health of Older Professionals and Agricultural Workers from a Gender Perspective in India. J Research Health 2025; 15 (1) :41-50
URL: http://jrh.gmu.ac.ir/article-1-2546-en.html
URL: http://jrh.gmu.ac.ir/article-1-2546-en.html



1- Department of Statistics, Central University of South Bihar, Gaya, India.
2- Department of Statistics, Central University of South Bihar, Gaya, India. ,sunit@cusb.ac.in
2- Department of Statistics, Central University of South Bihar, Gaya, India. ,
Full-Text [PDF 894 kb]
(712 Downloads)
| Abstract (HTML) (3792 Views)
Full-Text: (1133 Views)
Introduction
The relevance of the workplace in mental well-being is increasing. We spend most of our time at the workplace; hence, the work environment is essential for mental well-being. Work can provide economic fulfillment and satisfaction, but work-related stress may also cause mental health issues [1]. Prior research indicates that poor working environments can cause workplace-related stress [2], psychological distress [3] and other mental health issues [4]. Work productivity is essential to physical and mental health [5]. Work stress negatively impacts mental health, and different occupations have distinct work conditions. Farmers are frequently subjected to unfavorable working conditions, including lengthy working hours, monotonous labor, and a hazardous work environment [6]. Similarly, in the professional sector, mental health issues are caused by inflexible timetables and obligatory overtime hours [7]. Moreover, healthcare professionals frequently encounter mental health problems [7-9]. These effects can vary depending on the gender of the individual. Female doctors were 32% more likely than male colleagues to suffer from depression [10]. Male educators are less inclined to seek social assistance, reflecting significant gender disparities in seeking help for mental disorders [11, 12]. Farmers reported higher rates of depression and anxiety compared to other occupations [13, 14]. However, not all studies match that the mental health of farmers is inferior to others [15].
The Indian population continues to grow and change [16]. According to the 2011 census, 9% of India’s population is 60 or older [17]. Aging is linked to a decline in functioning and the development of several disabilities, such as mental, physical, social, and economic restrictions [18, 19]. Agriculture, which serves as the foundation of the Indian economy, plays a pivotal role in the country’s socio-economic domain [20]. Growth in agriculture is believed to be essential in India, with over 70% of total workers dependent on this sector [21]. The physical strength needed for agricultural productivity drops around middle age, necessitating more labor for the same amount of yield. On average, older workers are less productive than younger workers, and labor force aging has a slight negative impact on productivity [22]. However, older farmers’ expertise improves input combinations, making a unit of effort more efficacious [23]. Future climate change will render farmers’ jobs harder [24]. The literature review identified four primary factors that significantly impact farmers’ mental well-being: Financial challenges, climate variabilities, and compromised physical health due to past incidents. Women are especially vulnerable to these challenges [14].
The agricultural sector in India is in the midst of a crisis, including diminishing land sizes, inflation, rising production expenses, etc. [25]. The National Commission of Farmers (NCF, 2005) [26] indicates that as the number of males abandoning rural areas increases, more women are taking on agricultural responsibilities [27]. Despite their hard work, women in agriculture are often undervalued. They perform physically demanding tasks in agriculture and household chores, yet men reap the benefits of their labor [27]. Male dominance over women exists in the Indian sociocultural setting [27]. Women are generally overrepresented in unpaid, seasonal, and part-time labor [27]. Such inequalities have resulted in higher psychological distress levels among female farmers than their male counterparts [28, 29]. We must acknowledge gender-based disparities and strive toward a more equitable future.
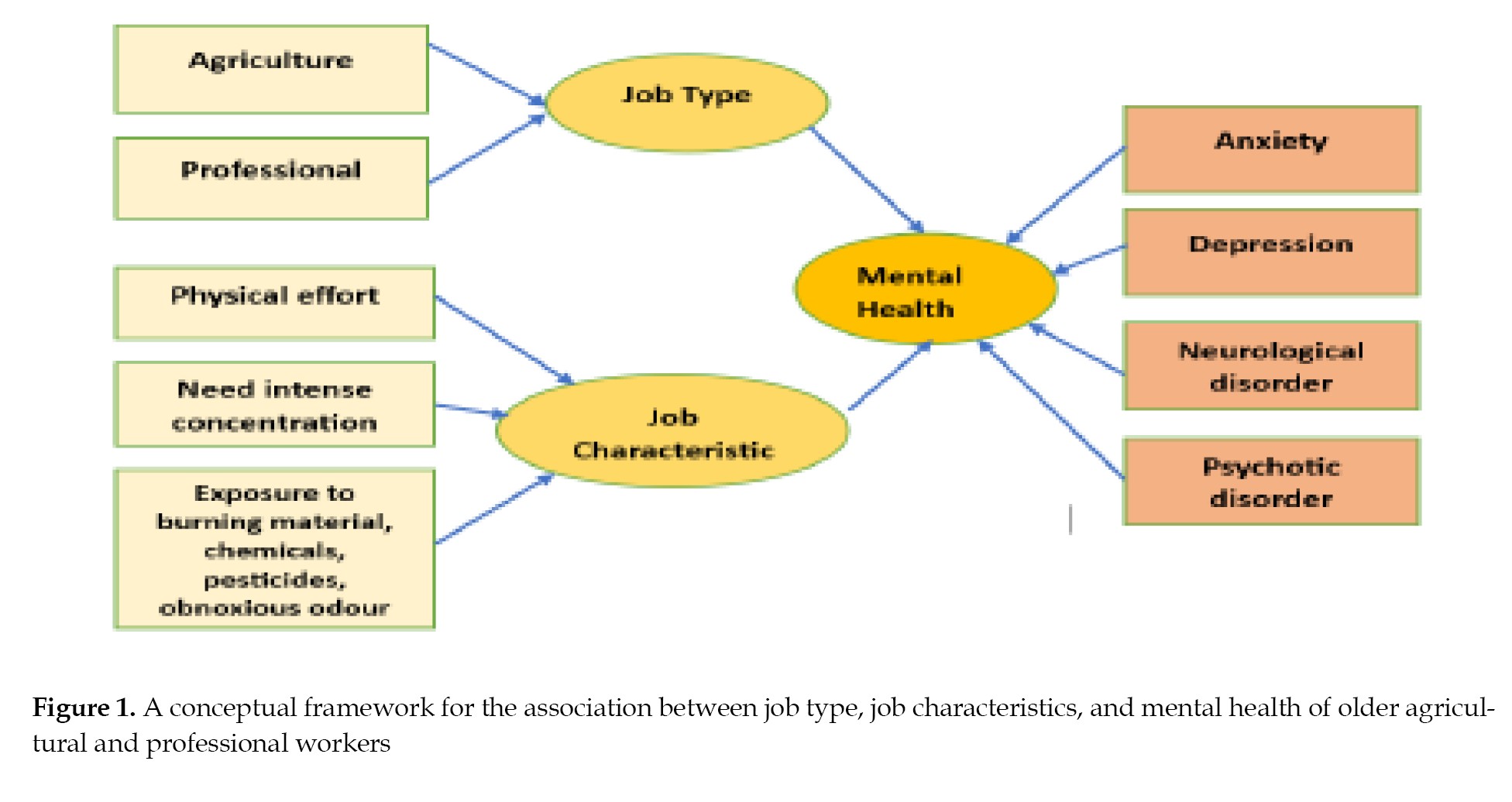
Previous research suggests that occupation and work environment influence mental health [1-4]. However, many studies fall short of providing a thorough knowledge of older workers’ mental health, particularly when gender is considered. In most countries, men’s duties in agricultural operations must be directed and unambiguous. Nevertheless, women’s contributions to agriculture are seldom appreciated. Job strain has been found to affect life stress among women [30]. Furthermore, earlier research did not focus on agricultural workers. However, India is an agriculture-based country; thus, it is critical to emphasize agricultural workers’ mental health. To comprehensively evaluate, we will compare the mental health of agricultural workers to other professionals. This study aimed to understand better the links between occupation, work environment, and mental health in older individuals of both genders considering gender differences. The present study revolves around the following (Figure 1) conceptual model.
Methods
This study utilized the longitudinal ageing study in India (LASI), a national longitudinal study on aging and health encompassing all Indian states and UTs except Sikkim. It is supervised by the Indian government, coordinated by the International Institute for Population Sciences (IIPS), Mumbai, and partners with the Harvard T.H. Chan School of Public Health and the University of Southern California. It is financially supported by various national and international bodies, including the national program for health care of older people and the United Nations Population Fund. LASI is the world’s largest and India’s only study of its kind, offering crucial insights into the economic dimensions of aging in India.
Our study examined 31,464 individuals aged 60 and above, drawn from the initial LASI wave of 72,250 individuals, focused on those with at least three months of work experience. The sample included 9936 in agriculture, 1856 in professional sectors (including higher education, accountancy, and health), and 11792 working in other sectors (mining, construction, manufacturing, wholesale and retail trade, and transportation). The aim was to investigate mental health disparities between workers in agriculture and professional fields, noting a gender divide with 7149 males (56.95% in agriculture) and 4643 females (92.14% in agriculture). This comparison seeks to shed light on sector-specific mental health challenges among older employees.
Outcome variable
The study considered mental health as the outcome variable. According to the World Health Organization (WHO), “mental health is not just the absence of mental disorders. It is a state of mental well-being that empowers individuals to handle life’s challenges, learn efficiently, work productively, and contribute to society” [31]. To measure mental health, we relied on the international classification of diseases (ICD-10), a globally recognized standard for diagnosing mental disorders [32], which focuses on four key indicators of mental disorders: Anxiety, depression, neurological, and psychotic disorders. In LASI, self-reported questions related to the symptoms of mental disorder were asked. These questions include sleep disorder (waking up during the night, waking up too early, and feeling unrested), appetite (eating enough food, being hungry but not eating, not eating for a whole day, and losing weight in the last 12 months) and loss of interest (lost interest in hobbies and work), low mood (trouble in concentration, feeling tired, feeling satisfied, feeling alone, bothered by things, hopeful about the future, and feeling happy), difficulty in daily life activities (eating, preparing meals, shopping groceries, making phone calls, taking medications, working around the house, managing money, paying bills, and picking up a coin from the table), and orientation (day, month, year, village/town/city, landmarks, and district name). These questions were asked as “yes” or “no”.
Anxiety disorders are characterized by excessive panic and worry and related behavioral disturbances [33]. Anxiety disorder symptoms include restlessness, difficulty in concentration, being easily fatigued, and experiencing sleep issues [34]. To measure the presence of anxiety, variables related to three factors were considered: Sleep disorder, appetite, and loss of interest in daily life activities over the previous two weeks.
Depression differs from regular mood swings. Mood swings may persist for two weeks or more continuously. Depressive symptoms include inability to focus, hopelessness, guilt, disturbed sleep, changes in food or weight, and extreme fatigue or low energy [33]. To measure the presence of depression, variables related to four factors were considered: Sleep disorder, appetite, low mood, and loss of interest in daily life activities over the previous two weeks.
Neurological conditions are behavioral and cognitive problems that develop from childhood and involve severe difficulty learning adaptive behavior and executing specific intellectual, physical, or social functions [33]. To measure the presence of neurological disorder, variables related to three factors were considered: Difficulty in daily life activity, orientation, and loss of interest in daily life activities over the previous two weeks.
Psychotic illnesses lose contact with reality and experience a variety of intense symptoms, including hallucinations (hearing or seeing imaginary things, such as voices) [35]. To measure the presence of psychotic illnesses, variables related to four factors were considered: Sleep disorder, appetite, orientation, and loss of interest in daily life activities over the previous two weeks.
Statistical measures
Data were codified, scored, tabulated, and analyzed using SPSS software, version 26, covering three primary analyses. Initially, it described the sociodemographic characteristics of older workers in both agricultural and professional sectors using frequency and percentage calculations. The second phase identified differences in job characteristics between sectors through descriptive statistics. Lastly, it assessed the odds ratio with a 95% confidence interval of mental disorder symptoms by gender within each sector. An odds ratio represents the odds of an event occurring in the exposed group to the odds of it happening in the unexposed group. Here, agricultural workers were considered an exposed group, and professional sector workers were considered an unexposed group. We compared the odds of the mental health status of agriculture sector workers to those of professional sector workers with significance tested via significance value.
Results
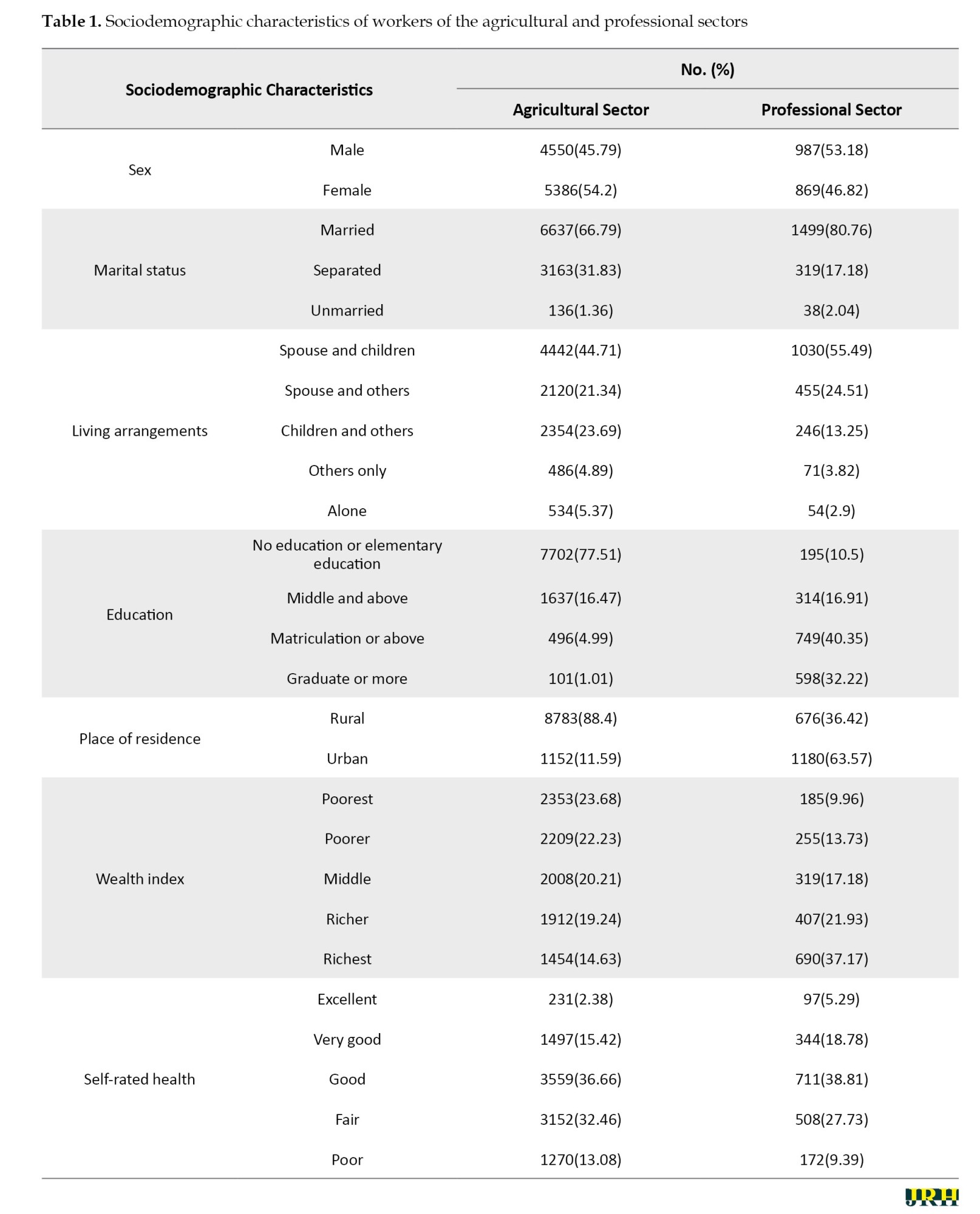
This study was based on the LASI wave-1. Our research examined the comparative mental health status of agricultural and professional workers. Mental health was considered the absence of different mental disorders symptoms. In this study, we categorized the data according to different sociodemographic characteristics: Sex, marital status, living arrangement, education, residence, and wealth index. Table 1 presents the various sociodemographic characteristics of both agricultural and professional workers.
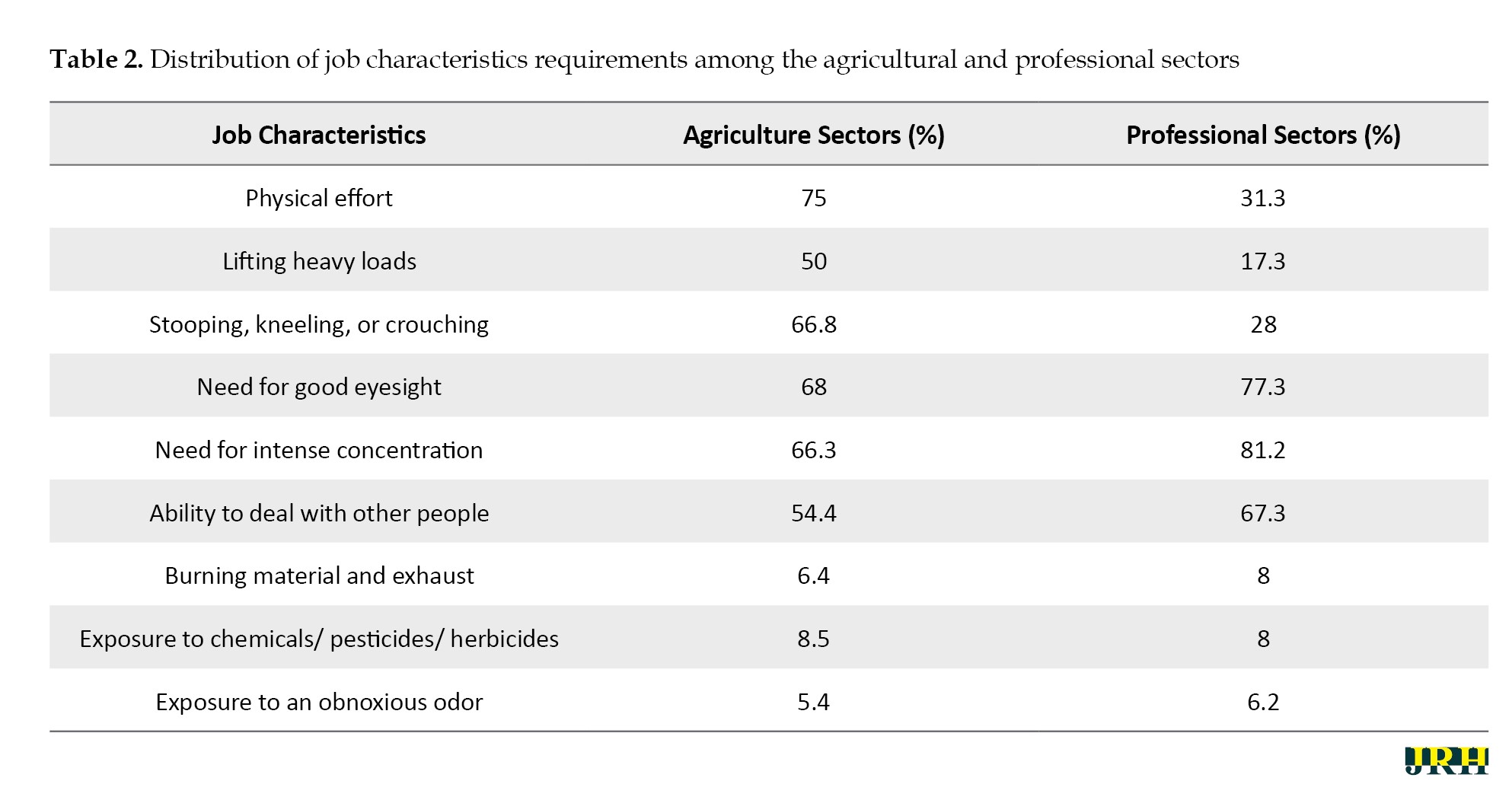
After that, we measured the distribution of job characteristics regarding agricultural and professional workers. Table 2 outlines the job characteristics for both agriculture and professional sector works.
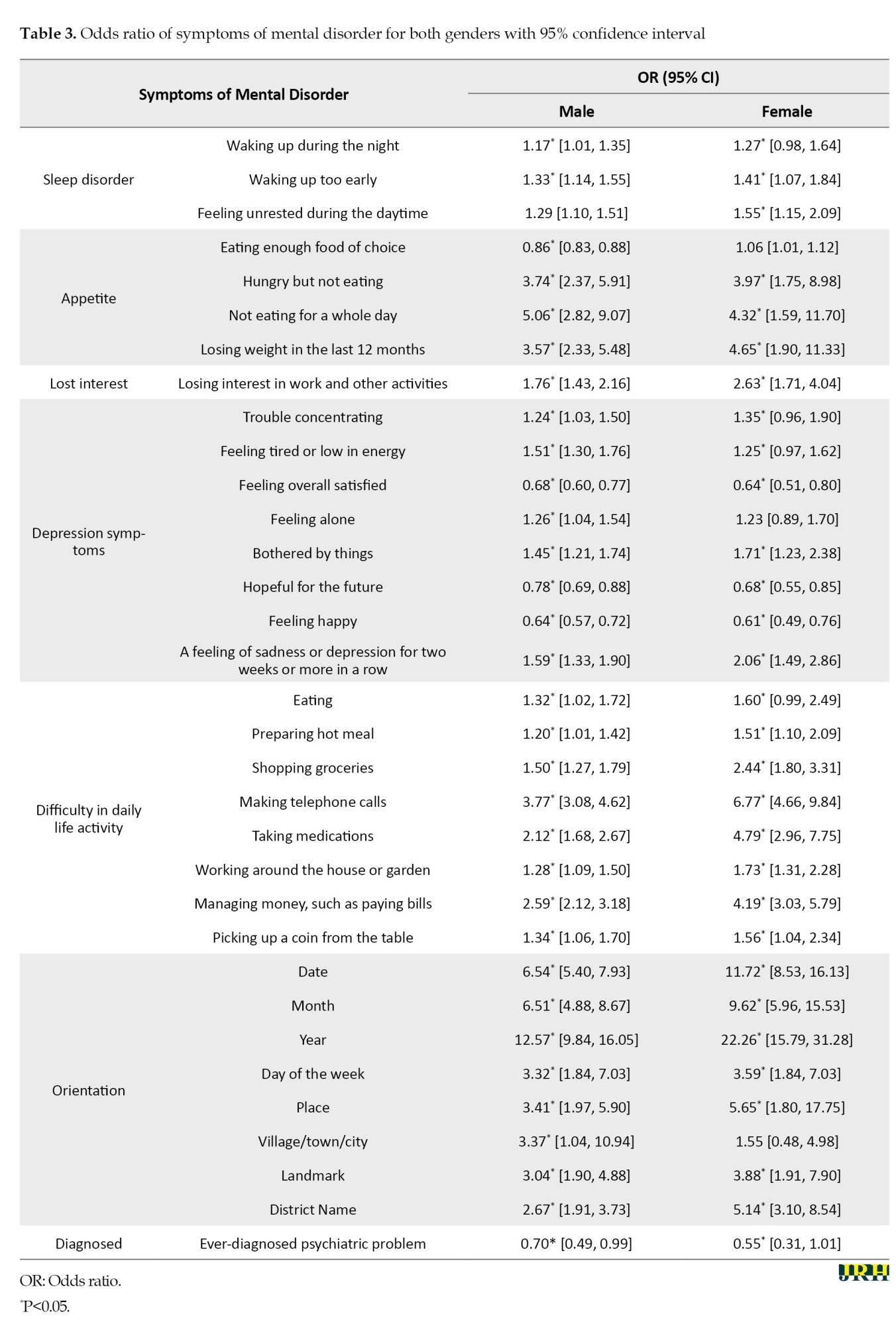
We inferred that agricultural workers encounter challenges related to their respective working environments. To measure mental health in older Indian adults in agricultural and professional sectors, we considered mental disorders, like anxiety, depression, neurological, and psychotic disorders. Table 3 examines the impact of these symptoms by gender and sector.
Demographic characteristics of worker in India
This paper considered only those who worked for at least three months and those aged 60 and above. The findings of this paper suggest that 48.5% of people in the agriculture sector above 60 were still working. However, in the professional sector, only 16% of people over 60 still were working in India. Sociodemographic characteristics included sex, marital status, living arrangement, education, residence, and wealth index.
Table 1 depicts the sociodemographic profile of the Indian elderly agricultural and professional sector workers. A total of 9936 were included in this study. The overall female participation (54.2%) in the agricultural sector was more than male participation (45.79%). Similarly, in the professional sector, male participation (53.18%) was higher than female participation (46.82%). A significant educational gap existed between the agricultural and professional sectors. Also, 77.51% of agricultural workers had minimal or no schooling, compared to 10.5% in the professional sector.
Moreover, only 1.01% of those in agriculture had a college degree compared to 33.22% of professionals. We found a residency gap: 88.4% of agriculture workers were living in rural areas, compared to 36.42% of professional sector workers. Regarding the wealth index, agricultural workers belonged to households with lower living standards. Specifically, 23.68% of agricultural workers were among the poorest, while only 9.96% of professional sector workers were in the same category. The self-rated health of professional workers was better than that of agriculture sector workers, but there was no significant difference in other groups.
The work characteristics of the agriculture and professional sectors were distinct. Table 2 illustrates the fundamental distinction between these sectors. While the agricultural sector demands physical effort, such as lifting heavy loads and stooping, kneeling, or crouching, the professional sector requires different skills, such as good eyesight, concentration, and effective communication.
Table 3 shows the odds ratio of agricultural sector workers by professional sector workers with a 95% confidence interval of symptoms of mental disorder for both genders.
All three symptoms of sleep disorders showed a statistically significant difference in workers of the agricultural and professional sectors, and agricultural workers were more likely to face sleep disorders compared to professional workers. Furthermore, the odds ratio for men feeling unrest during the daytime was 1.29 (95% CI, 1.10%, 1.51%), while for women, it was significantly higher at 1.55 (95% CI, 1.15%, 2.09%) compared to professional sector workers. Furthermore, we compared the higher appetite-related issues among farmers with those of professional sector workers. The results showed that the likelihood of feeling hungry but not eating was significantly higher, with odds ratios of 3.74 (95% CI, 2.37%, 5.91%) for men and 3.97 (95% CI, 1.75%, 8.98%) for women, indicating a significant disparity when compared to workers of professional sectors. Agricultural sector workers were more likely to experience symptoms of depression than workers in professional sectors. This disparity is reflected in the odds ratios for various symptoms of depression. Regarding the experience of sadness or depression for two weeks or more consecutively, male workers in the agricultural sector had an odds ratio of 1.59 (95% CI, 1.33%, 1.9%) compared to their professional counterparts, while females had a significantly higher odds ratio of 2.06 (95% CI, 1.49%, 2.86%).
Agricultural workers were more likely to face difficulties in their daily activities than their professional counterparts. According to the data, agricultural workers were significantly more likely to encounter trouble performing essential tasks. Specifically, the odds ratio for challenges in activities, such as making telephone calls was 3.77 (95% CI, 3.08%, 4.62%) for males and 6.77 (95% CI, 4.66%, 9.84%) for females. For taking medications, the odds ratio was 2.12 (95% CI, 1.68%, 2.67%) for males and 4.79 (95% CI, 2.96%, 7.75%) for females.
This study illustrates that agricultural sector workers have a higher likelihood of experiencing memory struggles compared to professional workers, evidenced by an odds ratio two times higher for remembering things, with this disparity observed in both males and females. We found differences in the prevalence of sleep disorders, appetite issues, loss of interest, depression symptoms, difficulty with daily life activities, and orientation difficulties, with agricultural workers being more vulnerable than workers in the professional sector.
Discussion
This study supports the hypothesis that occupation type and work environment affect older adults’ mental health in India. The findings suggest that elderly agricultural workers are more susceptible than professional workers in education, income, and health. Additionally, the situation is devastating for elderly females compared to their male peers in both sectors. Also, this research highlights that most agricultural workers reside in rural areas, where health infrastructure and services are poor. Consequently, mental health problems are often overlooked, especially in rural and agricultural communities, suggesting an increased risk of mental health challenges among these groups [36]. Literature has identified issues related to mental health problems among agricultural and professional sector workers [5]. However, the same has not been discussed in much detail in India. This study investigated the mental well-being of elderly professionals and agricultural laborers and compared the mental health outcomes between both genders. We revealed that for different symptoms of mental disorders, such as sleep disorders, appetite issues, loss of interest in daily life activities, low mood, difficulty in daily life activities, and memory problems, agricultural workers are more vulnerable than professional sector workers. Also, farmers reported greater incidence of anxiety and depression symptoms than other occupations due to long working hours, much physical work, and low wages [13]. Furthermore, the involvement of rural older adults in non-agricultural activity improves their mental health significantly [37].
Along with comparing the mental health of agricultural and professional workers, there are gender-based differences in the prevalence of different symptoms of mental disorders, with females having higher chances of experiencing sleep disorders and appetite-related issues. Research indicates that most agricultural workers are compelled to take these jobs due to a lack of alternatives, facing long hours and limited personal development opportunities [38]. Furthermore, the study shows that agricultural workers, particularly females, are twice as likely to lose interest in their work than those in professional sectors. Additionally, agricultural workers struggle more with daily tasks and memory retention than their professional counterparts. Despite facing greater difficulties, agricultural workers had fewer diagnosed cases than professional workers, which can be attributed to a lack of literacy, financial resources, and limited health infrastructure. Various factors contribute to gender differences in mental health in the workplace [39]. These include unequal distribution of work and employment conditions, discrimination based on gender, and assault [40, 41]. This article establishes an adverse relationship between agricultural working conditions and mental health.
It is essential to acknowledge that the current study has some limitations. This study was based on self-reported symptoms of mental disorders, and self-reported health may be biased, given that an individual’s subjective health evaluation influences it. Also, this study compared only older agricultural workers with professional sector workers; future research can extend this work by comparing the mental health status of agricultural workers with other sector workers. Despite these limitations, the present study has some strengths. We analyzed nationally representative data of workers in India, which means that the findings can be considered reliable and generalizable. Moreover, the study found striking differences in the symptoms of mental health among male and female workers of both sectors, which highlights the need for gender-specific interventions to improve mental health in the workplace.
This study examined the impact of occupation type on mental health among elderly agricultural and professional workers in India, highlighting a stronger prevalence of mental disorders among agricultural workers, particularly women who juggle household and agricultural responsibilities. This study assists policymakers in developing policies addressing the work environment and mental health. It suggests that improving work conditions, especially in agriculture, through enhanced labor laws, protections against workplace discrimination and violence, education, financial literacy, and social security schemes could benefit mental health and productivity. The study further recommends the establishment of geriatric mental health units and community programs to boost social interaction, the expansion of pension schemes for financial stability, and the promotion of part-time employment to enhance the mental well-being and quality of life for India’s elderly.
Conclusion
This study sheds light on the mental health of older adults in India in the professional and agricultural sectors, considering gender. The study found that work-related stress and poor working conditions are major contributors to workplace stress and mental health issues among workers. Our analysis showed that workers in the agricultural sector are more susceptible to exhibiting symptoms of poor mental health compared to workers in the professional sector. Additionally, this study revealed that older women face more severe challenges in both sectors compared to men, with mental health issues being more prevalent among them due to factors, like long working hours, physical labor, low wages, and poor working conditions in agriculture. It also points out the need for government intervention to protect farmers, especially women, who are more affected by these challenges, highlighting the role of unequal work distribution, employment conditions, and gender discrimination in exacerbating mental health problems. This study highlights the persistent need for enhanced awareness and strategies to address mental health problems among elderly workers in both the professional and agricultural sectors across genders. We urge the government and policymakers to prioritize workplace mental health and implement preventative measures to ensure employees’ healthy and safe working environments.
Ethical Considerations
Compliance with ethical guidelines
For this study, we used LASI data without being involved in its collection, which does not require ethical approval or consent. The data are accessible upon request. Survey agencies obtained respondent consent and adhered to protocols, with the Indian Council of Medical Research (ICMR), New Delhi, India providing ethical guidelines.
Funding
This research didn’t receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Sunit Kumar; Data analysis and interpretation: Anjali Mishra, and Ashutosh Gaurav; Writing the original draft: Anjali Mishra, and Ashutosh Gaurav; Review, editing and final approval: All auhors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to the LASI investigators and all the respondents for their tremendous efforts in data collection.
References
The relevance of the workplace in mental well-being is increasing. We spend most of our time at the workplace; hence, the work environment is essential for mental well-being. Work can provide economic fulfillment and satisfaction, but work-related stress may also cause mental health issues [1]. Prior research indicates that poor working environments can cause workplace-related stress [2], psychological distress [3] and other mental health issues [4]. Work productivity is essential to physical and mental health [5]. Work stress negatively impacts mental health, and different occupations have distinct work conditions. Farmers are frequently subjected to unfavorable working conditions, including lengthy working hours, monotonous labor, and a hazardous work environment [6]. Similarly, in the professional sector, mental health issues are caused by inflexible timetables and obligatory overtime hours [7]. Moreover, healthcare professionals frequently encounter mental health problems [7-9]. These effects can vary depending on the gender of the individual. Female doctors were 32% more likely than male colleagues to suffer from depression [10]. Male educators are less inclined to seek social assistance, reflecting significant gender disparities in seeking help for mental disorders [11, 12]. Farmers reported higher rates of depression and anxiety compared to other occupations [13, 14]. However, not all studies match that the mental health of farmers is inferior to others [15].
The Indian population continues to grow and change [16]. According to the 2011 census, 9% of India’s population is 60 or older [17]. Aging is linked to a decline in functioning and the development of several disabilities, such as mental, physical, social, and economic restrictions [18, 19]. Agriculture, which serves as the foundation of the Indian economy, plays a pivotal role in the country’s socio-economic domain [20]. Growth in agriculture is believed to be essential in India, with over 70% of total workers dependent on this sector [21]. The physical strength needed for agricultural productivity drops around middle age, necessitating more labor for the same amount of yield. On average, older workers are less productive than younger workers, and labor force aging has a slight negative impact on productivity [22]. However, older farmers’ expertise improves input combinations, making a unit of effort more efficacious [23]. Future climate change will render farmers’ jobs harder [24]. The literature review identified four primary factors that significantly impact farmers’ mental well-being: Financial challenges, climate variabilities, and compromised physical health due to past incidents. Women are especially vulnerable to these challenges [14].
The agricultural sector in India is in the midst of a crisis, including diminishing land sizes, inflation, rising production expenses, etc. [25]. The National Commission of Farmers (NCF, 2005) [26] indicates that as the number of males abandoning rural areas increases, more women are taking on agricultural responsibilities [27]. Despite their hard work, women in agriculture are often undervalued. They perform physically demanding tasks in agriculture and household chores, yet men reap the benefits of their labor [27]. Male dominance over women exists in the Indian sociocultural setting [27]. Women are generally overrepresented in unpaid, seasonal, and part-time labor [27]. Such inequalities have resulted in higher psychological distress levels among female farmers than their male counterparts [28, 29]. We must acknowledge gender-based disparities and strive toward a more equitable future.
Previous research suggests that occupation and work environment influence mental health [1-4]. However, many studies fall short of providing a thorough knowledge of older workers’ mental health, particularly when gender is considered. In most countries, men’s duties in agricultural operations must be directed and unambiguous. Nevertheless, women’s contributions to agriculture are seldom appreciated. Job strain has been found to affect life stress among women [30]. Furthermore, earlier research did not focus on agricultural workers. However, India is an agriculture-based country; thus, it is critical to emphasize agricultural workers’ mental health. To comprehensively evaluate, we will compare the mental health of agricultural workers to other professionals. This study aimed to understand better the links between occupation, work environment, and mental health in older individuals of both genders considering gender differences. The present study revolves around the following (Figure 1) conceptual model.
Methods
This study utilized the longitudinal ageing study in India (LASI), a national longitudinal study on aging and health encompassing all Indian states and UTs except Sikkim. It is supervised by the Indian government, coordinated by the International Institute for Population Sciences (IIPS), Mumbai, and partners with the Harvard T.H. Chan School of Public Health and the University of Southern California. It is financially supported by various national and international bodies, including the national program for health care of older people and the United Nations Population Fund. LASI is the world’s largest and India’s only study of its kind, offering crucial insights into the economic dimensions of aging in India.
Our study examined 31,464 individuals aged 60 and above, drawn from the initial LASI wave of 72,250 individuals, focused on those with at least three months of work experience. The sample included 9936 in agriculture, 1856 in professional sectors (including higher education, accountancy, and health), and 11792 working in other sectors (mining, construction, manufacturing, wholesale and retail trade, and transportation). The aim was to investigate mental health disparities between workers in agriculture and professional fields, noting a gender divide with 7149 males (56.95% in agriculture) and 4643 females (92.14% in agriculture). This comparison seeks to shed light on sector-specific mental health challenges among older employees.
Outcome variable
The study considered mental health as the outcome variable. According to the World Health Organization (WHO), “mental health is not just the absence of mental disorders. It is a state of mental well-being that empowers individuals to handle life’s challenges, learn efficiently, work productively, and contribute to society” [31]. To measure mental health, we relied on the international classification of diseases (ICD-10), a globally recognized standard for diagnosing mental disorders [32], which focuses on four key indicators of mental disorders: Anxiety, depression, neurological, and psychotic disorders. In LASI, self-reported questions related to the symptoms of mental disorder were asked. These questions include sleep disorder (waking up during the night, waking up too early, and feeling unrested), appetite (eating enough food, being hungry but not eating, not eating for a whole day, and losing weight in the last 12 months) and loss of interest (lost interest in hobbies and work), low mood (trouble in concentration, feeling tired, feeling satisfied, feeling alone, bothered by things, hopeful about the future, and feeling happy), difficulty in daily life activities (eating, preparing meals, shopping groceries, making phone calls, taking medications, working around the house, managing money, paying bills, and picking up a coin from the table), and orientation (day, month, year, village/town/city, landmarks, and district name). These questions were asked as “yes” or “no”.
Anxiety disorders are characterized by excessive panic and worry and related behavioral disturbances [33]. Anxiety disorder symptoms include restlessness, difficulty in concentration, being easily fatigued, and experiencing sleep issues [34]. To measure the presence of anxiety, variables related to three factors were considered: Sleep disorder, appetite, and loss of interest in daily life activities over the previous two weeks.
Depression differs from regular mood swings. Mood swings may persist for two weeks or more continuously. Depressive symptoms include inability to focus, hopelessness, guilt, disturbed sleep, changes in food or weight, and extreme fatigue or low energy [33]. To measure the presence of depression, variables related to four factors were considered: Sleep disorder, appetite, low mood, and loss of interest in daily life activities over the previous two weeks.
Neurological conditions are behavioral and cognitive problems that develop from childhood and involve severe difficulty learning adaptive behavior and executing specific intellectual, physical, or social functions [33]. To measure the presence of neurological disorder, variables related to three factors were considered: Difficulty in daily life activity, orientation, and loss of interest in daily life activities over the previous two weeks.
Psychotic illnesses lose contact with reality and experience a variety of intense symptoms, including hallucinations (hearing or seeing imaginary things, such as voices) [35]. To measure the presence of psychotic illnesses, variables related to four factors were considered: Sleep disorder, appetite, orientation, and loss of interest in daily life activities over the previous two weeks.
Statistical measures
Data were codified, scored, tabulated, and analyzed using SPSS software, version 26, covering three primary analyses. Initially, it described the sociodemographic characteristics of older workers in both agricultural and professional sectors using frequency and percentage calculations. The second phase identified differences in job characteristics between sectors through descriptive statistics. Lastly, it assessed the odds ratio with a 95% confidence interval of mental disorder symptoms by gender within each sector. An odds ratio represents the odds of an event occurring in the exposed group to the odds of it happening in the unexposed group. Here, agricultural workers were considered an exposed group, and professional sector workers were considered an unexposed group. We compared the odds of the mental health status of agriculture sector workers to those of professional sector workers with significance tested via significance value.
Results
This study was based on the LASI wave-1. Our research examined the comparative mental health status of agricultural and professional workers. Mental health was considered the absence of different mental disorders symptoms. In this study, we categorized the data according to different sociodemographic characteristics: Sex, marital status, living arrangement, education, residence, and wealth index. Table 1 presents the various sociodemographic characteristics of both agricultural and professional workers.
After that, we measured the distribution of job characteristics regarding agricultural and professional workers. Table 2 outlines the job characteristics for both agriculture and professional sector works.
We inferred that agricultural workers encounter challenges related to their respective working environments. To measure mental health in older Indian adults in agricultural and professional sectors, we considered mental disorders, like anxiety, depression, neurological, and psychotic disorders. Table 3 examines the impact of these symptoms by gender and sector.
Demographic characteristics of worker in India
This paper considered only those who worked for at least three months and those aged 60 and above. The findings of this paper suggest that 48.5% of people in the agriculture sector above 60 were still working. However, in the professional sector, only 16% of people over 60 still were working in India. Sociodemographic characteristics included sex, marital status, living arrangement, education, residence, and wealth index.
Table 1 depicts the sociodemographic profile of the Indian elderly agricultural and professional sector workers. A total of 9936 were included in this study. The overall female participation (54.2%) in the agricultural sector was more than male participation (45.79%). Similarly, in the professional sector, male participation (53.18%) was higher than female participation (46.82%). A significant educational gap existed between the agricultural and professional sectors. Also, 77.51% of agricultural workers had minimal or no schooling, compared to 10.5% in the professional sector.
Moreover, only 1.01% of those in agriculture had a college degree compared to 33.22% of professionals. We found a residency gap: 88.4% of agriculture workers were living in rural areas, compared to 36.42% of professional sector workers. Regarding the wealth index, agricultural workers belonged to households with lower living standards. Specifically, 23.68% of agricultural workers were among the poorest, while only 9.96% of professional sector workers were in the same category. The self-rated health of professional workers was better than that of agriculture sector workers, but there was no significant difference in other groups.
The work characteristics of the agriculture and professional sectors were distinct. Table 2 illustrates the fundamental distinction between these sectors. While the agricultural sector demands physical effort, such as lifting heavy loads and stooping, kneeling, or crouching, the professional sector requires different skills, such as good eyesight, concentration, and effective communication.
Table 3 shows the odds ratio of agricultural sector workers by professional sector workers with a 95% confidence interval of symptoms of mental disorder for both genders.
All three symptoms of sleep disorders showed a statistically significant difference in workers of the agricultural and professional sectors, and agricultural workers were more likely to face sleep disorders compared to professional workers. Furthermore, the odds ratio for men feeling unrest during the daytime was 1.29 (95% CI, 1.10%, 1.51%), while for women, it was significantly higher at 1.55 (95% CI, 1.15%, 2.09%) compared to professional sector workers. Furthermore, we compared the higher appetite-related issues among farmers with those of professional sector workers. The results showed that the likelihood of feeling hungry but not eating was significantly higher, with odds ratios of 3.74 (95% CI, 2.37%, 5.91%) for men and 3.97 (95% CI, 1.75%, 8.98%) for women, indicating a significant disparity when compared to workers of professional sectors. Agricultural sector workers were more likely to experience symptoms of depression than workers in professional sectors. This disparity is reflected in the odds ratios for various symptoms of depression. Regarding the experience of sadness or depression for two weeks or more consecutively, male workers in the agricultural sector had an odds ratio of 1.59 (95% CI, 1.33%, 1.9%) compared to their professional counterparts, while females had a significantly higher odds ratio of 2.06 (95% CI, 1.49%, 2.86%).
Agricultural workers were more likely to face difficulties in their daily activities than their professional counterparts. According to the data, agricultural workers were significantly more likely to encounter trouble performing essential tasks. Specifically, the odds ratio for challenges in activities, such as making telephone calls was 3.77 (95% CI, 3.08%, 4.62%) for males and 6.77 (95% CI, 4.66%, 9.84%) for females. For taking medications, the odds ratio was 2.12 (95% CI, 1.68%, 2.67%) for males and 4.79 (95% CI, 2.96%, 7.75%) for females.
This study illustrates that agricultural sector workers have a higher likelihood of experiencing memory struggles compared to professional workers, evidenced by an odds ratio two times higher for remembering things, with this disparity observed in both males and females. We found differences in the prevalence of sleep disorders, appetite issues, loss of interest, depression symptoms, difficulty with daily life activities, and orientation difficulties, with agricultural workers being more vulnerable than workers in the professional sector.
Discussion
This study supports the hypothesis that occupation type and work environment affect older adults’ mental health in India. The findings suggest that elderly agricultural workers are more susceptible than professional workers in education, income, and health. Additionally, the situation is devastating for elderly females compared to their male peers in both sectors. Also, this research highlights that most agricultural workers reside in rural areas, where health infrastructure and services are poor. Consequently, mental health problems are often overlooked, especially in rural and agricultural communities, suggesting an increased risk of mental health challenges among these groups [36]. Literature has identified issues related to mental health problems among agricultural and professional sector workers [5]. However, the same has not been discussed in much detail in India. This study investigated the mental well-being of elderly professionals and agricultural laborers and compared the mental health outcomes between both genders. We revealed that for different symptoms of mental disorders, such as sleep disorders, appetite issues, loss of interest in daily life activities, low mood, difficulty in daily life activities, and memory problems, agricultural workers are more vulnerable than professional sector workers. Also, farmers reported greater incidence of anxiety and depression symptoms than other occupations due to long working hours, much physical work, and low wages [13]. Furthermore, the involvement of rural older adults in non-agricultural activity improves their mental health significantly [37].
Along with comparing the mental health of agricultural and professional workers, there are gender-based differences in the prevalence of different symptoms of mental disorders, with females having higher chances of experiencing sleep disorders and appetite-related issues. Research indicates that most agricultural workers are compelled to take these jobs due to a lack of alternatives, facing long hours and limited personal development opportunities [38]. Furthermore, the study shows that agricultural workers, particularly females, are twice as likely to lose interest in their work than those in professional sectors. Additionally, agricultural workers struggle more with daily tasks and memory retention than their professional counterparts. Despite facing greater difficulties, agricultural workers had fewer diagnosed cases than professional workers, which can be attributed to a lack of literacy, financial resources, and limited health infrastructure. Various factors contribute to gender differences in mental health in the workplace [39]. These include unequal distribution of work and employment conditions, discrimination based on gender, and assault [40, 41]. This article establishes an adverse relationship between agricultural working conditions and mental health.
It is essential to acknowledge that the current study has some limitations. This study was based on self-reported symptoms of mental disorders, and self-reported health may be biased, given that an individual’s subjective health evaluation influences it. Also, this study compared only older agricultural workers with professional sector workers; future research can extend this work by comparing the mental health status of agricultural workers with other sector workers. Despite these limitations, the present study has some strengths. We analyzed nationally representative data of workers in India, which means that the findings can be considered reliable and generalizable. Moreover, the study found striking differences in the symptoms of mental health among male and female workers of both sectors, which highlights the need for gender-specific interventions to improve mental health in the workplace.
This study examined the impact of occupation type on mental health among elderly agricultural and professional workers in India, highlighting a stronger prevalence of mental disorders among agricultural workers, particularly women who juggle household and agricultural responsibilities. This study assists policymakers in developing policies addressing the work environment and mental health. It suggests that improving work conditions, especially in agriculture, through enhanced labor laws, protections against workplace discrimination and violence, education, financial literacy, and social security schemes could benefit mental health and productivity. The study further recommends the establishment of geriatric mental health units and community programs to boost social interaction, the expansion of pension schemes for financial stability, and the promotion of part-time employment to enhance the mental well-being and quality of life for India’s elderly.
Conclusion
This study sheds light on the mental health of older adults in India in the professional and agricultural sectors, considering gender. The study found that work-related stress and poor working conditions are major contributors to workplace stress and mental health issues among workers. Our analysis showed that workers in the agricultural sector are more susceptible to exhibiting symptoms of poor mental health compared to workers in the professional sector. Additionally, this study revealed that older women face more severe challenges in both sectors compared to men, with mental health issues being more prevalent among them due to factors, like long working hours, physical labor, low wages, and poor working conditions in agriculture. It also points out the need for government intervention to protect farmers, especially women, who are more affected by these challenges, highlighting the role of unequal work distribution, employment conditions, and gender discrimination in exacerbating mental health problems. This study highlights the persistent need for enhanced awareness and strategies to address mental health problems among elderly workers in both the professional and agricultural sectors across genders. We urge the government and policymakers to prioritize workplace mental health and implement preventative measures to ensure employees’ healthy and safe working environments.
Ethical Considerations
Compliance with ethical guidelines
For this study, we used LASI data without being involved in its collection, which does not require ethical approval or consent. The data are accessible upon request. Survey agencies obtained respondent consent and adhered to protocols, with the Indian Council of Medical Research (ICMR), New Delhi, India providing ethical guidelines.
Funding
This research didn’t receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Sunit Kumar; Data analysis and interpretation: Anjali Mishra, and Ashutosh Gaurav; Writing the original draft: Anjali Mishra, and Ashutosh Gaurav; Review, editing and final approval: All auhors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to the LASI investigators and all the respondents for their tremendous efforts in data collection.
References
- The Lancet Global Health. Mental health matters. The Lancet. Global Health. 2020; 8(11):e1352. [DOI:10.1016/S2214-109X(20)30432-0] [PMID]
- Bhui K, Dinos S, Galant-Miecznikowska M, de Jongh B, Stansfeld S. Perceptions of work stress causes and effective interventions in employees working in public, private and non-governmental organisations: A qualitative study. BJPsych Bulletin. 2016; 40(6):318-25. [DOI:10.1192/pb.bp.115.050823] [PMID] [PMCID]
- Cazabat S, Barthe B, Cascino N. Work load and job stress: Two facets of the same situation? Exploratory study in a gerontology department. Perspectives interdisciplinaires sur le travail et la santé. 2008; 1-10. [DOI:10.4000/pistes.2165]
- Chandola T. Stress at work. London: British Academy Policy Centre; 2010. [Link]
- Chopra P. Mental health and the workplace: Issues for developing countries. International journal of Mental Health Systems. 2009; 3(1):4. [DOI:10.1186/1752-4458-3-4] [PMID] [PMCID]
- Parent-Thirion A, Fernández-Macías E, Hurley J, Vermeylen G. Fourth European working conditions survey. County Dublin: European Foundation for the Improvement of Living and Working Conditions; 2007. [Link]
- Ahmad W, Taggart F, Shafique MS, Muzafar Y, Abidi S, Ghani N, et al. Diet, exercise and mental-wellbeing of healthcare professionals (doctors, dentists and nurses) in Pakistan. PeerJ. 2015; 3:e1250. [DOI:10.7717/peerj.1250] [PMID] [PMCID]
- Galián-Muñoz I, Ruiz-Hernández JA, Llor-Esteban B, López-García C. User violence and nursing staff burnout: the modulating role of job satisfaction. Journal of Interpersonal Violence. 2016; 31(2):302-15. [DOI:10.1177/0886260514555367] [PMID]
- Huri M, Bağış N, Eren H, Umaroğlu M, Orhan K. Association between burnout and depressive symptoms among Turkish dentists. Journal of Dental Sciences. 2016; 11(4):353-9. [DOI:10.1016/j.jds.2016.03.006] [PMID] [PMCID]
- McFadden T, Simon C, Kobeissi B, Gerin-Lajoie C. Physicians' access to primary care: Results from the Canadian Medical Association National Physician Health Survey. Journal Canadien D'ophtalmologie. 2020; 55(3 Suppl 1):27-28. [DOI:10.1016/j.jcjo.2020.03.009] [PMID]
- Ferguson K, Mang. Teacher stress and social support usage. Brock Education Journal. 2017; 26(2):62-86. [DOI:10.26522/brocked.v26i2.606]
- Berg LD, Huijbens EH. Producing anxiety in the neoliberal university. The Canadian Geographer. 2016; 60(2):168-80. [DOI:10.1111/cag.12261]
- Torske MO, Hilt B, Glasscock D, Lundqvist P, Krokstad S. Anxiety and depression symptoms among farmers: The HUNT study, Norway. Journal of Agromedicine. 2016; 21(1):24-33. [DOI:10.1080/1059924X.2015.1106375] [PMID] [PMCID]
- Daghagh Yazd S, Wheeler SA, Zuo A. Key risk factors affecting farmers' mental health: A systematic review. International Journal of Environmental Research and Public Health. 2019; 16(23):4849. [DOI:10.3390/ijerph16234849] [PMID] [PMCID]
- Feng D, Ji L, Xu L. Effect of subjective economic status on psychological distress among farmers and non-farmers of rural China. The Australian Journal of Rural Health. 2015; 23(4):215-20. [DOI:10.1111/ajr.12187] [PMID]
- Kumar S, Pradhan MS, Singh AK. Chronic diseases and their association with disability among the elderly in India. Social Science Spectrum. 2017; 3(1): 27-37. [Link]
- Chandramouli C. Census of India [intrnet]. 2011 [updated 20 January 2025]. Available at: [Link]
- Nooripour R, Ghanbari N, Hosseinian S, Ronzani TM, Hussain AJ, Ilanloo H, et al. Validation of the spiritual well-being scale (SWBS) and its role in predicting hope among Iranian elderly. Ageing International. 2023; 48(2):593-611. [DOI:10.1007/s12126-022-09492-8]
- Goudarzvand-Chegini M, Mirghaderi NS, Emadi F, Soleimani-Farsani S, Nooripour R, Hasani-Abharian P, et al. The effectiveness of mindfulness-based compassion-therapy on sleep quality and satisfaction with life in elderly women. International Journal of Behavioral Sciences. 2023; 16(4):261-7. [DOI: 10.30491/IJBS.2023.363030.1856]
- Borthakur A, Singh P. History of agricultural research in India. Current Science. 2013; 105(5):587-93. [Link]
- Padhi K. Agricultural labour in India: A close look. Orissa Review. 2007; 23-8. [DOI:10.5555/20133370506]
- Tang J, MacLeod C. Labour force ageing and productivity performance in Canada. Canadian Journal of Economics. 2006; 39(2):582-603. [DOI:10.1111/j.0008-4085.2006.00361.x]
- Guo G, Wen Q, Zhu J. The impact of aging agricultural labor population on farmland output: From the perspective of farmer preferences. Mathematical problems in Engineering. 2015; 1-7. [DOI:10.1155/2015/730618]
- Kearney GD, Rafferty AP, Hendricks LR, Allen DL, Tutor-Marcom R. A cross-sectional study of stressors among farmers in Eastern North Carolina. North Carolina Medical Journal. 2014; 75(6):384-92. [DOI:10.18043/ncm.75.6.384] [PMID]
- Mishra S. Suicide mortality rates across states of India, 1975-2001: A statistical note. Economic and Political Weekly. 2006; 41(16):1566-9. [DOI: 10.2307/4418116]
- Pattnaik I, Lahiri-Dutt K, Lockie S, Pritchard B. The feminization of agriculture or the feminization of agrarian distress? Tracking the trajectory of women in agriculture in India. Journal of the Asia Pacific Economy. 2020; 23(1):138-55. [DOI:10.1080/13547860.2017.1394569]
- Gowda ND. An analysis on role of women in agriculture and rural development in the Indian context. International Journal of Legal Research and Studies. 2018; 3(1):127-33. [Link]
- Kallioniemi MK, Simola AJ, Kymäläinen HR, Vesala HT, Louhelainen JK. Mental symptoms among Finnish farm entrepreneurs. Annals of Agricultural and Environmental Medicine. 2009; 16(1):159-68. [PMID]
- Thomas HV, Lewis G, Thomas DR, Salmon RL, Chalmers RM, Coleman TJ, et al. Mental health of British farmers. Occupational and Environmental Medicine. 2003; 60(3):181-5. [DOI:10.1136/oem.60.3.181] [PMID] [PMCID]
- Padkapayeva K, Gilbert-Ouimet M, Bielecky A, Ibrahim S, Mustard C, Brisson C, et al. Gender/sex differences in the relationship between psychosocial work exposures and work and life stress. Annals of Work Exposures and Health. 2018; 62(4):416-25. [DOI:10.1093/annweh/wxy014] [PMID] [PMCID]
- WHO. Mental health. Geneva: World Health Organization; 2024. [Link]
- Gaebel W, Stricker J, Kerst A. Changes from ICD-10 to ICD-11 and future directions in psychiatric classification. Dialogues in Clinical Neuroscience. 2020; 22(1):7-15. [DOI:10.31887/DCNS.2020.22.1]
- WHO. Depressive disorder (depression). Geneva: World Health Organization; 2023. [Link]
- National Institute of Mental Health (NIH). Anxiety disorders. Bethesd:NIH; 2023. [Link]
- Substance Abuse and Mental Health Services Administration (SAMHSA). Schizophrenia [internet]. 2023 [Updated 24 April 2023]. Available from; [Link]
- Bomble P, Lhungdim. Mental health status of Farmers in Maharashtra, India: A study from farmer suicide prone area of Vidarbha region. Clinical Epidemiology and Global Health. 2020; 8(3):684-8. [DOI:10.1016/j.cegh.2020.01.002]
- Jia P, Zhuang J, Vaca Lucero AM, Osei CD, Li J. Does participation in local non-agricultural employment improve the mental health of elderly adults in rural areas? Evidence from China. Frontiers in Public Health. 2021; 9:746580. [DOI:10.3389/fpubh.2021.746580] [PMID] [PMCID]
- Agarwal B, Agrawal A. Do farmers really like farming? Indian farmers in transition. Oxford Development Studies. 2017; 45(4):460-78. [DOI:10.1080/13600818.2017.1283010]
- Harnois CE, Bastos JL. Discrimination, harassment, and gendered health inequalities: Do perceptions of workplace mistreatment contribute to the gender gap in self-reported health? Journal of Health and Social Behavior. 2018; 59(2):283-99. [DOI:10.1177/0022146518767407] [PMID]
- Attell BK, Kummerow Brown K, Treiber LA. Workplace bullying, perceived job stressors, and psychological distress: Gender and race differences in the stress process.Social Science Research. 2017; 65:210-21. [DOI:10.1016/j.ssresearch.2017.02.001] [PMID]
- Campos-Serna J, Ronda-Pérez E, Artazcoz L, Moen BE, Benavides FG. Gender inequalities in occupational health related to the unequal distribution of working and employment conditions: A systematic review. International Journal for Equity in Health. 2013; 12:57. [DOI:10.1186/1475-9276-12-57] [PMID] [PMCID]
Type of Study: Orginal Article |
Subject:
● Psychosocial Health
Received: 2024/05/10 | Accepted: 2024/07/1 | Published: 2025/01/1
Received: 2024/05/10 | Accepted: 2024/07/1 | Published: 2025/01/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
