

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 117-128 |
Back to browse issues page



Ethics code: Pharm.B/44/20-21
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hawlader M B, Islam M S, Prattay K M R, Sarkar M R, Raihan S Z, Muhit M A et al . Prescription and Drug Use Patterns in Non- COVID Ambulatory Patients in Bangladesh during COVID-19 pandemic. J Research Health 2026; 16 (2) :117-128
URL: http://jrh.gmu.ac.ir/article-1-2804-en.html
URL: http://jrh.gmu.ac.ir/article-1-2804-en.html
Md. Bappy Hawlader1 

 , Md. Saiful Islam2 , Kazi Milenur Rahman Prattay3 , Md. Raihan Sarkar1 , Sheikh Zahir Raihan4 , Md. Abdul Muhit4 , Nahid Sharmin5
, Md. Saiful Islam2 , Kazi Milenur Rahman Prattay3 , Md. Raihan Sarkar1 , Sheikh Zahir Raihan4 , Md. Abdul Muhit4 , Nahid Sharmin5
, Md. Saiful Islam2 , Kazi Milenur Rahman Prattay3 , Md. Raihan Sarkar1 , Sheikh Zahir Raihan4 , Md. Abdul Muhit4 , Nahid Sharmin5
1- Department of Pharmaceutical Technology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh.
2- Department of Pharmaceutical Chemistry, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh. & Pharmaceutical Sciences Research Division, BCSIR Dhaka Laboratories, Bangladesh Council of Scientific and Industrial Research (BCSIR), Dhaka-1205, Bangladesh.
3- Department of Clinical Pharmacy and Pharmacology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh. & Department of Pharmacy, School of Pharmacy, BRAC University, Dhaka-1212, Bangladesh.
4- Department of Clinical Pharmacy and Pharmacology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh.
5- Department of Pharmaceutical Technology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh. ,nahidsharmin@du.ac.bd
2- Department of Pharmaceutical Chemistry, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh. & Pharmaceutical Sciences Research Division, BCSIR Dhaka Laboratories, Bangladesh Council of Scientific and Industrial Research (BCSIR), Dhaka-1205, Bangladesh.
3- Department of Clinical Pharmacy and Pharmacology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh. & Department of Pharmacy, School of Pharmacy, BRAC University, Dhaka-1212, Bangladesh.
4- Department of Clinical Pharmacy and Pharmacology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh.
5- Department of Pharmaceutical Technology, Faculty of Pharmacy, University of Dhaka, Dhaka-1000, Bangladesh. ,
Keywords: WHO prescribing indicators, COVID-19, Tertiary level hospitals, Outpatients, Prescription errors, Bangladesh
Full-Text [PDF 960 kb]
(43 Downloads)
| Abstract (HTML) (384 Views)
Full-Text: (15 Views)
Introduction
Aprescription is a rightfully written instruction of medication given to the pharmacist and patients by a qualified and registered medical professional [1] that provides clinical care and ensures patient safety [2]. Ideally, all prescriptions warrant and should maximize the rational use of drugs. Inappropriate prescription of medications leads to irrational use of drugs, medication errors, lengthened hospitalization, and increased economic burden on patients [3]. Over 50% of all medications are administered, given, or marketed improperly on a global scale, while 50% of the patients do not take their medications as prescribed. Common irrational prescribing practices include polypharmacy, prescribing antimicrobials for nonbacterial infections, unnecessary injections, and deviation from clinical guidelines [4]. In developing countries, about 44%-97% of hospitalized patients are unreasonably prescribed antibiotics [5, 6], which has resulted in a rising rate of antibiotic resistance, posing a global public health concern. The reported 6-37% drug-drug interactions in prescriptions have been attributed to the practice of polypharmacy and lack of proper monitoring of prescriptions [7]. To lessen the intensity of these damages and encourage responsible drug use, World Health Organization (WHO) has established and verified key drug use indicators for prescribing, patient care, and facility-specific investigations, which are increasingly gaining importance in developing countries [8, 9].
Prescription error represents the major form of medication error. Reportedly, at least one mistake occurs in 15% to 21% of all written prescriptions [10]. Nearly 7,000 fatalities are documented each year consequent to medication errors [2]. The majority of these are regarded as errors of commission (incorrectly written information) and omission (crucial missing information) [11].
In developing countries, a large number of drugs are prescribed irrationally, burdening drug availability and the medical sector’s financial resources [4, 12]. Reportedly, most of the prescriptions in Bangladesh contained 3-8 drugs [12, 13], the majority of them were not prescribed by their generic name [12, 14], and the number of antibiotics exceeded the WHO permitted range [12, 14]. Although all the drugs should be prescribed from the essential drugs list, only about 30-46% of them belonged to this list [13, 15]. Moreover, prescription errors are also very common, which include illegible handwriting, wrong or missing dose strength, prescribing incompatible drugs, absence of practitioner’s name, patient information, date, diagnosis, and medication administration instructions for the patients [12, 13, 15, 16]. The persistence of these errors and deviation from WHO standards has encouraged polypharmacy, antibiotic resistance, and drug interactions, highlighting the need for stronger prescription monitoring and regulations [17].
The debilitating effect of the COVID-19 infection was first reported in China in December 2019 and attributed to the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The disease spread rapidly and was declared a global pandemic by the WHO in March 2020 [18]. The scarcity of knowledge regarding severe acute respiratory SARS-CoV-2’s spreadability, severity, and treatment guidelines, along with misleading social media prescriptions, triggered an extensive level of irrational drug prescribing [19]. The severity of COVID-19 was reportedly further enhanced by a number of underlying conditions, including diabetes, hypertension, asthma, and cancer, which also significantly contributed to the development of complex symptoms and the rising mortality rate [20]. To combat the virus, a plethora of medicines were repurposed without adequate clinical data, including paracetamol, leukotriene inhibitors, antibiotics, bronchodilators, angiotensin-converting-enzyme (ACE) inhibitors, antiviral and steroidal drugs, along with multivitamins [21]. Multiple studies were conducted globally to investigate drug use patterns during the pandemic [22-24]. Silva TM et al. reported a decrease in antibiotic prescription [22], while Aboulatta et al. found reduced use of antibiotics, cardiovascular drugs, and opioids [23]. However, another study showed a massive 96% increase in over-the-counter drug sales, particularly vitamins, painkillers, antipyretics, cough and cold preparations, irrespective of age groups and gender [24].
In Bangladesh, the first COVID-19 case was identified on March 8, 2020, and by August 11, 2020, the country had officially reported 263,503 cases, with 3,471 deaths [18]. Several studies assessed prescription patterns in COVID-19 patients in Bangladesh [21, 22]. However, although a few studies have been conducted across the world investigating the irrational use of drugs during the pandemic using WHO prescribing indicators [25-28], no such study focusing on the prescription pattern of the non-COVID outpatients is reported in Bangladesh yet.
Therefore, this cross-sectional study aimed to evaluate the prescribing patterns and errors among non-COVID outpatients based on WHO indicators and to understand healthcare-seeking behavior during the pandemic in tertiary hospitals of Dhaka, Bangladesh. The findings may help determine the impact of COVID-19 on prescribing behavior and provide insights to strengthen prescription monitoring policies for future health emergencies.
Methods
Study design, inclusion criteria
The present study is a hospital-based cross-sectional survey conducted in three tertiary-level hospitals of Dhaka, the capital city of Bangladesh. All three hospitals have facilities to provide both inpatient and outpatient services. Prescriptions were collected from the outpatients visiting various outdoor departments of the hospitals from December 1, 2020 to June 30, 2021 during the COVID-19 pandemic period. Patients who were confirmed to be non-COVID-19 cases were included in this study through simple random sampling to minimize selection bias. COVID-19 status was determined by verbal confirmation of symptom absence for general outpatients, and both verbal confirmation and review of antigen test results (as received via SMS in cell phones) for patients visiting the respiratory outpatient department.
Sampling technique and mode of data collection
This cross-sectional study analyzed the prevalence of different ailments, prescribing patterns, and assessed the WHO-established drug use indicators during the pandemic period. [8] Hence in accordance with the WHO guideline [8], 600 prescriptions were collected from the outpatient’s facilities of the hospitals. Photos of the prescriptions were taken after obtaining patient consent. The data from each prescription was recorded separately, eliminating any prescription from the inpatient unit. Patients’ demographic, clinical, diagnosed conditions, and prescribed drugs information were extracted while ensuring the anonymity and organized using Google Spreadsheets by a single trained reviewer under strict monitoring by the study team members to ensure consistency. This information was further studied to analyze the WHO prescription indicators and prescription errors [8].
Data analysis
Data from Google Spreadsheets were imported into and analyzed using MS Excel 2013 and SPSS software, version 26.0. For normally distributed continuous data, the mean and standard deviation were calculated while categorical data were expressed as proportions. One-way analysis of variance (ANOVA) was used to compare the mean number of drugs prescribed across different age groups, while independent sample t-tests were applied to compare means between male and female patients. Prior to conducting these tests, the assumptions of normality and homogeneity of variance were assessed using the Shapiro-Wilk test and Levene’s test, respectively. A P≤0.05 was considered statistically significant. The only missing data was the age for 8 patients, although all other relevant information was available for these cases. Therefore, for analyses where age was a necessary variable, specifically, while constructing the box plot and the ANOVA test evaluating the mean number of drugs prescribed, these 8 prescriptions we excluded and the analysis was conducted on the remaining 592 prescriptions.
Results
In this study, demographic information of the patients, WHO prescribing indicators, prescription errors, and data related to the prevalence of various diseases among outpatients during the COVID-19 period were gathered and analyzed from the 600 collected prescriptions.
Demographic characteristics
Of the 600 prescriptions reviewed, 323(53.83%) belonged to male patients, whereas 277(46.17%) prescriptions were from female patients. It was observed that, of the 592 prescriptions (age of 8 patients was not mentioned in the prescription), patients aged 25–40 years sought medical attention the most, 243(41.05%), followed by the younger (15–24 years) and senior adult (41–60 years) patients. Notably, children of 0-14 years of age and elderly patients (>60 years) visited the hospitals at the least frequency 16(2.70%) and 56(9.46%) respectively.
Prevalence of diseases among patients during the COVID-19
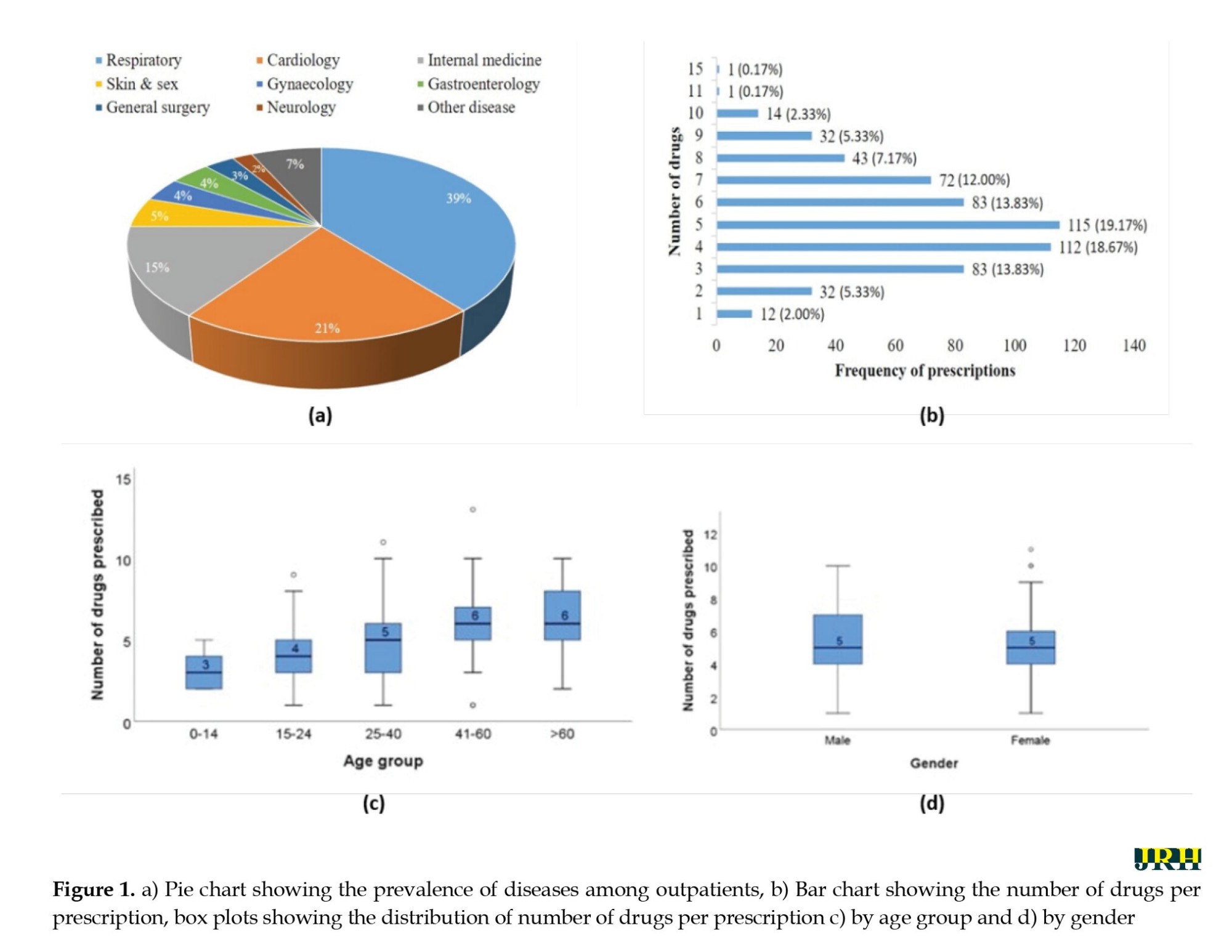
Over the seven months of prescription collection, it was observed that a hefty 234(39%) of the prescriptions belonged to patients suffering from various respiratory difficulties (Figure 1a). In addition, 126(21%) and 90(15%) of prescriptions were collected from cardiac patients’ and internal medicine departments, respectively. Patients attending the internal medicine departments were suffering from asthma, lower respiratory tract problems, and common cold symptoms mostly. A negligible percentage of patients visited other departments, including skin and sex, gynecology, gastroenterology, general surgery, neurology, and others (5%, 4%, 4%, 3%, 2% and 7%, respectively) (Figure 1a).
Assessment of WHO prescribing indicators
This study aimed to observe whether the collected 600 prescriptions complied with the following five indicators set by WHO:
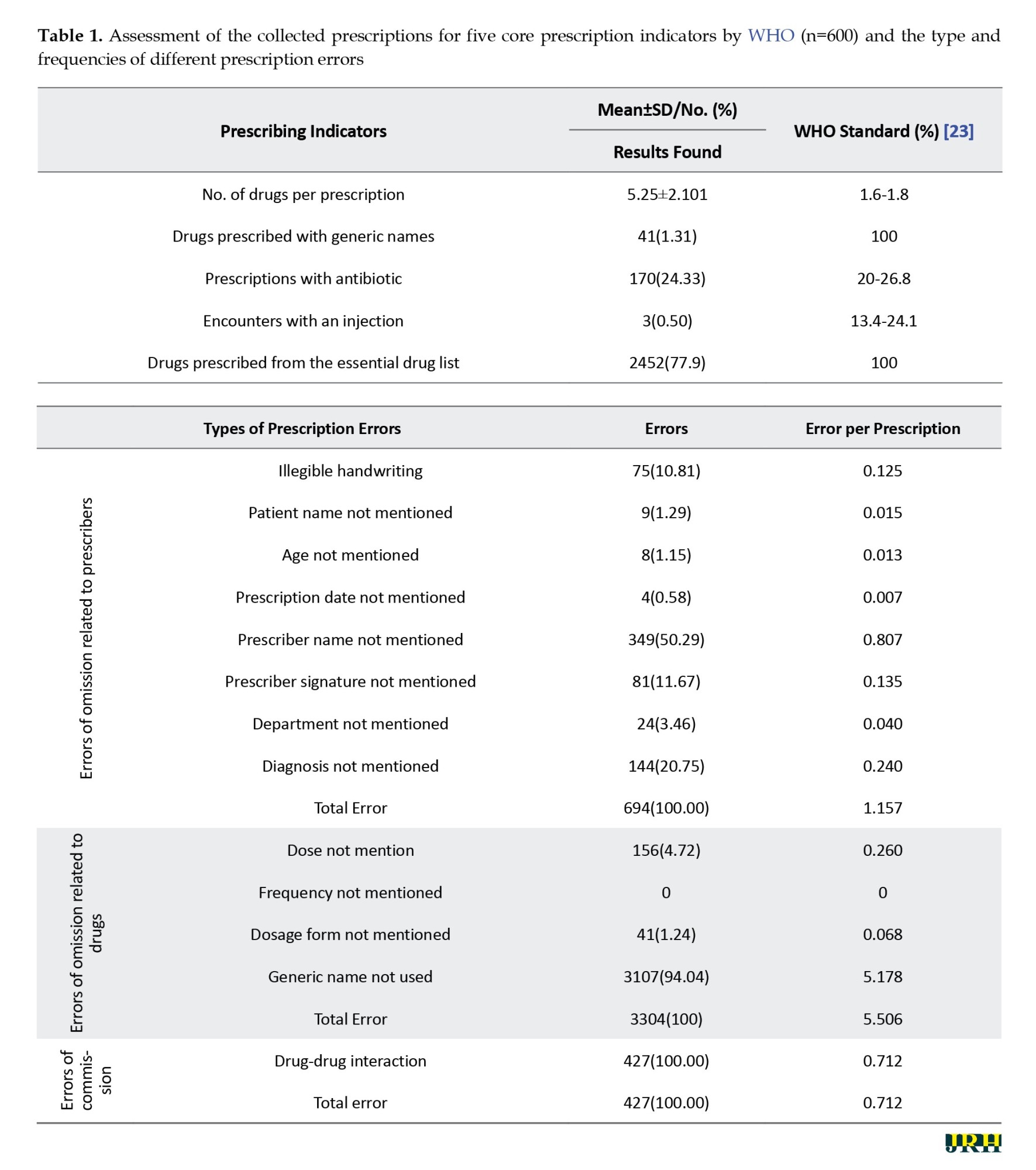
Mean number of drugs per encounter/prescription, percentage of drugs prescribed by generic name, percentage of encounters containing antibiotics, percentage of prescriptions containing injections, and percentage of drugs prescribed from the essential drug list. Table 1 presents the overall WHO prescription indicators observed from this study.
Mean number of drugs per encounter/prescription
A total of 3148 medicines were prescribed in the collected 600 prescriptions. Mean number of drugs prescribed per prescription was 5.25 with a standard deviation of 2.1 (Table 1). Notably, 115(19.17%) and 112(18.67%) encounters containing five and four drugs, respectively, accounted for the highest frequencies (Figure 1b). Only 12(2%) prescriptions contained a single drug, while the number of encounters with the highest number of drugs (15) was one. In addition, the mean number of drugs prescribed per prescription was found to differ significantly among patients from different age groups (F=25.557, P<0.001) and gender (P=0.013) (Figure 1c and Figure 1d).
Percentage of drugs prescribed by generic name
It was observed that 3107(98.69%) of the drugs in this study were prescribed by their brand names (Table 1), which did not meet the ideal WHO prescription standard.
Percentage of encounters containing antibiotics
The number of prescriptions containing antibiotics was found to be 170 representing 24.33% of the total encounters (Table 1), which complied with the WHO permissible range (20.0-26.8%) [29].
Percentage of prescriptions containing injections
The number of prescriptions that contained injections was 3(0.50%) (Table 1), which lay below the WHO prescribing standard of 13.4-24.1% [29].
Percentage of drugs prescribed from the essential drug list
WHO standard prescription indicators mandate that 100% of the prescribed drugs should follow the national essential drugs list of the respective country. In this survey, 2452 out of 3148 drugs were prescribed from this list, accounting for approximately 77.9% of the total drugs, which failed to fulfill the WHO prescribing guidelines (Table 1).
Prescription errors
A total of 4425 errors were found in 600 prescriptions, indicating 7.375 errors per prescription (Table 1). On average, each prescription carried 1.157 omission errors related to the prescriber, of which the absence of the prescriber’s name was the most frequent 349(50.29%). Additional omission errors included failure to mention diagnosis 144(20.75%), absence of the physician’s signature 81(11.67%), and name of the department 24 (3.46%) (Table 1). Seventy-five (10.81%) of the prescriptions had illegible handwriting, making it very difficult for both the patients and dispenser to understand the prescriptions, which again may lead to incorrect drugs and doses [30].
Errors of omission related to drugs are the most common type of prescription errors found in this study, with a mean of 5.506 errors per prescription. Generic name, dose, and dosage form were absent in 3304(94.04%), 156(4.72%), and 41(1.24%) encounters, respectively (Table 1). However, dosage frequency was mentioned for all the drugs prescribed. The only error of commission studied was drug-drug interaction, and 427(13.56%) of all the prescribed drugs were at risk of drug-drug interaction, resulting in a 0.712 mean number of errors of commission per prescription (Table 1).
Therapeutic duplication
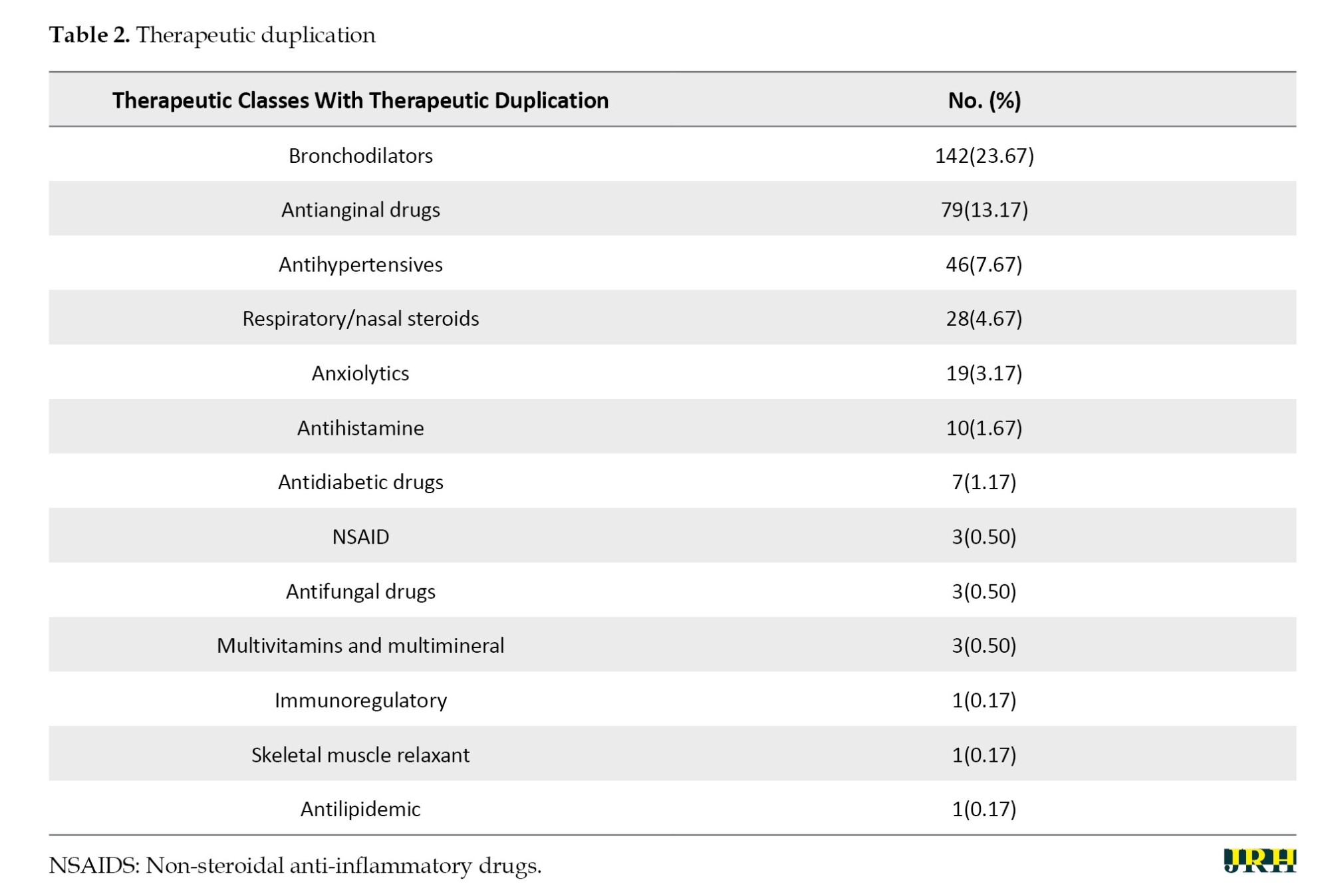
In this investigation, prescriptions containing multiple bronchodilators were found in the maximum number, 142(23.67%), followed by antianginal drugs, 79(13.17%), and antihypertensives, 46(7.67%) (Table 2). Nasal steroids and their combined sprays are quite popular in treating rhinitis [31] and in 28(4.67%) of the total prescriptions, nasal steroids were prescribed more than once (Table 2). Additionally, prescription of multiple non-steroidal anti-inflammatory drugs (NSAIDS), antihistamines, anxiolytics and antidepressants, topical preparations, locally and centrally acting skeletal muscle relaxants, multivitamins and multimineral preparations, antifungal, antidiabetic drugs, and statins were also found to a lesser extent (Table 2).
Prescribed drugs of different therapeutic classes
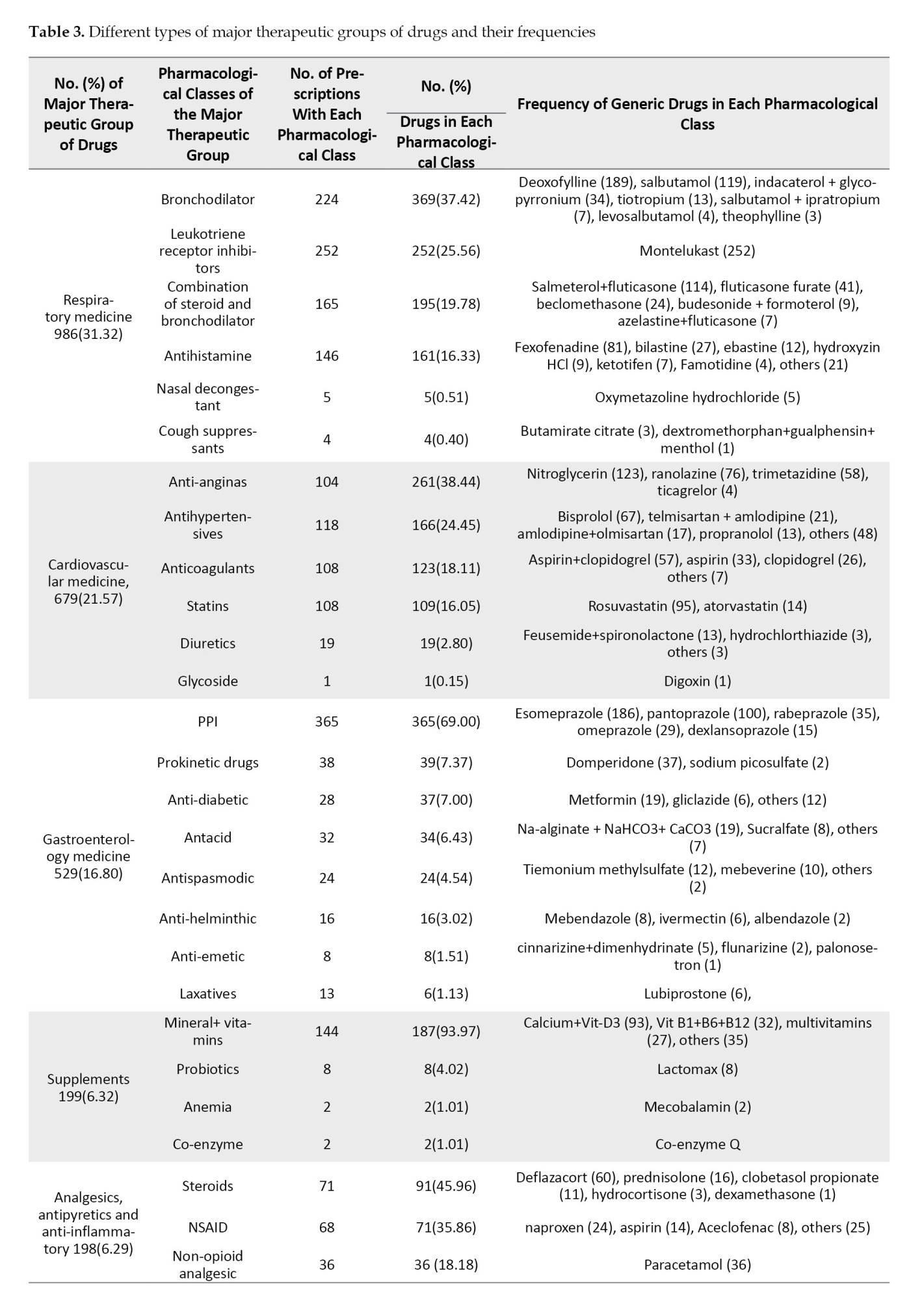
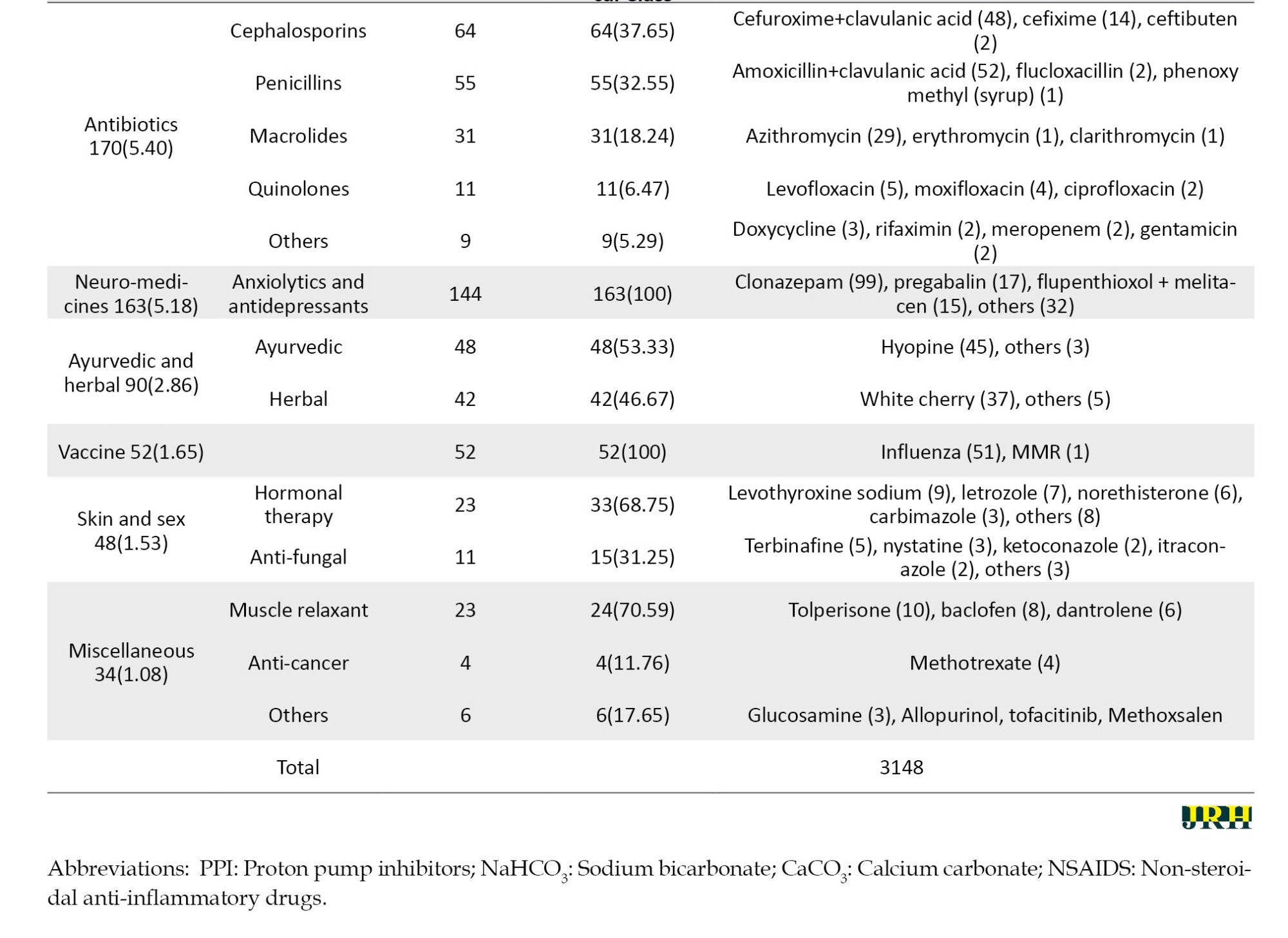
Different therapeutic classes of drugs prescribed for the ambulatory patients during the COVID-19 period were also assessed (Table 3).
Discussion
In this cross-sectional study, the prescription patterns of the non-COVID outpatients were surveyed for the very first time from three tertiary-level hospitals of Dhaka, Bangladesh, during the COVID-19 pandemic. Mostly middle-aged male patients suffering from respiratory diseases predominantly visited the outpatient section of the hospital. Most prescribed drugs were from gastroenterology and respiratory therapeutic classes. The mean number of drugs per prescription was more than the WHO prescribing indicators. In addition, only a few percent of the encounters contained the generic name of the drugs and prescribed medicines from the essential drugs list. However, the number of antibiotics prescribed was noticed to be within the permissible range. Prescription errors related to both omission and commission were observed in almost every encounter. Findings of this study may help in raising awareness on standard prescribing practice, to promote rational use of drugs, and may also provide valuable suggestions to the policy makers and clinicians of Bangladesh to guarantee better therapeutic management during any future pandemic outbreak.
The number of male outpatients outweighs the female patients in this survey, which is in support of a few previous studies [12, 16]. Male patients receive greater access to healthcare facilities because of the male-dominated socio-cultural nature of Bangladesh [29]. Most patients were 25–40 years of age, consistent with Rahman et al. in 2022 [13], because they were more likely to go outside of home regularly for living and other purposes, and hence were extra vigilant about getting infected by COVID-19.
A total of 234 patients (39%) visited the hospitals during this period due to various respiratory diseases. COVID-19 is predominantly a respiratory tract disorder producing symptoms, such as pneumonia. Hence it is understandable that people were cautious and adopted prophylactic measures to avoid contamination and admission to hospitals [32, 33].
The cumulative mean number of medicines per prescription (5.25±2.1) was more than 2 times greater than the WHO ideal value (1.6–1.8), indicating the practice of polypharmacy. We observed a comparable trend in medicine prescribing practice during the COVID-19 period in another work done by Samad et al. [34]. However, this number was observed to be much lower in India and Nigeria (2.89 and 3.1 drugs per prescription, respectively) in the pandemic period [27, 28]. Nearly 38% prescriptions contained 4 or more drugs, which was also greater than the previously conducted surveys [16, 35]. Prescriber’s poor knowledge of diseases and drugs, side-effects, incompatibilities; lack of regulation and monitoring on polypharmacy or unavailability of the appropriate therapeutics could be attributable to this situation.
According to WHO guidelines, all medicines should be prescribed by their generic names to minimize aggressive marketing competition among the pharmaceutical companies [36]. However, an opposite trend was observed in the current study, supporting the findings of some pre-COVID and COVID period investigations [12, 14, 27, 28, 34].
During COVID-19, a massive number of infected and suspected patients received antibiotics owing to the lack of appropriate antivirals or the advent of disease-specific therapy, fear of bacterial superinfection and adequate monitoring [26]. This study shows that the percentage of antibiotics per encounter was within the WHO acceptable range, which is superior to other comparable studies conducted in India and Nigeria [27, 28]. Although evidence-based antibiotic prescription practice and adaptation of antibiotic regulation policy are crucial to prevent bacterial resistance development [37], all the antibiotics were prescribed empirically, based solely on clinical experience and without performing any culture sensitivity test [15, 26].
The WHO guideline to prescribe 100% of the prescription drugs from the essential drugs list was not obeyed in this study. However, the observed percentage 2452(77.9%) is significantly higher than that reported by Afsan et al. in 2012, Samad et al. in 2024, and comparable to that of Nigeria (84.2%) as observed by M.M. Abubakar et al. in 2024 [14, 28, 34]. Essential drugs are selected depending on the prevailing disease condition of a country, available generic versions, affordability, safety, risk-benefit ratio, and the pharmacokinetic profile of the population, which led to improved quality of medicine use [38]. Hence, prescribing from the essential drugs list maximizes the drug availability, cost-effectiveness, eliminates the chances of drug incompatibilities, lowers adverse drug reaction incidents, and improves patient compliance [39].
According to the National Coordinating Council for Medication Error Reporting and Prevention, 15% of the prescription errors are linked to problems with handwriting, abbreviations, and incomplete medication orders [37]. In this study, omission errors related to the patient’s name and age were missing in 17 prescriptions, which is similar to another study conducted by Haque et al. [16]. Additionally, a large number of encounters (565 prescriptions) lack prescriber’s details, including name and signature. Prescribers’ affiliations are necessary to prove the authenticity of the prescription, discourage the incidents of self-medication, expedite the contact with the physicians in case of any ambiguity regarding dose and dosage form, and for prescribing controlled drugs, including narcotics, hormones and antibiotics [39]. Aziz et al. also reported a similar trend demonstrating the absence of prescribers’ details in analyzing the prescribing patterns in some districts of Bangladesh other than Dhaka [40]. Prescribers’ signature were found significantly missing in both Government and private hospitals of Dhaka city, Bangladesh in another prescription pattern survey during the COVID-19 pandemic [34]. However, the mean number of errors of omission related to the prescriber was found to be lower than the data reported in a pre-COVID study by Rahman et al. [13]. Another crucial omission error was the absence of diagnosis information, which is a violation of the professional code of conduct. Patients should be well informed of their ailment and have an appropriate explanation of the diagnosis. A wrong diagnosis can lead to patients’ health risks and financial waste, while the opposite may even help the pharmacist in dispensing the appropriate drug in case of illegible handwriting of the prescriber [41]. Out of 3148 drugs, dose and dosage forms were not mentioned for 156 and 41 prescribed drugs, respectively, which were lower than previously reported findings by Haque et al. et al. [16]. Mentioning the dose and dosage form of a drug in a prescription is crucial, as the same molecule could be available in different strengths and physical forms. Moreover, patients’ height, weight, and age are the key parameters to choose the correct dose and dosage form of drugs, which can ensure the safety and efficacy of the treatment.
Therapeutic duplicates were detected in 57% prescriptions, which is also higher than the previous findings. Practice of therapeutic duplication does not prove effectiveness by any epidemiological evidence, significantly increases medication cost, polypharmacy, and risk of adverse drug events, including drug-drug interaction. Proper knowledge and training of the prescribers, alongside imposing strict regulations, are necessary to reduce such therapeutic duplication [12].
This study also demonstrated the diverse ranges of therapeutic classes of drugs prescribed during the pandemic period. A substantial number of prescriptions containing various proton pump inhibitors (PPIs) suggest the extensive prevalence of gastritis/ulcer among the Bangladeshi population. Mizanur et al. also found esomeprazole as one of the most commonly prescribed medicines in Bangladesh [13]. Montelukast was the most frequently prescribed respiratory medicine during COVID-19 because its anti-inflammatory and cytokine secretion inhibiting effects were proven beneficial in the reduction of the severity of the upper airway inflammatory lung diseases in hospitalized patients [42].
This survey finds cephalosporins (37.65%) as the most extensively prescribed antibiotics, which is similar to the findings of other studies [43]. Cephalosporins are broad-spectrum antibiotics possessing widespread efficacy against various pathogens, readily available, and cost-effective. Reportedly, this group of drugs was the most prescribed antibiotics during the pre-pandemic and pandemic period compared with the macrolides [43]. It was also observed that rosuvastatin was the most preferred drug of choice from the cardiovascular group of drugs. In a randomized controlled single blind trial, Bangladeshi patients with atherosclerotic cardiovascular diseases encountered less muscle spasm, pain, myopathy, liver enzyme function, and gastrointestinal discomfort when treated with rosuvastatin in comparison with atorvastatin [44].
This study found that all the major therapeutic groups of drugs, including gastroenterology, respiratory, antibiotics, cardiovascular, and neuro medicines, were prescribed more to the male patients compared to female patients, which could be due to the presence of a higher number of male outpatients. However, a greater number of supplements were prescribed to the female patients, which matches the findings of previous studies [45]. In Bangladesh, women are the exclusive consumers of various nutritional supplements attributable to malnutrition, lack of proper education, poverty, and their reproductive system requirements [46].
However, the study was conducted on the outpatients of the tertiary-level hospitals located in Dhaka city, the capital of Bangladesh. To get a more precise and broader idea about the prescription pattern nationwide during that pandemic period, a larger survey is recommended across the country, including primary and secondary healthcare facilities alongside tertiary-level hospitals. Drug-drug interactions need to be further studied by clinical significance level and inpatients’ prescriptions should also be investigated and analyzed to enrich the study report. Furthermore, post-COVID prescription patterns need to be analyzed and compared with the current study findings for comprehensive interpretation of this study’s findings.
Conclusion
The current study gives a comprehensive demonstration of the healthcare-seeking tendency as well as the prescription pattern in the outpatient facilities in some Bangladeshi hospitals during the COVID-19 pandemic. The findings of this study may be helpful in guiding the concerned authority to design and implement appropriate strategies to promote prescription writing following the WHO prescription indicators, rational use of drugs, while minimizing polypharmacy practice and prescription errors. In addition, the outcomes of this survey may help in identifying and ensuring the availability of the essential medicines from different therapeutic groups while taking prophylactic measures for any prospective future outbreak of COVID-19.
Ethical Considerations
Compliance with ethical guidelines
The study was conducted following the principles of the World Medical Association and the Declaration of Helsinki. Permission to conduct the prescription survey was taken from the Faculty of Pharmacy (Reference no. Pharm.B/44/20-21), University of Dhaka, Bangladesh. The purpose of the study was explained to the non-COVID outpatients, and photos of the prescriptions were collected from the patients after obtaining consent. The confidentiality of personal information was ensured, and information was used for research purposes only.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Md. Raihan Sarkar, Nahid Sharmin; Data collection: Kazi Milenur Rahman Prattay, Md. Bappy Hawlader and Md. Saiful Islam; Formal analysis: Kazi Milenur Rahman Prattay, Md. Bappy Hawladerand Md. Saiful Islam; Investigation: Md. Bappy Hawlader and Md. Saiful Islam; Methodology: Md. Bappy Hawlader, Md. Saiful Islam, Kazi Milenur Rahman Prattay, Nahid Sharmin and Md. Raihan Sarkar; Software: Kazi Milenur Rahman Prattay, Sheikh Zahir Raihan and Md. Abdul Muhit; Supervision: Md. Raihan Sarkar and Nahid Sharmin; Writing the original draft: Md. Bappy Hawlader, Md. Saiful Islam, Kazi Milenur Rahman Prattay and Nahid Sharmin; Review and editing: Md. Raihan Sarkar, Sheikh Zahir Raihan, Md. Abdul Muhit and Nahid Sharmin
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors acknowledge the Department of Pharmacy, Faculty of Pharmacy, University of Dhaka, Bangladesh; Dhaka Medical College Hospital, Dhaka, Bangladesh; BSMMU, Dhaka, Bangladesh, and National Institute of Diseases of the Chest and Hospital, Dhaka, Bangladesh.
References
Aprescription is a rightfully written instruction of medication given to the pharmacist and patients by a qualified and registered medical professional [1] that provides clinical care and ensures patient safety [2]. Ideally, all prescriptions warrant and should maximize the rational use of drugs. Inappropriate prescription of medications leads to irrational use of drugs, medication errors, lengthened hospitalization, and increased economic burden on patients [3]. Over 50% of all medications are administered, given, or marketed improperly on a global scale, while 50% of the patients do not take their medications as prescribed. Common irrational prescribing practices include polypharmacy, prescribing antimicrobials for nonbacterial infections, unnecessary injections, and deviation from clinical guidelines [4]. In developing countries, about 44%-97% of hospitalized patients are unreasonably prescribed antibiotics [5, 6], which has resulted in a rising rate of antibiotic resistance, posing a global public health concern. The reported 6-37% drug-drug interactions in prescriptions have been attributed to the practice of polypharmacy and lack of proper monitoring of prescriptions [7]. To lessen the intensity of these damages and encourage responsible drug use, World Health Organization (WHO) has established and verified key drug use indicators for prescribing, patient care, and facility-specific investigations, which are increasingly gaining importance in developing countries [8, 9].
Prescription error represents the major form of medication error. Reportedly, at least one mistake occurs in 15% to 21% of all written prescriptions [10]. Nearly 7,000 fatalities are documented each year consequent to medication errors [2]. The majority of these are regarded as errors of commission (incorrectly written information) and omission (crucial missing information) [11].
In developing countries, a large number of drugs are prescribed irrationally, burdening drug availability and the medical sector’s financial resources [4, 12]. Reportedly, most of the prescriptions in Bangladesh contained 3-8 drugs [12, 13], the majority of them were not prescribed by their generic name [12, 14], and the number of antibiotics exceeded the WHO permitted range [12, 14]. Although all the drugs should be prescribed from the essential drugs list, only about 30-46% of them belonged to this list [13, 15]. Moreover, prescription errors are also very common, which include illegible handwriting, wrong or missing dose strength, prescribing incompatible drugs, absence of practitioner’s name, patient information, date, diagnosis, and medication administration instructions for the patients [12, 13, 15, 16]. The persistence of these errors and deviation from WHO standards has encouraged polypharmacy, antibiotic resistance, and drug interactions, highlighting the need for stronger prescription monitoring and regulations [17].
The debilitating effect of the COVID-19 infection was first reported in China in December 2019 and attributed to the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The disease spread rapidly and was declared a global pandemic by the WHO in March 2020 [18]. The scarcity of knowledge regarding severe acute respiratory SARS-CoV-2’s spreadability, severity, and treatment guidelines, along with misleading social media prescriptions, triggered an extensive level of irrational drug prescribing [19]. The severity of COVID-19 was reportedly further enhanced by a number of underlying conditions, including diabetes, hypertension, asthma, and cancer, which also significantly contributed to the development of complex symptoms and the rising mortality rate [20]. To combat the virus, a plethora of medicines were repurposed without adequate clinical data, including paracetamol, leukotriene inhibitors, antibiotics, bronchodilators, angiotensin-converting-enzyme (ACE) inhibitors, antiviral and steroidal drugs, along with multivitamins [21]. Multiple studies were conducted globally to investigate drug use patterns during the pandemic [22-24]. Silva TM et al. reported a decrease in antibiotic prescription [22], while Aboulatta et al. found reduced use of antibiotics, cardiovascular drugs, and opioids [23]. However, another study showed a massive 96% increase in over-the-counter drug sales, particularly vitamins, painkillers, antipyretics, cough and cold preparations, irrespective of age groups and gender [24].
In Bangladesh, the first COVID-19 case was identified on March 8, 2020, and by August 11, 2020, the country had officially reported 263,503 cases, with 3,471 deaths [18]. Several studies assessed prescription patterns in COVID-19 patients in Bangladesh [21, 22]. However, although a few studies have been conducted across the world investigating the irrational use of drugs during the pandemic using WHO prescribing indicators [25-28], no such study focusing on the prescription pattern of the non-COVID outpatients is reported in Bangladesh yet.
Therefore, this cross-sectional study aimed to evaluate the prescribing patterns and errors among non-COVID outpatients based on WHO indicators and to understand healthcare-seeking behavior during the pandemic in tertiary hospitals of Dhaka, Bangladesh. The findings may help determine the impact of COVID-19 on prescribing behavior and provide insights to strengthen prescription monitoring policies for future health emergencies.
Methods
Study design, inclusion criteria
The present study is a hospital-based cross-sectional survey conducted in three tertiary-level hospitals of Dhaka, the capital city of Bangladesh. All three hospitals have facilities to provide both inpatient and outpatient services. Prescriptions were collected from the outpatients visiting various outdoor departments of the hospitals from December 1, 2020 to June 30, 2021 during the COVID-19 pandemic period. Patients who were confirmed to be non-COVID-19 cases were included in this study through simple random sampling to minimize selection bias. COVID-19 status was determined by verbal confirmation of symptom absence for general outpatients, and both verbal confirmation and review of antigen test results (as received via SMS in cell phones) for patients visiting the respiratory outpatient department.
Sampling technique and mode of data collection
This cross-sectional study analyzed the prevalence of different ailments, prescribing patterns, and assessed the WHO-established drug use indicators during the pandemic period. [8] Hence in accordance with the WHO guideline [8], 600 prescriptions were collected from the outpatient’s facilities of the hospitals. Photos of the prescriptions were taken after obtaining patient consent. The data from each prescription was recorded separately, eliminating any prescription from the inpatient unit. Patients’ demographic, clinical, diagnosed conditions, and prescribed drugs information were extracted while ensuring the anonymity and organized using Google Spreadsheets by a single trained reviewer under strict monitoring by the study team members to ensure consistency. This information was further studied to analyze the WHO prescription indicators and prescription errors [8].
Data analysis
Data from Google Spreadsheets were imported into and analyzed using MS Excel 2013 and SPSS software, version 26.0. For normally distributed continuous data, the mean and standard deviation were calculated while categorical data were expressed as proportions. One-way analysis of variance (ANOVA) was used to compare the mean number of drugs prescribed across different age groups, while independent sample t-tests were applied to compare means between male and female patients. Prior to conducting these tests, the assumptions of normality and homogeneity of variance were assessed using the Shapiro-Wilk test and Levene’s test, respectively. A P≤0.05 was considered statistically significant. The only missing data was the age for 8 patients, although all other relevant information was available for these cases. Therefore, for analyses where age was a necessary variable, specifically, while constructing the box plot and the ANOVA test evaluating the mean number of drugs prescribed, these 8 prescriptions we excluded and the analysis was conducted on the remaining 592 prescriptions.
Results
In this study, demographic information of the patients, WHO prescribing indicators, prescription errors, and data related to the prevalence of various diseases among outpatients during the COVID-19 period were gathered and analyzed from the 600 collected prescriptions.
Demographic characteristics
Of the 600 prescriptions reviewed, 323(53.83%) belonged to male patients, whereas 277(46.17%) prescriptions were from female patients. It was observed that, of the 592 prescriptions (age of 8 patients was not mentioned in the prescription), patients aged 25–40 years sought medical attention the most, 243(41.05%), followed by the younger (15–24 years) and senior adult (41–60 years) patients. Notably, children of 0-14 years of age and elderly patients (>60 years) visited the hospitals at the least frequency 16(2.70%) and 56(9.46%) respectively.
Prevalence of diseases among patients during the COVID-19
Over the seven months of prescription collection, it was observed that a hefty 234(39%) of the prescriptions belonged to patients suffering from various respiratory difficulties (Figure 1a). In addition, 126(21%) and 90(15%) of prescriptions were collected from cardiac patients’ and internal medicine departments, respectively. Patients attending the internal medicine departments were suffering from asthma, lower respiratory tract problems, and common cold symptoms mostly. A negligible percentage of patients visited other departments, including skin and sex, gynecology, gastroenterology, general surgery, neurology, and others (5%, 4%, 4%, 3%, 2% and 7%, respectively) (Figure 1a).
Assessment of WHO prescribing indicators
This study aimed to observe whether the collected 600 prescriptions complied with the following five indicators set by WHO:
Mean number of drugs per encounter/prescription, percentage of drugs prescribed by generic name, percentage of encounters containing antibiotics, percentage of prescriptions containing injections, and percentage of drugs prescribed from the essential drug list. Table 1 presents the overall WHO prescription indicators observed from this study.
Mean number of drugs per encounter/prescription
A total of 3148 medicines were prescribed in the collected 600 prescriptions. Mean number of drugs prescribed per prescription was 5.25 with a standard deviation of 2.1 (Table 1). Notably, 115(19.17%) and 112(18.67%) encounters containing five and four drugs, respectively, accounted for the highest frequencies (Figure 1b). Only 12(2%) prescriptions contained a single drug, while the number of encounters with the highest number of drugs (15) was one. In addition, the mean number of drugs prescribed per prescription was found to differ significantly among patients from different age groups (F=25.557, P<0.001) and gender (P=0.013) (Figure 1c and Figure 1d).
Percentage of drugs prescribed by generic name
It was observed that 3107(98.69%) of the drugs in this study were prescribed by their brand names (Table 1), which did not meet the ideal WHO prescription standard.
Percentage of encounters containing antibiotics
The number of prescriptions containing antibiotics was found to be 170 representing 24.33% of the total encounters (Table 1), which complied with the WHO permissible range (20.0-26.8%) [29].
Percentage of prescriptions containing injections
The number of prescriptions that contained injections was 3(0.50%) (Table 1), which lay below the WHO prescribing standard of 13.4-24.1% [29].
Percentage of drugs prescribed from the essential drug list
WHO standard prescription indicators mandate that 100% of the prescribed drugs should follow the national essential drugs list of the respective country. In this survey, 2452 out of 3148 drugs were prescribed from this list, accounting for approximately 77.9% of the total drugs, which failed to fulfill the WHO prescribing guidelines (Table 1).
Prescription errors
A total of 4425 errors were found in 600 prescriptions, indicating 7.375 errors per prescription (Table 1). On average, each prescription carried 1.157 omission errors related to the prescriber, of which the absence of the prescriber’s name was the most frequent 349(50.29%). Additional omission errors included failure to mention diagnosis 144(20.75%), absence of the physician’s signature 81(11.67%), and name of the department 24 (3.46%) (Table 1). Seventy-five (10.81%) of the prescriptions had illegible handwriting, making it very difficult for both the patients and dispenser to understand the prescriptions, which again may lead to incorrect drugs and doses [30].
Errors of omission related to drugs are the most common type of prescription errors found in this study, with a mean of 5.506 errors per prescription. Generic name, dose, and dosage form were absent in 3304(94.04%), 156(4.72%), and 41(1.24%) encounters, respectively (Table 1). However, dosage frequency was mentioned for all the drugs prescribed. The only error of commission studied was drug-drug interaction, and 427(13.56%) of all the prescribed drugs were at risk of drug-drug interaction, resulting in a 0.712 mean number of errors of commission per prescription (Table 1).
Therapeutic duplication
In this investigation, prescriptions containing multiple bronchodilators were found in the maximum number, 142(23.67%), followed by antianginal drugs, 79(13.17%), and antihypertensives, 46(7.67%) (Table 2). Nasal steroids and their combined sprays are quite popular in treating rhinitis [31] and in 28(4.67%) of the total prescriptions, nasal steroids were prescribed more than once (Table 2). Additionally, prescription of multiple non-steroidal anti-inflammatory drugs (NSAIDS), antihistamines, anxiolytics and antidepressants, topical preparations, locally and centrally acting skeletal muscle relaxants, multivitamins and multimineral preparations, antifungal, antidiabetic drugs, and statins were also found to a lesser extent (Table 2).
Prescribed drugs of different therapeutic classes
Different therapeutic classes of drugs prescribed for the ambulatory patients during the COVID-19 period were also assessed (Table 3).
Discussion
In this cross-sectional study, the prescription patterns of the non-COVID outpatients were surveyed for the very first time from three tertiary-level hospitals of Dhaka, Bangladesh, during the COVID-19 pandemic. Mostly middle-aged male patients suffering from respiratory diseases predominantly visited the outpatient section of the hospital. Most prescribed drugs were from gastroenterology and respiratory therapeutic classes. The mean number of drugs per prescription was more than the WHO prescribing indicators. In addition, only a few percent of the encounters contained the generic name of the drugs and prescribed medicines from the essential drugs list. However, the number of antibiotics prescribed was noticed to be within the permissible range. Prescription errors related to both omission and commission were observed in almost every encounter. Findings of this study may help in raising awareness on standard prescribing practice, to promote rational use of drugs, and may also provide valuable suggestions to the policy makers and clinicians of Bangladesh to guarantee better therapeutic management during any future pandemic outbreak.
The number of male outpatients outweighs the female patients in this survey, which is in support of a few previous studies [12, 16]. Male patients receive greater access to healthcare facilities because of the male-dominated socio-cultural nature of Bangladesh [29]. Most patients were 25–40 years of age, consistent with Rahman et al. in 2022 [13], because they were more likely to go outside of home regularly for living and other purposes, and hence were extra vigilant about getting infected by COVID-19.
A total of 234 patients (39%) visited the hospitals during this period due to various respiratory diseases. COVID-19 is predominantly a respiratory tract disorder producing symptoms, such as pneumonia. Hence it is understandable that people were cautious and adopted prophylactic measures to avoid contamination and admission to hospitals [32, 33].
The cumulative mean number of medicines per prescription (5.25±2.1) was more than 2 times greater than the WHO ideal value (1.6–1.8), indicating the practice of polypharmacy. We observed a comparable trend in medicine prescribing practice during the COVID-19 period in another work done by Samad et al. [34]. However, this number was observed to be much lower in India and Nigeria (2.89 and 3.1 drugs per prescription, respectively) in the pandemic period [27, 28]. Nearly 38% prescriptions contained 4 or more drugs, which was also greater than the previously conducted surveys [16, 35]. Prescriber’s poor knowledge of diseases and drugs, side-effects, incompatibilities; lack of regulation and monitoring on polypharmacy or unavailability of the appropriate therapeutics could be attributable to this situation.
According to WHO guidelines, all medicines should be prescribed by their generic names to minimize aggressive marketing competition among the pharmaceutical companies [36]. However, an opposite trend was observed in the current study, supporting the findings of some pre-COVID and COVID period investigations [12, 14, 27, 28, 34].
During COVID-19, a massive number of infected and suspected patients received antibiotics owing to the lack of appropriate antivirals or the advent of disease-specific therapy, fear of bacterial superinfection and adequate monitoring [26]. This study shows that the percentage of antibiotics per encounter was within the WHO acceptable range, which is superior to other comparable studies conducted in India and Nigeria [27, 28]. Although evidence-based antibiotic prescription practice and adaptation of antibiotic regulation policy are crucial to prevent bacterial resistance development [37], all the antibiotics were prescribed empirically, based solely on clinical experience and without performing any culture sensitivity test [15, 26].
The WHO guideline to prescribe 100% of the prescription drugs from the essential drugs list was not obeyed in this study. However, the observed percentage 2452(77.9%) is significantly higher than that reported by Afsan et al. in 2012, Samad et al. in 2024, and comparable to that of Nigeria (84.2%) as observed by M.M. Abubakar et al. in 2024 [14, 28, 34]. Essential drugs are selected depending on the prevailing disease condition of a country, available generic versions, affordability, safety, risk-benefit ratio, and the pharmacokinetic profile of the population, which led to improved quality of medicine use [38]. Hence, prescribing from the essential drugs list maximizes the drug availability, cost-effectiveness, eliminates the chances of drug incompatibilities, lowers adverse drug reaction incidents, and improves patient compliance [39].
According to the National Coordinating Council for Medication Error Reporting and Prevention, 15% of the prescription errors are linked to problems with handwriting, abbreviations, and incomplete medication orders [37]. In this study, omission errors related to the patient’s name and age were missing in 17 prescriptions, which is similar to another study conducted by Haque et al. [16]. Additionally, a large number of encounters (565 prescriptions) lack prescriber’s details, including name and signature. Prescribers’ affiliations are necessary to prove the authenticity of the prescription, discourage the incidents of self-medication, expedite the contact with the physicians in case of any ambiguity regarding dose and dosage form, and for prescribing controlled drugs, including narcotics, hormones and antibiotics [39]. Aziz et al. also reported a similar trend demonstrating the absence of prescribers’ details in analyzing the prescribing patterns in some districts of Bangladesh other than Dhaka [40]. Prescribers’ signature were found significantly missing in both Government and private hospitals of Dhaka city, Bangladesh in another prescription pattern survey during the COVID-19 pandemic [34]. However, the mean number of errors of omission related to the prescriber was found to be lower than the data reported in a pre-COVID study by Rahman et al. [13]. Another crucial omission error was the absence of diagnosis information, which is a violation of the professional code of conduct. Patients should be well informed of their ailment and have an appropriate explanation of the diagnosis. A wrong diagnosis can lead to patients’ health risks and financial waste, while the opposite may even help the pharmacist in dispensing the appropriate drug in case of illegible handwriting of the prescriber [41]. Out of 3148 drugs, dose and dosage forms were not mentioned for 156 and 41 prescribed drugs, respectively, which were lower than previously reported findings by Haque et al. et al. [16]. Mentioning the dose and dosage form of a drug in a prescription is crucial, as the same molecule could be available in different strengths and physical forms. Moreover, patients’ height, weight, and age are the key parameters to choose the correct dose and dosage form of drugs, which can ensure the safety and efficacy of the treatment.
Therapeutic duplicates were detected in 57% prescriptions, which is also higher than the previous findings. Practice of therapeutic duplication does not prove effectiveness by any epidemiological evidence, significantly increases medication cost, polypharmacy, and risk of adverse drug events, including drug-drug interaction. Proper knowledge and training of the prescribers, alongside imposing strict regulations, are necessary to reduce such therapeutic duplication [12].
This study also demonstrated the diverse ranges of therapeutic classes of drugs prescribed during the pandemic period. A substantial number of prescriptions containing various proton pump inhibitors (PPIs) suggest the extensive prevalence of gastritis/ulcer among the Bangladeshi population. Mizanur et al. also found esomeprazole as one of the most commonly prescribed medicines in Bangladesh [13]. Montelukast was the most frequently prescribed respiratory medicine during COVID-19 because its anti-inflammatory and cytokine secretion inhibiting effects were proven beneficial in the reduction of the severity of the upper airway inflammatory lung diseases in hospitalized patients [42].
This survey finds cephalosporins (37.65%) as the most extensively prescribed antibiotics, which is similar to the findings of other studies [43]. Cephalosporins are broad-spectrum antibiotics possessing widespread efficacy against various pathogens, readily available, and cost-effective. Reportedly, this group of drugs was the most prescribed antibiotics during the pre-pandemic and pandemic period compared with the macrolides [43]. It was also observed that rosuvastatin was the most preferred drug of choice from the cardiovascular group of drugs. In a randomized controlled single blind trial, Bangladeshi patients with atherosclerotic cardiovascular diseases encountered less muscle spasm, pain, myopathy, liver enzyme function, and gastrointestinal discomfort when treated with rosuvastatin in comparison with atorvastatin [44].
This study found that all the major therapeutic groups of drugs, including gastroenterology, respiratory, antibiotics, cardiovascular, and neuro medicines, were prescribed more to the male patients compared to female patients, which could be due to the presence of a higher number of male outpatients. However, a greater number of supplements were prescribed to the female patients, which matches the findings of previous studies [45]. In Bangladesh, women are the exclusive consumers of various nutritional supplements attributable to malnutrition, lack of proper education, poverty, and their reproductive system requirements [46].
However, the study was conducted on the outpatients of the tertiary-level hospitals located in Dhaka city, the capital of Bangladesh. To get a more precise and broader idea about the prescription pattern nationwide during that pandemic period, a larger survey is recommended across the country, including primary and secondary healthcare facilities alongside tertiary-level hospitals. Drug-drug interactions need to be further studied by clinical significance level and inpatients’ prescriptions should also be investigated and analyzed to enrich the study report. Furthermore, post-COVID prescription patterns need to be analyzed and compared with the current study findings for comprehensive interpretation of this study’s findings.
Conclusion
The current study gives a comprehensive demonstration of the healthcare-seeking tendency as well as the prescription pattern in the outpatient facilities in some Bangladeshi hospitals during the COVID-19 pandemic. The findings of this study may be helpful in guiding the concerned authority to design and implement appropriate strategies to promote prescription writing following the WHO prescription indicators, rational use of drugs, while minimizing polypharmacy practice and prescription errors. In addition, the outcomes of this survey may help in identifying and ensuring the availability of the essential medicines from different therapeutic groups while taking prophylactic measures for any prospective future outbreak of COVID-19.
Ethical Considerations
Compliance with ethical guidelines
The study was conducted following the principles of the World Medical Association and the Declaration of Helsinki. Permission to conduct the prescription survey was taken from the Faculty of Pharmacy (Reference no. Pharm.B/44/20-21), University of Dhaka, Bangladesh. The purpose of the study was explained to the non-COVID outpatients, and photos of the prescriptions were collected from the patients after obtaining consent. The confidentiality of personal information was ensured, and information was used for research purposes only.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Md. Raihan Sarkar, Nahid Sharmin; Data collection: Kazi Milenur Rahman Prattay, Md. Bappy Hawlader and Md. Saiful Islam; Formal analysis: Kazi Milenur Rahman Prattay, Md. Bappy Hawladerand Md. Saiful Islam; Investigation: Md. Bappy Hawlader and Md. Saiful Islam; Methodology: Md. Bappy Hawlader, Md. Saiful Islam, Kazi Milenur Rahman Prattay, Nahid Sharmin and Md. Raihan Sarkar; Software: Kazi Milenur Rahman Prattay, Sheikh Zahir Raihan and Md. Abdul Muhit; Supervision: Md. Raihan Sarkar and Nahid Sharmin; Writing the original draft: Md. Bappy Hawlader, Md. Saiful Islam, Kazi Milenur Rahman Prattay and Nahid Sharmin; Review and editing: Md. Raihan Sarkar, Sheikh Zahir Raihan, Md. Abdul Muhit and Nahid Sharmin
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors acknowledge the Department of Pharmacy, Faculty of Pharmacy, University of Dhaka, Bangladesh; Dhaka Medical College Hospital, Dhaka, Bangladesh; BSMMU, Dhaka, Bangladesh, and National Institute of Diseases of the Chest and Hospital, Dhaka, Bangladesh.
References
- Ather A, Neelkantreddy P, Anand G, Manjunath G, Vishwanath J, Riyaz M. A study on determination of prescription writing errors in outpatient department of medicine in a teaching hospital. Indian journal of pharmacy practice. 2013; 6(2):21-4. [Link]
- Sheikh D, Mateti UV, Kabekkodu S, Sanal T. Assessment of medication errors and adherence to WHO prescription writing guidelines in a tertiary care hospital. Future Journal of Pharmaceutical Sciences. 2017; 3(1):60-4. [DOI:10.1016/j.fjps.2017.03.001]
- Melku L, Wubetu M, Dessie B. Irrational drug use and its associated factors at Debre Markos Referral Hospital’s outpatient pharmacy in East Gojjam, Northwest Ethiopia. SAGE Open Medicine. 2021; 9:20503121211025146. [DOI:10.1177/20503121211025146] [PMID]
- Bilal AI, Osman ED, Mulugeta A. Assessment of medicines use pattern using World Health Organization’s prescribing, patient care and health facility indicators in selected health facilities in eastern Ethiopia. BMC Health Services Research. 2016; 16:144. [DOI:10.1186/s12913-016-1414-6] [PMID]
- Čižman M. The use and resistance to antibiotics in the community. International Journal of Antimicrobial Agents. 2003; 21(4):297-307. [DOI:10.1016/S0924-8579(02)00394-1] [PMID]
- Saleem Z, Hassali MA, Godman B, Hashmi FK, Saleem F. Antimicrobial prescribing and determinants of antimicrobial resistance: a qualitative study among physicians in Pakistan. International Journal of Clinical Pharmacy. 2019; 41(5):1348-58. [DOI:10.1007/s11096-019-00875-7] [PMID]
- Obreli-Neto PR, Nobili A, de Oliveira Baldoni A, Guidoni CM, de Lyra Júnior DP, Pilger D, et al. Adverse drug reactions caused by drug-drug interactions in elderly outpatients: A prospective cohort study. European Journal of Clinical Pharmacology. 2012; 68(12):1667-76. [DOI:10.1007/s00228-012-1309-3] [PMID]
- WHO. The rational use of drugs: report of the Conference of Experts, Nairobi, 25-29 November 1985. Geneva: World Health Organization; 1987. [Link]
- Hogerzeil HV, Bimo, Ross-Degnan D, Laing RO, Ofori-Adjei D, Santoso B, Azad Chowdhury AK, et al. Field tests for rational drug use in twelve developing countries. Lancet. 1993; 342(8884):1408-10. [DOI:10.1016/0140-6736(93)92760-Q] [PMID]
- Mohan P, Sharma AK, Panwar SS. Identification and quantification of prescription errors. Medical Journal, Armed Forces India. 2014; 70(2):149-53. [DOI:10.1016/j.mjafi.2014.01.002] [PMID]
- Mortazavi SA, Hajebi G. An investigation on the nature and extent of occurrence of errors of commission in hospital prescriptions. Iranian Journal of Pharmaceutical Research. 2003; 2(2):83-7. [DOI:10.22037/ijpr.2010.17]
- Sultana F, Rahman A, Paul TR, Sarwar MS, Islam MA, Rashid M. Prescribing pattern and prescription errors: A study at a tertiary care hospital of Bangladesh. Bangladesh Pharmaceutical Journal. 2015; 18(1):20-4. [DOI:10.3329/bpj.v18i1.23509]
- Rahman MM, Munia AT, Sikdar KMYK, Sarkar MR. A cross-sectional study on current prescription trends and errors in outpatient department of a Bangladeshi secondary care district hospital. Perspectives in Clinical Research. 2022; 13(3):161-7. [DOI:10.4103/picr.PICR_245_20] [PMID]
- Afsan M, Alam MM, Noor N, Ahmed AH. Prescribing practices in the outpatient department in a tertiary care teaching hospital in Bangladesh. Update Dental College Journal. 2012; 2(2):13-7. [DOI:10.3329/updcj.v2i2.15483]
- Begum F, Uddin MR, Islam MS, Sarker MN, Barman RC, Ali MY. Evaluation of prescribing pattern of the private practitioners in Bangladesh. Faridpur Medical College Journal. 2012; 7(2):51-3. [DOI:10.3329/fmcj.v7i2.13497]
- Haque MU, Barik SA, Bashar S, Islam R, Bashar S, Kumar A, et al. Errors, omissions and medication patterns of handwritten outpatient prescriptions in Bangladesh: a cross-sectional health survey. Journal of Applied Pharmaceutical Science. 2016; 6(6):042-6. [DOI:10.7324/JAPS.2016.60608]
- Negligence in medical sector and legal remedies [Internet]. The Daily Star. 2024. Available from: [Link]
- Islam MT, Talukder AK, Siddiqui MN, Islam T. Tackling the COVID-19 pandemic: The Bangladesh perspective. Journal of Public Health Research. 2020; 9(4):1794. [DOI:10.4081/jphr.2020.1794] [PMID]
- Tobaiqy M, Qashqary M, Al-Dahery S, Mujallad A, Hershan AA, Kamal MA, et al. Therapeutic management of patients with COVID-19: a systematic review. Infection Prevention in Practice. 2020; 2(3):100061. [DOI:10.1016/j.infpip.2020.100061] [PMID]
- Wang T, Du Z, Zhu F, Cao Z, An Y, Gao Y, et al. Comorbidities and multi-organ injuries in the treatment of COVID-19. Lancet. 2020; 395(10228):e52. [DOI:10.1016/S0140-6736(20)30558-4] [PMID]
- Singh S, Patil L, Nishat SA. A prospective cross-sectional study of prescription pattern of drugs used in the treatment of COVID-19 in a tertiary care hospital. National Journal of Physiology, Pharmacy and Pharmacology. 2022; 12(11):1816-20. [DOI:10.5455/njppp.2022.12.03105202212032022]
- Silva TM, Estrela M, Gomes ER, Piñeiro-Lamas M, Figueiras A, Roque F, et al. The impact of the COVID-19 pandemic on antibiotic prescribing trends in outpatient care: A nationwide, quasi-experimental approach. Antibiotics. 2021; 10(9):1040. [DOI:10.3390/antibiotics10091040] [PMID]
- Aboulatta L, Peymani P, Vaccaro C, Leong C, Kowalec K, Delaney J, et al. Drug utilization patterns before and during COVID-19 pandemic in Manitoba, Canada: A population-based study. PLoS One. 2022; 17(11):e0278072. [DOI:10.1371/journal.pone.0278072] [PMID]
- Karlsson P, Nakitanda AO, Löfling L, Cesta CE. Patterns of prescription dispensation and over-the-counter medication sales in Sweden during the COVID-19 pandemic. PloS One. 2021; 16(8):e0253944. [DOI:10.1371/journal.pone.0253944] [PMID]
- Hussain AZ, Paudyal V, Hadi MA. Impact of the COVID-19 pandemic on the prescribing patterns of first-line antibiotics in English primary care: A longitudinal analysis of national prescribing dataset. Antibiotics. 2021; 10(5):591. [DOI:10.3390/antibiotics10050591] [PMID]
- Molla MMA, Yeasmin M, Islam MK, Sharif MM, Amin MR, Nafisa T, et al. Antibiotic prescribing patterns at COVID-19 dedicated wards in Bangladesh: Findings from a single center study. Infection Prevention in Practice. 2021; 3(2):100134. [DOI:10.1016/j.infpip.2021.100134] [PMID]
- Jacob S, Malviya R, Sandhan S, Deshpande P. Evaluation of prescribing pattern based on World Health Organization indicators in Maharashtra during COVID-19 pandemic. Indian Journal of Community and Family Medicine. 2022; 8(2):121-8. [DOI:10.4103/ijcfm.ijcfm_100_21]
- Abubakar MM, Loosli K, Isah A, Usman M, Fatokun O, Amidu I, et al. Assessing the impact of COVID-19 on prescription patterns and antibiotic use: Insights from three military health facilities. Research in Social and Administrative Pharmacy. 2024; 20(2):157-62. [DOI:10.1016/j.sapharm.2023.10.013] [PMID]
- Atif M, Azeem M, Sarwar MR, Shahid S, Javaid S, Ikram H, et al. WHO/INRUD prescribing indicators and prescribing trends of antibiotics in the Accident and Emergency Department of Bahawal Victoria Hospital, Pakistan. Springerplus. 2016; 5(1):1928. [DOI:10.1186/s40064-016-3615-1] [PMID]
- Rodríguez-Vera FJ, Marín Y, Sánchez A, Borrachero C, Pujol E. Illegible handwriting in medical records. Journal of the Royal Society of Medicine. 2002; 95(11):545-6. [DOI:10.1177/014107680209501105] [PMID]
- Stelmach R, do Patrocínio T Nunes M, Ribeiro M, Cukier A. Effect of treating allergic rhinitis with corticosteroids in patients with mild-to-moderate persistent asthma. Chest. 2005; 128(5):3140-7. [DOI:10.1378/chest.128.5.3140] [PMID]
- Hossen A, Westhues A. Improving access to government health care in rural Bangladesh: The voice of older adult women. Health Care for Women International. 2011; 32(12):1088-110. [DOI:10.1080/07399332.2011.603862] [PMID]
- Onay ZR, Mavi D, Ayhan Y, Can Oksay S, Bilgin G, Girit S. Did hospital admissions caused by respiratory infections and asthma decrease during the COVID-19 pandemic? Medeniyet Medical Journal. 2022; 37(1):92-8. [DOI:10.4274/MMJ.galenos.2022.02779] [PMID]
- Samad MA, Sikdar KMYK, Munia AT, Patwary FT, Sarkar MR, Rashed MRI. Comparative analysis of prescription patterns and errors in government versus private hospitals in Dhaka: A cross-sectional study. Health Science Reports. 2024; 7(8):e2302. [DOI:10.1002/hsr2.2302] [PMID]
- Summoro TS, Gidebo KD, Kanche ZZ, Woticha EW. Evaluation of trends of drug-prescribing patterns based on WHO prescribing indicators at outpatient departments of four hospitals in southern Ethiopia. Drug Design, Development and Therapy. 2015; 9:4551-7. [DOI:10.2147/DDDT.S83588] [PMID]
- De Vries TP, Henning RH, Hogerzeil HV, Fresle DA, WHO. Guide to good prescribing: A practical manual. Geneva: World Health Organization; 1994. [Link]
- Shrestha R, Prajapati S. Assessment of prescription pattern and prescription error in outpatient Department at Tertiary Care District Hospital, Central Nepal. Journal of pharmaceutical policy and practice. 2019; 12:16. [DOI:10.1186/s40545-019-0177-y] [PMID]
- Haque M. Essential medicine utilization and situation in selected ten developing countries: a compendious audit. Journal of International Society of Preventive & Community Dentistry. 2017; 7(4):147-60. [DOI:10.4103/jispcd.JISPCD_224_17] [PMID]
- Horn DB, Vu L, Porter BR, Afzal M. Responsible controlled substance and opioid prescribing. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. [PMID]
- Aziz MA, Kamal MAHM, Sajon SR, Akter MI, Hossain, MS, Tajmim A, et al. Prescribing pattern and analysis of prescription errors of seven hospitals of Jessore, Jhenaidah, Kushtia and Chuadanga districts of Bangladesh. Pharmacologyonline. 2018; 1:5-13. [Link]
- Atif M, Azeem M, Rehan Sarwar M, Malik I, Ahmad W, Hassan F, et al. Evaluation of prescription errors and prescribing indicators in the private practices in Bahawalpur, Pakistan. Journal of the Chinese Medical Association. 2018; 81(5):444-9. [DOI:10.1016/j.jcma.2017.12.002] [PMID]
- Khan AR, Misdary C, Yegya-Raman N, Kim S, Narayanan N, Siddiqui S, et al. Montelukast in hospitalized patients diagnosed with COVID-19. The Journal of Asthma. 2022; 59(4):780-6. [DOI:10.1080/02770903.2021.1881967] [PMID]
- Al-Nuaimi S, Alkuwari S, Al-Jubouri AM, Hegazi S, Jolo L, Khalid H, et al. Antibiotics prescriptions pattern among Patients Visiting Primary Health Care Centers (PHCC) before and during COVID-19 pandemic: A cross-sectional population-based study from Qatar. Antibiotics. 2023; 12(8):1228. [DOI:10.3390/antibiotics12081228] [PMID]
- Rashed MR, Banerjee SK, Ahsan SA, Zaman SM, Ahmed K, Rahman MM, et al. A Comparative study of muscle symptoms of atorvastatin with rosuvastatin in patients of atherosclerotic cardiovascular disease. University Heart Journal. 2018; 14(1):9-20. [DOI:10.3329/uhj.v14i1.38481]
- Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of medication use in the ambulatory adult population of the United States: the Slone survey. Jama. 2002; 287(3):337-44. [DOI:10.1001/jama.287.3.337] [PMID]
- Tasfia SZ, Kabir MA, Islam MR, Al Mamun ME. Study on nutritional supplements for females in Dhaka City, Bangladesh. Bangladesh Pharmaceutical Journal. 2020; 23:39-43. [DOI:10.3329/bpj.v23i1.45318]
Type of Study: Orginal Article |
Subject:
● International Health
Received: 2025/05/14 | Accepted: 2025/10/18 | Published: 2026/03/1
Received: 2025/05/14 | Accepted: 2025/10/18 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
