

Volume 16, Issue 2 (March & April 2026)
J Research Health 2026, 16(2): 149-158 |
Back to browse issues page


Ethics code: IR.GMU.REC.1401.074
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
dogonchi M, Mohammadzadeh F, moshki M, safari S, ahmadpour A, alizadeh H et al . Fertility Desires and Related Social Factors in Married Individuals in Northeast Iran. J Research Health 2026; 16 (2) :149-158
URL: http://jrh.gmu.ac.ir/article-1-2723-en.html
URL: http://jrh.gmu.ac.ir/article-1-2723-en.html
Mitra Dogonchi1 

 , Fatemeh Mohammadzadeh2 , Mahdi Moshki2 , Sajedeh Safari3 , Aida Ahmadpour3 , Homa Alizadeh3 , Hosein Rezaei4
, Fatemeh Mohammadzadeh2 , Mahdi Moshki2 , Sajedeh Safari3 , Aida Ahmadpour3 , Homa Alizadeh3 , Hosein Rezaei4
, Fatemeh Mohammadzadeh2 , Mahdi Moshki2 , Sajedeh Safari3 , Aida Ahmadpour3 , Homa Alizadeh3 , Hosein Rezaei4
1- Department of Health Education and Health Promotion, Social Determinants of Health Research Center, School of Public Health, Gonabad University of Medical Sciences, Gonabad, Iran. , dogonchi.mitra@yahoo.com
2- Department of Health Education and Health Promotion, Social Determinants of Health Research Center, School of Public Health, Gonabad University of Medical Sciences, Gonabad, Iran.
3- School of Public Health, Gonabad University of Medical Sciences, Gonabad, Iran.
4- School of Nursing, Gonabad University of Medical Sciences, Gonabad, Iran.
2- Department of Health Education and Health Promotion, Social Determinants of Health Research Center, School of Public Health, Gonabad University of Medical Sciences, Gonabad, Iran.
3- School of Public Health, Gonabad University of Medical Sciences, Gonabad, Iran.
4- School of Nursing, Gonabad University of Medical Sciences, Gonabad, Iran.
Full-Text [PDF 649 kb]
(199 Downloads)
| Abstract (HTML) (776 Views)
Full-Text: (242 Views)
Introduction
Fertility and childbearing decisions are influenced by a complex interplay of personal, financial, occupational, social, and psychological factors. Key influences on the decision to have children include economic issues, occupation, interests, education, emotional readiness, and familiarity with childcare and its requirements [1]. Declining fertility is a global challenge, with the fertility rate dropping from 2.3 to 2.5 live births per woman between 1990 and 2019. Today, nearly half of the world’s population resides in countries with a lifetime fertility rate of less than 1.2 births per woman [2]. For example, China’s fertility rate decreased from 1.6 live births in 2017 to 1.3 live births in 2020 [3].
Our society faces this challenge. Iran is among the countries that have experienced a severe decline in fertility, with a decrease of more than 50%. During 2002-2006, it joined the countries with a replacement fertility level or below (a fertility rate of 1.7). According to the latest census, the population growth rate in the country was 1.2 [4]. Consequently, the childbearing rate in Iran has noticeably decreased across all age groups. Some young couples prefer to start having children later, some married women space their births, and older women stop having children [5].
If the fertility rate falls below the replacement level of 2 children per woman, the population ages, and the economic dependency ratio increases. Governments also encounter significant challenges, including a diminished supply of active labor, a crisis in pension systems, and increased strain on healthcare services. Therefore, understanding the factors influencing the desire and reluctance to have children is essential for effective population policies [6]. The decision to have children is a pivotal event in the lives of couples influenced by various aspects of life, including health, economic status, well-being, and family culture [7]. Research conducted in Bangladesh, Indonesia, and Nigeria has indicated that the influence of religious beliefs on fertility rates in these countries has decreased due to advancements in education and trends toward urbanization and individualism [8]. Research indicates that religious beliefs in Iran influence fertility rates. Religious beliefs may affect fertility by affecting the marriage age, family size, and number of children [9, 10].
Social factors and demographic characteristics influence individuals’ desire to have children [11]. These factors include age, infant mortality, religion, education level, exposure to mass media, poverty, and unemployment [12]. Additional reasons and perspectives contributing to the decline in fertility include urbanization, delayed marriage, increased education and employment for women, reduced infant mortality, enhanced empowerment and status of women, awareness of contraceptive methods, and the impact of technology and communication [13].
Another pertinent factor influencing fertility desires is social status. Social status encompasses the distinctions between social groups regarding the respect and recognition they receive from others. Indicators of an individual’s social status may include income, education, occupation, and residence. Research has demonstrated that educated parents with high occupational status and greater opportunity costs tend to desire fewer children. In contrast, low-income parents with lower occupational status and limited access to fertility control methods are more likely to have larger families. Consequently, the fertility desires of each household are closely linked to the parents’ social status [14].Various systematic studies in Iran have confirmed the impact of social factors and demographic characteristics on fertility rates [10, 15].
Social capital is another factor influencing fertility. Social capital encompasses the interactions and relationships individuals maintain within groups, social networks, and mass media, facilitating access to opportunities, information, material resources, and social status. This social capital significantly impacts an individual’s position within social space. Social networks and communication channels can provide resources such as time, financial support, employment, services, and power, enabling individuals to leverage these assets to achieve their objectives. One such objective is childbearing. Women often choose to reduce their fertility through education and employment, as they perceive childbearing as a potential obstacle to their aspirations and goals [16].
The factors leading to the decline in fertility are particularly complex. The degree of people’s desire to have children can change depending on their socio-economic characteristics and individual attitudes. Since one of the Ministry of Health’s goals is to design and implement programs to promote childbearing in the country’s healthcare network, one of the health system’s priorities is to plan and implement various educational and counseling programs and encourage eligible couples to have children. In this regard, the first step towards solving the problem and then planning to eliminate the problem is to recognize the causes and factors affecting the problem [17].
Despite humans’ real desire to have children, what factors have led to the decrease in childbearing in Iranian society? What social factors affect the desire for fertility among married women and men? Therefore, this study aimed to investigate the desire for fertility and its related social factors among married individuals in Gonabad City, Iran.
Methods
Study design and sample
This study employed a cross-sectional analytical design. This report was prepared using the Strengthening the Reporting of observational studies in epidemiology statement checklist for cross-sectional studies.
Participants and setting
Participants were married couples receiving care from comprehensive health service centers in Gonabad City, Northeast Iran, during 2022-2023. The inclusion criteria included married individuals of reproductive age (15-49 years) who provided informed consent to participate. The exclusion criteria included pregnancy, prior vasectomy or tubectomy, menopause in women, and infertility in both men and women. Individuals who did not complete the questionnaire in full were excluded.
Sample size and sampling strategy
The sample size was calculated based on a similar study [18], with S=11.23, using a formula that accounted for a type I error of 0.05, a test power of 0.8, and an error margin of d=1.4. This calculation yielded an initial sample size of 505, then adjusted to 556 to accommodate a 10% dropout rate.
The sampling method was random stratified sampling, proportional to the population size. Using this approach, each comprehensive health service center in Gonabad City was classified into a distinct category. The number of married men and women served by each center was first determined, after which a proportionate sample was selected from each center’s population, using a simple random sampling technique among those meeting the inclusion criteria for the study.
Study tools
The data collection tool in this study was a multidimensional questionnaire, which included a demographic questionnaire with questions on age, gender, place of residence, housing status, education level of the couple, occupation of the couple, economic status, number of children, number of deceased children, number of abortions, number of stillbirths, participants’ opinions about the sufficient number of children, and age of marriage.
In addition, the intention to have children in the future was measured using six questions (yes or no). The next section is the fertility desire questionnaire, which includes 19 questions using a five-point Likert scale from strongly agree (score 1) to disagree (score 5). In this questionnaire, questions 1, 2, 3, 4, 7, 11, 12, 14, 15, and 18 have positive points, while questions 5, 6, 8, 9, 10, 13, 16, 17, and 19 have negative points. This questionnaire’s validity and reliability coefficient have been reported to be 0.89 [19].
The onyx and bolen social capital questionnaire comprises 36 items categorized into eight domains. These domains include value of life, consisting of two items; participation in local communities, composed of seven items; initiative in social activities, consisting of seven items; trust and security, composed of five items; relationship with neighbors, consisting of five items; relationship with friends and family, consisting of three items; tolerance of differences, composed of two items; and work relationship, consisting of two items. Additionally, two items were analyzed separately due to their relevance across multiple domains, allowing for the calculation of the total social capital score.
This questionnaire includes response options that evaluate individuals’ levels of social capital across four ranges, from “not at all” to “many times”. To determine the overall level of social capital, responses were scored from 1 to 4, with the cumulative score representing the total social capital; a higher score indicated greater social capital. The minimum possible score for the questionnaire was 36, while the maximum score was 144. The validity and reliability of the questionnaire have been confirmed in numerous studies in Iran, with a reliability coefficient of 0.82 [20, 21]. The reliability coefficient of this questionnaire has been reported to be 0.79 [22]. The scoring system ranges from a very low score of 1 to a very high score of 5.
Statistical analysis
Data analysis was conducted using SPSS software, version 21. The normality of quantitative variables was assessed using the Kolmogorov-Smirnov test by evaluating skewness and kurtosis indices. Descriptive statistics were reported for normally distributed quantitative variables as Mean±SD, non-normally distributed quantitative variables as median (first quartile, third quartile), and qualitative variables as frequencies and percentages. Pearson’s correlation coefficient test was used to analyze the relationship between fertility, socioeconomic status, and social capital. A simple linear regression model was initially utilized to examine the relationship between fertility desire and the subscales of social capital. Variables with a P<0.25 in the univariate analysis were included in the multiple linear regression model, with a significance level set at <0.05.
Results
Demographic and individual characteristics of participants
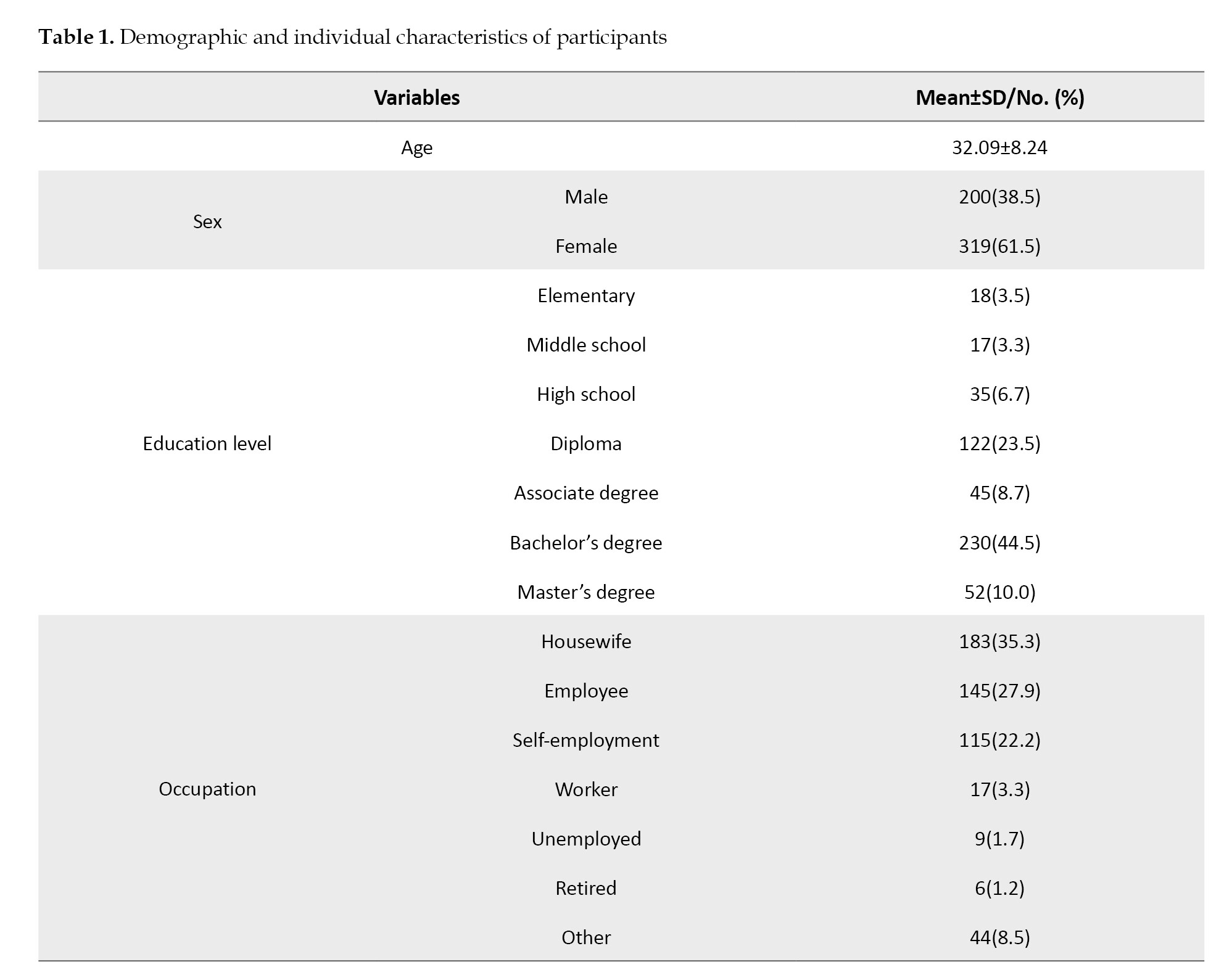
In this study, data from 519 participants were analyzed. The Mean±SD age of participants was 32.09±8.25 years, ranging from 18 to 49 years. The Mean±SD age at marriage was 21.68±4.16 years, ranging from 10 to 40 years. Female participants comprised 61.5% of the sample. Additionally, 63.0% of participants and 61.0% of their spouses held university degrees. Most participants (87.9%) resided in urban areas. The Mean±SD number of children among participants was 1.55±1.35, ranging from zero to eight children; of the participants, 29.7% reported having no children, and 18.3% had only one child. Most participants (41.2%) considered two children to be the ideal number. Table 1 presents the participants’ other characteristics.
Socioeconomic status
Participants’ Mean±SD socioeconomic status score was 15.83±4.37. Of the participants, 25.6% were categorized as having low or lower-middle socioeconomic status, 47.2% were classified at the middle level, and the remaining participants were identified as upper-middle or upper-level (Table 1).
Fertility desire
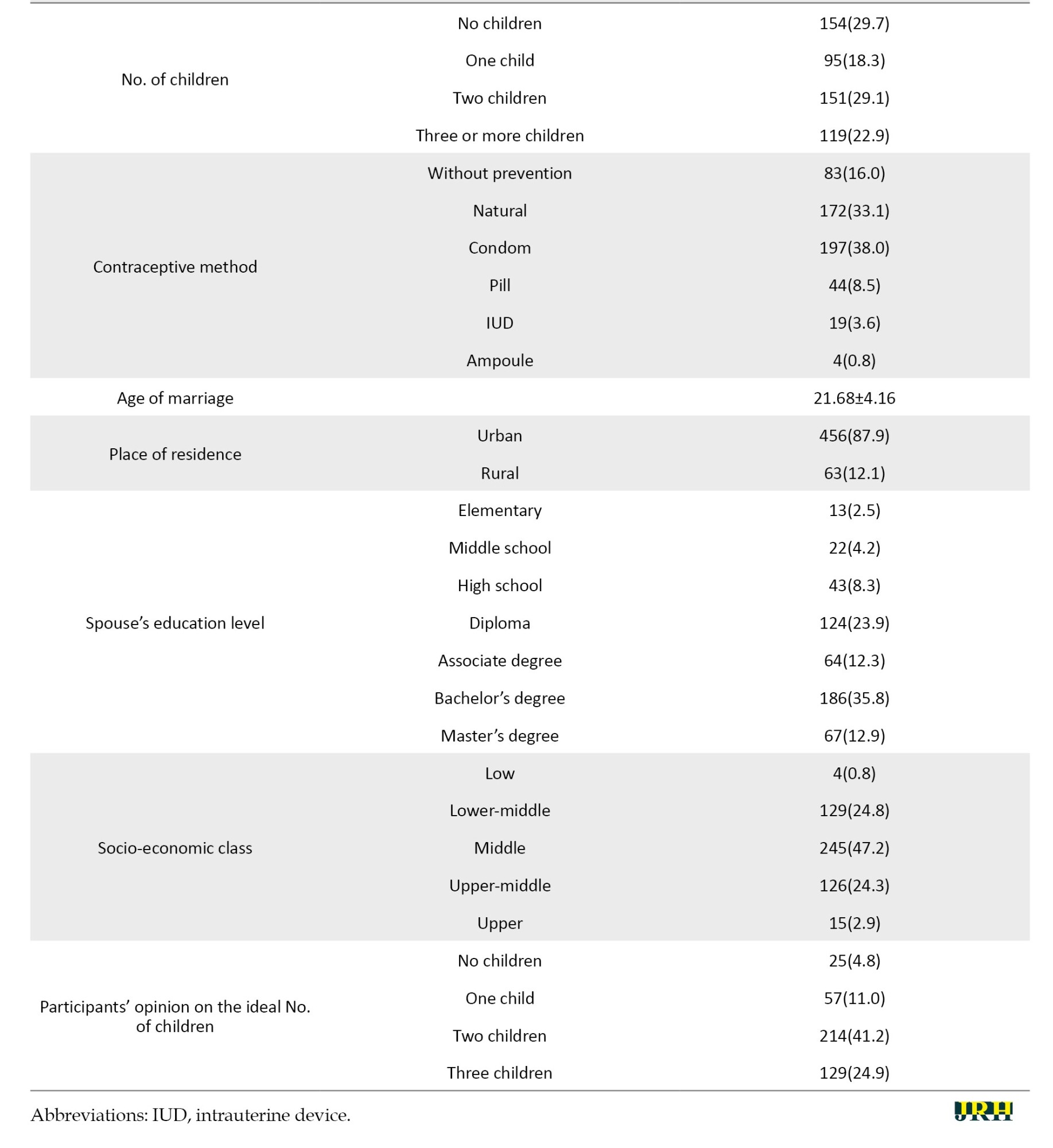
Table 2 presents the descriptive statistics of fertility desire components among participants. The highest Mean±SD score was for positive childbearing motivations (22.01±4.54), followed by social beliefs (12.54±3.03). The overall Mean±SD score of fertility desire among participants was 53.68±4.57. Based on the cut-off points defined in this study—determined by the quartiles of the questionnaire score distribution (very low: 19–38, low: 38–57, moderate: 57–76, and high: 76–95)—17.7% of participants had a low level of fertility desire, while the rest had a moderate level.
Social capital status among participants
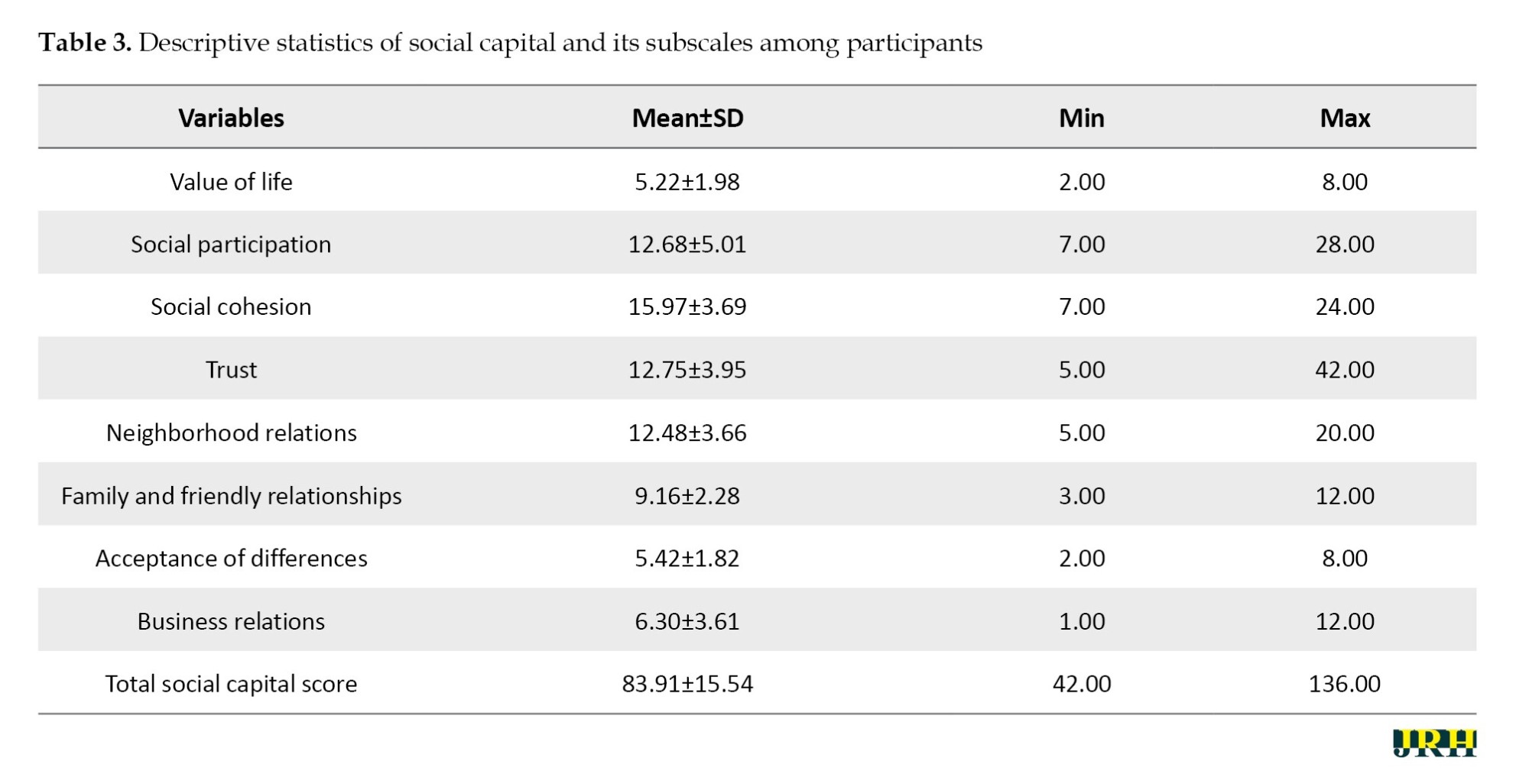
Table 3 presents the descriptive statistics for the components of social capital. The highest Mean±SD score was for social cohesion (15.97±3.69), while the lowest mean score was for the value of life (5.22±1.98). According to the cut-off points derived from the quartiles of the score distribution (36-63, 63-90, 90-117, and 117-144), the participants’ levels of social capital were categorized as very low (8.1%), low (59.9%), moderate (29.5%), and high (2.5%).
Relationship between fertility desire, socioeconomic status, and social capital
The Pearson correlation test results indicated no statistically significant relationship between fertility desire and socioeconomic status (P=0.542, r=0.027) or between fertility desire and social capital (P=0.949, r=0.003).
Relationship between fertility desire and social capital subscales
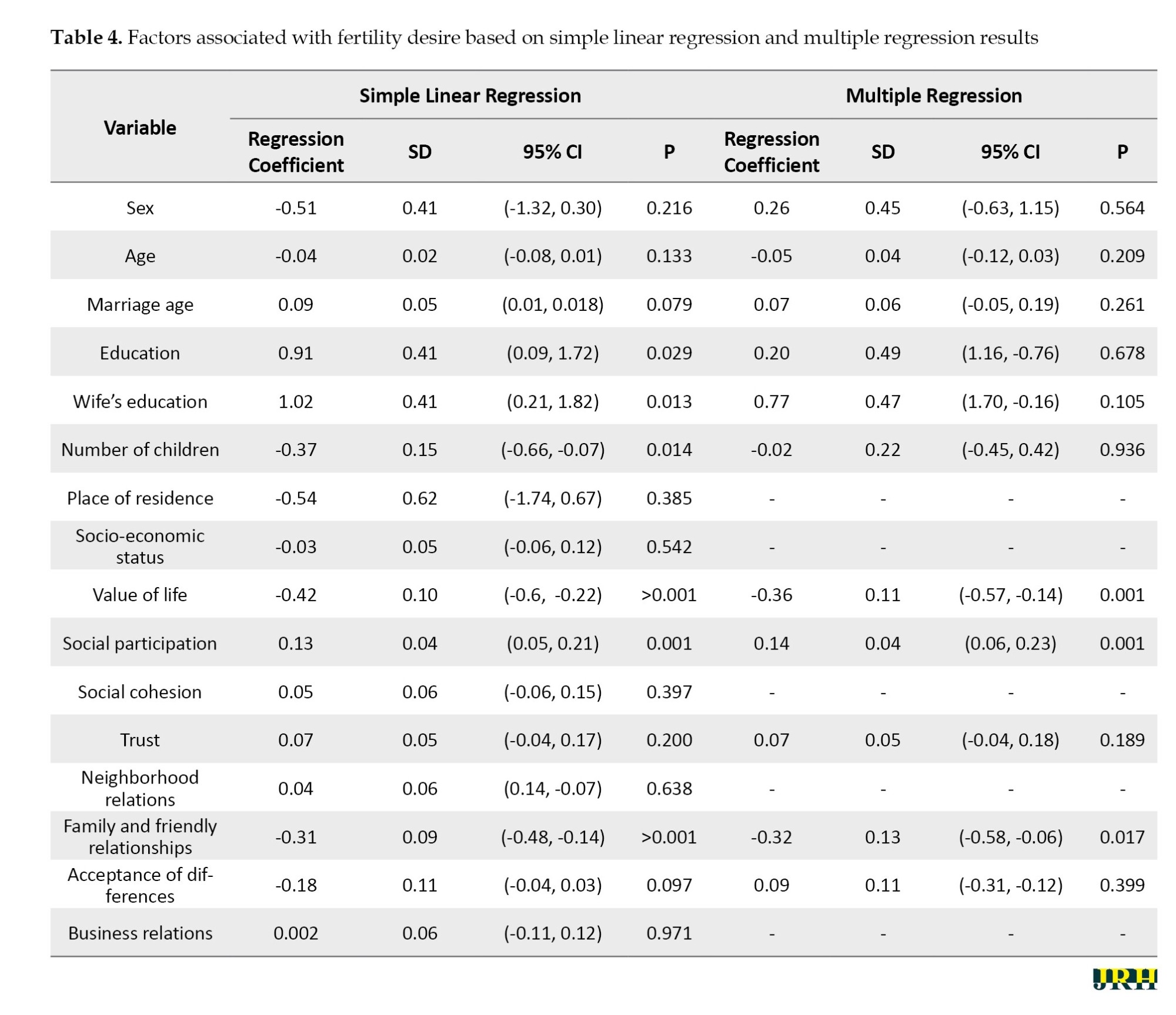
Based on the results of simple linear regression, the subscales of value of life, social participation, trust, family and friendship relations, and acceptance of differences exhibited P<0.25 in the simple regression analysis. These subscales were subsequently included in a multiple regression analysis alongside individual characteristics, such as gender, age, age at marriage, education level, spouse’s education, and number of children because these characteristics were also identified as potential confounding variables with P<0.25. The results of the multiple regression model indicated that, after adjusting for the effects of confounding variables, a statistically significant relationship was observed between the value of life, social participation, family and friendship relations, and fertility desire. Specifically, for each one-unit increase in the value of life score, the average fertility desire score decreased by 0.36 units (P=0.001). For each one-unit increase in the social participation score, the average fertility desire score increased by 0.14 units (P=0.001). Additionally, for every one-unit increase in the family and friendship relationships, the average fertility desire score decreased by 0.32 units (P=0.017) (Table 4).
The adjusted R² of the multiple regression model was 0.075, indicating that only 7.5% of the variability in fertility desire is explained by the predictors, highlighting the model’s limited explanatory power. Additionally, the mean squared error (MSE) of 18.90 reflected a relatively high average deviation between observed and predicted values, further emphasizing the model’s limited predictive accuracy. Together, the low adjusted R² and high MSE suggested that the model has limited ability to explain or predict fertility desire based on the current predictors.
Discussion
In recent years, shifting economic and social dynamics in Iran have contributed to a gradual transformation of the traditional family model, which has led to a reduction in the number of children being born. This study investigates fertility levels and the associated social factors among married individuals. The results of studies on individuals’ fertility desires indicate that, in general, women’s desire for fertility has decreased. Among the components of social capital, the highest average score was associated with social cohesion, while the lowest average score was related to the value of life. Overall, most participants had a low social capital level. Additionally, the results revealed no relationship between the desire for fertility and socio-economic status or social capital. The findings showed that 29.7% of participants were childless, while 18.3% reported being only children. Among the components of fertility desire, the highest mean score was linked to positive motivations for childbearing, followed by social beliefs. However, the overall fertility levels among individuals at the county level were low.
Research indicates a general decline in women’s desire for fertility [23, 24]. Regarding social capital, the highest mean score was attributed to social cohesion, while the lowest was associated with the perceived value of life. Overall, the level of social capital among the participants was low.
The results indicated no relationship between the desire for fertility, socioeconomic status, and social capital. However, a statistically significant relationship was found between the desire for fertility and the value of life, social participation, and family and friendship relationships. Specifically, for each one-unit increase in the value of the life score, the average score for the desire for fertility decreased by 0.36 units. Conversely, for each one-unit increase in the social participation score, the average desire for fertility score increased by 0.14 units. Additionally, for each one-unit increase in the score for family and friendship relationships, the average score for the desire for fertility decreased by 0.32.
According to the study by Alidousti et al. (2024) [25] in Iran, approximately 2.7% of individuals are childless, while 33.1% have one child and do not intend to have any more. In contrast, countries, such as Ethiopia, exhibit a high fertility desire [26]. A systematic review and meta-analysis were performed to explore the prevalence of factors influencing the intention to have a second child among urban women in China. The findings revealed that the overall prevalence of the desire for a second child among women is 37%. Furthermore, the degree of urban development is inversely related to the fertility intentions of urban women, indicating that as urban areas become more developed, the preference for a second child decreases [27]. In the present study, no significant relationship was observed between social capital and fertility desires, consistent with the findings of a study conducted in Tabriz City, Iran [28]. Social capital refers to the collective assets that facilitate action and assist individuals in achieving their goals. It acts as an intermediary through which individuals gain insights into population behaviors. Conversely, the study by Ma et al. (2024) [29] conducted in China demonstrated that social capital significantly influences childbearing among rural women, which contradicts the results of this study. Additional research [13, 16, 24, 30] indicates that higher levels of social capital are correlated with an increased desire for fertility. Social capital is a valuable resource in individuals’ lives, and a supportive social environment fosters a specific type of social capital related to fertility. It can be concluded that reciprocal relationships characterized by help and support enhance the propensity to have children. Women’s social participation and engagement in social matters can enhance their economic independence [31]. As women become acquainted with various educational and recreational opportunities, as well as social and cultural associations through mass media and networks of friends, their increased activity may lead to a heightened desire for motherhood.
In a study conducted [32] in Tehran, it was observed that most participants displayed an average level of social capital. In contrast, the present study revealed that participants have a low level of social capital. This difference may be due to cultural variations between large and small cities. Research by Alidousti et al. [25] and Kermanshah and Abbasi et al. [33] showed no significant relationship between the desire to have children and socioeconomic status, which is consistent with the results of the current study.
The results of the present study indicate that a higher social participation score correlates with an increased desire to have children. However, a systematic study [33] revealed a negative relationship between women’s social participation and their desire to have children, which contrasts with the results of the present study. Additionally, Atif et al. (2024) [34] found that the fertility rate among women with greater social participation was relatively lower than that of those without, further highlighting inconsistencies with the present findings. Social participation allows individuals to understand social realities differently, which may affect their decisions to increase or decrease childbearing more than social interactions do.
In contemporary societies, families have designated significant leisure time and engaged in occupations outside traditional family roles, leveraging each member’s unique talents and expertise. Consequently, with the availability of social clubs and associations, the roles of childbearing and childcare have diminished, enabling individuals to participate more actively and confidently in societal and recreational activities [35].
The results of the present study indicate that as the value placed on life, family, and friendship relationships increases, the fertility desire decreases. In contrast, other studies [36] have shown that fertility desire also increases as the value of life and social support from mothers, sisters, and friends increases. The difference in findings may be affected by cultural issues in the region. Individuals often prioritize the opinions of friends, family, and society when making decisions about having children. If an individual perceives a high level of social acceptance for having children, they may comply with this expectation, whether willingly or unwillingly, and vice versa.
A key strength of the study is the active cooperation and participation of the participants in expressing their views and interests. A limitation of this study was the low participation of men, and the sample was exclusively drawn from Gonabad City. Future research should explore women’s fertility desires and the factors influencing them in other cities.
Conclusion
The results of the present study indicate that women’s desire for fertility is currently low. This finding reflects a shift in women’s attitudes toward fertility, suggesting that the government should consider the factors affecting fertility when formulating policies, particularly cultural and social influences. Given the significance of childbearing and the existing population incentive policies in Iran, policymakers should develop programs and implement practical measures to encourage women to have children. While the findings of this study highlight factors associated with childbearing, and given that childbearing helps strengthen the foundations of young families and society, the high reluctance to have children is a crucial indicator that should be considered in national planning by relevant officials. This consideration assists the country in mitigating the potential harms of population decline and aging in the future. Also, the results of the present study indicated that the independent variables examined explained only a small portion of the variability in fertility desire, suggesting that the changes in fertility desire are likely dependent on other factors not included in this study. Therefore, future studies should focus on identifying and investigating these additional variables.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Gonabad University of Medical Sciences, Gonabad, Iran (Code: IR.GMU.REC.1400.215). After explaining the objectives of the study, the subjects were assured that their characteristics and information would remain confidential, and informed consent was obtained from them to participate in the study before answering the questions.
Funding
This study was financially supported by Gonabad University of Medical Sciences, Gonabad, Iran, supported this study (Grant No.: 1071).
Authors' contributions
Conceptualization and study design: Mitra Dogonchi and Mahdi Moshki; Data collection and processing: Aida Ahmadpour, Hosein Rezaei, Homa Alizadeh and Sajedeh Safari; Data analysis and interpretation: Fatemeh Mohammadzadeh; Literature search: Mitra Dogonchi; Manuscript writing: Mitra Dogonchi and Fatemeh Mohammadzadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express their appreciation and gratitude to all those who participated in this study.
References
Fertility and childbearing decisions are influenced by a complex interplay of personal, financial, occupational, social, and psychological factors. Key influences on the decision to have children include economic issues, occupation, interests, education, emotional readiness, and familiarity with childcare and its requirements [1]. Declining fertility is a global challenge, with the fertility rate dropping from 2.3 to 2.5 live births per woman between 1990 and 2019. Today, nearly half of the world’s population resides in countries with a lifetime fertility rate of less than 1.2 births per woman [2]. For example, China’s fertility rate decreased from 1.6 live births in 2017 to 1.3 live births in 2020 [3].
Our society faces this challenge. Iran is among the countries that have experienced a severe decline in fertility, with a decrease of more than 50%. During 2002-2006, it joined the countries with a replacement fertility level or below (a fertility rate of 1.7). According to the latest census, the population growth rate in the country was 1.2 [4]. Consequently, the childbearing rate in Iran has noticeably decreased across all age groups. Some young couples prefer to start having children later, some married women space their births, and older women stop having children [5].
If the fertility rate falls below the replacement level of 2 children per woman, the population ages, and the economic dependency ratio increases. Governments also encounter significant challenges, including a diminished supply of active labor, a crisis in pension systems, and increased strain on healthcare services. Therefore, understanding the factors influencing the desire and reluctance to have children is essential for effective population policies [6]. The decision to have children is a pivotal event in the lives of couples influenced by various aspects of life, including health, economic status, well-being, and family culture [7]. Research conducted in Bangladesh, Indonesia, and Nigeria has indicated that the influence of religious beliefs on fertility rates in these countries has decreased due to advancements in education and trends toward urbanization and individualism [8]. Research indicates that religious beliefs in Iran influence fertility rates. Religious beliefs may affect fertility by affecting the marriage age, family size, and number of children [9, 10].
Social factors and demographic characteristics influence individuals’ desire to have children [11]. These factors include age, infant mortality, religion, education level, exposure to mass media, poverty, and unemployment [12]. Additional reasons and perspectives contributing to the decline in fertility include urbanization, delayed marriage, increased education and employment for women, reduced infant mortality, enhanced empowerment and status of women, awareness of contraceptive methods, and the impact of technology and communication [13].
Another pertinent factor influencing fertility desires is social status. Social status encompasses the distinctions between social groups regarding the respect and recognition they receive from others. Indicators of an individual’s social status may include income, education, occupation, and residence. Research has demonstrated that educated parents with high occupational status and greater opportunity costs tend to desire fewer children. In contrast, low-income parents with lower occupational status and limited access to fertility control methods are more likely to have larger families. Consequently, the fertility desires of each household are closely linked to the parents’ social status [14].Various systematic studies in Iran have confirmed the impact of social factors and demographic characteristics on fertility rates [10, 15].
Social capital is another factor influencing fertility. Social capital encompasses the interactions and relationships individuals maintain within groups, social networks, and mass media, facilitating access to opportunities, information, material resources, and social status. This social capital significantly impacts an individual’s position within social space. Social networks and communication channels can provide resources such as time, financial support, employment, services, and power, enabling individuals to leverage these assets to achieve their objectives. One such objective is childbearing. Women often choose to reduce their fertility through education and employment, as they perceive childbearing as a potential obstacle to their aspirations and goals [16].
The factors leading to the decline in fertility are particularly complex. The degree of people’s desire to have children can change depending on their socio-economic characteristics and individual attitudes. Since one of the Ministry of Health’s goals is to design and implement programs to promote childbearing in the country’s healthcare network, one of the health system’s priorities is to plan and implement various educational and counseling programs and encourage eligible couples to have children. In this regard, the first step towards solving the problem and then planning to eliminate the problem is to recognize the causes and factors affecting the problem [17].
Despite humans’ real desire to have children, what factors have led to the decrease in childbearing in Iranian society? What social factors affect the desire for fertility among married women and men? Therefore, this study aimed to investigate the desire for fertility and its related social factors among married individuals in Gonabad City, Iran.
Methods
Study design and sample
This study employed a cross-sectional analytical design. This report was prepared using the Strengthening the Reporting of observational studies in epidemiology statement checklist for cross-sectional studies.
Participants and setting
Participants were married couples receiving care from comprehensive health service centers in Gonabad City, Northeast Iran, during 2022-2023. The inclusion criteria included married individuals of reproductive age (15-49 years) who provided informed consent to participate. The exclusion criteria included pregnancy, prior vasectomy or tubectomy, menopause in women, and infertility in both men and women. Individuals who did not complete the questionnaire in full were excluded.
Sample size and sampling strategy
The sample size was calculated based on a similar study [18], with S=11.23, using a formula that accounted for a type I error of 0.05, a test power of 0.8, and an error margin of d=1.4. This calculation yielded an initial sample size of 505, then adjusted to 556 to accommodate a 10% dropout rate.
The sampling method was random stratified sampling, proportional to the population size. Using this approach, each comprehensive health service center in Gonabad City was classified into a distinct category. The number of married men and women served by each center was first determined, after which a proportionate sample was selected from each center’s population, using a simple random sampling technique among those meeting the inclusion criteria for the study.
Study tools
The data collection tool in this study was a multidimensional questionnaire, which included a demographic questionnaire with questions on age, gender, place of residence, housing status, education level of the couple, occupation of the couple, economic status, number of children, number of deceased children, number of abortions, number of stillbirths, participants’ opinions about the sufficient number of children, and age of marriage.
In addition, the intention to have children in the future was measured using six questions (yes or no). The next section is the fertility desire questionnaire, which includes 19 questions using a five-point Likert scale from strongly agree (score 1) to disagree (score 5). In this questionnaire, questions 1, 2, 3, 4, 7, 11, 12, 14, 15, and 18 have positive points, while questions 5, 6, 8, 9, 10, 13, 16, 17, and 19 have negative points. This questionnaire’s validity and reliability coefficient have been reported to be 0.89 [19].
The onyx and bolen social capital questionnaire comprises 36 items categorized into eight domains. These domains include value of life, consisting of two items; participation in local communities, composed of seven items; initiative in social activities, consisting of seven items; trust and security, composed of five items; relationship with neighbors, consisting of five items; relationship with friends and family, consisting of three items; tolerance of differences, composed of two items; and work relationship, consisting of two items. Additionally, two items were analyzed separately due to their relevance across multiple domains, allowing for the calculation of the total social capital score.
This questionnaire includes response options that evaluate individuals’ levels of social capital across four ranges, from “not at all” to “many times”. To determine the overall level of social capital, responses were scored from 1 to 4, with the cumulative score representing the total social capital; a higher score indicated greater social capital. The minimum possible score for the questionnaire was 36, while the maximum score was 144. The validity and reliability of the questionnaire have been confirmed in numerous studies in Iran, with a reliability coefficient of 0.82 [20, 21]. The reliability coefficient of this questionnaire has been reported to be 0.79 [22]. The scoring system ranges from a very low score of 1 to a very high score of 5.
Statistical analysis
Data analysis was conducted using SPSS software, version 21. The normality of quantitative variables was assessed using the Kolmogorov-Smirnov test by evaluating skewness and kurtosis indices. Descriptive statistics were reported for normally distributed quantitative variables as Mean±SD, non-normally distributed quantitative variables as median (first quartile, third quartile), and qualitative variables as frequencies and percentages. Pearson’s correlation coefficient test was used to analyze the relationship between fertility, socioeconomic status, and social capital. A simple linear regression model was initially utilized to examine the relationship between fertility desire and the subscales of social capital. Variables with a P<0.25 in the univariate analysis were included in the multiple linear regression model, with a significance level set at <0.05.
Results
Demographic and individual characteristics of participants
In this study, data from 519 participants were analyzed. The Mean±SD age of participants was 32.09±8.25 years, ranging from 18 to 49 years. The Mean±SD age at marriage was 21.68±4.16 years, ranging from 10 to 40 years. Female participants comprised 61.5% of the sample. Additionally, 63.0% of participants and 61.0% of their spouses held university degrees. Most participants (87.9%) resided in urban areas. The Mean±SD number of children among participants was 1.55±1.35, ranging from zero to eight children; of the participants, 29.7% reported having no children, and 18.3% had only one child. Most participants (41.2%) considered two children to be the ideal number. Table 1 presents the participants’ other characteristics.
Socioeconomic status
Participants’ Mean±SD socioeconomic status score was 15.83±4.37. Of the participants, 25.6% were categorized as having low or lower-middle socioeconomic status, 47.2% were classified at the middle level, and the remaining participants were identified as upper-middle or upper-level (Table 1).
Fertility desire
Table 2 presents the descriptive statistics of fertility desire components among participants. The highest Mean±SD score was for positive childbearing motivations (22.01±4.54), followed by social beliefs (12.54±3.03). The overall Mean±SD score of fertility desire among participants was 53.68±4.57. Based on the cut-off points defined in this study—determined by the quartiles of the questionnaire score distribution (very low: 19–38, low: 38–57, moderate: 57–76, and high: 76–95)—17.7% of participants had a low level of fertility desire, while the rest had a moderate level.
Social capital status among participants
Table 3 presents the descriptive statistics for the components of social capital. The highest Mean±SD score was for social cohesion (15.97±3.69), while the lowest mean score was for the value of life (5.22±1.98). According to the cut-off points derived from the quartiles of the score distribution (36-63, 63-90, 90-117, and 117-144), the participants’ levels of social capital were categorized as very low (8.1%), low (59.9%), moderate (29.5%), and high (2.5%).
Relationship between fertility desire, socioeconomic status, and social capital
The Pearson correlation test results indicated no statistically significant relationship between fertility desire and socioeconomic status (P=0.542, r=0.027) or between fertility desire and social capital (P=0.949, r=0.003).
Relationship between fertility desire and social capital subscales
Based on the results of simple linear regression, the subscales of value of life, social participation, trust, family and friendship relations, and acceptance of differences exhibited P<0.25 in the simple regression analysis. These subscales were subsequently included in a multiple regression analysis alongside individual characteristics, such as gender, age, age at marriage, education level, spouse’s education, and number of children because these characteristics were also identified as potential confounding variables with P<0.25. The results of the multiple regression model indicated that, after adjusting for the effects of confounding variables, a statistically significant relationship was observed between the value of life, social participation, family and friendship relations, and fertility desire. Specifically, for each one-unit increase in the value of life score, the average fertility desire score decreased by 0.36 units (P=0.001). For each one-unit increase in the social participation score, the average fertility desire score increased by 0.14 units (P=0.001). Additionally, for every one-unit increase in the family and friendship relationships, the average fertility desire score decreased by 0.32 units (P=0.017) (Table 4).
The adjusted R² of the multiple regression model was 0.075, indicating that only 7.5% of the variability in fertility desire is explained by the predictors, highlighting the model’s limited explanatory power. Additionally, the mean squared error (MSE) of 18.90 reflected a relatively high average deviation between observed and predicted values, further emphasizing the model’s limited predictive accuracy. Together, the low adjusted R² and high MSE suggested that the model has limited ability to explain or predict fertility desire based on the current predictors.
Discussion
In recent years, shifting economic and social dynamics in Iran have contributed to a gradual transformation of the traditional family model, which has led to a reduction in the number of children being born. This study investigates fertility levels and the associated social factors among married individuals. The results of studies on individuals’ fertility desires indicate that, in general, women’s desire for fertility has decreased. Among the components of social capital, the highest average score was associated with social cohesion, while the lowest average score was related to the value of life. Overall, most participants had a low social capital level. Additionally, the results revealed no relationship between the desire for fertility and socio-economic status or social capital. The findings showed that 29.7% of participants were childless, while 18.3% reported being only children. Among the components of fertility desire, the highest mean score was linked to positive motivations for childbearing, followed by social beliefs. However, the overall fertility levels among individuals at the county level were low.
Research indicates a general decline in women’s desire for fertility [23, 24]. Regarding social capital, the highest mean score was attributed to social cohesion, while the lowest was associated with the perceived value of life. Overall, the level of social capital among the participants was low.
The results indicated no relationship between the desire for fertility, socioeconomic status, and social capital. However, a statistically significant relationship was found between the desire for fertility and the value of life, social participation, and family and friendship relationships. Specifically, for each one-unit increase in the value of the life score, the average score for the desire for fertility decreased by 0.36 units. Conversely, for each one-unit increase in the social participation score, the average desire for fertility score increased by 0.14 units. Additionally, for each one-unit increase in the score for family and friendship relationships, the average score for the desire for fertility decreased by 0.32.
According to the study by Alidousti et al. (2024) [25] in Iran, approximately 2.7% of individuals are childless, while 33.1% have one child and do not intend to have any more. In contrast, countries, such as Ethiopia, exhibit a high fertility desire [26]. A systematic review and meta-analysis were performed to explore the prevalence of factors influencing the intention to have a second child among urban women in China. The findings revealed that the overall prevalence of the desire for a second child among women is 37%. Furthermore, the degree of urban development is inversely related to the fertility intentions of urban women, indicating that as urban areas become more developed, the preference for a second child decreases [27]. In the present study, no significant relationship was observed between social capital and fertility desires, consistent with the findings of a study conducted in Tabriz City, Iran [28]. Social capital refers to the collective assets that facilitate action and assist individuals in achieving their goals. It acts as an intermediary through which individuals gain insights into population behaviors. Conversely, the study by Ma et al. (2024) [29] conducted in China demonstrated that social capital significantly influences childbearing among rural women, which contradicts the results of this study. Additional research [13, 16, 24, 30] indicates that higher levels of social capital are correlated with an increased desire for fertility. Social capital is a valuable resource in individuals’ lives, and a supportive social environment fosters a specific type of social capital related to fertility. It can be concluded that reciprocal relationships characterized by help and support enhance the propensity to have children. Women’s social participation and engagement in social matters can enhance their economic independence [31]. As women become acquainted with various educational and recreational opportunities, as well as social and cultural associations through mass media and networks of friends, their increased activity may lead to a heightened desire for motherhood.
In a study conducted [32] in Tehran, it was observed that most participants displayed an average level of social capital. In contrast, the present study revealed that participants have a low level of social capital. This difference may be due to cultural variations between large and small cities. Research by Alidousti et al. [25] and Kermanshah and Abbasi et al. [33] showed no significant relationship between the desire to have children and socioeconomic status, which is consistent with the results of the current study.
The results of the present study indicate that a higher social participation score correlates with an increased desire to have children. However, a systematic study [33] revealed a negative relationship between women’s social participation and their desire to have children, which contrasts with the results of the present study. Additionally, Atif et al. (2024) [34] found that the fertility rate among women with greater social participation was relatively lower than that of those without, further highlighting inconsistencies with the present findings. Social participation allows individuals to understand social realities differently, which may affect their decisions to increase or decrease childbearing more than social interactions do.
In contemporary societies, families have designated significant leisure time and engaged in occupations outside traditional family roles, leveraging each member’s unique talents and expertise. Consequently, with the availability of social clubs and associations, the roles of childbearing and childcare have diminished, enabling individuals to participate more actively and confidently in societal and recreational activities [35].
The results of the present study indicate that as the value placed on life, family, and friendship relationships increases, the fertility desire decreases. In contrast, other studies [36] have shown that fertility desire also increases as the value of life and social support from mothers, sisters, and friends increases. The difference in findings may be affected by cultural issues in the region. Individuals often prioritize the opinions of friends, family, and society when making decisions about having children. If an individual perceives a high level of social acceptance for having children, they may comply with this expectation, whether willingly or unwillingly, and vice versa.
A key strength of the study is the active cooperation and participation of the participants in expressing their views and interests. A limitation of this study was the low participation of men, and the sample was exclusively drawn from Gonabad City. Future research should explore women’s fertility desires and the factors influencing them in other cities.
Conclusion
The results of the present study indicate that women’s desire for fertility is currently low. This finding reflects a shift in women’s attitudes toward fertility, suggesting that the government should consider the factors affecting fertility when formulating policies, particularly cultural and social influences. Given the significance of childbearing and the existing population incentive policies in Iran, policymakers should develop programs and implement practical measures to encourage women to have children. While the findings of this study highlight factors associated with childbearing, and given that childbearing helps strengthen the foundations of young families and society, the high reluctance to have children is a crucial indicator that should be considered in national planning by relevant officials. This consideration assists the country in mitigating the potential harms of population decline and aging in the future. Also, the results of the present study indicated that the independent variables examined explained only a small portion of the variability in fertility desire, suggesting that the changes in fertility desire are likely dependent on other factors not included in this study. Therefore, future studies should focus on identifying and investigating these additional variables.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Gonabad University of Medical Sciences, Gonabad, Iran (Code: IR.GMU.REC.1400.215). After explaining the objectives of the study, the subjects were assured that their characteristics and information would remain confidential, and informed consent was obtained from them to participate in the study before answering the questions.
Funding
This study was financially supported by Gonabad University of Medical Sciences, Gonabad, Iran, supported this study (Grant No.: 1071).
Authors' contributions
Conceptualization and study design: Mitra Dogonchi and Mahdi Moshki; Data collection and processing: Aida Ahmadpour, Hosein Rezaei, Homa Alizadeh and Sajedeh Safari; Data analysis and interpretation: Fatemeh Mohammadzadeh; Literature search: Mitra Dogonchi; Manuscript writing: Mitra Dogonchi and Fatemeh Mohammadzadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors express their appreciation and gratitude to all those who participated in this study.
References
- Chan SL, Thumboo J, Boivin J, Saffari SE, Yin S, Yeo SR, et al. Effect of fertility health awareness strategies on fertility knowledge and childbearing in young married couples (FertStart): study protocol for an effectiveness-implementation hybrid type I multicentre three-arm parallel group open-label randomised clinical trial. BMJ open. 2022; 12(1):e051710. [DOI:10.1136/bmjopen-2021-051710] [PMID]
- Arrazy S, Purnama TB, Susanti N, Ashar YK, Sitorus MA, Fajarningtiyas DN. Family support in use of contraception in coastal slums area in Medan, North Sumatra, Indonesia. Contagion: Scientific Periodical Journal of Public Health and Coastal Health. 2022; 4(2):193-204. [DOI:10.30829/contagion.v4i2.14820]
- No Author. China’s fertility rate. 202.
- Noubakht R, Dorahaki A, Ghasemi Ardahaee A. [Estimating the total fertility rate required for the replacement level in Iran using Preston’s method from 2006 to 2015 (Persian)]. Quarterly Journal of Social sciences. 2023; 30(101):1-28. [DOI:10.7862/rz.2023.hss.09]
- Ghanbari Barzain A, Hashemianfar A, Davoodi B. [Sociological study of influencing factors in the tendency of divorced women to remarry (case study of Isfahan city) (Persian)]. Journal of Applied Sociology. 2023; 34(1):89-112. [DOI:10.22108/jas.2023.132909.2277]
- Erfani A, Shojaei J. [Reasons for intending to have no children in Tehran, Iran (Persian)]. Community Health. 2019; 6(2):116-29. [Link]
- Acharjee MK, Forhad MN, Das KP. Prevalent factors influencing women’s intention to limit childbearing: Empirical evidence based on Bangladesh demography and health surveys. Asian Journal of Pregnancy and Childbirth. 2020; 3(4):17-33. [DOI:10.9734/ajpcb/2020/v3i139]
- Kaufmann E. Islamism, religiosity and fertility in the muslim world. paper presented: annual meeting of the ISA’s 50th annual convention “Exploring the past, anticipating the future”. 15 Feb 2009; New York: United States. [Link]
- Azmoude E, Barati-Far S, Behnam H, Aradmehr M. Socio-demographic and religious factors affecting fertility rate among childbearing women in Easter Iran: A population-based study. Journal of Midwifery and Reproductive Health. 2019; 7(1):1553-9. [Link]
- Rahnama A, Roozbeh N, Salimi Asl A, Kazemi Gerashi Z, Abbaszadeh M, Dabiri F. [Factors related to childbearing in Iran: A systematic review (Persian)]. Journal of Preventive Medicine. 2022; 9(1):6-17. [Link]
- Casterline JB, Agyei-Mensah S. Fertility desires and the course of fertility decline in sub-Saharan Africa. Population and Development Review. 2017; 43:84-111. [DOI:10.1111/padr.12030]
- Akinyemi JO, Odimegwu CO. Social contexts of fertility desire among non-childbearing young men and women aged 15-24 years in Nigeria. Reproductive Health. 2021; 18(1):186. [DOI:10.1186/s12978-021-01237-1] [PMID]
- Besnier E. Women’s political empowerment and child health in the sustainable development era: A global empirical analysis (1990-2016). Global Public Health. 2023; 18(1):1849348. [DOI:10.1080/17441692.2020.1849348] [PMID]
- Lim AJ, Li NP, Manesi Z, Neuberg SL, van Vugt M, Meltzer AL, et al. Desire for social status affects marital and reproductive attitudes: A life history mismatch perspective. Current Research in Ecological and Social Psychology. 2023; 4:100125. [DOI:10.1016/j.cresp.2023.100125]
- Rashidi Fakari F, Simbar M, Saei Ghare Naz M, Rashidi Fakari F. Factors related to empowering iranian women’s fertility behaviors: A systematic review. Journal of Obstetrics, Gynecology and Cancer Research. 2022; 3(3):115-22. [DOI:10.30699/jogcr.3.3.115]
- Firouzbakht M, Tirgar A, Hajian-Tilaki K, Bakouei F, Riahi ME, Nikpour M. Social capital and fertility behaviors: a cross-sectional study in Iranian women health care workers. BMC women’s health. 2020; 20(1):83. [DOI:10.1186/s12905-020-00943-5] [PMID]
- Khojeh Z, Naghibi A, Khazaee-Pool M, Abdollahi F. [Investigating factors affecting childbearing, a review study (Persian)]. Journal of Mazandaran University of Medical Sciences. 2024; 34(238):101-12. [Link]
- Rad F, Savabi H. [Examining fertility tendency and social factors related to it (a case study of married women aged 15-50 living in Tabriz city) (Persian)]. Woman and Family Studies. 2015; 3(1):127-55. [Link]
- Naghibi SA, Khazaee-Pool M, Moosazadeh M. Psychometric properties of fertility desire scale (FDS) developed for Iranian parents. BMC Public Health. 2019; 19(1):1113. [DOI:10.1186/s12889-019-7413-x] [PMID]
- Yari A, Nadrian H, Rashidian H, Nedjat S, Esmaeilnasab N, Doroudi R, et al. Psychometric properties of the Persian version of Social Capital Questionnaire in Iran. Medical journal of the Islamic Republic of Iran. 2014; 28:17. [PMID]
- Eftekharian R, Kaldi A, Sum S, Sahaf R, Fadaye Vatan R. [Validity and reliability of Persian version of Onyx Social Capital Scale in elderly people (Persian)]. Iranian Journal of Ageing. 2016; 11(1):174-89. [DOI:10.21859/sija-1101174]
- Ghodratnama A, Heidarinejad S, Davoodi I. [The relationship between socio-economic status and the rate of physical activity in Shahid Chamran University Students of Ahwaz (Persian)]. Sport Management Journal. 2013; 5(16):5-20. [Link]
- Esmaeili N, Abbasi-Shavazi MJ. Impact of family policies and economic situation on low fertility in Tehran, Iran. Demographic Research. 2024; 51:107-54. [DOI:10.4054/DemRes.2024.51.5]
- Bagi M. [Childlessness and one-child intentions among recently married couples in Iran (Persian)]. Payesh. 2022; 21(1):69-79. [DOI:10.52547/payesh.21.1.69]
- Alidousti H, Safarian M, Khajeh A. [Incentive policies for childbirth and their impact on the willingness to have children: A quantitative study in the city of Islamabad-Gharb (Persian)]. Ferdowsi University of Mashhad Journal of Social Sciences. 2024; 21(1):143-74. [Link]
- Faraji E, Safiri K, Kamali A. [Social factors affecting tendency to fertility within women 18-40 years old in Ilam city (Persian)]. Journal of Woman and Society. 2018; 9(3):289-316. [Link]
- Yang Y, He R, Zhang N, Li L. Second-child fertility intentions among urban women in China: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2023; 20(4):3744. [DOI:10.3390/ijerph20043744] [PMID]
- Alizadeh Aghdam MB, Aghayari T, Soltani Bahram S, Ansari Ozi N. [Investigating the relationship between body management, social capital and generational belonging with women's reproductive behavior (Persian)]. The Women and Families Cultural-Educational. 2024; 19(69):183-201. [Link]
- Ma X, Hu Q, He J, Li C, Song M, Wang Y, et al. A study on the factors influencing the vulnerability of women of childbearing age to health poverty in rural western China. Scientific Reports. 2024; 14(1):13219. [DOI:10.1038/s41598-024-64070-z] [PMID]
- Zhao J, Zou Z, Chen J, Chen Y, Lin W, Pei X, et al. Offline social capital, online social capital, and fertility intentions: evidence from China. Humanities and Social Sciences Communications. 2024; 11(1):1-13. [DOI:10.1057/s41599-024-03643-9]
- Abbasi Shavazi MJ, Khajehsalehi Z. [Measuring the impact of women’s independence, social participation, and education on the desire to have children (Persian)]. Journal of Women in Development and Politics. 2013; 11(1):45-64. [Link]
- Kavehfirouz Z, Ramazi N, Farash N. [Investigating factors affecting the gap between actual and ideal fertility of women in Tehran (Persian)]. Women’s Strategic Studies. 2022; 24(96):113-46. [Link]
- Abbasi A, Sadeghi R, Maleki A, Balakhani G. [A meta-analysis of factors related to fertility attitudes, desires, and childbearing intentions in Iranian studies (Persian)]. Interdisciplinary Studies in the Humanities. 2022; 14(4):63-92. [Link]
- Atif M, Ayub G, Zeb J, Farooq M, Ilyas M, Shafiq M, et al. Variability in reproductive choices: A comprehensive analysis of women's working status and fertility behavior in Pakistan. Inquiry. 2024; 61:469580241237106.[DOI:10.1177/00469580241237106] [PMID]
- Huntington S. Political order in societies undergoing transformation, translated [M. Talasi, Persian trans.]. Tehran: Alam Publications; 2015. [Link]
- Nematian S, Noghani Dokht Bahmani M. [The impact of couples’ decision-making process in delayed childbearing and related social conditions (Persian)]. Sociology of Social Institutions. 2022; 8(18):139-73. [DOI:10.22080/ssi.2022.22905.1955]
Type of Study: Orginal Article |
Subject:
● Health Education
Received: 2025/01/15 | Accepted: 2025/06/21 | Published: 2026/03/1
Received: 2025/01/15 | Accepted: 2025/06/21 | Published: 2026/03/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
